lines, tubes, drains
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
why is acute care important?
- patients being discharged sooner- require more assistance
- skills can be applied to any setting
- important to understand how effects of hospitalization can impact care in other settings
- important to engage in collaborative practice with other healthcare providers!
key points to remember:
don't pull anything out!
have a plan in mind before moving the patient
ask for help!
have enough slack on lines
nurses are your friends<3
types of lines
peripheral lines and central lines
peripheral lines types
- arterial line or A-line
- intravenous IV line
central lines types
- central venous catheter
- swan-ganz catheter
- peripherally inserted central catheter/PICC
a peripheral line is
lines entering into circulation through any peripheral vessel
short term use
fluids and meds
a central line catheter is threaded through the
- internal jugular vein
- antecubital vein
- basilic vein
- subclavian vein
a central line has a tip usually resting in the ________, is there for _____ of time, more prone to _____
superior vena cava or right atrium; longer periods; infection
a central line is used for
chemotherapy, long term antibiotics, or total parenteral nutrition (TPN fluid that has every nutrient needed)
intravenous line (IV):
placement (duration and placed by)
any accessible vein (arm, leg, foot)
placed by RN
duration 3 days
intravenous line (IV): indication
administration of drugs/fluids
blood transfusions
obtaining venous blood
cannot be used to draw blood
intravenous line (IV): PT role
can usually be heparin locked (heplocked)
should obtain MD order
heplocked
The term "heplocked" usually refers to a "heparin lock", which is a medical term used in intravenous (IV) therapy.
Instead, it's "locked" with a small amount of heparin, an anticoagulant (blood thinner), to keep the IV line from clotting when it's not in use.
This setup allows quick access to the vein if medications need to be given later, without needing to insert a new IV.
It avoids the need to have a patient hooked up to fluids all the time. EASIER manageable ability of PT to move patients
Example: A nurse may say a patient is "heplocked" when the patient has an IV line in place, but no fluids are running, and the line is flushed and sealed with heparin.
arterial line (A-line):
placement (duration)
brachial artery
radial artery
femoral artery
placed by MD
arterial line (A-line): indication
monitors arterial blood pressure
access for ABG
lab data
arterial line (A-line): PT role
cannot be heplocked
transducer placed at the level of left atrium when reading
if femoral A line discontinued, pt cannot be seen/on bed rest for 60-90 minutes
central venous catheter:
placement (duration and placed by)
subclavian
internal jugular
femoral vein into superior vena cava
placed by MD
duration 2-3 weeks
central venous catheter: indication
monitoring central venous pressures
administering drugs
fluids
transfusions
TPN (total parenteral nutrition)
central venous catheter: PT role
NO ROM greater than 90 degrees at shoulder and hip;
no horizontal adduction
do not take BP on side of the line
swan-ganz catheter (PA line or pulmonary artery line)
placement (placed by)
subclavian or internal jugular vein to pulmonary artery
placed by MD
swan-ganz catheter (PA line or pulmonary artery line) indication
monitoring heart pressures
cardiac output
core temperature
pulmonary activity
swan-ganz catheter (PA line or pulmonary artery line) PT role
no ROM greater than 90 degrees at the shoulder
no horizontal adduction
avoid head and neck movements (for subclavian) that may disrupt PA line
peripherally inserted central catheter (PICC)
placement
basilic (most common)
cephalic
median cubital vein to superior or inferior vena cava
peripherally inserted central catheter (PICC) indication
access for long term administration of TPN
meds
fluids
blood products
chemotherapy
peripherally inserted central catheter (PICC) PT role
NO BP taken on involved extremity
what is the purpose of intracranial pressure monitoring? what degree do we keep the head of the bed at?
maintenance of normal cerebral perfusion pressure (CCP) and early identification of increased ICP
keep head of bed at 30 degrees
what is "normal ICP"?
4 to 15 mmHg
what will increase ICP?
lowering the head of the bed
trendelenburg position
lateral neck flexion or extreme hip flexion
valsalva maneuver (hold breath and bearing down)
noxious stimulation (vomit nausea)
pain
stress
coughing
frequent arousal from sleep
what are the values for abnormal ICP/an ICP that causes concern?
15-20 mmHg causes concern
anything greater than 20 mmHg is clearly abnormal and medical intervention is warranted
*keep ICP monitored and in mind when performing exercises- make sure it stays within normal range
ICP bolt (intracranial pressure bolt or subarachnoid bolt)
placement (placed by)
subarachnoid space via burr hole placed by MD
ICP bolt (intracranial pressure bolt or subarachnoid bolt) indication
short term use if cerebral edema prevents use of other devices
ICP bolt (intracranial pressure bolt or subarachnoid bolt) PT role
no out of bed activities-
rarely if ever put in upright position- if so need two people
focus on things that can be done in bed
ventriculostomy aka intraventricular catheter
placement (placed by)
anterior horn of lateral ventricle via burr hole placed by MD
ventriculostomy aka intraventricular catheter indication
drainage or sampling of CSF (cerebrospinal fluid)
monitoring ICP
ventriculostomy aka intraventricular catheter PT role
need to look for color changes
must note color of CSF before during and after treatment
notify nurse if color changes i.e. clear to bloody
CSF should be clear with light pink hue
ventriculostomy is considered
gold standard for measuring ICP
foramen of monro
connects lateral ventricles to third ventricle
have to be careful with ICP regarding?
open or closed catheters-
open (unclamped) allows for release of pressure
closed (clamped) means increasing pressure with movement has no way to be relieved
signs of increased ICP
headache
blurred vision
decrease in alertness
vomiting
changes in mental status: confusion
weakness or problems with moving or talking
be aware! any sudden changes are not normal
monitor symptoms with exercise
oriented x4 means?
able to answer all mental status orientation questions correctly:
person? place? time? situation?
supplemental oxygen:
placement
nasal cannula
face mask
trach mask
ventilator
supplemental oxygen indication
oxygen delivery
supplemental oxygen PT role
ask nurse if patient needs O2 with activity
is portable O2 needed?
how many liters?
does patient desaturate with activity?
check O2 sats PRN
what percentage of oxygen saturation (O2 sats) is considered normal?
normal is above 92%
no ailments or lung disorders
pulse oximeter
placement
ear lobe
finger
toe
forehead
bridge of nose
pulse oximeter indication
measure percentage of hemoglobin saturated with O2 in arterial blood
pulse oximeter PT role
have portable machine PRN to monitor patient
what is hemoglobin?
Hemoglobin is a protein in red blood cells that carries oxygen from the lungs to the body's tissues and returns carbon dioxide from the tissues back to the lungs.
telemetry (ECG)
placement
colored leads that coincide with different locations to monitor HR/RR/ and O2 sats
telemetry indication
continuous monitoring of HR and rhythm and RR
telemetry PT role
talk with nurse or telemetry tech before unhooking any leads and before and after working with pt
nasogastric/orogastric (NG/OG) tube
placement
tube placed in nose or mouth to stomach
placed by RN
nasogastric/orogastric (NG/OG) tube indication
enteral feeding
gastric drainage
decompression of the stomach
nasogastric/orogastric (NG/OG) tube PT role
may be hooked up to wall suction which may limit distance patient can be away from the bed
if clamped; monitor pt for nausea or abdominal distention BC! pressure can pull on attachment sites from the weight of it
put feedings on hold if lying flat
dobhoff tube
placement
mercury weighted tube to be passed with a guide wire thru nose into small intestines
placed by MD or special trained RN
dobhoff tube indication
long term use in a pt who cant orally ingest (surgical, comotose, stroke)
dobhoff tube PT role
don't pull it out!!!!!!
head of bed at least 30 degrees when in use- put feedings on hold if pt needs to lie flat
stop feedings when laying flat
PEG/PEJ tube
placement
percutaneous endoscopic gastronomy
percutaneous endoscopic jejunostomy
surgically placed in the stomach/jejunum
placed by MD
PEG/PEJ tube indication
enteral feeding
small intestine drainage
gastric drainage
PEG/PEJ tube PT role
watch gait belt placement/hand placements
gait belt should be placed above tube
put feedings on hold if pt lay flat
Endotrachial Tube (ET tube)
placement
PVC tube placed in trachea via nose or mouth
placed by MD
INTUBATION! attaches to ventilator
Endotrachial Tube (ET tube) indication
used to relieve airway obstruction
prevent aspiration
facilitate tracheal suction
mechanical ventilation
Endotrachial Tube (ET tube) PT role
should know if patient is weaning
must monitor vitals especially RR
tracheostomy (trach) tube
placement
indication
PT role
PVC tubing placed in trachea thru an opening in the neck (stoma)
placed by MD
tracheostomy (trach) tube indication
mechanical ventilation
prolonged ventilatory support
after laryngectomy
tracheal resection
other head/neck surgeries
tracheostomy (trach) tube PT role
if off ventilator, watch patient for coughing, sputum issue when cover is off
direct line to lung must be suctioned and cleaned
suction (yankauer suction) tube
placement
where needed
suction (yankauer suction) tube indication
used for suction of saliva
mucus
blood
etc
suction (yankauer suction) tube indication PT role
this is your friend so use it!!
physical exercise breaks up mucus
prevents aspiration
chest tube
placement
surgically placed in chest between ribs
placed by MD
chest tube indication
promotes normal intrapleural pressures/mechanics by:
1. removing air/fluid from pleural space
2. prevents re-entry of air/fluid
3. reinflates a collapsed lung
chest tube PT role
- DONT TIP!
- extension tubing if cannot be removed from wall suction
- coughing, deep breathe, and lying on side of insertion can cause discomfort
- if on water seal (removed from suction) can gait train further
- dependent position: tubes lower than insertion so drainage can occur
urinary/foley catheter
placement
bladder
placed by RN
urinary/foley catheter indication
bladder drainage
urinary/foley catheter PT role
must be taken during PT session
communication on amount and color before drainage if needed for easier ambulation
rectal tube/pouch
placement
rectum
by RN
rectal tube/pouch indication
rectal drainage
collect liquid stool
prevent skin breakdown 2 degrees runny stool
rectal tube/pouch PT role
may or may not want to sit patient up 2 degrees to discomfort or dislodging
keep collection bag below level of insertion
colostomy/ileostomy tube
placement
colon is surgically opened and brought to abdominal surface
bag placed by RN after surgery
colostomy/ileostomy tube indication
bowel elimination when colon is obstructed or not functioning
when there is a need for diversion of fecal matter
colostomy/ileostomy tube PT role
watch gait belt/hand placement
may need to be emptied before or after tx
if bag comes off- notify nurse immediately
jackson pratt (JP) drain
placement
placed at surgical site- may have one or many
placed by MD
jackson pratt (JP) drain indication
drainage of local edema/blood
jackson pratt (JP) drain PT role
don't let bulb dangle
secure bulb to gown so doesnt pull
elimates excess fluid of surgical site
constavac drain
placement
indication
PT role
placed at surgical site
drainage of local edema and blood
gravity or suction set up
what is the difference between the constavac and JP drains?
JP is gravity dependent
constavac is not gravity dependent- suctions
JP does mild drainage whilst constavac is a more efficient drainer
incentive spirometer
placement
given to patient at bedside
incentive spirometer indication
to assist with deep breathing in hopes to prevent pulmonary complications during hospital stays
prescription ex. "10x/hour"
incentive spirometer PT role
incentivize them to get to a certain number and keep increasing
encourage patient to use when in bed
sequential compression device (SCD)
placement
inflatable sleeves applied to leg (full or just lower)
prevents blood clotting
"dont like? you have to walk w me!"
sequential compression device (SCD) indication
promotes venous return and prevents DVT
inflates and deflates to encourage circulation
sequential compression device (SCD) PT role
contraindicted in extremity with DVT
dont use over top of open wound or acute cellulitis
2 point vs 4 point
arms or legs 2 limbs constrained
all 4 limbs constrained
restraints
- cloth
- leather
- 2 point
- 4 point
- mitt
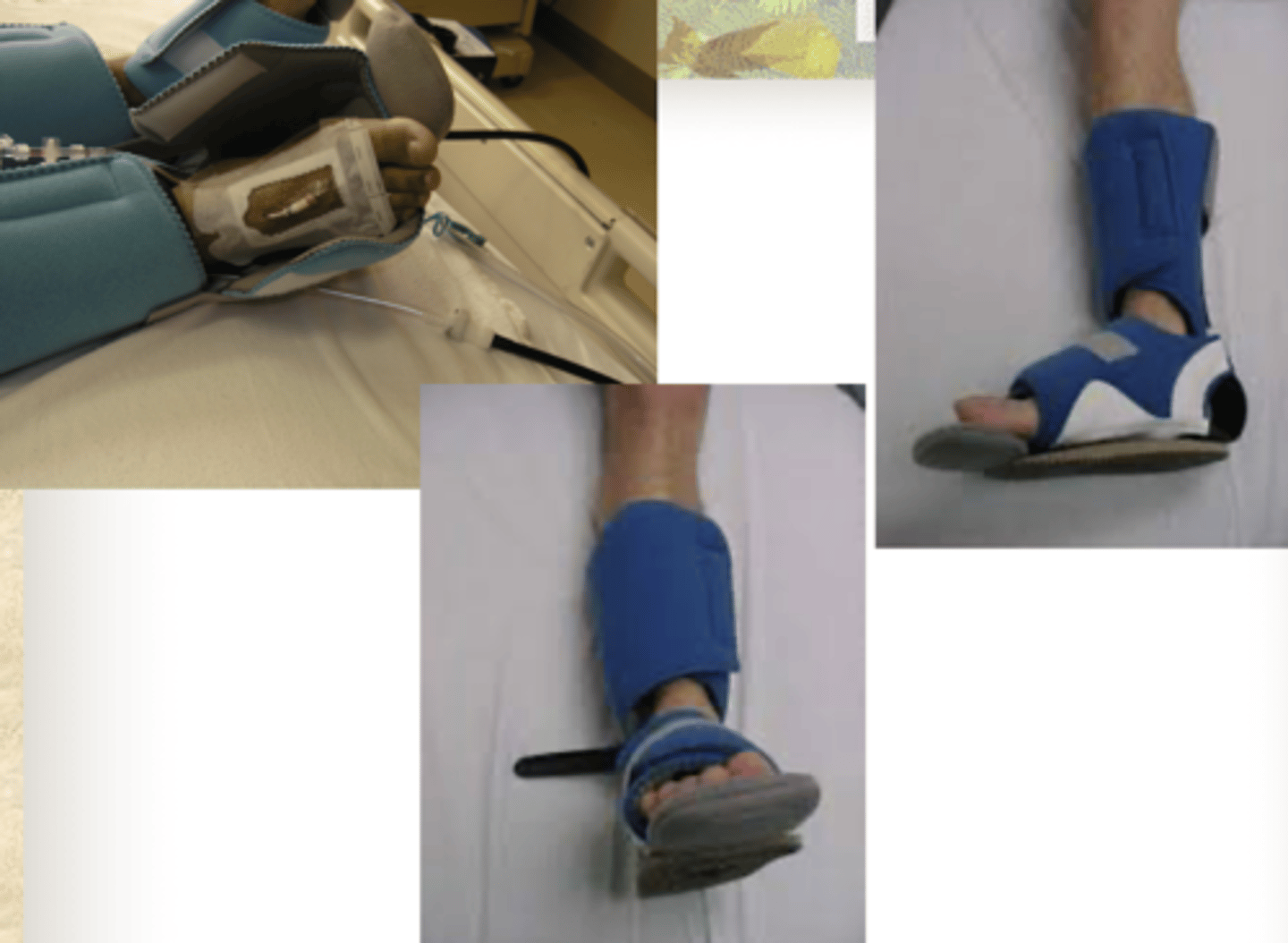
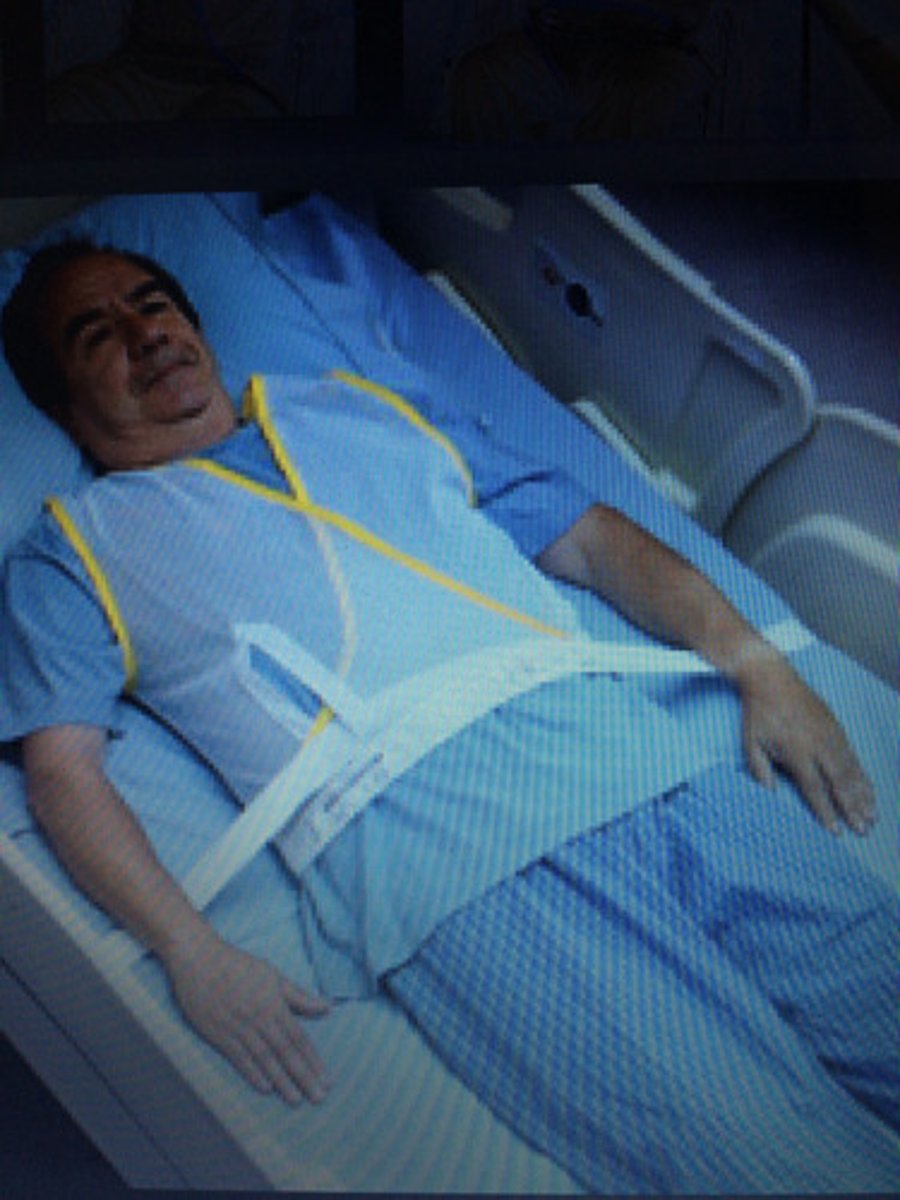
posey vests
L'nard boots