PPO III: Intro to posterior Segment
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Structures of the posterior segment
Vitreous
Optic nerve
Macula
Vasculature
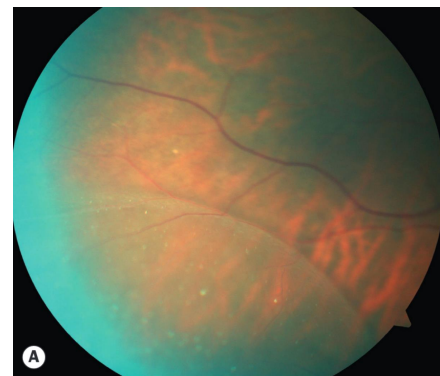
Periphery
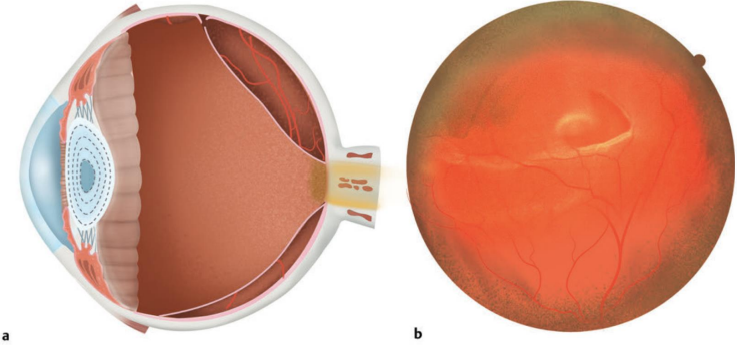
En-face
Refers to the view that fundus photos get of the retina
Anatomically accurate as if the eye is pointed at you
Functions of the vitreous
80% of total globe volume
Stabilizer
Shock absorber
Light transmitter
Buffering zone for metabolic waste
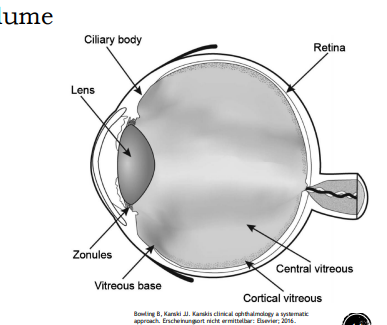
Categories of vitreous
Cortical vitreous
Peripheral shell of vitreous
Densely packed collagen fibrils
Thicker anterior > posterior
Central vitreous
Loosely packed collagen fibrils
Strength of vitreous attachments within the globe
Vitreous Base (strongest) > Posterior lens > Optic Disc > Macula > Retinal Vessels (weakest)
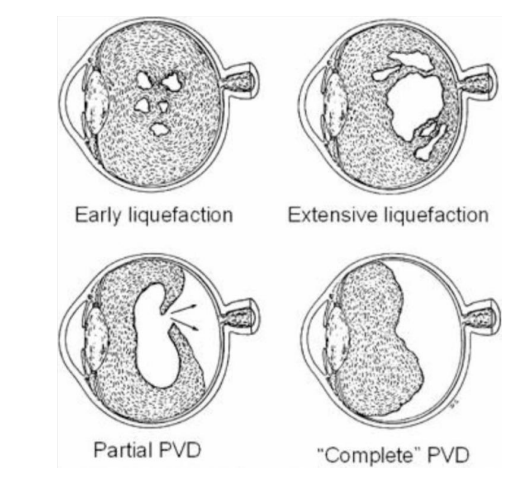
Syneresis
Liquefaction of the vitreous
Begins centrally
Increases with age & axial length
Posterior vitreous detachment
Detachment of the vitreous from the retina
Occurs in over 60% over 80 years old
Flashes and floaters (Photopsia)
Not painful
PVD leads to complications in 27% of pts
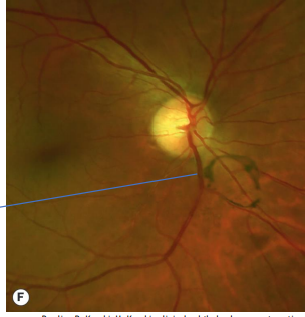
Weiss ring
Circular floater of condensed vitreous
Previously attached to the ONH
Retinal tear
Can occur as the vitreous detaches from the retina
Strong adhesions rip the retina off the RPE
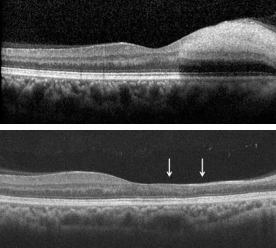
Macular hole
During a PVD strong adhesions may remain on the fovea
As the vitreous pulls away, this pulls the macula from the RPE
→ Central scotoma

Epiretinal membrane
As PVD progresses, cortical vitreous remnants secrete collagen
→ Sheet of glial cells develops
→ Epiretinal membrane
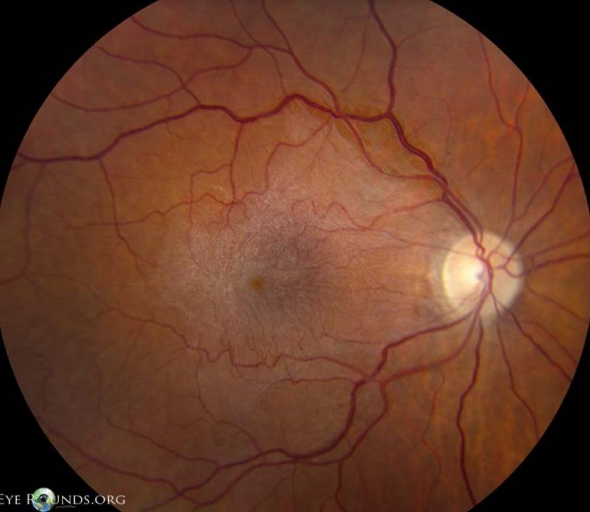
Epiretinal membrane
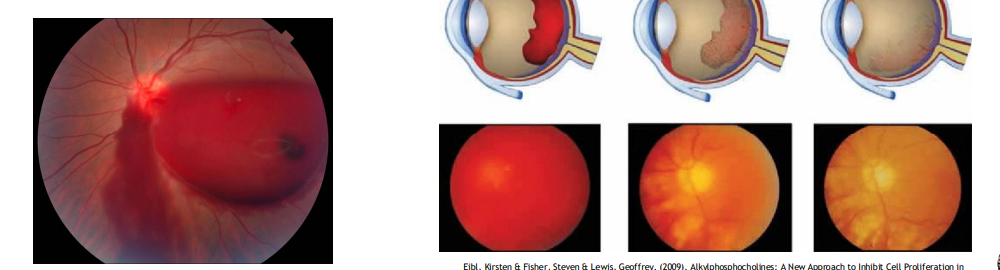
Vitreous hemorrhage
PVD → Tears blood vessel → Vitreous hemorrhage
Traumatic
Associated with retinal tears
Vitritis
Inflammatory cells within the vitreous
Associated with systemic diseases that are
Infesctious
Inflammatory
Autoimmune
Diseases associated with vitritis
Tuberculosis
Sarcoidosis
Multiple Sclerosis
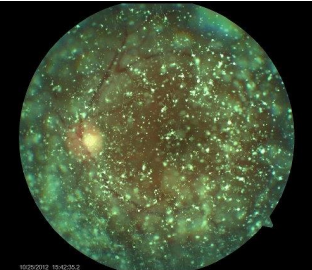
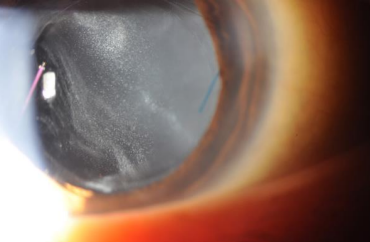
Asteroid Hyalosis
Calcium-lipid deposits within the vitreous collagen
Benign finding
How many ganglion cell axons pass through the lamina cribrosa
~1.1 million
Cup / Disk ratio
Compares size of central depression of the ONH (The cup) to the full diameter of the disc
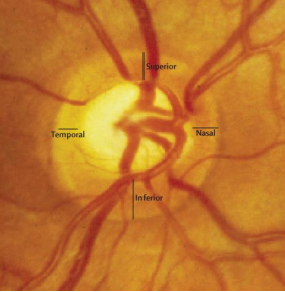
ONH rim tissue is usually thickest…
Inferior > Superior > Nasal > Temporal
ISNT rule
Normal recording of the optic nerve
Healthy, pink rim tissue 360
Recording c/d ratio
0.50 V/0.45 H OD
⁃ 0.20 V/0.25 H OS
Glaucoma
Death of ganglion cells in the inner retina and loss of their axons within the optic nerve
Associated with increased intra-ocular pressure
Glaucoma statistics
1/40 adults over 40 have vision loss from glaucoma
8.4 million bilaterally blind
Half of all cases are undiagnosed in developed countries
Open vs. Narrow-angle glaucoma
Open-angle
Optic nerve damage while the anterior angle is open
Narrow-angle
Optic nerve damage from an acute or chronic rise in IOP from narrowed trabeculae
Most common glaucoma
Primary open-angle glaucoma (POAG)
Risk factors for POAG
High IOP
Age
Race
Genetics
Myopia
Smoking
Thin cornea
Work-up requirements for POAG exam
24-2 SITA-Standard
RNFL OCT
Macular OCT with GC analysis
Pachymetry
Gonioscopy
Secondary open-angle glaucoma
Associated with a specific cause for a rise in IOP
Pre-trabecular → Neovascular glaucoma
Trabecular → Pseudo exfoliation, pigmentary glaucoma
Post trabecular → Carotid-cavernous fistula
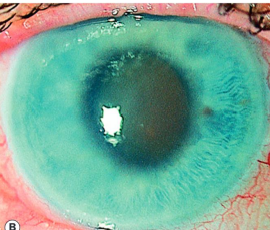
Symptoms of acute angle closure
Intense ocular or peri-ocular pain
Blurry vision, haloes around lights
Nausea, vomiting
Acute angle closure signs
High IOP (50-100 mmHg)
Corneal edema
Mid-dilated pupil
Conjunctival injection
Optic neuritis
Inflammation of the optic nerve
Typically unilateral
Pain on eye movements
Associated with autoimmune conditions
Multiple sclerosis
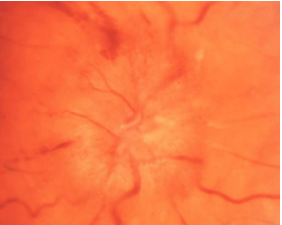
Papilledema
Bilateral swelling due to increased intracranial pressure
Risk: Obese, young females
Headaches
Untreated → Optic atrophy

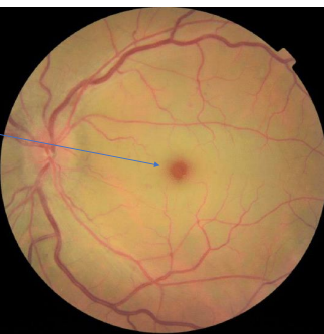
Regions of the macula
Perifovea (Outer) → Parafovea → Fovea → Foveola
Oxidation of the macula
Macula is one of the most metabolically active tissues
Light exposure → Reactive oxygen species (ROS)
Defense: RPE transports ROS from subretinal space → Choroid
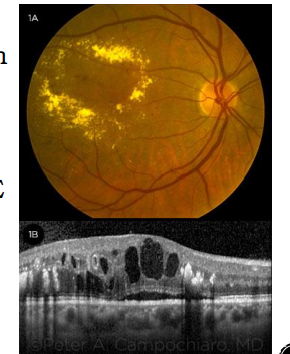
Age-related macular degeneration
Acquired degeneration of the retina that causes central vision impairment
Non-exudative = Dry AMD
Exudative/CNVM = Wet AMD
Choroidal Neovascular Membrane
Statistics about AMD
Leading cause of blindness in the US for pts >60 yrs
8 million pts have early AMD
Risk factors for AMD
Age
Race
Genetics
Smoking
Diet
UV exposure
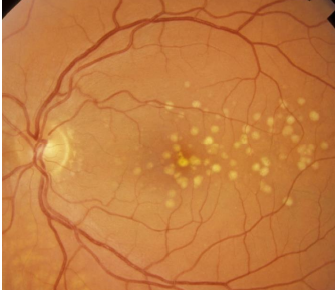
Drusen definition
Hard Vs. Soft drusen
Build up of waste products from visual cycle metabolism
Partially digested photoreceptors
Hard drusen → Small, yellow, discreet margins (Image)
Soft drusen → Large, yellow, nodules with indistinct borders
Geographic atrophy
Late-stage AMD
Loss of photoreceptors and RPE
On the fovea → Permanent, central scotoma
Choroidal neovascular membrane
New vessel growth from choroid → Leaks fluid into the subretinal space
Finding that makes exudative-AMD “wet”
Left untreated → Forms disciform scar
Bullseye Maculopathy
Changes in RPE due to Hydroxychloroquine (Plaquenil)
Irreversible
Risk factors for Plaquenil toxicity
High daily dose
Medication use > 5 years
Concomitant renal or liver disease
Age > 60 years
Screening requirements when bullseye maculopathy is presented
HVF 10-2
Macular OCT
Retinal capillaries supply….
Choricocapillaries supply…
Retinal capillaries supply the inner 2/3rd of the retina
CRA/CRV
Choricocapillaries supply the outer 1/3rd of the retina
Long and short ciliary arteries
Vortex
Retinal vein occlusion associated systemic disorders
Hypertension 66%
Hyperlipidemia 33%
Diabetes 15%
Central retinal vein occlusion
Thrombus formation at the ONH
“Blood and thunder”
Ischemic & non-ischemic form
What type of CRVO causes (+) RAPD
Ischemic
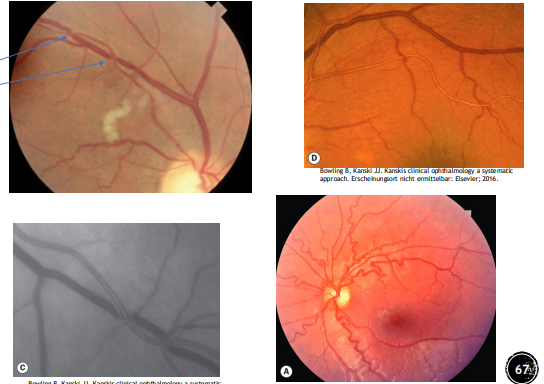
Main mechanism of a BRVO
Thickening/hardening of arterial wall
Compression of vein at crossing point
CRAO is most likely caused by…
Typically from cholesterol embolus
→ Ischemia → Thickening + whitening of the retina → Necrosis
Signs of CRAO
Cherry red spot
90 minutes to unlock → Permanent, irreversible VA loss
Changes in the retina from CRAO
Acute thickening of the inner retina
Thinning of inner retina upon resolution
Microangiopathy
Damage to very small blood vessels
Seen in diabetic retinopathy
Hyperglycemia degrades vessel walls
Inflammation + pericyte damage
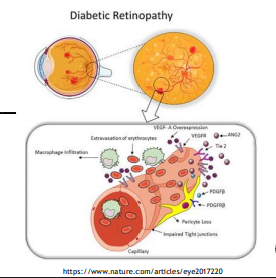
Ischemia of the retina from diabetic retinopathy results in upregulation of…
VEGF
Formation of new leaky blood vessels
Non-proliferative diabetic retinopathy (NPDR) signs
Micro-aneurysm
Dot and blot hemorrhage
Cotton wool spot
Venous beading
Intraretinal microvascular abnormality (IRMA)
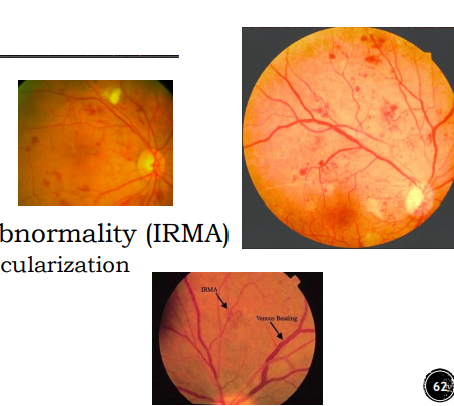
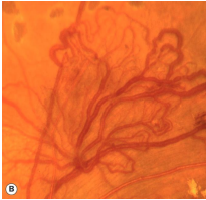
Signs of proliferative diabetic retinopathy (PDR)
PDR → VEGF upregulation → Neovascularization
Neovascularization of the disc (NVD)
Neovascularization elsewhere (NVE)
Neovessles = Fragile, leaky
Increased risk of DME
Main cause of decreased VA from diabetic retinopathy
Macular edema
Occurs at any stage of DMR
Exudates
Circular ring
Signal presence of DME
Clinically significant diabetic macular edema (CSME)
DME defined by ETDRS VA score
Hypertensive retinopathy signs
Arterial attenuation
Copper wiring
AV nicking (Picture)
Venous tortuosity
Optic disc edema
Retinal landmarks anterior to the equator
Ora serrata
Vortex veins
Long + Short posterior ciliary nerves
Floaters
Subjective perception of an opacity
Dark/Translucent
1-2 is normal, many new floaters is concerning
Flashes
AKA photopsia
Subjective perception of a burst of illumaince
Occurs due to traction on the retina
Concerning symptom
Lattice degeneration
Focal patch of inner retinal thinning
Vitreous attached at the periphery
Vitreous liquified over the lesion
Present in 8% of patients
Most common lesion associated with retinal detachment
Lattice Degeneration
40% of retinal detachments
Associated with retinal holes
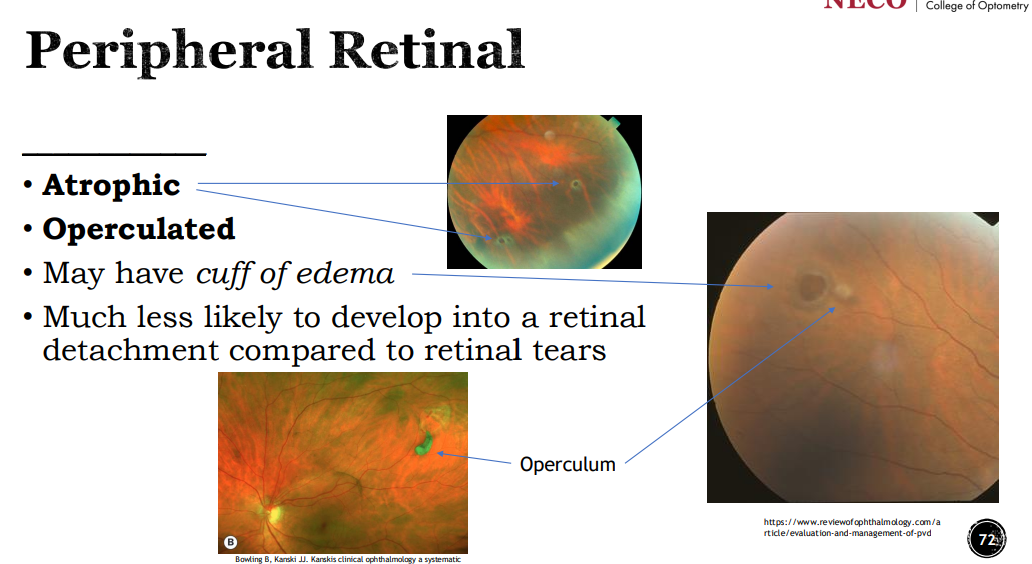
Retinal holes
Atrophic (thinning)
Operculated (Tractional)
May have a cuff of edema
Less likely to lead to attachment (Compared to retinal tears)
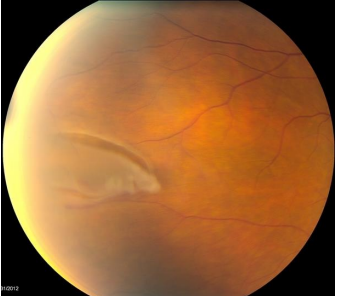
Horseshoe tear
AKA flap tear
Apex attached to the vitreous
Base attached to the retina
Most common lesion leading to Rhegomatogenous retinal deatchment
Definition of retinal detachment (RD)
2 types
Detachment of the sensory retina from the RPE
Mac-on → Fovea still attached
Treat immediately
Mac-off → Fovea detached from RPE
Treated urgently (Within the week)
Damage already done
Retinochiasis
Splitting the retina at the outer plexiform layer
Causes an absolute visual field defect
Most common inferior + temporal