BASIC PRINCIPLES OF MUSCULOSKELETAL PHYSIOTHERAPY
1/48
Earn XP
Description and Tags
Lectures 1-5
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Stages of healing: INITIAL TRAUMA
tensile strength of soft tissue following injury
tensile strength = max stress a material can withstand before breaking
Initial injury:
Immediate drop in tensile strength
Primary damage to myofibrils, fascia and blood vessels
Local bleeding (vasoconstriction follows quickly)
Inflammatory response (swelling and anoxia)
Secondary tissue swelling → goal of physio = limit further healing
healing ability and time frame depends on age, vascularity of tissue, intensity of exercise, fitness, general health
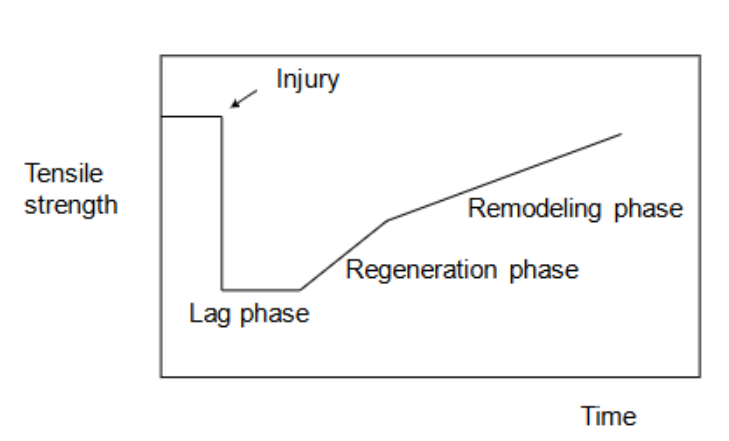
Stages of healing: INFLAMMATORY PHASE
1-4 days until phase complete
Lag, acute or granulation phase
AIMS:
seal wound
phagocytosis
initiate fibroblastic activity
neurovascularisation
establish fibrin network
Events:
Inflammatory cells enter site (ia torn b.v.) → clean up wound
Bleeding stimulates release of leucocytes + macrophages
histamine released → vasodilation
bradykinins → increase vascular permeability
prostaglandins -. prolong vasodilation
SWELLING
Chronic inflammation
Repeated trauma
Persistent irritation by chemical irritants
Prolonged swelling
Inadequate/inappropriate physiological response
Increase tensile force to quickl
Stages of healing: Fibroblastic/ proliferation phase
starts at 3-5 days → lasts 2-12 weeks
AIMS:
Epitheliasation
Wound contraction
Collagen Production
Process:
Collagen production (stimulated by fibroblasts)
More collagen = stronger scar. Collagen III laid down first followed by collagen I which is stronger.
Intermolecular bonds responsible for scar strength
GAG lubricates and fills space
FIbroblastic / Proliferation stage: Immobilisation vs. mobilisation
Effects of immobilisation on healing:
longer immobilisation = bigger scar
Mobilisation is the mechanical stress needed to adhere the regenerating ends of the muscle to the lateral extracellular matrix
Stages of healing: REMODELING PHASE
starts day 21 → 6-12 months
AIMS:
strengthen scar w/o increasing inflammation
restore normal strength, endurance + coordination
Process only starts when lysis = synthesis
Inflammation → collagenase → increases lysis
collagen contracts to bring regenerating ends of muscle tg
Phase complete = when functional scar formed
scar must be: right length, non-adherent to other tissue, in line with healthy tissue, able to withstand force
Clinical implications of healing phases
INFLAMMATORY PHASE
Initially:
reduce impact of injury/ from site of injury (e.g. field)
immobilisation/support → crutches or brace
Protect injury site: fibrin network
Avoid anti-inflammatories
Ultra sound disintegrates macrophages (non thermal)
Reduce swelling (Peace and Love)
No deep soft tissue work
FIBROBLASTIC/ PROLIFERATION PHASE
movement + tension to optimize strength + reorganisation of tissue
motility exercises + stability & strengthening programs
SSTM
REMODELING PHASE
add load + ensure length for optimal function
tension increased, strengthening programs increased, heating

SUBJECTIVE INTERVIEW
Goals of subjective exam
to determine:
level of functioning (ICF)
source of symptoms
pathobiological mechanisms (stage of healing/ type of disorder)
precautions and contraindications
predisposing/contributing factors
insight about management
1st session with patient overview
introduction (welcome and inform)
interview
physical exam
preliminary treatment and reassessment
reflection
Subjective examination
5 parts:
main problem (kind of disorder)
includes: pain, stiffness, sensation of instability, weakness, loss of function
body chart
diagram/reference depicting areas of pain
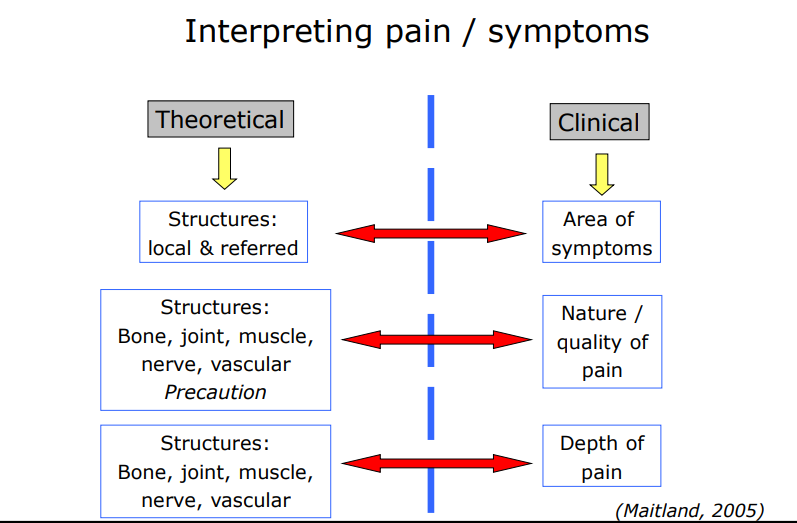
What to note:
area of symptoms
nature/quality of pain
depth of pain
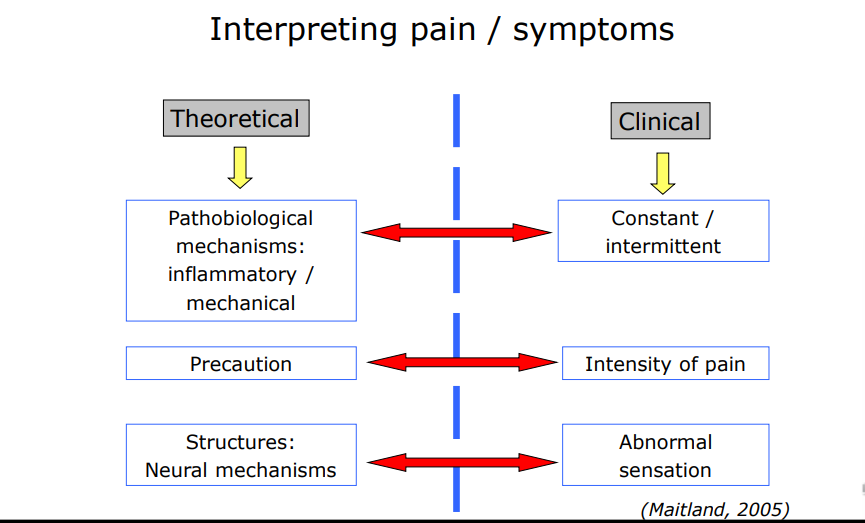
severity/intensity of pain ?/10
constant/intermittent
abnormal sensation
relationship of symptoms/areas
clear unaffected areas with a tick
behaviour of symptoms
history
special questions
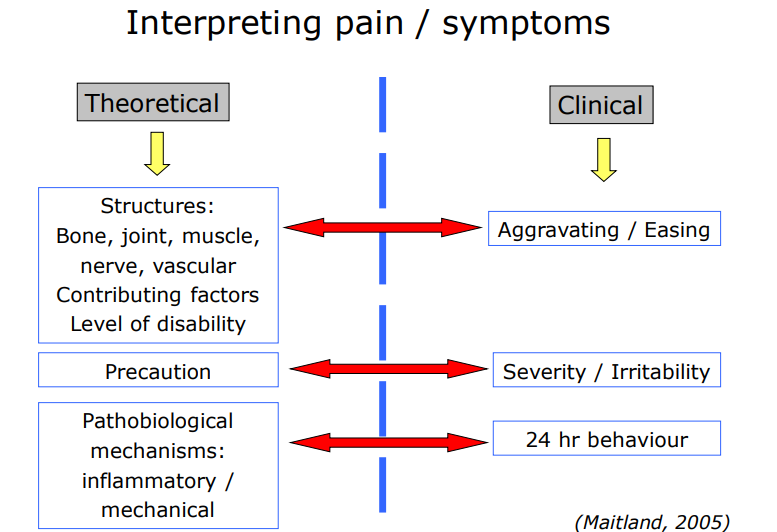
Interpreting pain/symptoms 1
Interpreting pain/ symptoms 2
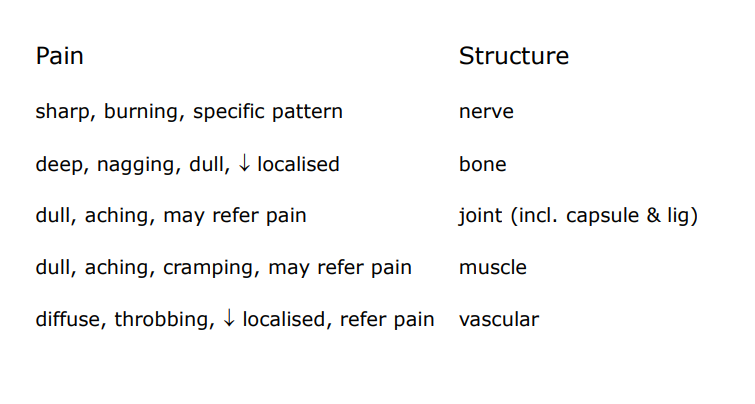
Nature/ quality of symptoms and correlation to body structures
Abnormal sensation
anaesthesia (no sensation)
paraeathesia (abnormal sensation (“pins & needles”)
hypoaesthesia / hyperaesthesia (decreased / increased sensation to touch)
analgesia (no sensation of pain)
hypoalgesia / hyperalgesia (decreased / increased sensation of pain)
allodynia (pain due to a stimulus that does not normally provoke pain)
Summary of body chart
Area pain – structure
Nature of Pain- structure
VAS ( intensity of pain)
Superficial or deep – structure
Constant versus Intermittent – Inflammatory versus Mechanical
Abnormal Sensations – structure and pain mechanisms
Relationship between areas
Interpreting pain/symptoms 3
Behaviour of symptoms
the symptoms that the patient feels & their changes in site & intensity need to be related to daily activities & positions, including periods of rest
can indicate:
how the symptoms affect the patient’s daily life
the severity of symptoms
insight into the overall level of disability
precautions & contraindications
treatment objectives
Aggravating + easing factors
Aggravating factors:
what aggravates the pain
quality (slow, fast, rapid, etc.) of movement/ position
quantity (how much/often) of movement/position
can activity/position be continued despite pain
Easing factors:
what/how makes main subside → do symptoms completely subside
how long does it take to ease
can activity/position be resumed once pain subsides
SIN (Severity, Irritability + Nature)
if patient presents 2/3, consider a SIN patient
Severity (VAS):
pain response /10
0-3 = low, 4-7 = medium, 8-10 = high
Irritability:
how quickly patients pain is provoked/ how long it lasts or to subside
degree + quality of increased symptoms
Nature:
how pain is generated (mechanical = movement, inflammatory = constant and worsening, neuropathic = burning/tingling, etc.)
Pattern of pain
Constant vs intermittent
Local vs spreading
Superficial vs deep
24-hour behaviour (including sleep)
Morning symptoms:
pain on waking (instabilities)
pain getting out of bed → eases quickly = mechanical
pain getting out of bed → lasts unusually long (2-3) = inflammatory
ischaemic disorders (caused by reduced blood supply to tissues, leading to pain, dysfunction, and possible tissue damage due to lack of oxygen.) → require repeated movement to relieve symptoms
Evening/ night symptoms:
pain that subsides with rest = mechanical
pain getting into bed = inflammatory
pain that disturbs sleep = inflammatory → may indicate serious pathology
note effects of patients home environment and behaviour
Pain during day
may vary depends on activity
pain diary can be useful → record symptoms over 7 days (useful if symptoms not regular)

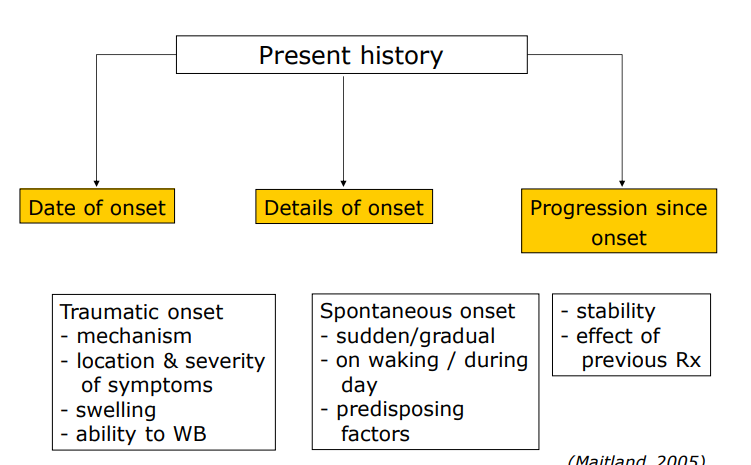
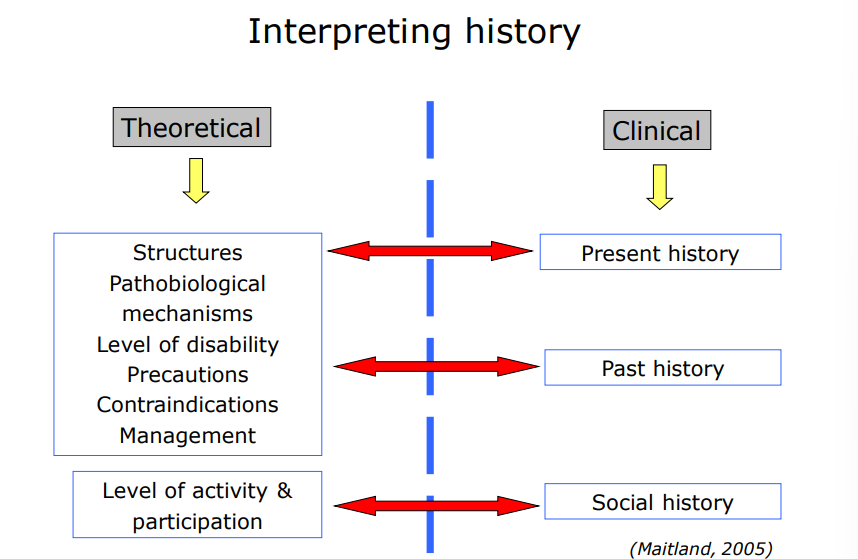
Present history
Previous history
no. of previous episodes
aggravating + easing factors
previous treatment + effectiveness of treatment
current episode compared to previous episodes
changes in frequency of episodes
level of impairment, activity loss between episodes
how pain/level of disability has developed over the years
Social history
get to know your patient
understand activities & participation
interests, hobbies, sport
psychosocial influences
Interpreting history
Contraindications to treatment
significant trauma
severe, unremitting night pain (cant go back to sleep)
unexplained / sudden weight loss or weight gain
malaise / unexplained fatigue / tiredness
fever
night sweats
medication
steroid use
intravenous drug use
cord signs
bilateral pins & needles in hands or feet
gait disturbances
cauda equina syndrome (a medical emergency caused by severe compression of nerve roots at the base of the spinal cord, often due to a massive herniated disc, tumor, or fracture)
saddle anaesthesia/paraesthesia (loss of sensation when in the saddled sitting postion)
loss of anal sphincter tone or faecal incontinence (problems with bladder/bowel)
urinary retention
special investigations
dizziness** → possible suggest involvement with vertebral artery
cardiac symptoms
cancer + malignancy
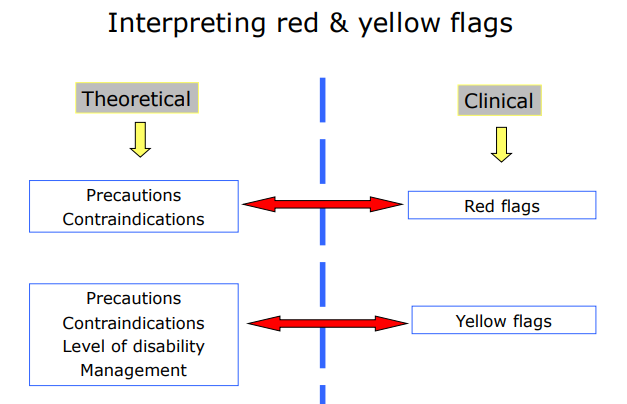
Precautions
SIN
pathobiological processes
stage of healing, tissue mechanisms, pathological processes
stage + stability of disability
patient at risk of developing long term disability die to pain
psychosocial risk factors
How to identify precautions during examination
observe: body language + posture and movements, non verbal expressions
assess: discrepancy between pain + percieved disability, attitude of patient,
ABCDEFW
attitude (pain means harm, must stop before activity, expect pain with work, can’t control it, rehab is passive.)
behaviour (too much rest, less activity, skipping exercise, more substances.)
compensatory issues (money reasons to stay off work (past claims, disability grants, lack of incentive to return).)
diagnostic (doctors reinforce disability, give passive care, conflicting explanations, scary language, and advice to stop work/activities.)
emotion (fear of pain with activity, low mood/loss of joy, anxiety about body sensations, stress/lack of control, feeling useless.)
family (overprotective/solicitous spouse, family discouraging return to activity/work, and lack of supportive person to talk to.)
work (heavy physical demands, rigid schedules, belief work is harmful, no gradual return plan, and employer disinterest.)
Interpreting red and yellow flags
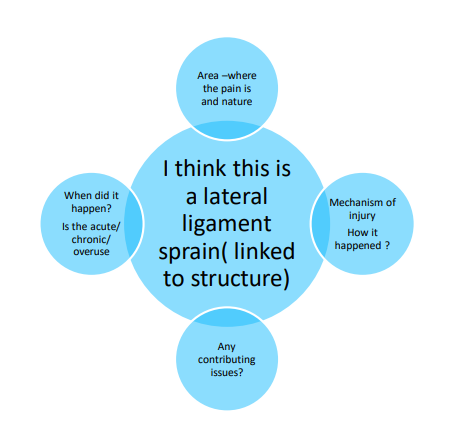
Provisional hypothesis
based on subjective interview, what is wrong with patient??
story you start developing
Planning physical exam
plan sequence
any special tests?
any positions to avoid?
is referral needed/indicated??
OBJECTIVE EXAMINATION
objective examination musts
ensure patient comfort + safety
be comprehensive + standardised
appropriate for patient + patient disorder
Components of objective examination
Observation
functional demonstration of functional tests
Clearing tests of joints above and below
Active movements
Passive Movements
Isometric muscle tests
Special tests- to isolate and test for specific structures and their involvement
Neurological tests ( Conduction and/ or Neurodynamic testing)*
Muscle strength tests*
Flexibility tests ( Muscle length) *
Palpation
Check case records & radiographs
hypothesis planning
treatment planning
Warnings, instructions & recommendations to patient
Observation in objective exam - purpose + structure
Purpose:
obtain info about functional deficits with regards to
posture, alignment, joint positions, local tissues
any unusual pain behaviours noted
Informal observation:
observe way patient moves/posture
get feel for: attitude, willingness, quality of mvmnt + any unusual pain behaviour
Formal observation:
posture (lat., post., ant.) → abnormalities that may/may not contribute to patients symptoms
change in skin (texture, colour, hairloss, swelling), muscle tone/atrophy & body alignment
gait: willingness to walk, pain, compensatory movements→ deformities
Objective exam test procedures
correct posture & starting position
determine symptoms at rest before EACH test
ensure correct movement & accuracy of testing
test unaffected side first; then test affected side
clearly determine patient’s response to test
SPECIFIC
accurate recording & documentation essential
remember - goal is to reproduce patient’s symptoms & to establish comparable sign
Functional demonstration
Patient’s demonstration of movement/function associated with disorder
active mvmnts in WB allows assessment of:
muscle balance
muscle control
neuromuscular function
co-ordination of movement
Clearing/screening tests of other joints
joints (& structures that refer symptoms) above + below symptomatic area to be tested
Active movements - objective assessment
assess contractile + non-contractile structures
determine:
willingness to move
document ROM + limiting factors (LF)
pattern of mvmnt
indicate pain response (VAS)
co-ordination of mvmnt
reproduction of symptoms
principle of overpressure (an active movement cannot be classified as normal unless unless relatively firm overpressure can be applied painlessly)
Passive movements - objective assessment
assesses non-contractile structures + stretch contractile structures
determine:
pain amount, resistance + spasm thru ROM
end feel (w/ overpressure)
document ROM, LF, end feel, pain response
physiological & accessory movements
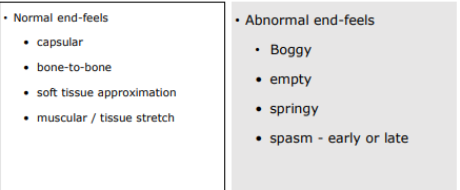
Passive movement end feels
Passive movements - capsular & non-capsular patterns
Capsular patterns:
Definition: Predictable decrease in passive movement around a joint.
Indicates: Lesion of the capsule or synovial membrane (common in arthritis).
Features:
Restriction in multiple directions, each to varying degrees.
Each joint has a typical pattern of limitation (useful for diagnosis).
listen in descending order of limitation
Causes: Degeneration, inflammation, trauma.
Non-capsular patterns:
Definition: Restriction of passive movement not following a predictable capsular pattern.
Indicates: Lesion in extra-articular structures (ligaments, tendons, fascia, muscles).
Features:
Decreased ROM in a single movement.
Or restriction that does not match the capsular pattern.
Cause: Obstruction or limitation from surrounding soft tissues rather than the joint capsule itself.
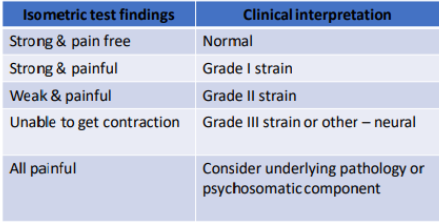
Isometric tests
assess contractile structures
indicates muscle weakness + pain
document muscle weakness + pain response
isometric testing does NOT allow for grading of muscle strength
Neurological tests - integrity, neurodynamic, other
Nerve conduction (integrity)tests
muscle tests (myotomes)
sensation (dermatomes)
reflexes
Neurodynamic tests
assesses mechano-sensitivity of nerves
Other neurological tests
CNS (babinski, etc.)
Special tests
stress or instability tests to isolate structures (Ligaments)
Also specific tests for menisci, capsular structures etc
Can include
palpation of vascular pulses
compression during active or passive tests - to determine the presence of intra-articular pathology
cardiorespiratory tests
Muscle tests
Concentric + eccentric tests (strength)
muscle control
muscle length (flexibility)
muscle bulk
isokinetic testing
Palpation
provides info about:
temp, swelling
sweating
muscle tone
bony abnormalities or misalignments
soft tissue thickening, tightness
End of objective interview
reflect on findings of objective examination
explain findings of the subjective & objective examination to the patient
give a brief outline of management plan, including some preliminary goal setting
warn the patient of a possible exacerbation of symptoms within 24-48 hours after the initial session
ask patient to monitor behaviour of symptoms
Must have a comparable sign *– i.e. an objective measure that reproduces the patients symptoms and which you can use to monitor effectiveness of treatment
Hypothesis – based on findings which confirms one of your provisional hypothesis and identifies:
structure/s involved in symptom development; stage of disorder and patho-mechanics
cause and contributing factors
Developing hypothesis from exam
sources of symptoms
precautions + contraindications
contributing factors (intrinsic + extrinsic)
level of disability
management (treatments/interventions)
prognosis