Quiz 5 RBC Disorders, Upper GI, Lower GI
1/174
Earn XP
Description and Tags
N220 Pathophysiology Spring 26 Week 9, 10, 11
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
175 Terms
What is the purpose of a Complete Blood Count (CBC)?
Use the values to assess and identify any abnormalities
Blood Cells Quantity (RBCs, WBCs, PLTs)
Oxygen Carrying Capacity
RBC Morphology
Blood Disorders
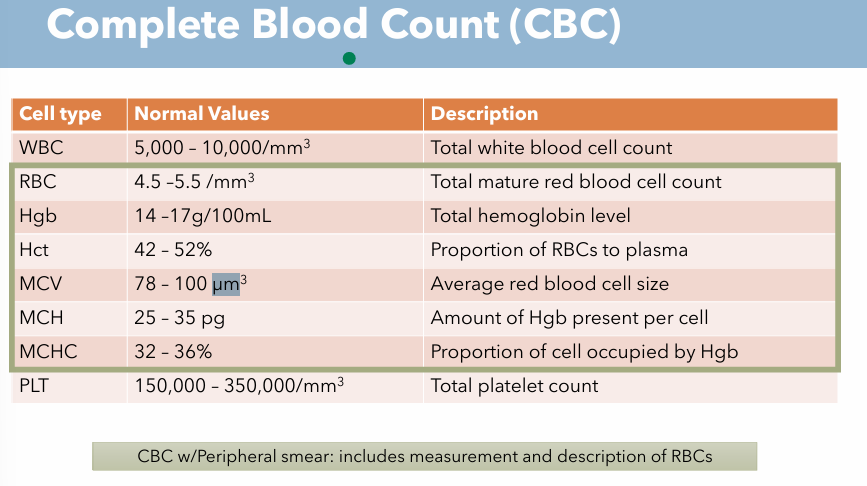
What are the 4 main values of CBC? What are normal values of each one?
WBC (white blood cells
RBC (red blood cells)
Hgb (hemoglobin)
Hct (hematocrit)
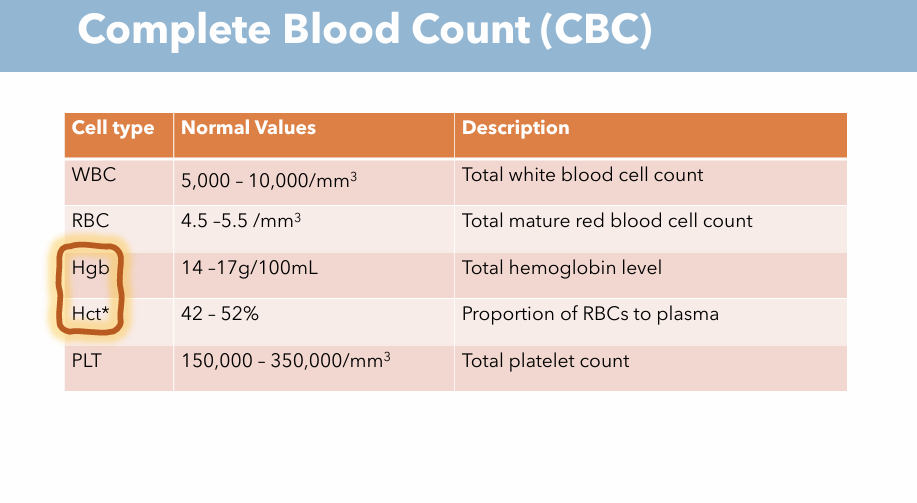
What are the 4 main values of CBC? Description & What are normal values of each one? (WBC)
Description: Total white blood cell count
Normal Value: 5,000 - 10,000 / mm³
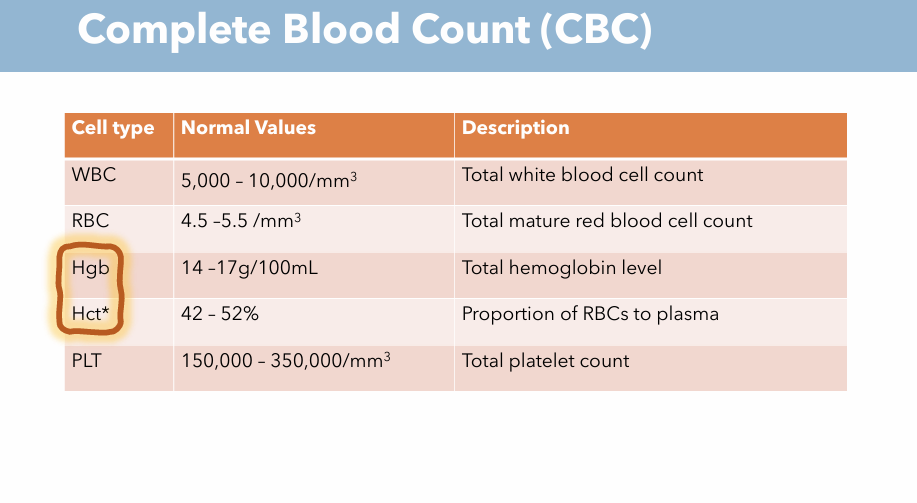
What are the 4 main values of CBC? Description & What are normal values of each one? (RBC)
Description: Total Mature Red Blood Cell Count
Normal Value: 4.5 - 5.5 / mm³
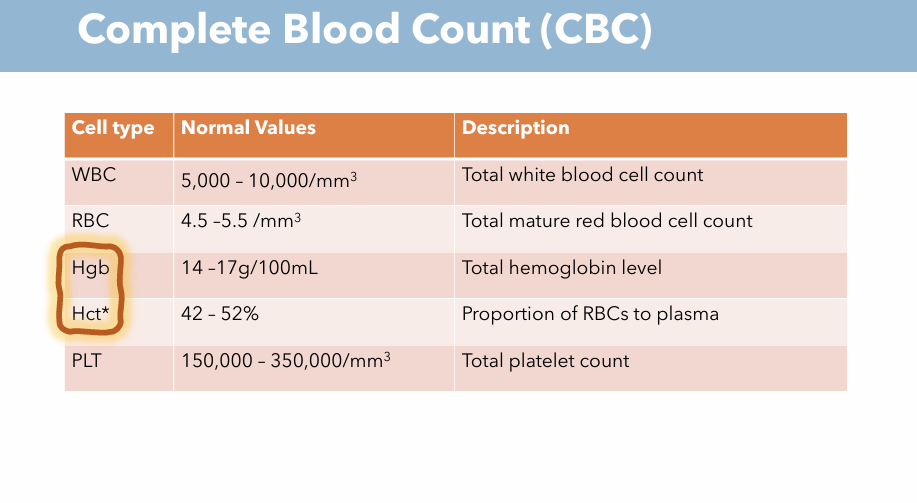
What are the 4 main values of CBC? Description & What are normal values of each one? (Hgb)
Description: Total hemoglobin level
Normal value: 14-17 g/100 mL
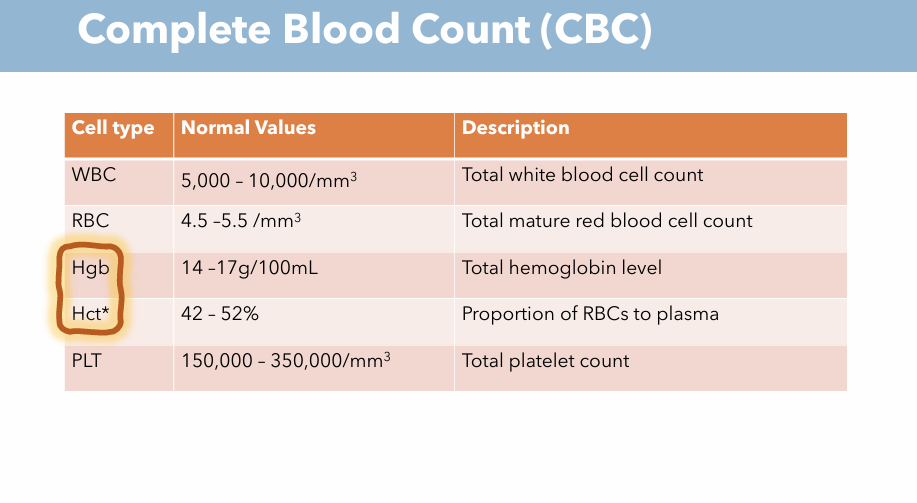
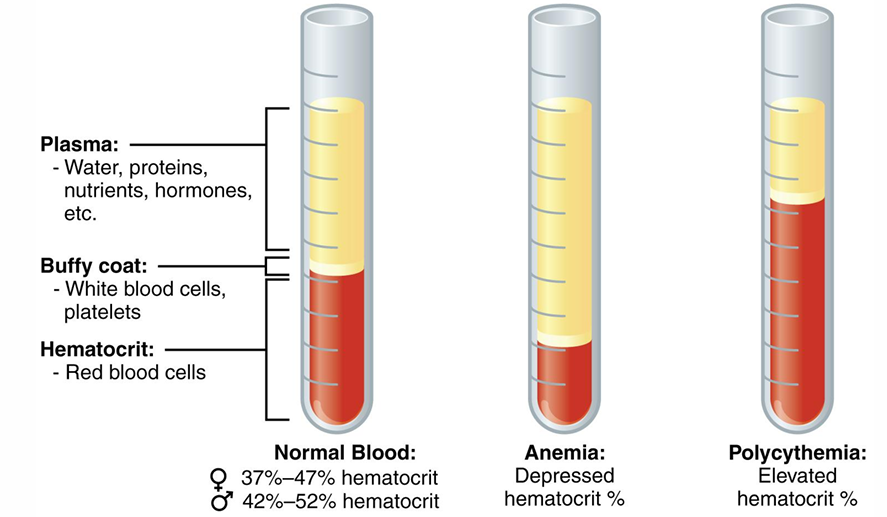
What are the 4 main values of CBC? Description & What are normal values of each one? (Hct) What is abnormal Hct?
Description: Proportion of RBCs to plasma
Normal value: 42 - 52%
Anemia: Depressed hematocrit %
Polycythemia: Elevated hematocrit %
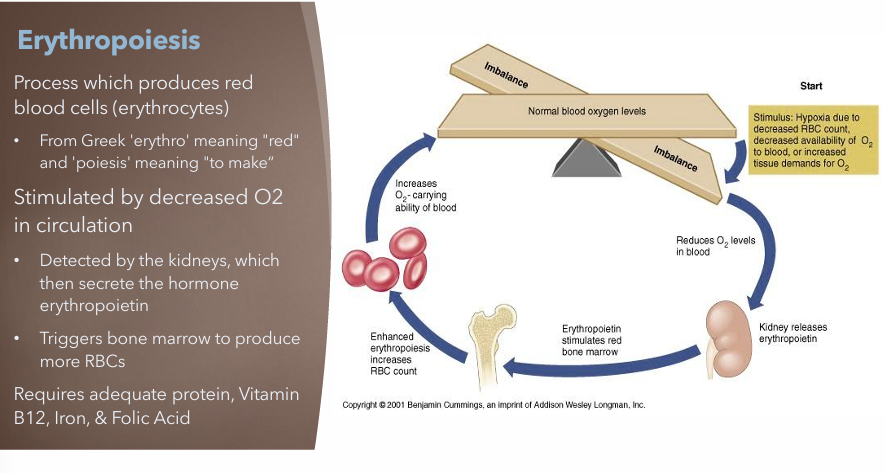
Explain Erythropoiesis & how red blood cells (RBCs) are monitored?
Process which produces red blood cells (erythrocytes) and monitored by the Complete Blood Count (CBC)
Define Anemia and how does it affect the tissues?
Deficit of mature, healthy RBCs in circulation
Insufficient delivery of O2 to the tissues
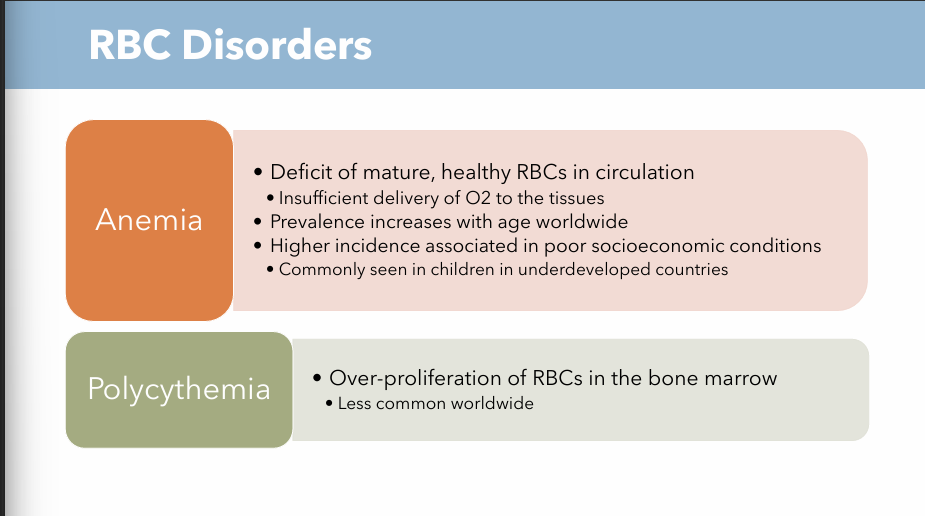
Define Polycythemia
Over-proliferation of RBCs in the bone marrow
What is hematopoiesis? What are the two stages?
Hemostatic process
Bone marrow stem cells → Differentiate blood cells
Two stages: Proliferation & Maturation
Proliferation: “-poietin” → suffix for growth or multiplication of specific cell types
Maturation: Bone marrow stem cells mature to WBCs, RBCs, PLTs
What is purpose of RBCs
Most numerous cell type in circulation: Transporters
Deliver O2 to tissues via hemoglobin chains
Remove CO2 from tissues for release via lungs
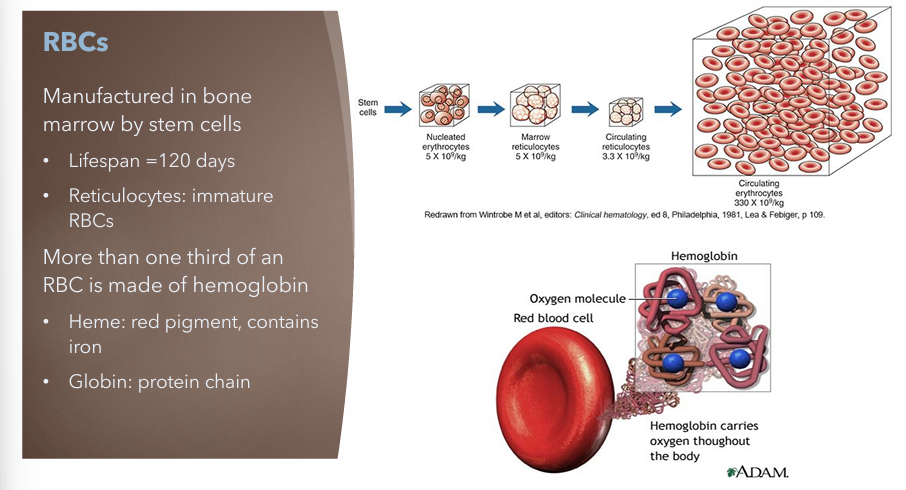
Where are RBCs made, lifespan, and what’s it made of
Manufactured in bone marrow by stem cells
Lifespan = 120 days
Reticulocytes: Immature RBCs
More than one third of an RBC is made of hemoglobin
Heme: red pigment, contains iron
Globin: protein chain
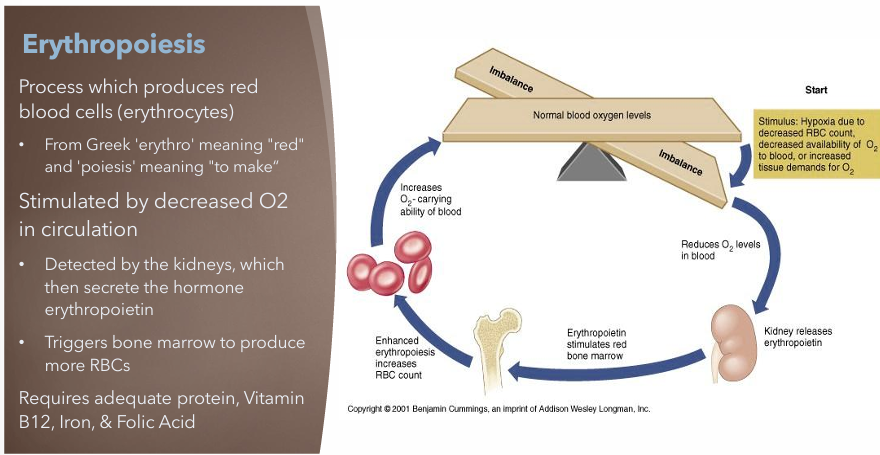
What is Erythropoiesis? What is it stimulated by? What adequate nutrition does it need?
Process which produces red blood cells (erythrocytes)
Stimulated by decreased O2 in circulation
Detected by the kidneys which then secrete the hormone erythropoietin
Triggers bone marrow to produce more RBCs
Requires adequate
Protein
Vitamin B12
Iron
Folic Acid
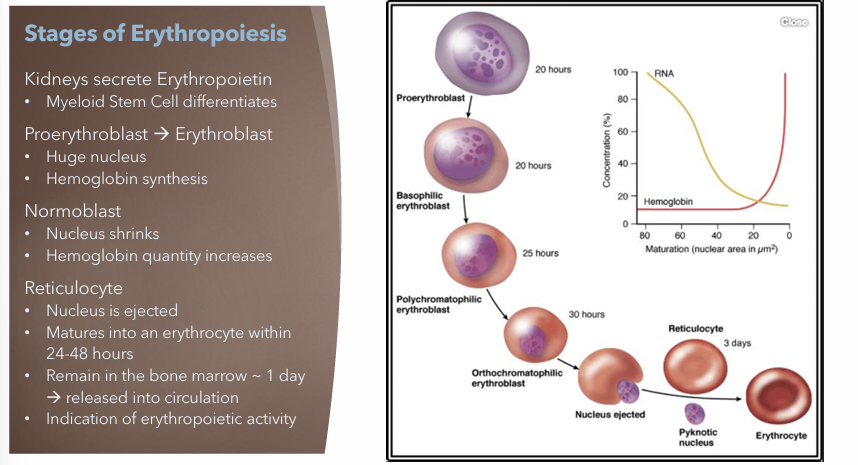
What are stages of Erythropoiesis?
Kidneys secrete Erythropoietin
Bone marrow stem cell → myeloid stem cell
Proerythroblast → Erythroblast
Huge nucleus
Hemoglobin synthesis begins this phase
Normoblast
Nucleus shrinks
Hemoglobin quantity increases
Reticulocyte
Nucleus ejected
Erythrocyte within 24 - 48 hours
Remain in bone marrow ~ 1 day → released into circulation
Reticulocytes are indication of erythropoietic activity
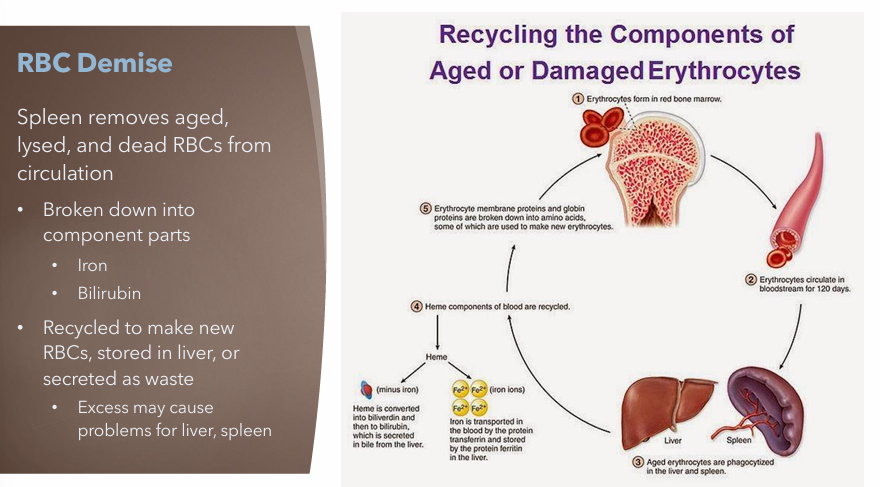
What organ recycles aged, lysed and dead RBCs? What is it broken down into? Where is it stored?
Spleen
Broken down into component parts
Iron
Bilirubin
Recycled to make new RBCs, stored in liver or secreted as waste
May cause problems for liver, spleen
Complete Blood Count; Description & Normal Value for MCV
Description: Average red blood cell size
Normal Value: 78 - 100 µm³
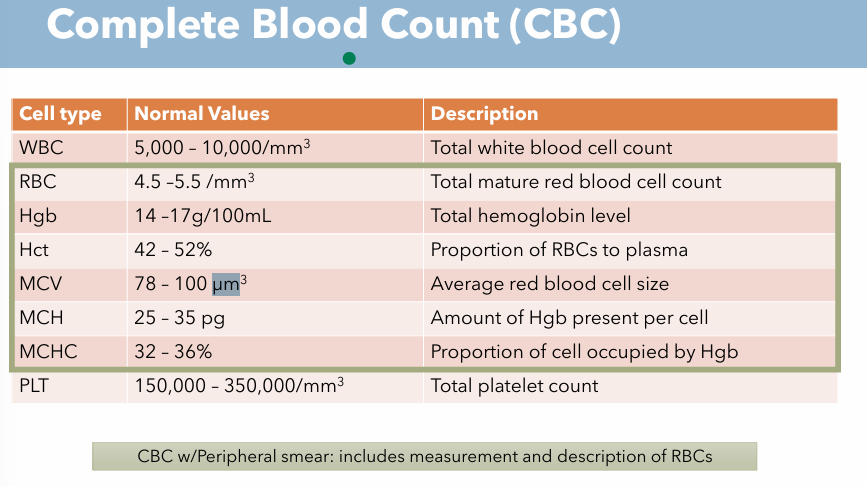
Complete Blood Count; Description & Normal Value for MCH
Description: Amount of Hgb present per cell
Normal value: 25 - 35 pg
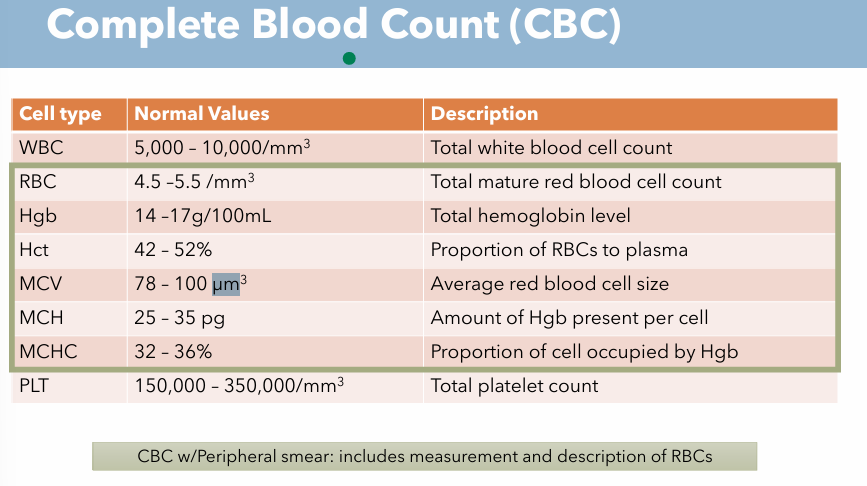
Complete Blood Count; Description & Normal Value for MCHC
Description: Proportion of cell occupied by Hgb
Normal value: 32 - 36 %
What is RBC morphology? What are the different categories?
Categorized RBC based on appearance on peripheral blood smear
Normocytic
Normochromic
Microcytic
Hypochromic
Megaloblastic
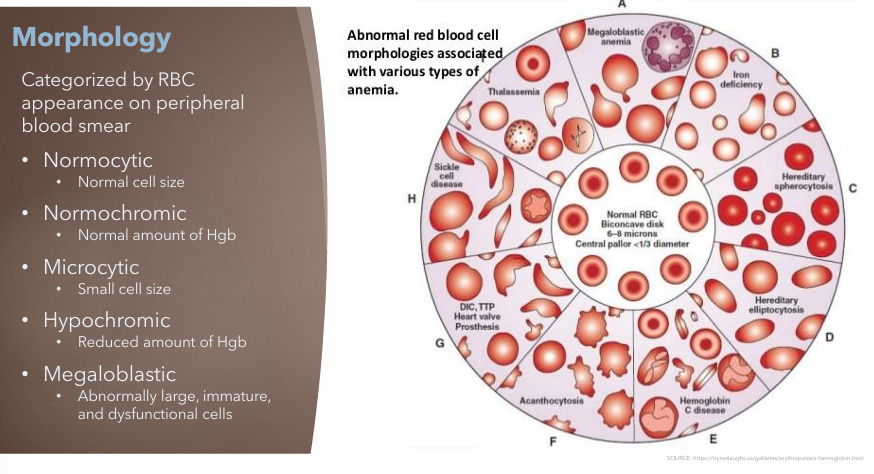
Normocytic
Normal cell size
Normochromic
Normal amount of Hgb
Microcytic
Small cell size
Hypochromic
Reduced amount of Hgb
Megaloblastic
Abnormally large, immature and dysfunctional cells
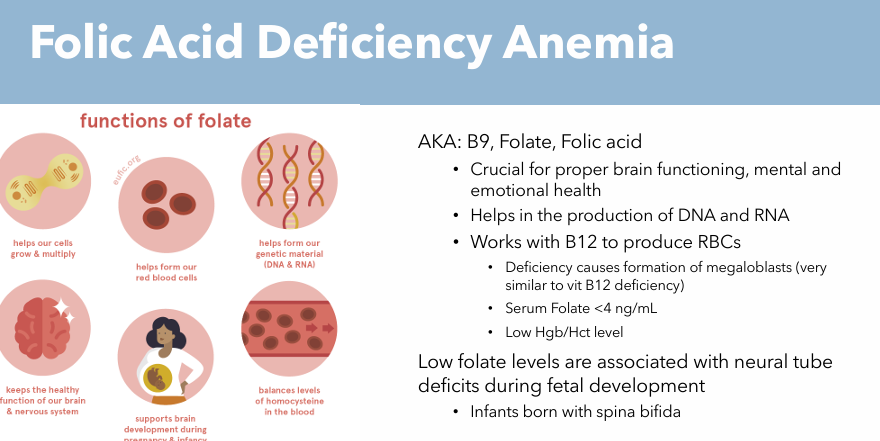
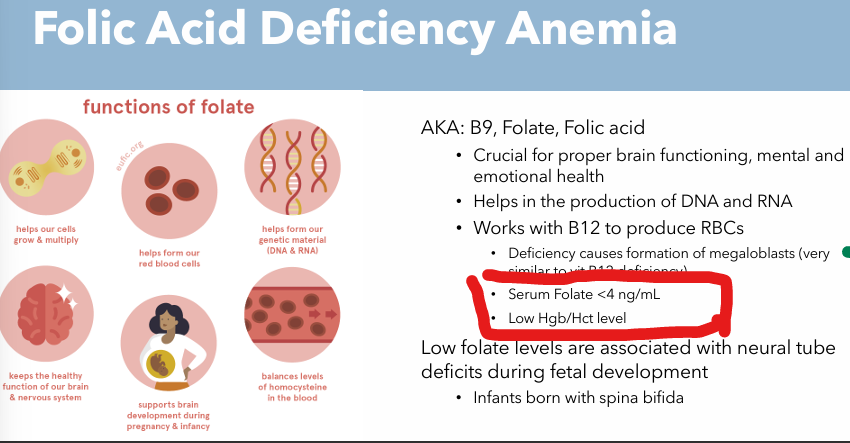
What is Folic Acid (Folate) necessary for?
Necessary for RBC production
What is Vit B12 necessary for?
Necessary for RBC production
What is Iron needed for?
Needed for Hgb production
Review Question: Red blood cells differ from other cell types in the body because they
A. Contain cytoplasmic protein
B. Have no cytoplasmic organelles
C. Have a longer life span
D. Contain glycolytic enzymes
B. Have no cytoplasmic organelles
The primary source of erythropoietin is the
A. Bone marrow
B. Kidney
C. Lung
D. Liver
B. Kidney
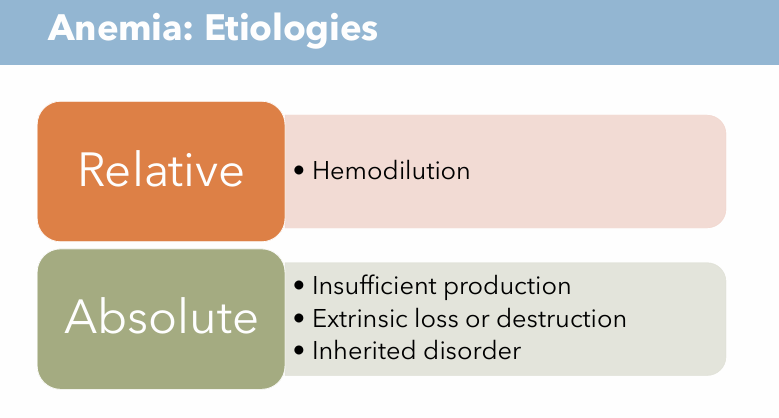
What are the Anemia Etiologies?
Relative Anemia
Hemodilution
concentration of RBCs low because plasma has increased, RBC count is normal, the plasma is just too much that it dilutes
Absolute Anemia
Insufficient production
bone marrow cannot produce enough RBCs to meet needs
Extrinsic loss of destruction
Trauma or surgery; bleeding out; RBCs destroyed faster than produced
Inherited disorder
Genetic mutation; abnormal hemoglobin or misshapen cells
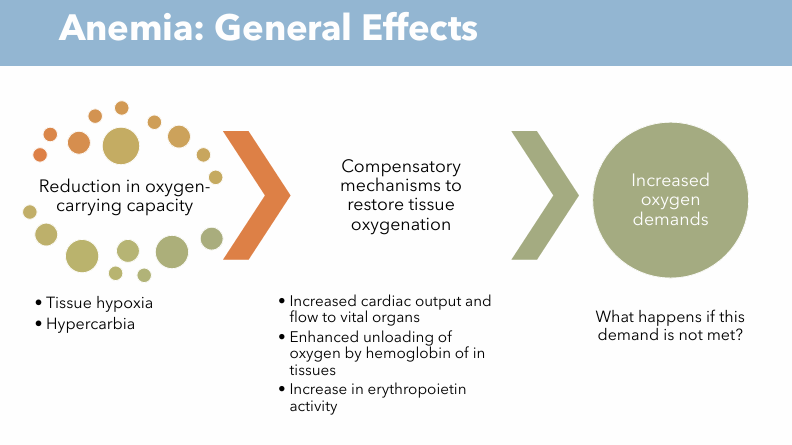
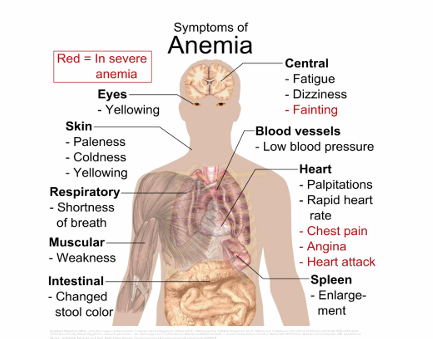
General effects (Clinical Implications) of Anemia
Reduction in oxygen carrying capacity
Tissue hypoxia (tissues don’t get enough oxygen)
Hypercarbia (elevated CO2 levels)
Compensatory mechanisms to restore tissue oxygenation
Increased cardiac output and flow to vital organs
Enhanced unloading of oxygen by hemoglobin in tissues
Increase in erythropoietin activity
Increased Oxygen demands
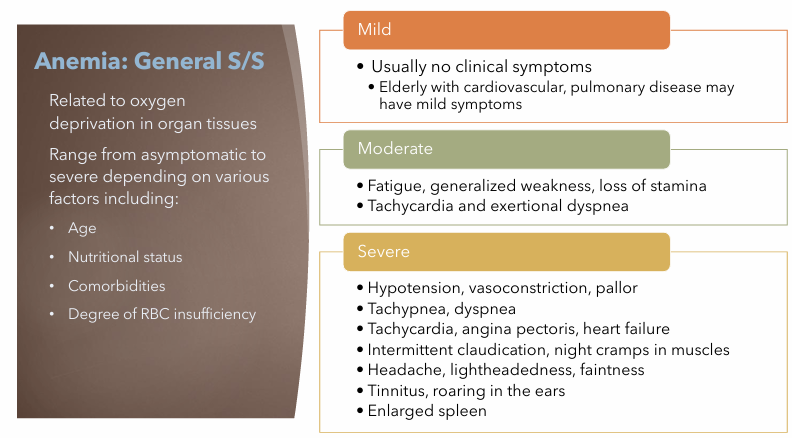
Anemia General S/S; Mild, Moderate, Severe
Mild
Usually no clinical symptoms
Moderate
Fatigue, generalized weakness, loss of stamina
Tachycardia and exertional dyspnea
Severe
Hypotension, vasoconstriction, pallor
Tachypnea, dyspnea
Tachycardia, angina pectoris, heart failure
Intermittent claudication, night cramps in muscles
Headache, lightheadedness, faintness
Tinnitus, roaring in the ears
Enlarged spleen
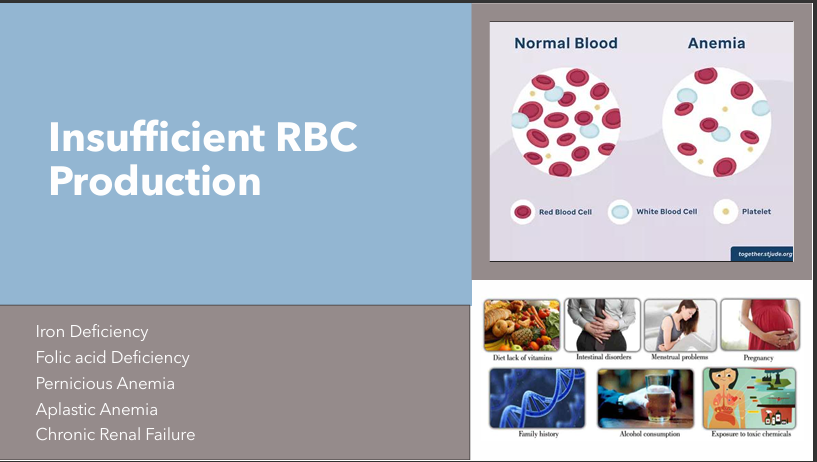
What CONDITIONS cause Insufficient RBC production?
Iron Deficiency Anemia
Folic acid Deficiency
Pernicious Anemia
Aplastic Anemia
Chronic Reneal Failure
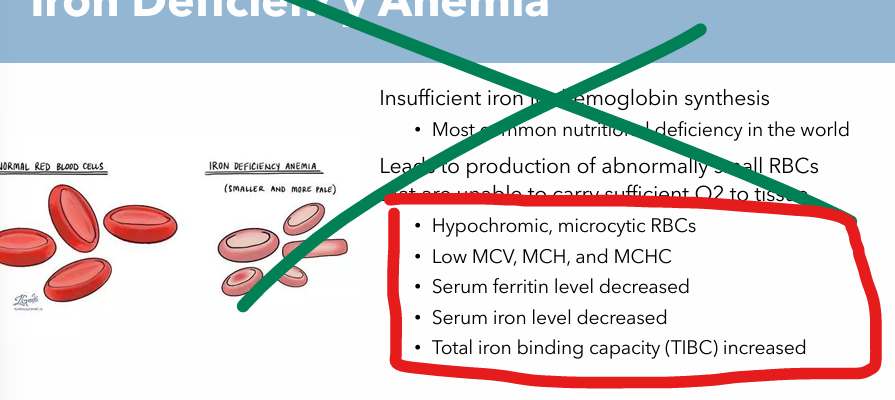
Iron Deficiency Anemia: Etiology
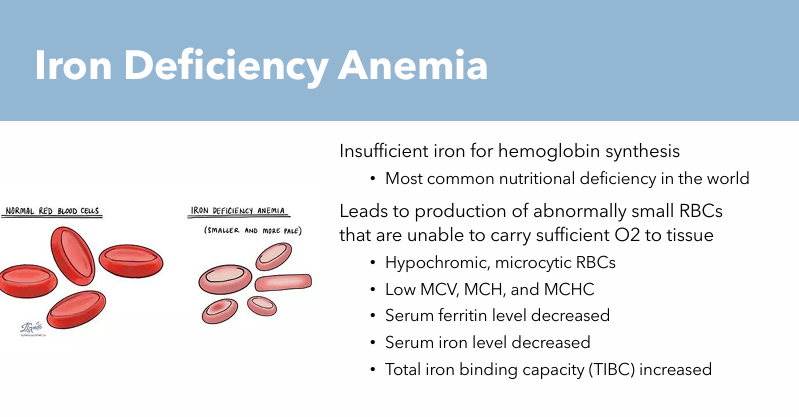
Insufficient iron for hemoglobin synthesis
Abnormally small RBCs unable to carry sufficient O2 to tissues
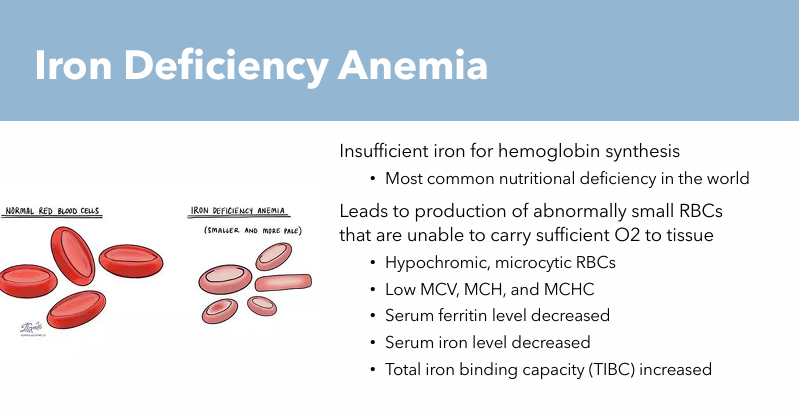
Iron Deficiency Anemia: Pathogenesis
Leads to production of abnormally small RBCs that are unable to carry sufficient O2 to tissue
Hypochromic RBCs
Microcytic RBCs
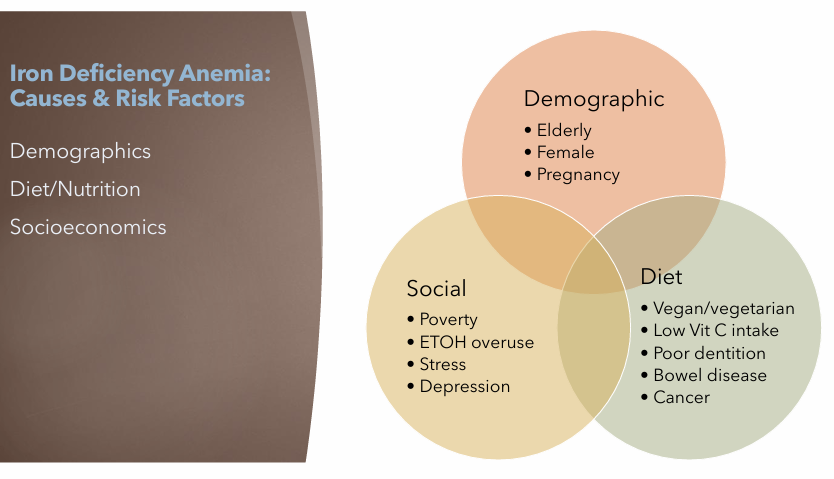
Iron Deficiency Anemia: Risk Factors
Demographic
Elderly
Female
Pregnancy
Diet
Vegan/vegetarian
Low Vit C
Poor dentition
Bowel disease
Cancer
Social
Poverty
ETOH overuse (Alcohol overuse)
Stress
Depression
Iron Deficiency Anemia: Clinical Manifestations
General S/S of Anemia (gradual onset)
PICA (craving nonfood substances)
Dirt, clay, ice, laundry starch, cardboard, hair
Koilonychias (spoon shaped nails)
Blue sclerae (white part of eye appears blue)

Iron Deficiency Anemia: Treatments
Treat underlying cause
Iron (Fe) replacement
Iron supplement tablets
Ferrous Sulfate elixir
Iron Sucrose Injection
Foods that ENHANCE Iron absorption
Citrus fruits
Tomatoes
Chili peppers
Foods that IMPAIR iron Absorption
Tea
Cereal (if it contains phytates)

Iron Deficiency Anemia: Nursing Considerations
Monitor for Fe replacement side effects
Nausea
Black stools
Teeth staining
Pain upon injection and can cause Orthostatic hypotension (IV forms)
Beware of Iron Toxicity
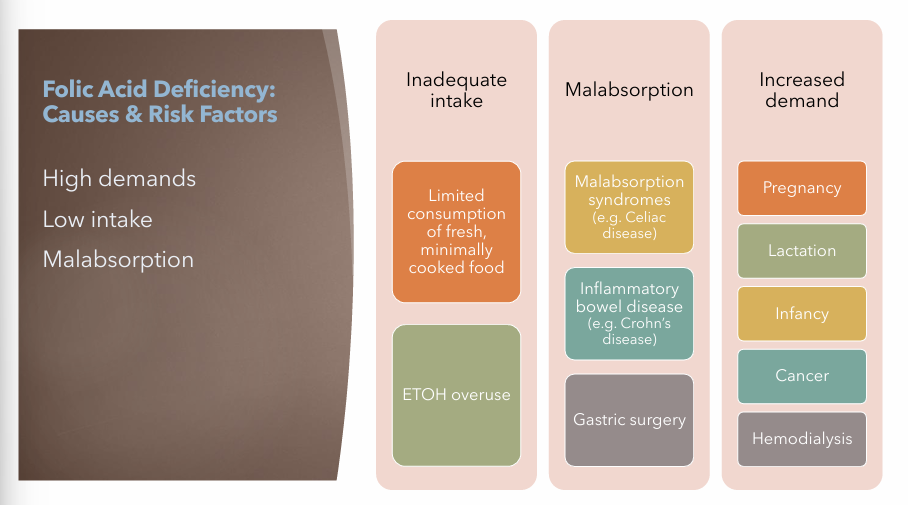
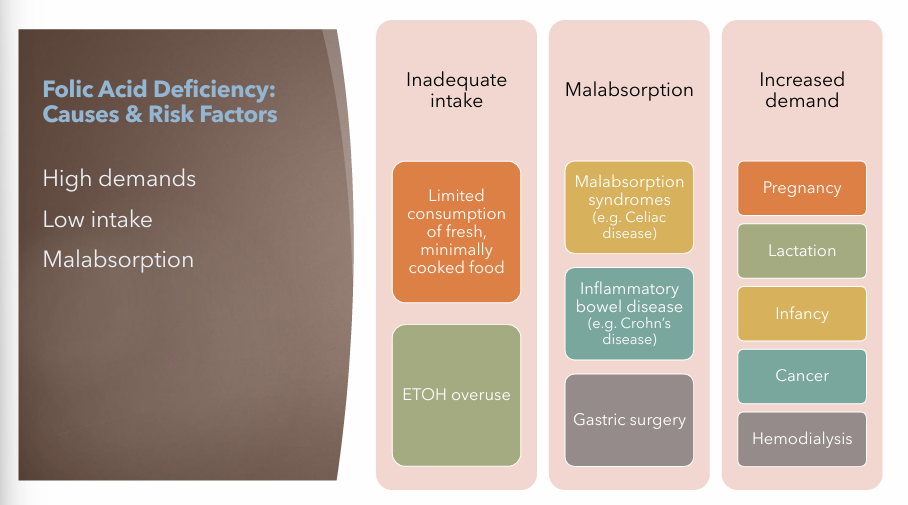
Folic Acid Deficiency Anemia: Etiology
Inadequate Intake
Limited consumption of fresh, minimally cooked food
ETOH (alcohol) overuse
Malabsorption
Malabsorption syndrome (E.g. Celiac Disease)
Inflammatory bowel disease (E.g. Crohn’s Disease)
Gastric Surgery
Increased Demand
Pregnancy
Lactation
Infancy
Cancer
Hemodialysis
Folic Acid Deficiency Anemia: Pathogenesis
Deficiency causes formation of megaloblasts
Very similar to Vit B12 deficiency
Folic Acid Deficiency Anemia: Risk Factors
Inadequate Intake
Limited consumption of fresh, minimally cooked food
ETOH (alcohol) overuse
Malabsorption
Malabsorption syndrome (E.g. Celiac Disease)
Inflammatory bowel disease (E.g. Crohn’s Disease)
Gastric Surgery
Increased Demand
Pregnancy
Lactation
Infancy
Cancer
Hemodialysis
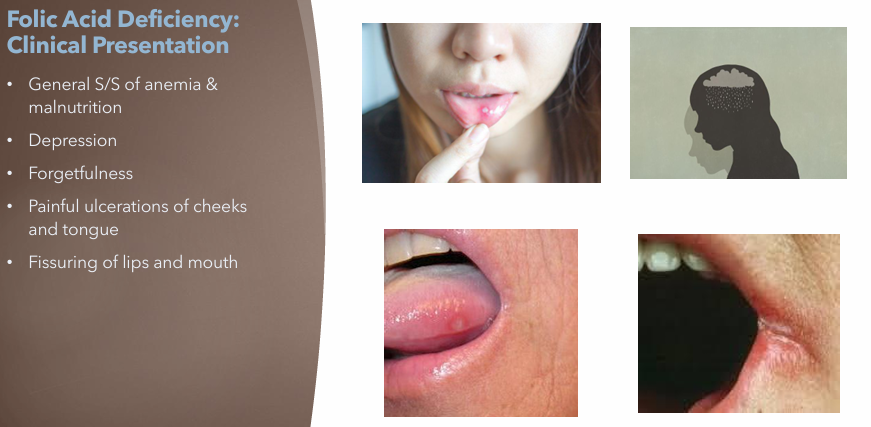
Folic Acid Deficiency Anemia: Clinical Manifestations
General S/S of Anemia
Malnutrition
Depression
Forgetfulness
Painful ulcerations of cheeks and tongue
Fissuring of lips and mouth
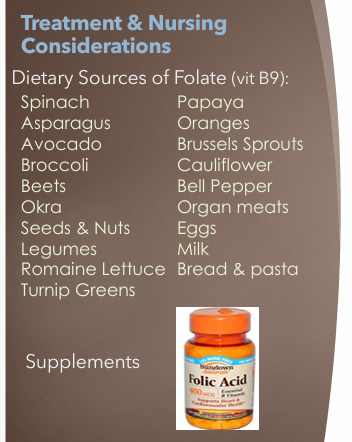
Folic Acid Deficiency Anemia: Treatments
Folic Acid Supplements
Dietary Sources of Folate (Vit B9)
Spinach
Asparagus
Avocado
Broccoli
Eggs
Milk
Bread & Pasta
Etc….
Folic Acid Deficiency Anemia: Nursing Considerations
Associate low folate with neural tube deficits (spina bifida) in infants
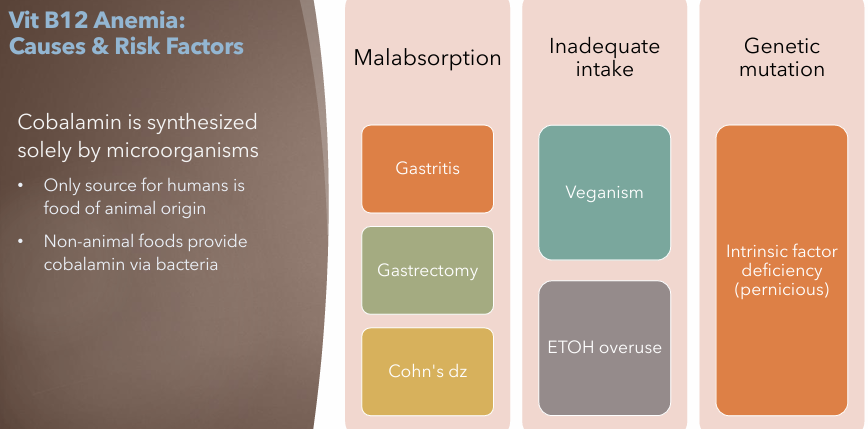
Vitamin B12 Anemia: Etiology
Inadequate intake
Malabsorption
Genetic Mutation
Intrinsic factor deficiency (pernicious)
Vitamin B12 Anemia: Pathogenesis
Disruption in DNA synthesis of blast cells;
RBCs cannot be properly synthesized → Megaloblastic RBCs
Poor oxygen carrying capacity
Vitamin B12 Anemia: Risk Factors
Malabsorption
Gastritis
Gastrectomy
Crohn’s Disease
Inadequate Intake
Veganism
ETOH overuse
Genetic Mutation
Intrinsic factor deficiency (pernicious)
Vitamin B12 Anemia: Clinical Manifestations
General S/S of Anemia
Brain fog memory issues, lack of motivation or prolonged feelings of apathy
Mood swings and grouchiness
Fatigue, low energy
Neuropathy (tingling in extremities)
Muscle weakness
Depression, dementia, blindness, or brain damage
Vitamin B12 Anemia: Treatments
Treat underlying cause
B12 Supplements or B12 Rich diet
Cyanocobalamin (Vitamin B12)
Usually administered via IM injection
Also available in PO and intranasal spray
Vitamin B12 Anemia: Nursing Considerations
Patient education on dietary sources of B12
Aplastic Anemia: Etiology
Caused by toxic, radiant or immunologic injury to the bone marrow stem cells
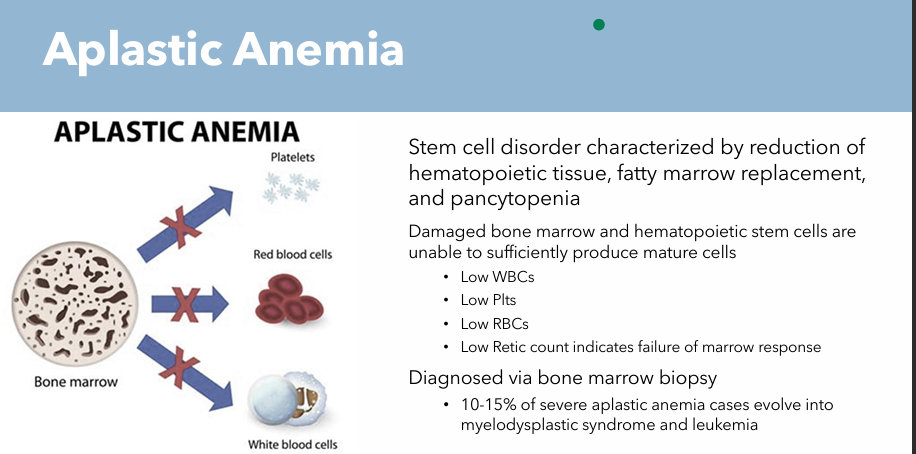
Diagnosed via bone marrow biopsy
10-15% of severe aplastic anemia cases evolve into myelodysplastic syndrome and leukemia
Aplastic Anemia: Pathogenesis
Stem cell disorder characterized by reduction of hematopoietic tissue, fatty marrow replacement and pancytopenia
Damaged bone marrow and hematopoietic stem cells are unable to sufficiently produce mature cells
Low WBCs
Low Plts
Low RBCs
Low Retic count (indicates failure of bone marrow response)
Aplastic Anemia: Clinical Manifestations
Onset of S/S may be abrupt or insidious
General S/S of anemia due to low RBCs
Additional S/S include those to low Plts (bleeding)
May also include S/S due to low WBCs
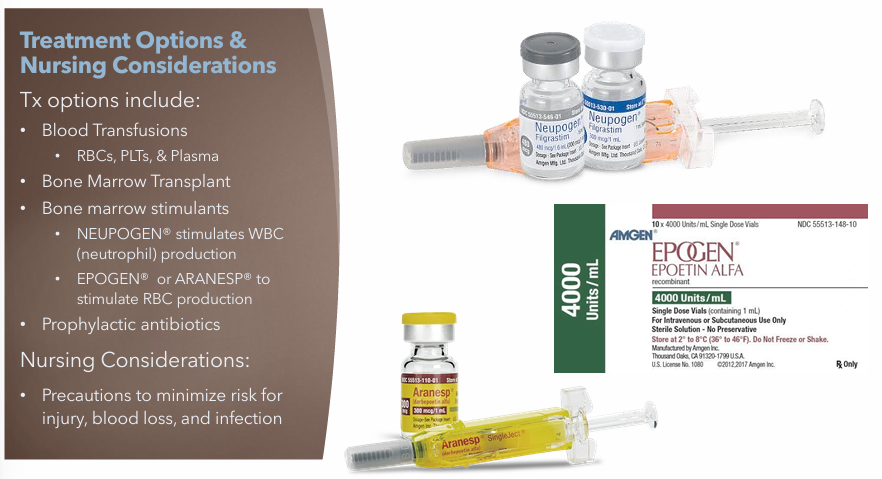
Aplastic Anemia: Treatments
Blood Transfusions
RBCs, PLTs, Plasma
Bone Marrow Transplants
Bone Marrow Stimulants
NEUPOGEN (Stimulates WBC production)
EPOGEN or ARANESP (Stimulates RBC production)
Prophylactic antibiotics
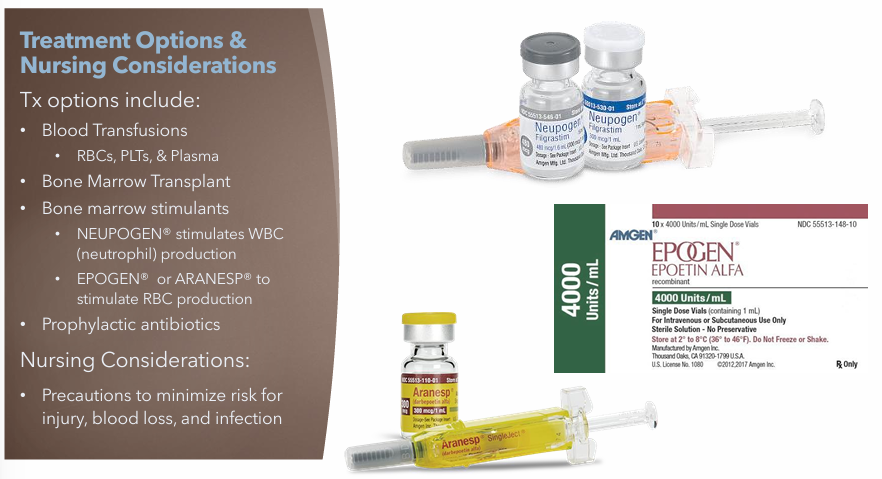
Aplastic Anemia: Nursing Considerations
Precautions to minimize risk for injury, blood loss, and infection
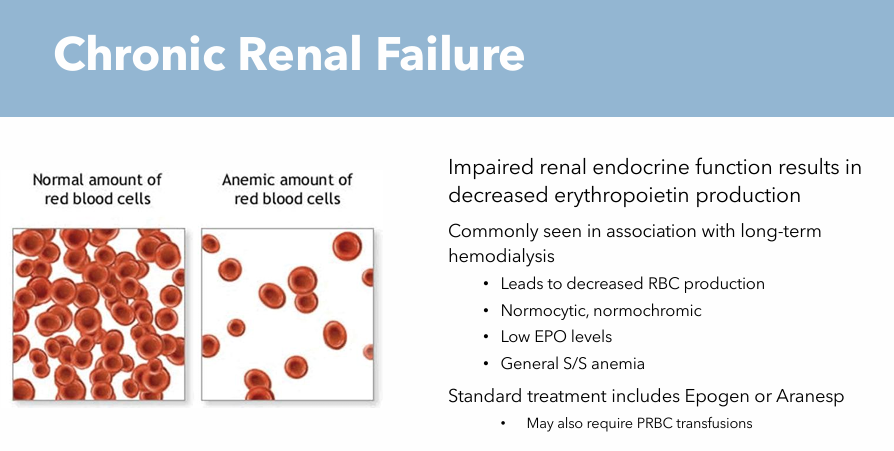
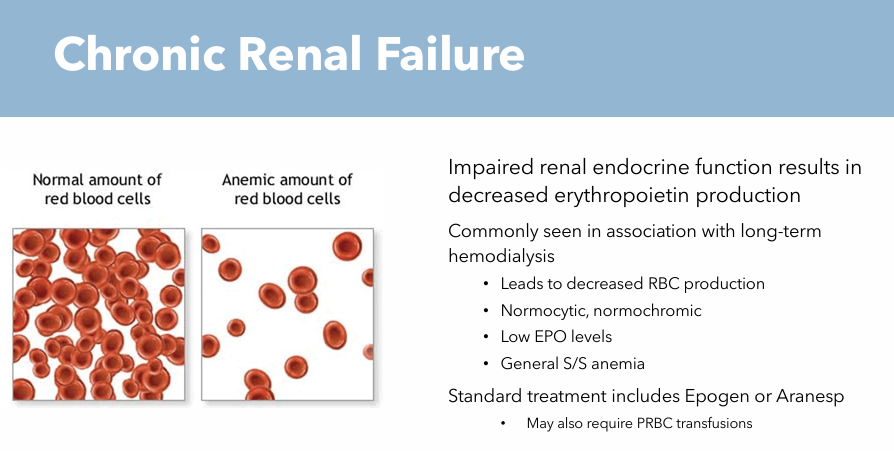
Chronic Renal Failure: Etiology
Impaired renal endocrine function
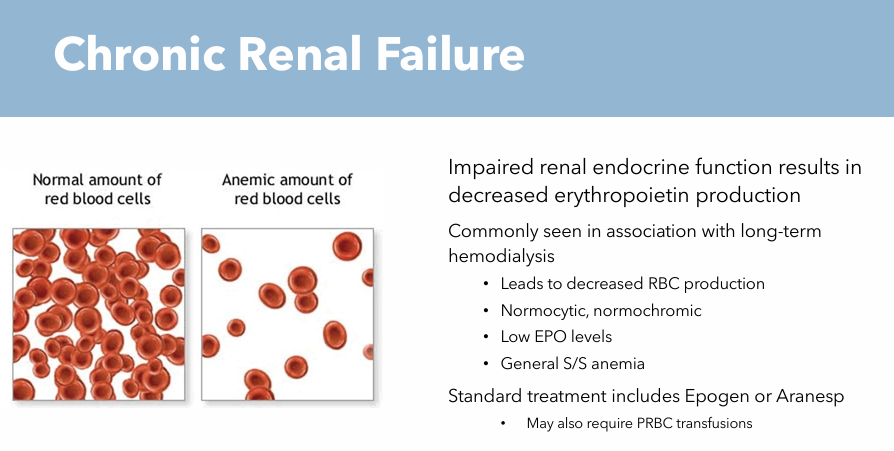
Chronic Renal Failure: Pathogenesis
Decreased erythropoietin production leads to decreased RBC production
Chronic Renal Failure: Risk Factors
Long term hemodialysis
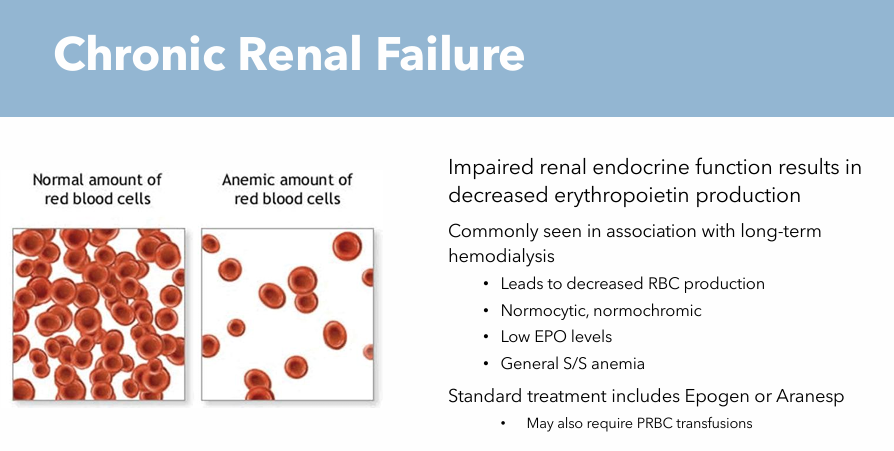
Chronic Renal Failure: Clinical Manifestations
General S/S of anemia
Normocytic
Normochromic cells
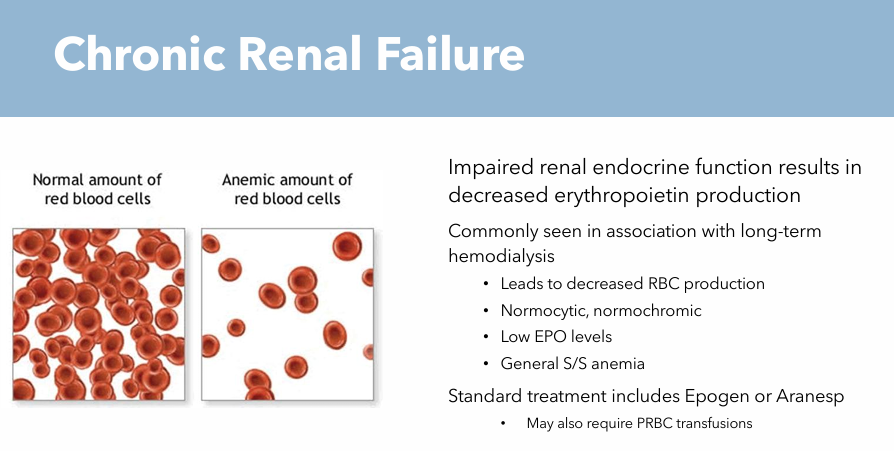
Chronic Renal Failure: Treatments
Epogen
Aranesp
May also require PRBC transfusions
Chronic Renal Failure: Nursing Considerations
Monitor and assess for signs of Renal Failure when long-term hemodialysis
Blood Work: Signs of Iron Deficiency Anemia
Hypochromic, Microcytic RBCs
Low MCV, MCH, and MCHC
Serum ferritin level decreased
Serum Iron level decreased
Total Iron binding capacity (TIBC) increased
Blood work: Sign of Vitamin B12 Anemia
Megaloblastic (enlarged, oval shaped)
Serum B12 decreased
Serum Folate decreased
Blood Work: Signs of Folic Acid Deficiency Anemia
Serum Folate <4 ng/mL
Low Hgb/Hct level
Blood Work: Signs of Aplastic Anemia
Low WBCs
Low Plts
Low RBCs
Low Retic count indicates failure of marrow response
Blood work: Sign of Chronic Renal Failure
Leads to decreased RBC production
Normocytic, Normochromic
Low EPO levels
General S/S Anemia
Extrinsic RBC loss/destruction conditions
Hemorrhagic Anemia
Hemolytic Anemia
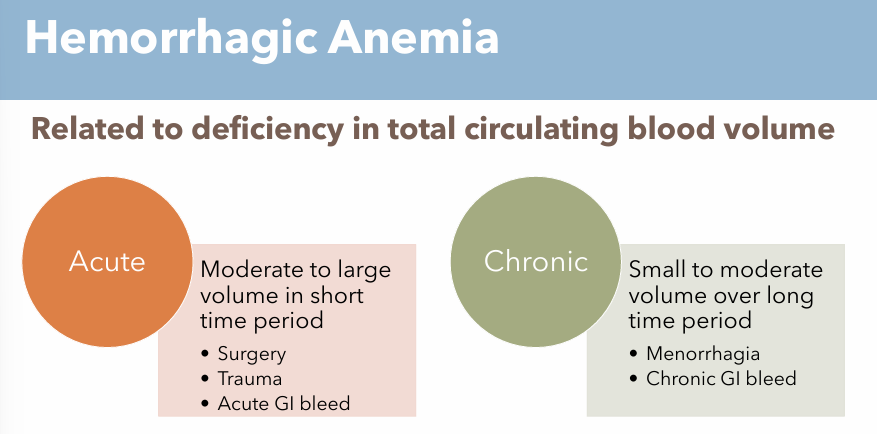
Hemorrhagic Anemia Etiology (Acute & Chronic)
Acute
Moderate to large volume of total circulating blood loss in short time period
Surgery
Trauma
Acute GI bleed
Chronic
Small to moderate volume of total circulating blood loss over long time period
Menorrhagia
Chronic GI bleed
Hemorrhagic Anemia Pathogenesis (Acute & Chronic)
Deficiency in total circulating blood volume Acute or Chronic
Hemorrhagic Anemia Risk Factors (Acute & Chronic)
Acute
Surgery
Trauma
Acute GI bleed
Chronic
Menorrhagia
Chronic GI bleed
Hemorrhagic Anemia Clinical Manifestations (Acute & Chronic)
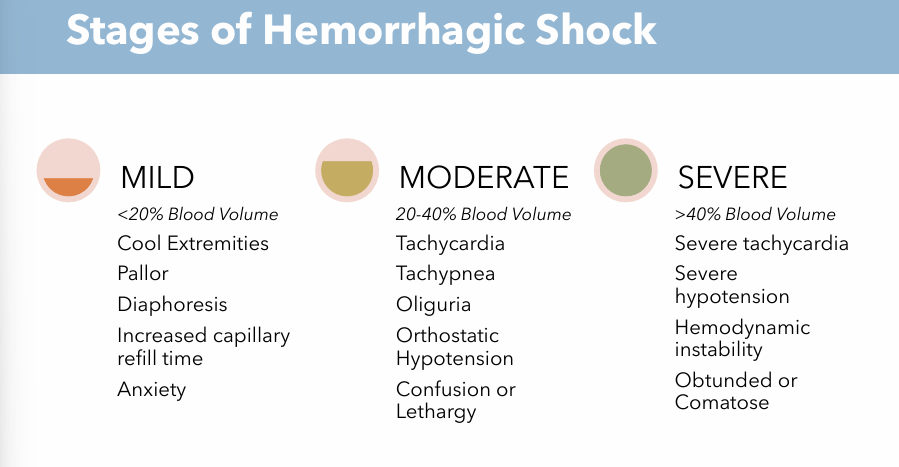
Stages of Hemorrhagic Shock
Mild: (<20% Blood Volume Loss)
Cool Extremities
Pallor
Diaphoresis
Increased capillary refill time
Anxiety
Moderate: (20-40% Blood Volume Loss)
Tachycardia
Tachypnea
Oliguria
Orthostatic Hypotension
Confusion or Lethargy
Severe: (>40% Blood Volume Loss)
Severe tachycardia
Severe hypotension
Hemodynamic instability
Obtunded or Comatose
Hemorrhagic Anemia Treatments (Acute & Chronic)
Treat underlying cause
Transfusion of blood products

Hemorrhagic Anemia Nursing Considerations (Acute & Chronic)
Monitor Closely for changes from baseline
Mental status changes can be early sign
Correlation between palpable pulses and systolic BP

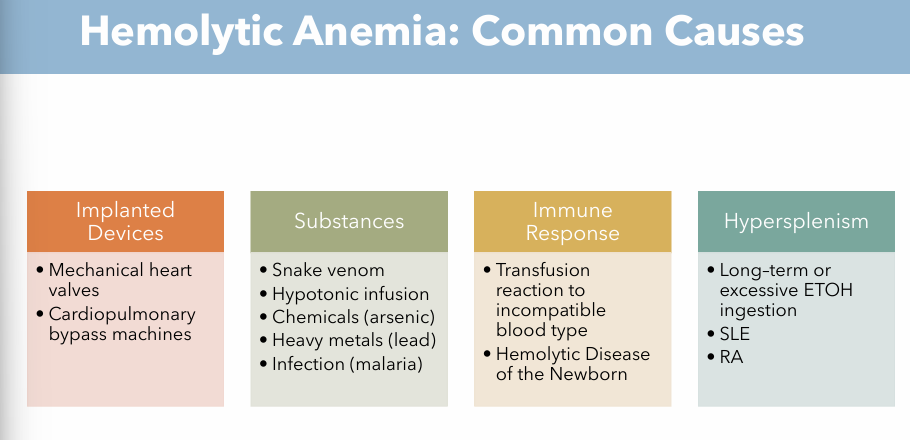
Hemolytic Anemia Etiology
Implanted Devices (Mechanical)
Mechanical heart valves
Cardiopulmonary bypass machines
Immune Response (Autoimmune response)
Transfusion reaction to incompatible blood type
Hemolytic disease of the Newborn
Hypersplenism (Organ Dysfunction)
Long term or excessive ETOH ingestion
SLE
RA
Substances (Chemical)
Snake venom
Hypotonic infusion
Chemicals (arsenic)
Heavy metals (lead)
Infection (malaria)
Hemolytic Anemia Pathogenesis
RBCs are destroyed faster than they are replaced
Hemolytic Anemia Risk Factors
Malaria infection
Transfusion reactions
Hypersplenism (SLE, RA)
Mechanical Heart Valves
Cardiopulmonary bypass machines
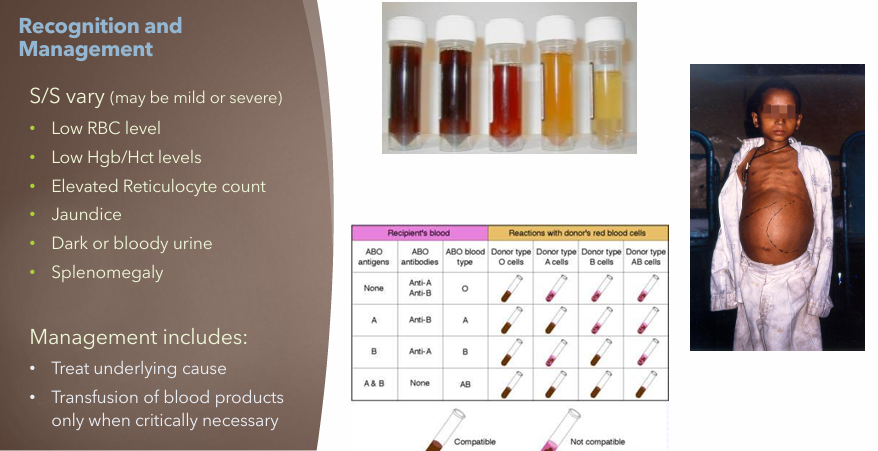
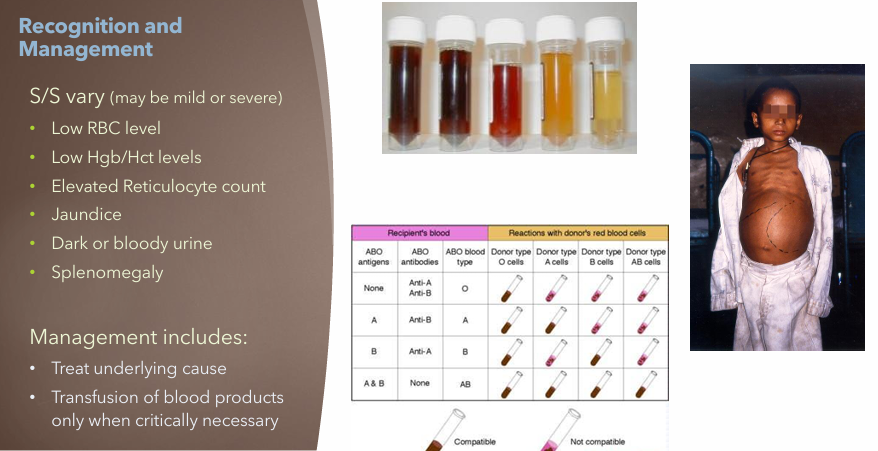
Hemolytic Anemia Clinical Manifestations
S/S vary mild or severe
Dark or bloody urine
Jaundice
Splenomegaly
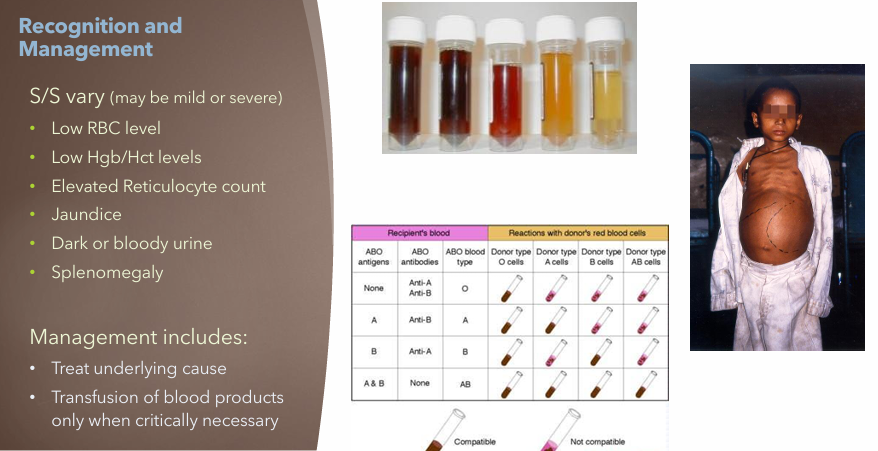
Hemolytic Anemia Treatment
Treat underlying cause
Transfusion of blood products only when critically necessary
Blood Work: Signs of Hemorrhagic Anemia
Low RBC level
Normocytic, Normochromic
Low Hgb/Hct levels
Blood work: Signs of Hemolytic Anemia
Low RBC level
Low Hgb/Hct levels
Elevated Reticulocyte count
What are the inherited blood anemia disorders?
Sickle Cell Anemia
Thalassemia

Sickle Cell Anemia: Etiology
Inherited genetic mutation
African American, Arab, Asian descent
Sickle Cell Anemia: Pathogenesis
Abnormal HGB (hemoglobin) production resulting in decreased O2 carrying capacity
Misshaped RBCs leading to increased RBC hemolysis (destruction)
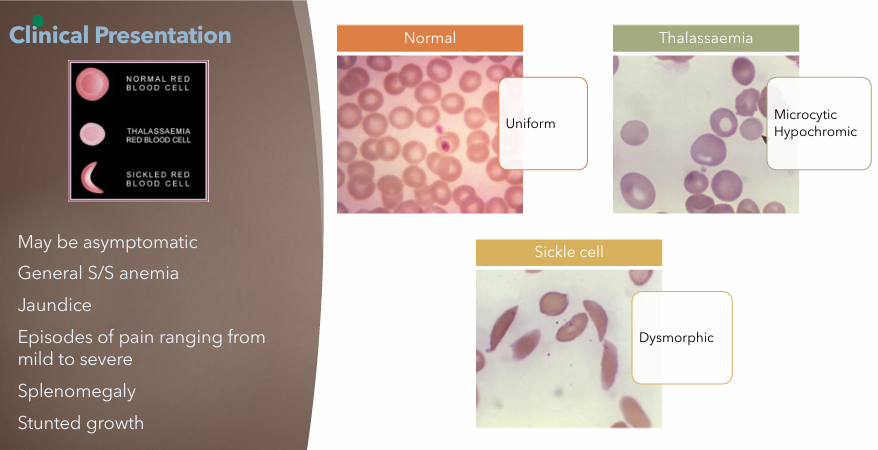
Dysmorphic
Sickle Cell Anemia: Risk Factors
Genetics, family hx
Ancestry
Sickle Cell Anemia: Clinical Manifestations
May be asymptomatic
General S/S anemia
Jaundice
Pain episodes (mild to severe)
Splenomegaly
Stunted growth
Sickle Cell Anemia: Treatment
Rx to prevent RBC sickling
Voxelotor
Hydroxyurea
Folic Acid Supplement
Reduce Risk for exacerbation (SCC)
Vaccinations
Allogenic Bone Marrow Transplant
Gene Therapy (limited availability)
Sickle Cell Anemia: Nursing Consideration
SCD Crisis Management
Identify and treat cause
Pain management
Supplemental O2
Blood transfusions
Hydration
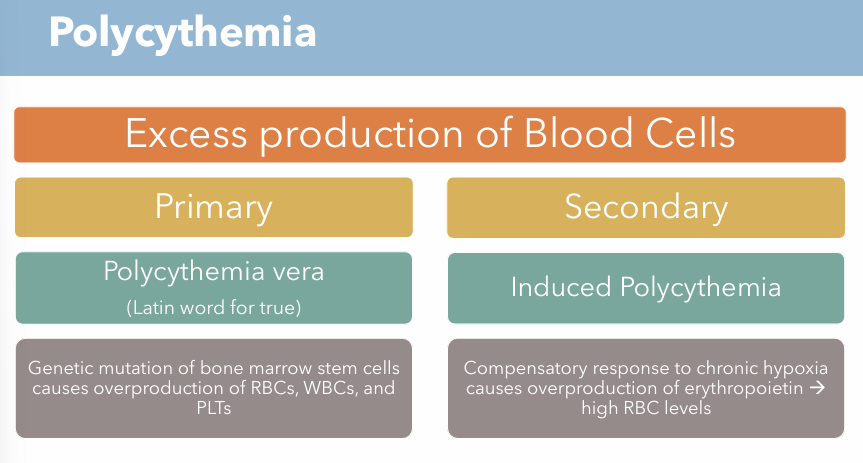
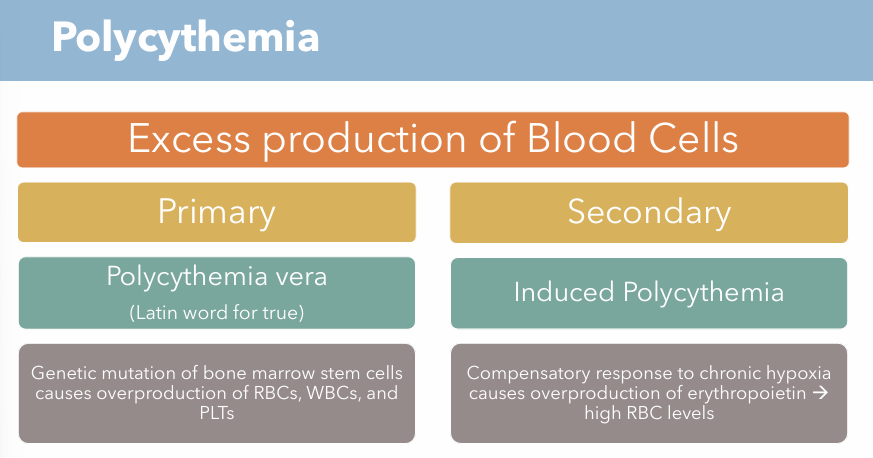
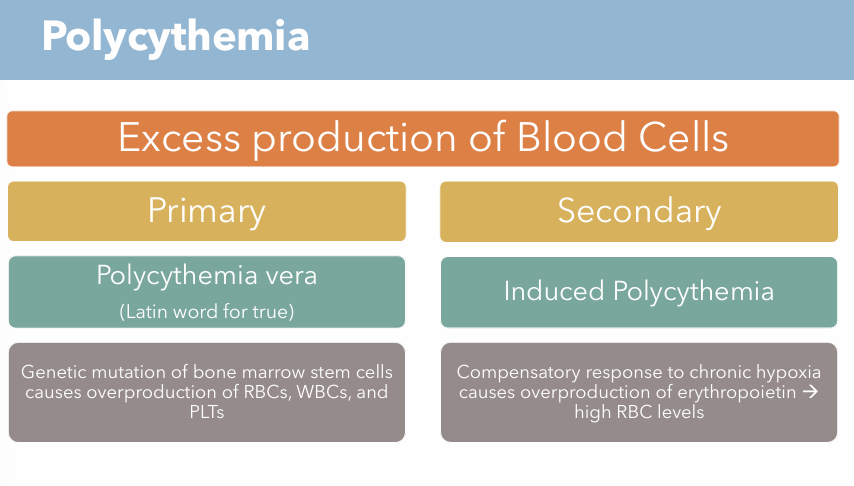
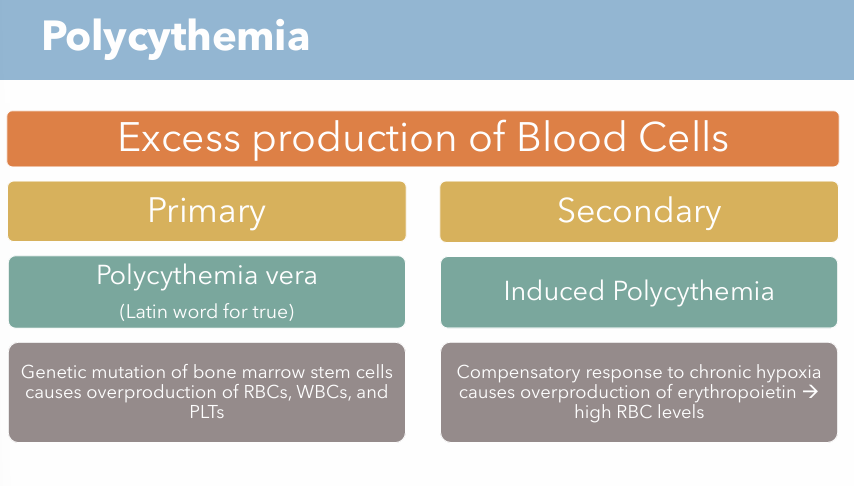
What is polycythemia? What are the two types of conditions?
Excess production of blood cells
Polycythemia vera (Primary)
Induced Polycythemia (Secondary)
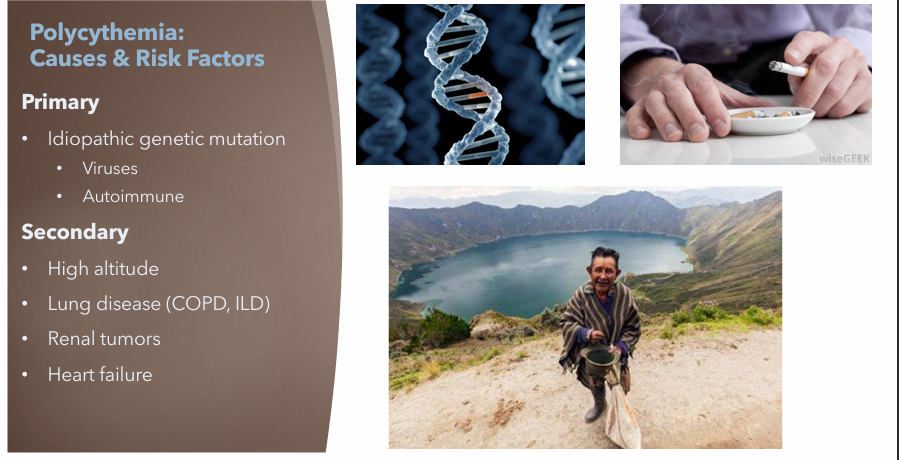
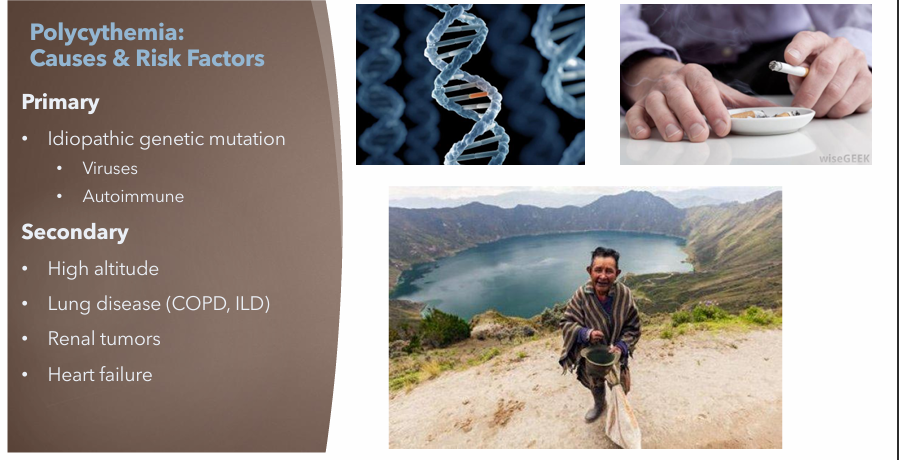
Polycythemia Vera: Etiology
Idiopathic genetic mutation
Polycythemia Vera: Pathogenesis
Genetic mutation of bone marrow stem cells causes overproduction of RBCs, WBCs, and PLTs
Polycythemia Vera: Risk Factors
Viruses
Autoimmune
Polycythemia Vera: Clinical Manifestations
Usually insidious onset of S/S
Pruritus
HA
Weakness
Fatigue
Dyspnea
Dizziness
Visual disturbances
Weight loss
Enlarged spleen
Abdominal discomfort
Erythromelalgia
Increased PLT aggregation → tiny blood clots in extremities vessels

Polycythemia Vera: Treatment & Nursing Considerations
Therapeutic phlebotomy
Radiation
Chemotherapy
Interferon alpha: off label use now being researched

Secondary Polycythemia: Etiology
Chronic hypoxia
Secondary Polycythemia: Pathogenesis
Compensatory response to chronic hypoxia causes overproduction of erythropoietin → high RBC levels
Secondary Polycythemia: Risk Factors
High altitude
Lung Disease (COPD, ILD)
Renal tumors
Heart failure
Secondary Polycythemia: Clinical Manifestations
Usually insidious onset of S/S
Pruritus
HA
Weakness
Fatigue
Dyspnea
Dizziness
Visual disturbances
Weight loss
Enlarged spleen
Abdominal discomfort
Erythromelalgia
Increased PLT aggregation → tiny blood clots in extremities vessels

Secondary Polycythemia: Treatment & Nursing Considerations
Treat underlying cause
Admin O2
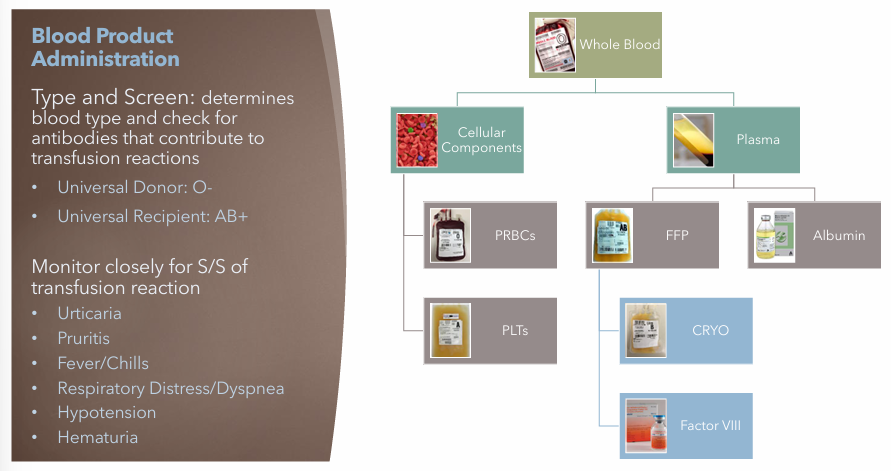
Blood Product Administration S/S
Monitor closely for S/S of transfusion reaction
Urticaria
Pruritis
Fever/Chills
Respiratory Disease/Dyspnea
Hypotension
Hematuria