L05 The Adrenergic System
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
Abbreviations
Adrenaline (ADR) = Epinephrine (EPI)
Noradrenaline (NA) = Norepinephrine (NE)
Related to ADR or NA = adrenergic or noradrenergic
Though ADR and NA share features, they also have important differences
Our focus is NA, as it is more important to the brain
notably, noradrenaline is more important within the brain
ADR + NA
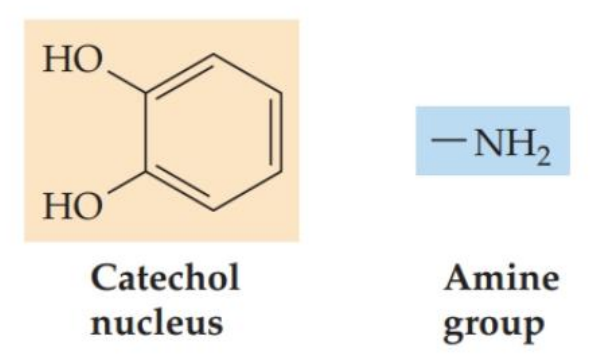
Monoamine (w/DA + 5-HT) and catecholamine (w/DA only) families
Catecholamines have a similar structure as well as shared synthesis + metabolism pathways
Numerous implications, including shared drug sensitivity
in group of DA, which is why it is affected by same compounds
hence, ADHD drugs affect both dopaminergic + adrenergic systems
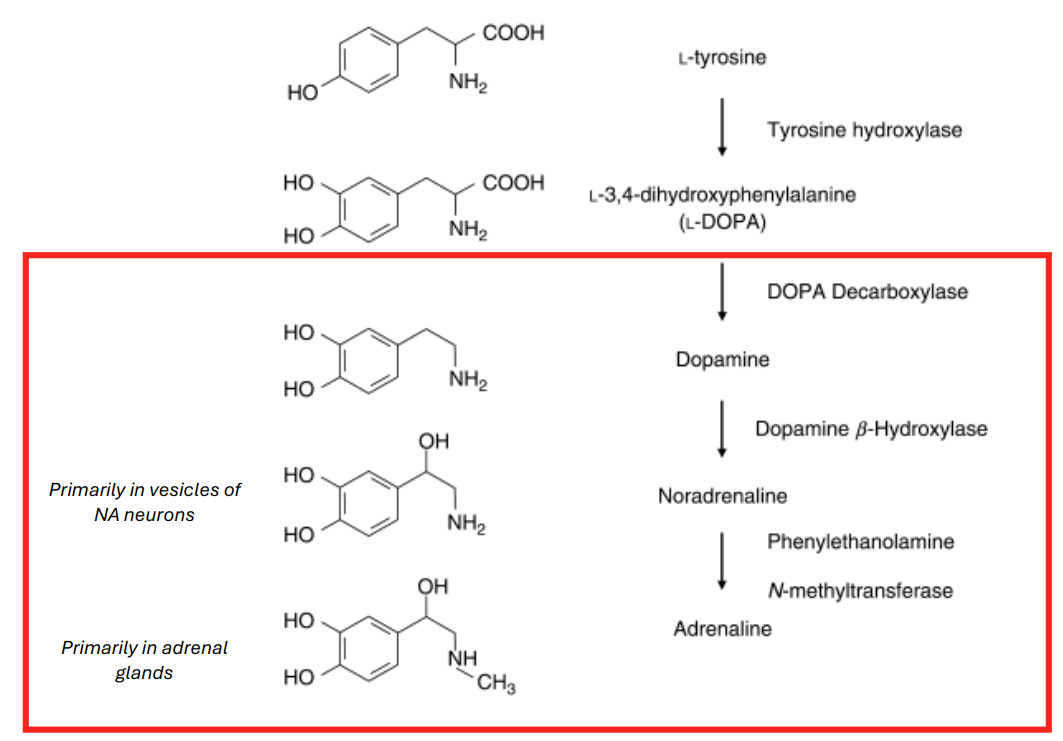
ADR + NA Synthesis
Begins w/dopamine (DA) production (see L04)
DA then reacts with the enzyme dopamine-B-hydroxylase to produce NA
Enzymes act on NA to produce ADR
tyrosine → DA → NA→ adrenaline
LHS: fine print where synthesis is occurring → neurons that make DA that don’t have to make NA in their vesicles
make DA and if you’re the right type of neuron → you turn that into something else (NA made by vesicles in NA neurons) → NA important in brain
in periphery, ADR important, made by adrenal glands → most doesn’t reach the brain
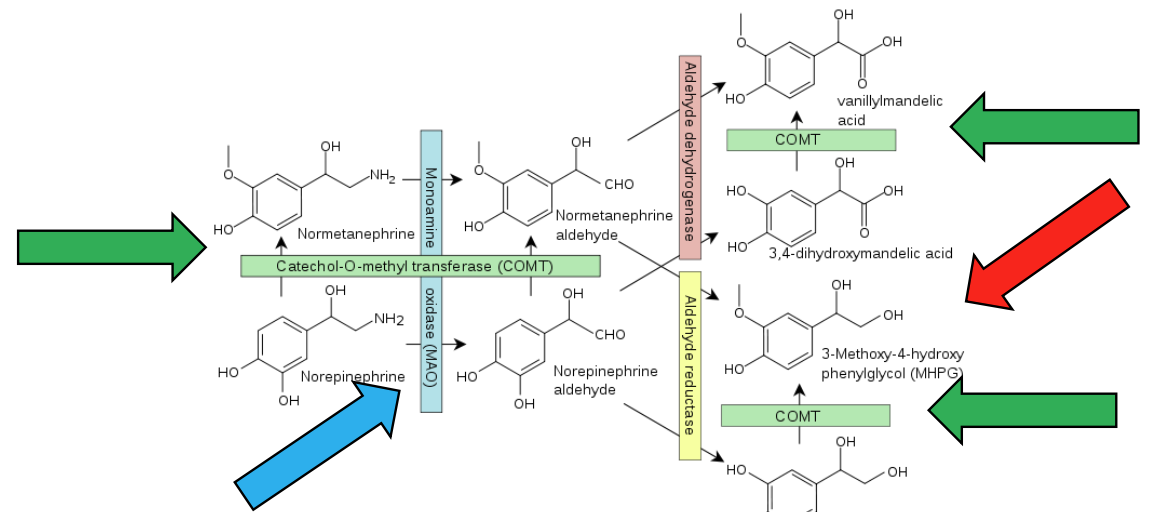
Metabolism
• Metabolized by COMT (1) and MAO (2)*
MAO inhibitors for depression, COMT + MAO inhibitors for Parkinson’s (adjuncts)
MHPG is a metabolite (surrogate measure of NA)1-4 • Bipolar disorder, eating disorders, gambling disorders, PTSD (recall: weak correlations + not strong enough to be diagnostically useful)
catechol-O-methol transferase (COMT) → acts on catecholamines, including DA and NA
NA also a monoamine and can also be targeted by monoamine oxidase (MAO)
therefore 2 metabolic routes for NA
with COMT/MAO inhibitor → will affect breakdown of NA and other NTs → such compounds associated w higher NA levels
MAO inhibitors used for depression
COMT + MAO inhibitors used for PD
MHPG (DNM name) → a metabolite important as index of NA (if lots of metabolite in periphery, it may mean lots of NA in the brain or somewhere else)
Receptors
ADR + NA:
alpha 1: Excitatory
alpha 2: Generally inhibitory
α2A, PFC = postsynaptic
α2 can be pre-synaptic
beta: Generally excitatory
3 classes of receptors
a1 and a2 more well studied + better understood
significance of pre-synaptic receptors = usually inhibitory (often for turning off)
lever for shutting things is AP at axon hillock
presynaptic usually a2

Receptor affinity
Strength of binding between agent and receptors
Receptor affinity varies across subtypes
Some receptors are fully active at low NA levels (high affinity, α2) whereas other require higher levels (low affinity, α1)
At low NA concentrations, α2 more active (receptor is high affinity)
At high NA concentrations, both α2 and α1 are active
Relevant to theories of noradrenergic function (e.g. PFC for working memory)
a1 has this affinity for NA = strength of association for those 2 things
high affinity of receptor for agent = strong bond, meaning a very low concentration of agent is needed to bind all receptors
low affinity = need lots of agent for receptors to be bound
when we know affinity, we know how much agent is needed to bind receptors
leads to concept that if agent is of low concentration, this means only high affinity receptors are bound
if concentration of agent high, we expect low + high affinity receptors to be bound
stress or arousal = situations where NA and ADR concs vary
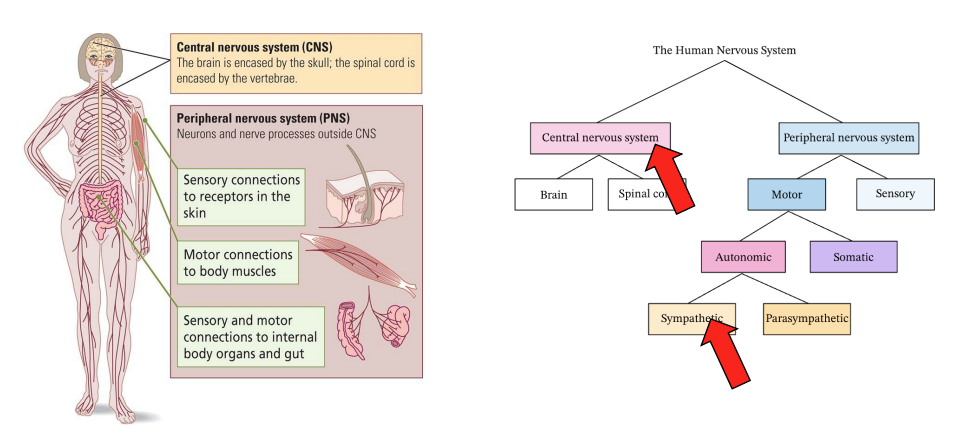
Where do we find NA-releasing (adrenergic) neurons?
The NA system
Widely distributed across PNS and CNS
noradrenergic neurons in CNS but also PNS, which branches into autonomic > sympathetic division
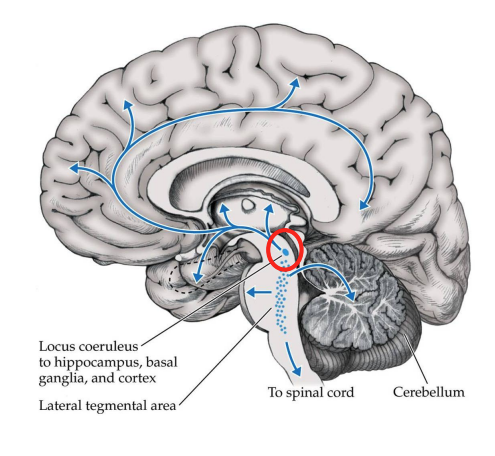
NA system (Central) – Main area
The locus coeruleus (LC) contains most of the NA neurons in your brain
Small (~30 000 neurons) but has many projections
LC innervation of the hippocampus, prefrontal cortex and basolateral amygdala is critical (projections to these areas)
PFC innervation may be important for attention, hippocampus innervation for memory, etc.
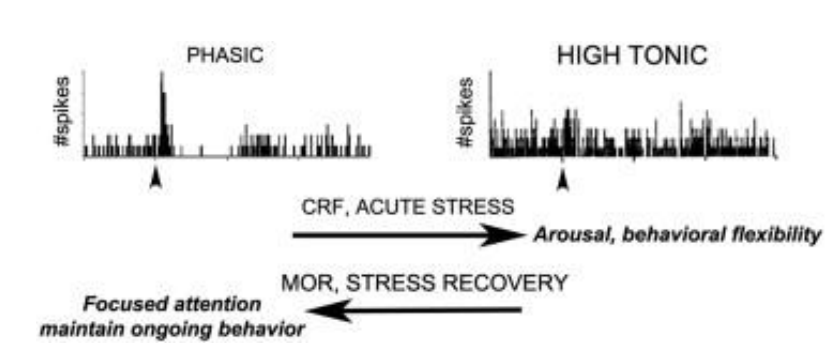
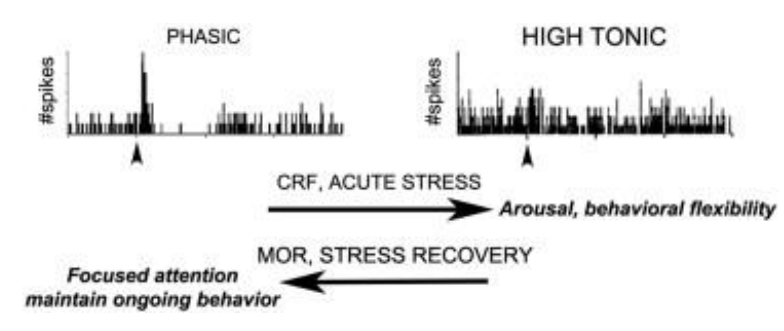
About the LC
Tonic (maintained) and phasic (brief) firing (L04)
Tonic correlates with overall arousal state (~ exploration)
like states of awake, alert, drowsy, asleep, deep sleep, etc. (like walking around env, taking in sights)
Phasic correlates w/specific responses (~ exploitation)
interacting intensively for a brief episode
Controlled stimulation of the LC (e.g. via optogenetics) can have strikingly different effects on the brain1
demonstrates tonic firing (maintained all the time but tends to be low) even when nothing special is going on
potential for great increase in firing rate in short time interval = phasic firing (phasic bursts + tonic over long time)
theory - activity firing associated w different things
diagram - stress is associated w change in firing rate of these neurons
acute stress = high tonic rate
CRF = neuropeptide released by brain to initiate response to acute stress
The NA system (Peripheral)
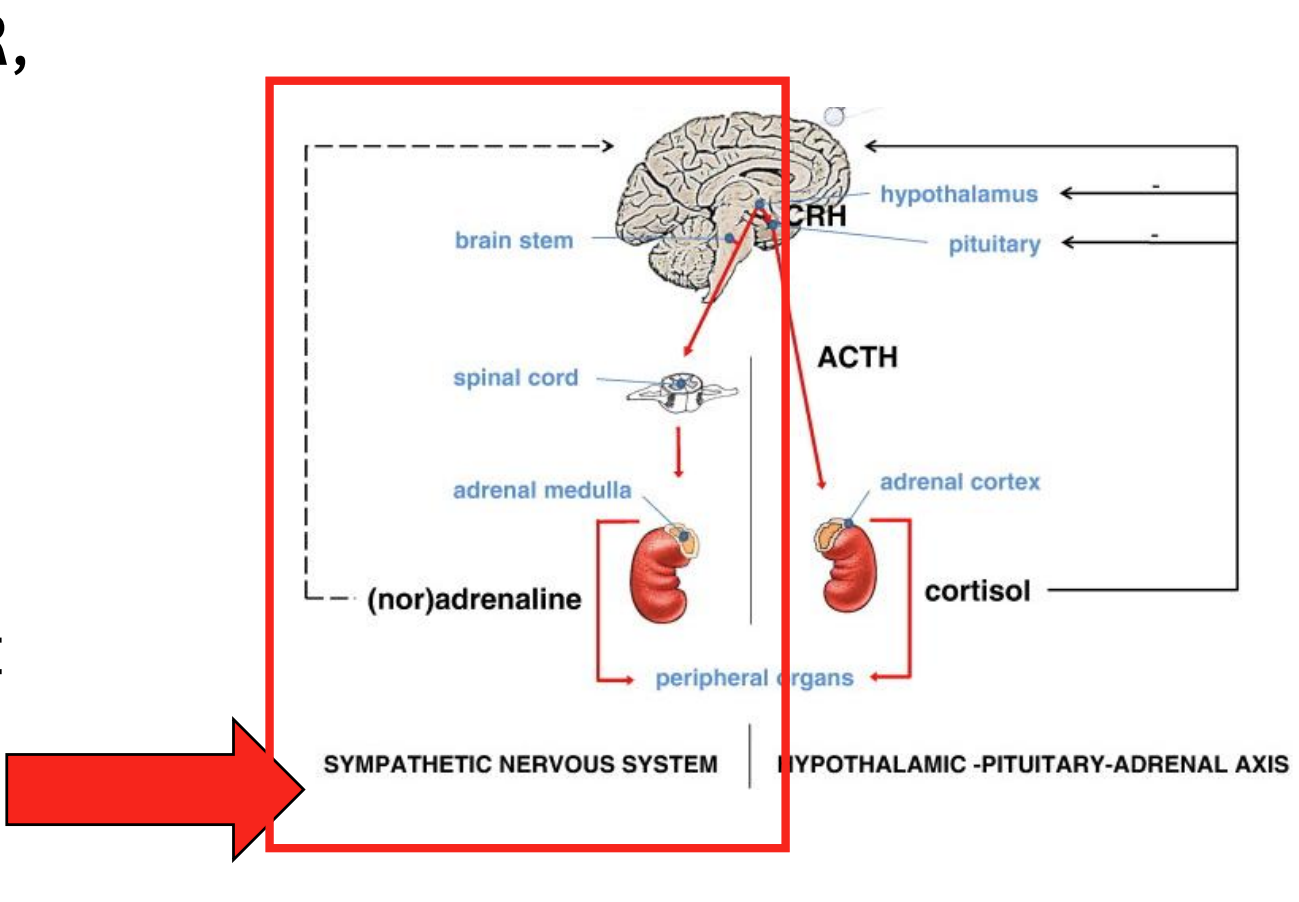
The ANS is involved in automatic, involuntary changes in organ function
The ANS has sympathetic and parasympathetic divisions (SNS + PNS)
SNS = “fight or flight”]
often NA signal is major NT
PNS = “rest and digest”
PNS component where we find these cells → part of sympathetic division (LHS)
recall PNS = everything not at the midline + not encased in bone, so NS in contact w organs → in some fibers in sympathetic division, NA signaling happens
![<ul><li><p>The <strong>ANS </strong>is involved in automatic, involuntary changes in organ function</p></li><li><p>The ANS has <span style="color: red;"><strong>sympathetic </strong></span>and <span style="color: blue;"><strong>parasympathetic </strong></span>divisions (SNS + PNS)</p></li><li><p>SNS = “fight or flight”]</p><ul><li><p>often NA signal is major NT </p></li></ul></li><li><p>PNS = “rest and digest”</p></li></ul><div data-type="horizontalRule"><hr></div><ul><li><p>PNS component where we find these cells → part of sympathetic division (LHS)</p><ul><li><p>recall PNS = everything not at the midline + not encased in bone, so NS in contact w organs → in some fibers in sympathetic division, NA signaling happens </p></li></ul></li></ul><p></p>](https://assets.knowt.com/user-attachments/b6e4ee1e-add2-47e6-8342-9777b31f24f8.png)
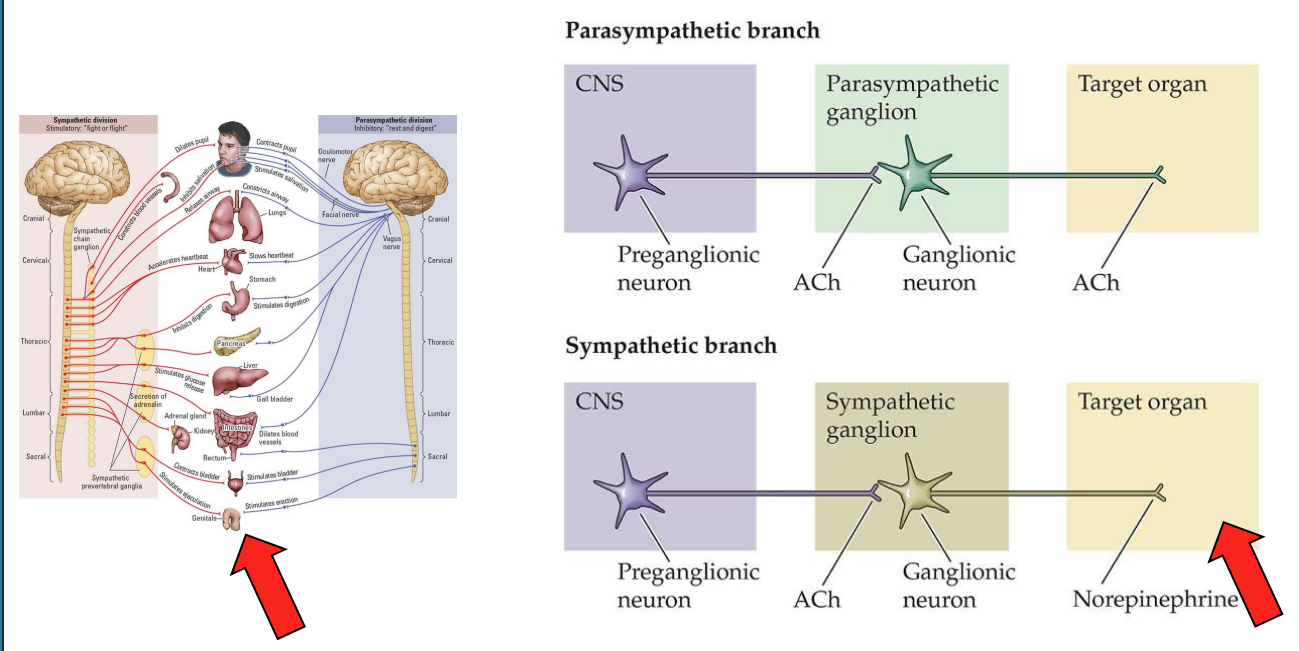
The NA system (Peripheral)
Certain effects – like pupillary diameter – are going to be important later
target organ = NA in SNS (contact/signaling to organ is via NA)
importantly, neurons in brain in LC are noradrenergic → involved in affecting organ function in many stress + arousal-like states + flight/fight (speeding up heart, changing breahting)
notably an effect is pupillary diameter → index of SNS activation
Indexing adrenergic function
Pupillary diameter measures (SNS marker)
note: not a LC marker
Salivary amylase (SNS marker)
can measure non-invasively
Metabolite measurement
MHPG
MRI adapted for the LC (i.e. LC neuromelanin MRI; see L4)
MRI signals that pick up certain structures associated w noradrenergic transmission
in situations where NA levels are high + noradrenergic transmission is significant → we can see this things as indices
Adrenal Gland releases ADR
Adrenal gland mixture is 80% ADR, 20% NA
ADR + NA in the blood does not easily cross the BBB
Direct effects unlikely but indirect possible
almost none of ADR/NA gets to brain bc it cannot cross BBB easily
large amount at periphery released at certain states has peripheral actins that are significant but central actions in brain less significant bc it can’t penetrate
peripheral effects can indirectly give rise to central effects via indirect mechanisms downstream, even thought ADR + NA doesn’t enter the brain
injected mice w ADR in periphery but were found to be smarter due to indirect effects
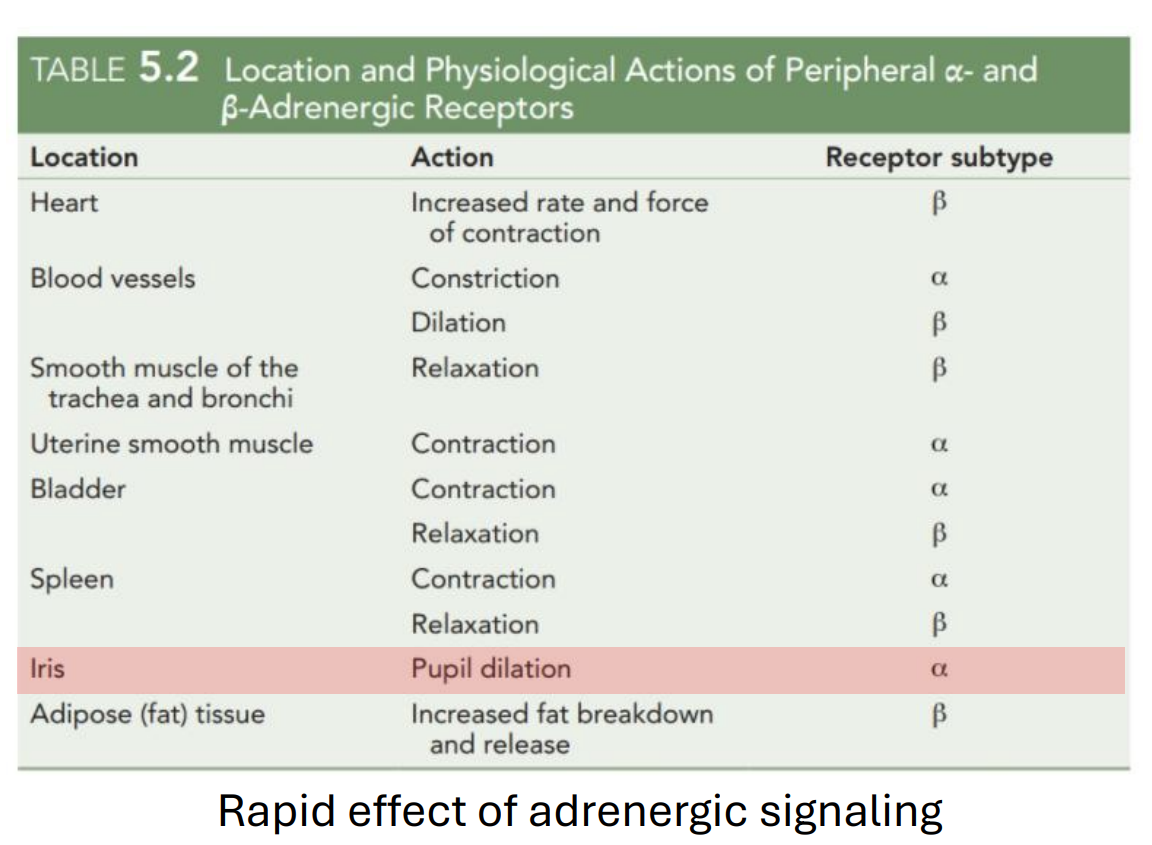
Rapid effect of adrenergic signalling
lots of peripheral effects associated w NA signaling
DN receptor subtype
when taking a drug, you could predict the type of physiological effect if you know the receptor type involved
pupil dilation = rapid effect
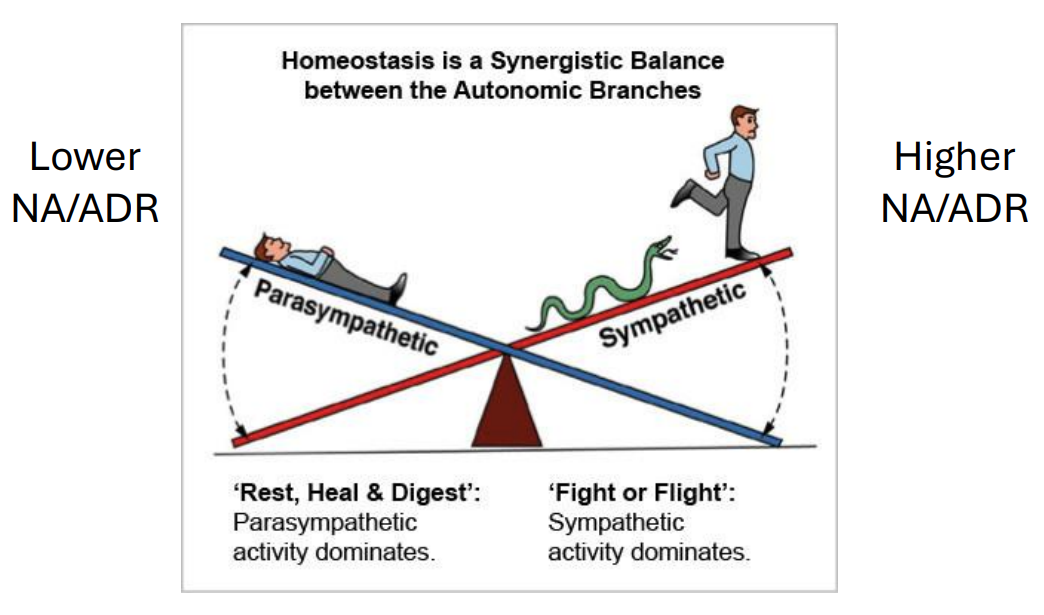
PNS, SNS + the adrenergic system
ADR + NA levels vary w states of consciousness
lower NA/ADR → anticipate more relaxed state
higher NA/ADR → anticipate more fight/fight state (stress, arousal, etc.)
states where sympathetic NS is likely to be more active = more noradrenergic signaling happening
Lower NA/ADR in PNS dominance
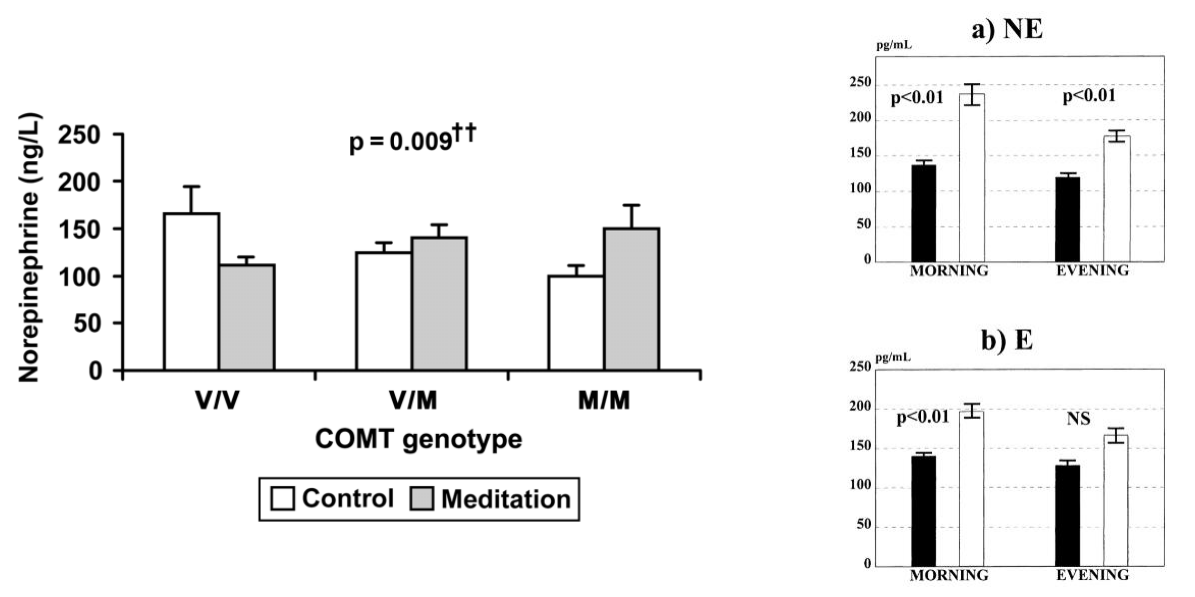
Meditation is associated with lower NA + ADR (depends on style, genetics) → more parasympathetic activation
note: it is not just 1 system being on; there is both to various degrees → so one is more dominant
noradrenaline + adrenaline levels lower in those that meditate and also low in those that meditate regularly
note crude proxy → looking at diff substance in diff compartment + drawing inferences about what could be going on in brain
Meaning of basal NA/ADR is complex
Individual variability is high
Peripheral measures of metabolites may not reflect central activity of transmitter
Understanding stress requires measurement of the stress states and coping responses, not just the baseline
Ignores cortisol
hormones often written as ranges because lots of individual variability → eg. log cortisol
therefore measurements should also be done at several time points → ideally to capture a change in levels over time bc starting point differs across individuals
Importantly…
NA + ADR increase during stress and SNS activation
Though many people might find arousal and SNS activation unappealing (even terrifying), this might not be the case for everyone
Some might find states exhilarating and actively seek them out
This brings us to a popular idea…
“Adrenaline addict”
A person who engages in high-risk, arousing behaviors for pleasure (thrill-seeker)
Extreme sports is a common example
Exercise addiction considered separate
Not a clinical term
Except gambling, behavioral addictions are controversial
Studies are very few and almost entirely psychological (i.e. not neurochemical)
ADR released during stress does not enter the brain
many behavioral problems aren’t considered addictions, except problematic gambling
NA/ADR in risk-taking
In humans, NA levels are higher in problematic gambling
In animals, NA levels are correlated with high-risk, exploratory behaviors
Genes in the NA system are weakly linked to risk-taking
Drugs affecting NA levels affect decision-making
SNS activation (w/ADR + NA increases) contributes to stress. However, the SNS is not the only system active during stress.
NA signaling and its association with SNS activation
but it’s not the only signaling form that changes in those states
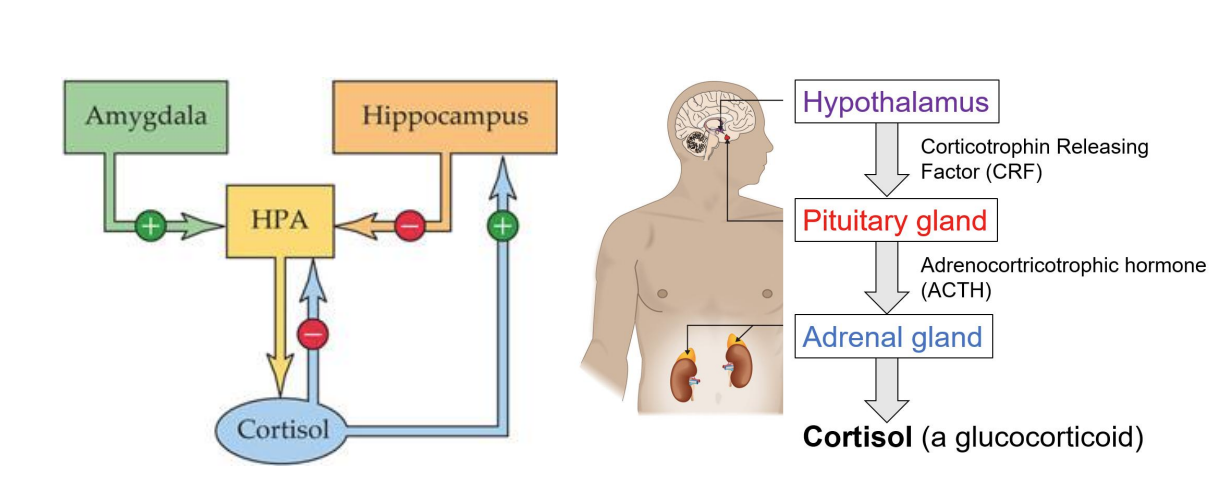
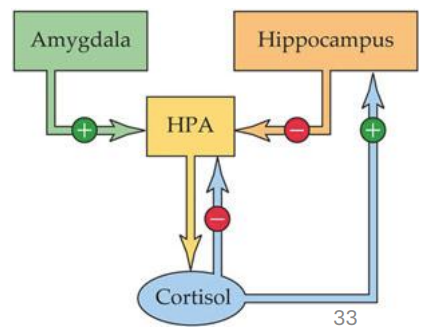
Stress + the HPA axis
cortisol also changes in states of stress/arousal
cortisol is likely changes around the same time + likely interacts with NA signaling
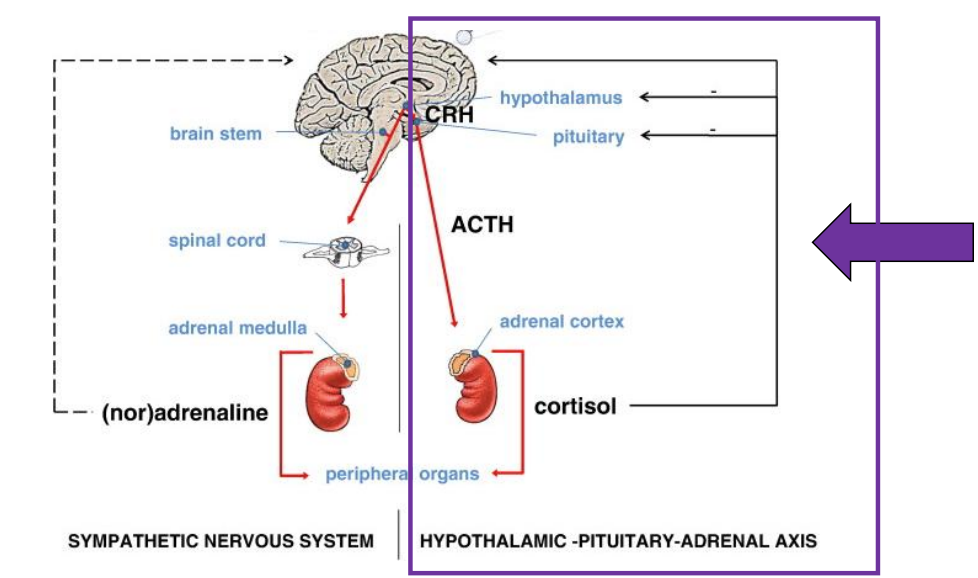
Stress and the HPA axis
Comparisons – SNS vs. HPA
The SNS response is…
Involved in the orientation to stressors
Fast-acting and short-lasting
The HPA response is…
A defeat response for stressors perceived as uncontrollable
Associated w/avoidance, withdrawal and mental illness
Slow-acting and long-lasting
SNS and HPA responses overlap and interact
Activity of these systems may be abnormal in disorders
SNS response occurs first, then HPA response kicks in, but may be both in play at same time
Post-traumatic stress disorder
lots of study into LT effects of these systems being active on your immune system
PTSD not only associated w military service, it can be associated w any traumatic event (even witnessing one)
is one of the few disorders with a clear cause (anticipant event) → but also outcomes are among the more serious ones → but opportunity for treatment
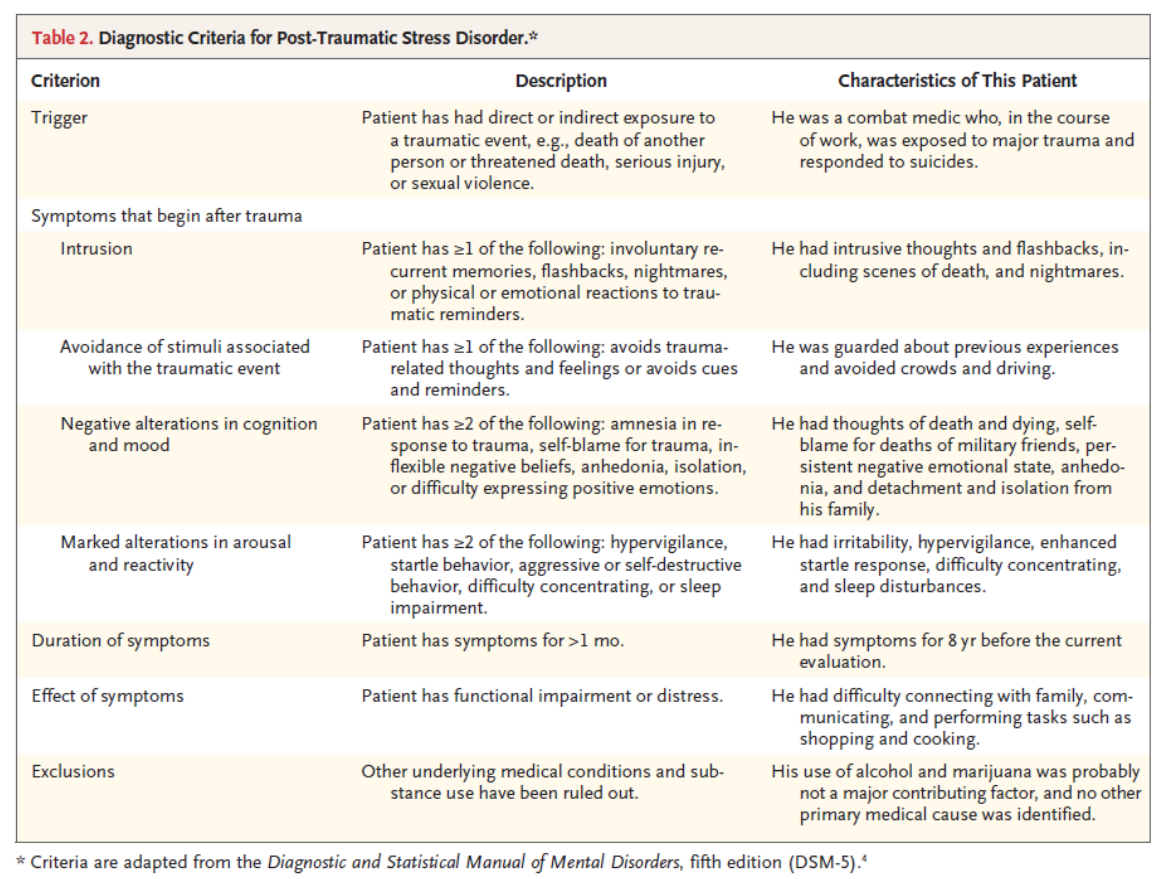
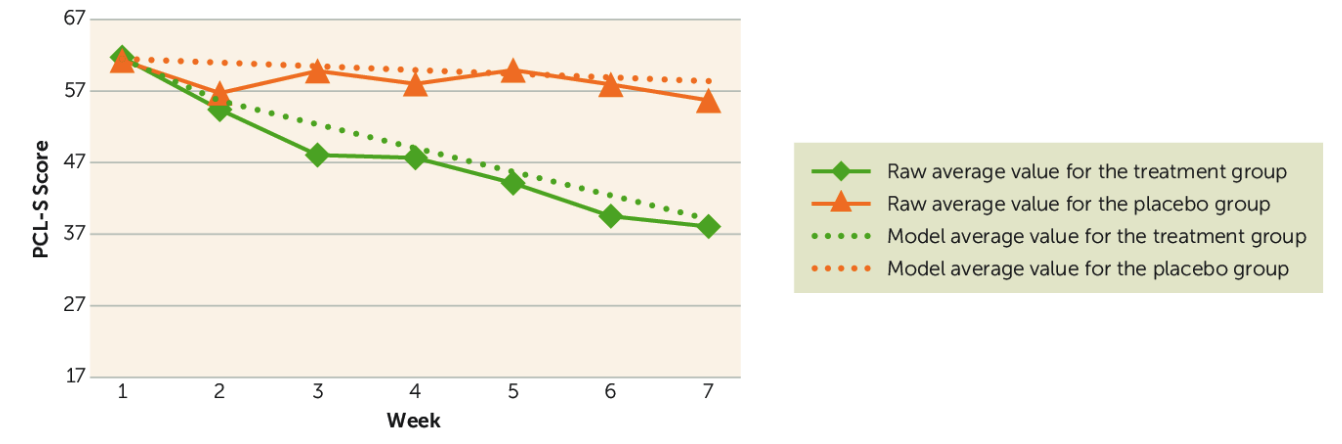
How might NA and cortisol levels be affected in PTSD?
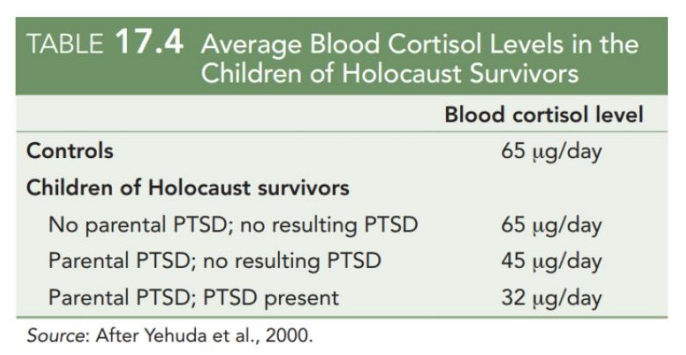
Cortisol and NA levels in PTSD
In veterans + others w/PTSD, NA may be higher with cortisol + CRF lower
Weak cortisol responses to a stressor predict future PTSD
In the treatment of PTSD, increases in salivary cortisol predict recovery
NA levels at baseline are higher in PTSD
changes in baseline cortisol tone = predictor of recovery
Why does this occur?
Amygdala activity is affected by baseline cortisol tone
When tone is moderate
stress responses are terminated quickly, NA levels lower
When tone is weak
stress responses stronger, NA levels higher
certain healthy cortisol level needed for normal functioning
lower cortisol = circuits involved in stress responses may be tuned improperly
baseline cortisol if good but it being too low would mean system responds to strongly and strong stressors go on for too long
NA system in stress
Though we are discussing PTSD here, these findings might apply more generally to many disorders
Early life stress is a risk factor for multiple mental health disorders, and has been correlated with alterations in the NA system
Disrupted NA signaling during adolescence might be associated with long-term consequences in adulthood
so both PNS and SNS in play at the same time, but NA is higher and cortisol lower in PTSD
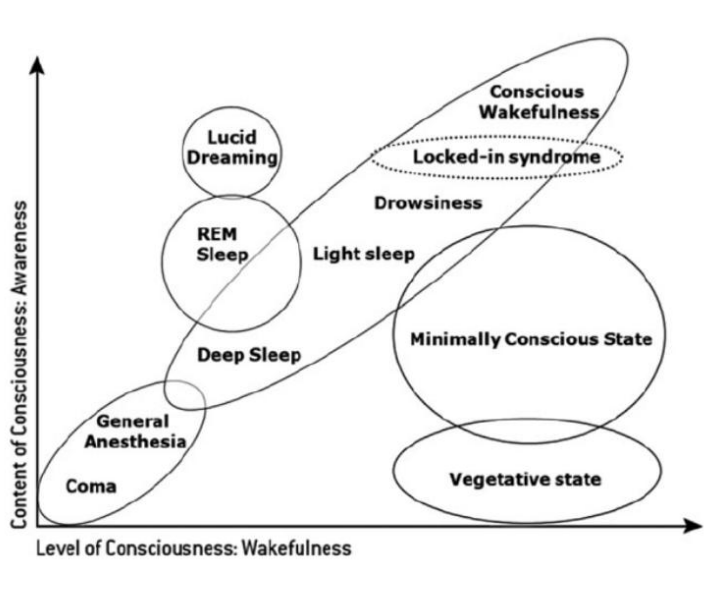
Conscious states
Many states of consciousness might exist. We’re always moving from one to another (e.g. wakefulness to sleep, and from one sleep state to another)
noradrenergic signaling can change as you move between states (like from REM to light sleep to awake)
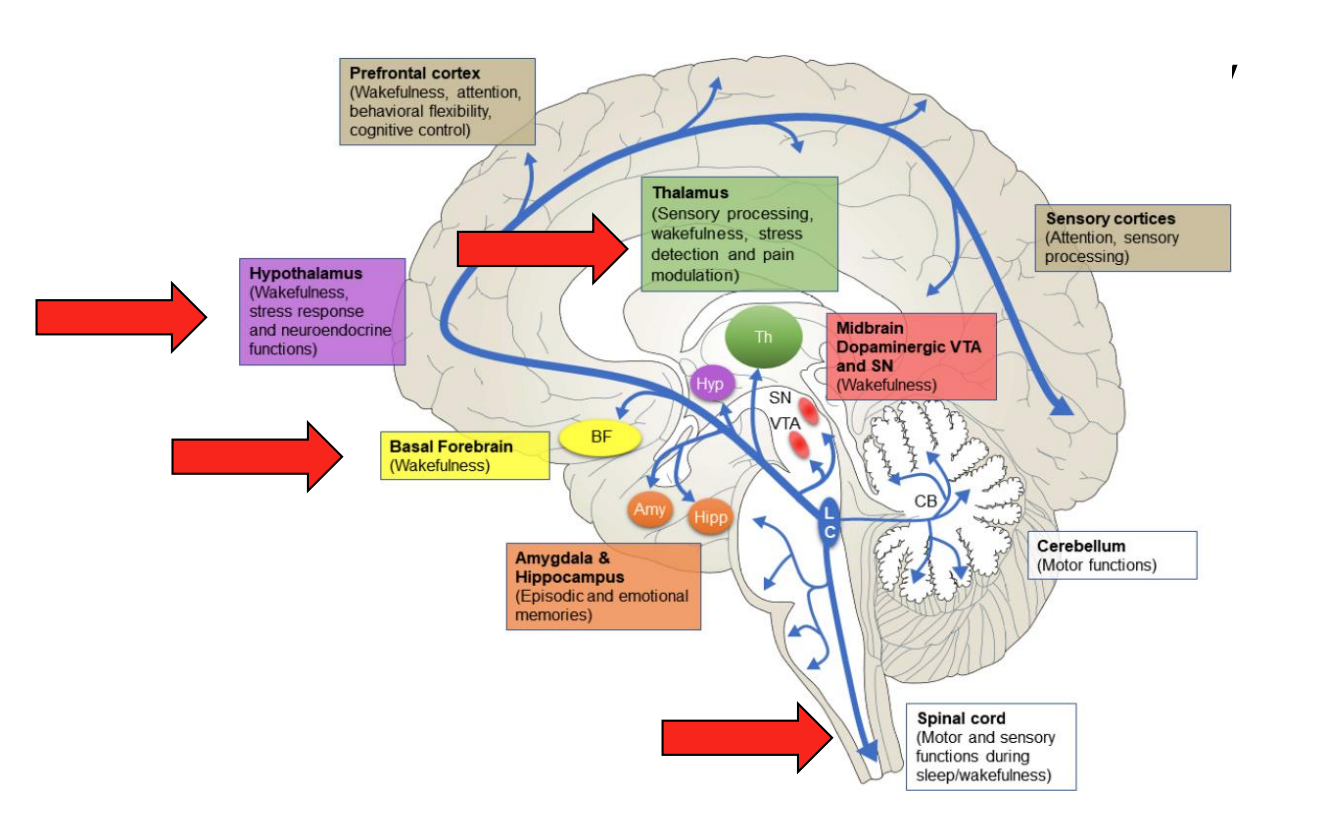
Many functions regulated by NA
different noradrenergic targets
there are potential functions of connections from LC to other brain areas → like wakefulness associated w transitions across diff states
Modulation of arousal
Drugs increasing catecholamine signaling ~ stimulants (e.g. amphetamine - they increase arousal, energy, alertness, etc)
Mimic catecholamine release during arousal, affect sleep-promoting + reward circuits
β1 mutations are associated with familial natural short sleep (also mice)
certain families where mutation is seen that allows individuals to function normally even with less sleep (5-6 hrs)
α1 agonists increase arousal (mechanisms indirect)
Drugs acting on α2 receptors can be sedative
dexmedetomidine (adjunct in anesthesia) inhibits LC
drugs that target these receptors affect consciousness/arousal
LC = major source of noradrenergic innervation → may promote wakefulness → any effect to LC may change wakefulness
Many other signaling systems (and drugs targeting them) might affect arousal. Any guesses?
melatonin, adenosine, etc.
biggest one is acetylcholine signaling (cholinergic signaling)
NA signaling in other states
flow states - state you experience where you are doing well at a challenging activity (time is distorted, you feel fantastic)
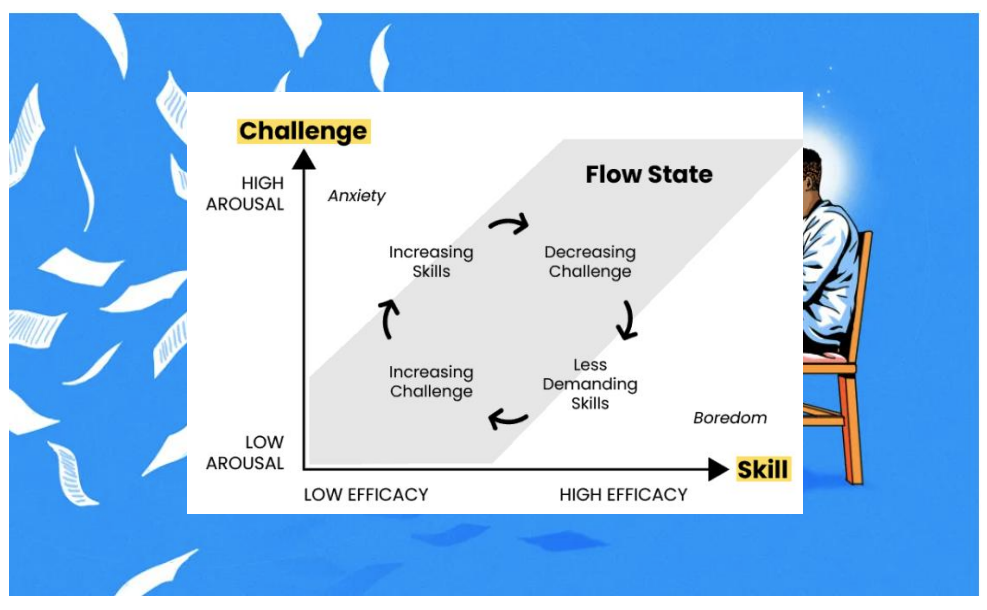
Psychological flow
A subjective experience generated from intense engagement in an activity
Loss of self-awareness, sense of surroundings
Distorted passage of time
Positive valence (i.e. enjoyable)
Associated with performance and well-being
Originally proposed based on expert interviews
Relatively little is known about its neural basis
little known about its neural basis → but might have to do something with noradrenergic signaling
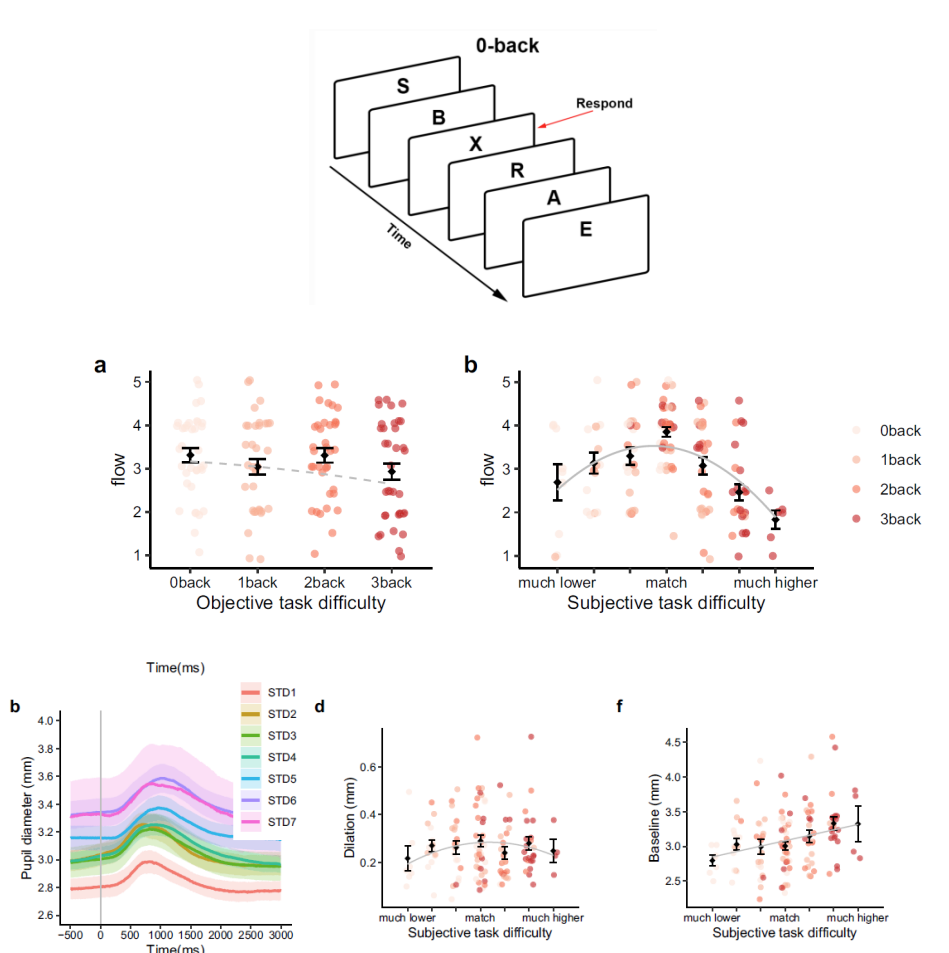
Flow + NA signaling
Subjective flow is related to subjective task difficulty on the n-back
U-shaped
Subjective task difficulty is related to pupil diameter
U-shaped
Pupil diameter ~ LC-NA tone (proxy) and other factors
correlates of noradrenergic are correlated w flow reports
pupil diameter associated w subjective reports
measured both difficulty + measures associated w "flow”
Many functions of NA
function of NA signaling in attention → in PFC + sensory cortices
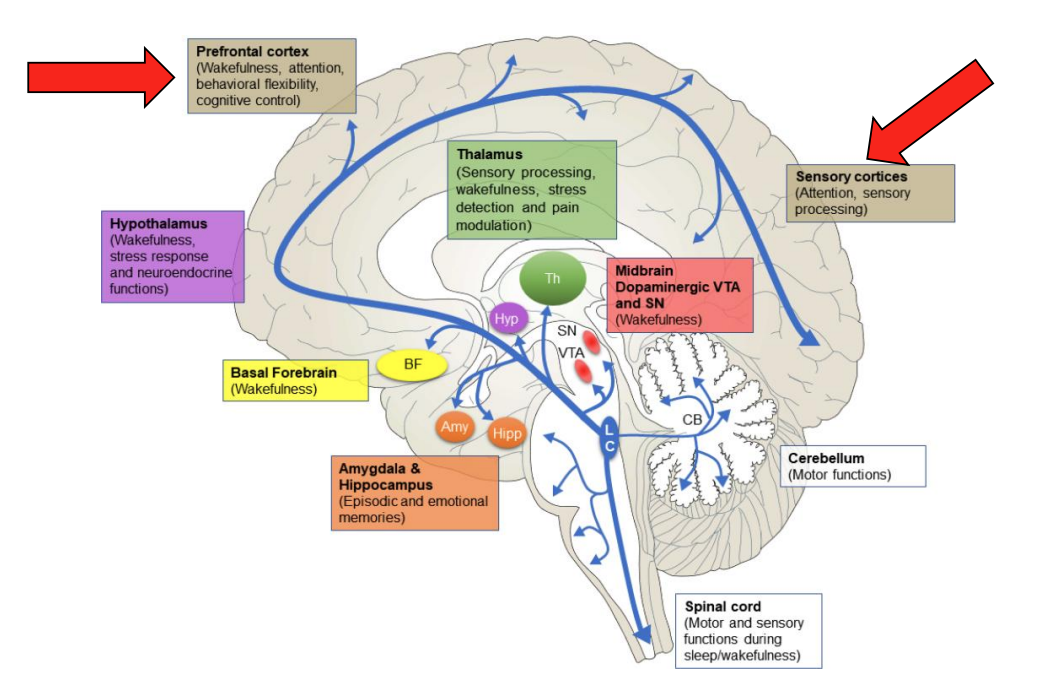
NA and attention
In each environment, we must use the correct cues (relevant stimuli) to guide our behavior
An attentional set is a set of rules used to determine which stimuli are relevant (in the current env)
diff attentional sets across diff envs
As our environment changes, we must shift between attentional sets
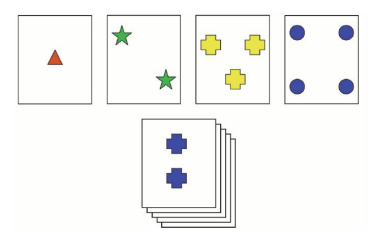
A model of attentional set shifting in humans is the Wisconsin Card Sorting Task
Wisconsin Card Sorting Task
Cards w/symbols varying in shape, color and number
Subjects must sort the cards according to rules
Rules change; set shifting is required to perform
Set shifting is impaired in certain disorders (neurodegenerative disease, depression, SZ + ADHD)
task - sort cards according to rules that will be changed throughout game (shape, colour, number)
this is impaired in disorders
Set shifting involves the PFC…
…and PFC neurons have receptors for NA
Trade-off: α1Rs facilitate set-shifting but inhibit working memory
NA signaling is associated with performance
Reduced NA levels are associated w/impairments
Adrenergic agonists can affect memory performance
Blockers of NA transport associated with improved set shifting
neural basis of set shifting → PFC plays a role (PFC neurons sensitive to NA inputs)
two things to consider: flexibility (shifting b/w sets) + working memory capacity (trade off b/w the two)
people good at shifting may have poor memory
people poor at shifting may have good memory
In ADHD treatment
First-line drugs are stimulants; while these work they have side effects and are not suitable in every case
DAT + NAT blockers (Methylphenidate)
DAT/NAT reversal + release (Amphetamine) → not blockade, reversing how they work
Also non-stimulant drugs → not associated w arousal/alertness (more focused on effects of NA transport/receptors rather than DA transport)
NAT blockers (atomoxetine), ADR receptor agonists (guanfacine, clonidine)
Recently, centanafadine has attracted interest
Blocks NA transport strongly, blocks DA transport moderately
Possibly less abuse liability while still having beneficial effects
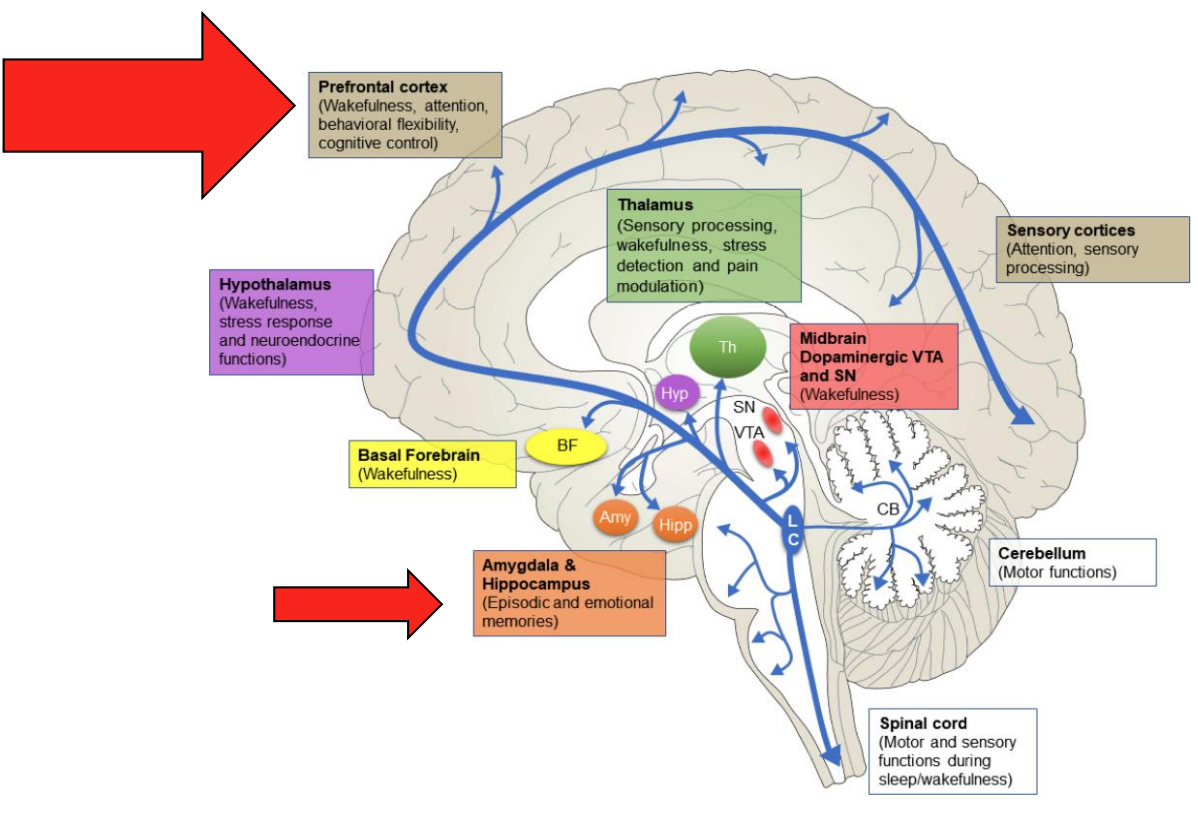
Many functions of NA
NA signaling in PFC + amygdala + HPC
Memory
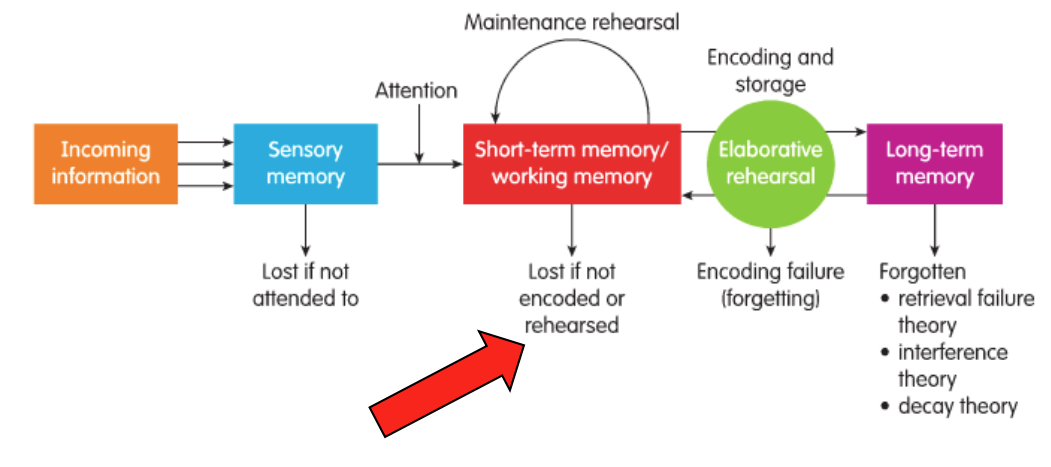
Process whereby information is stored, consolidated + retrieved
Several types (or stores) with different properties: sensory, short-term/working + long-term
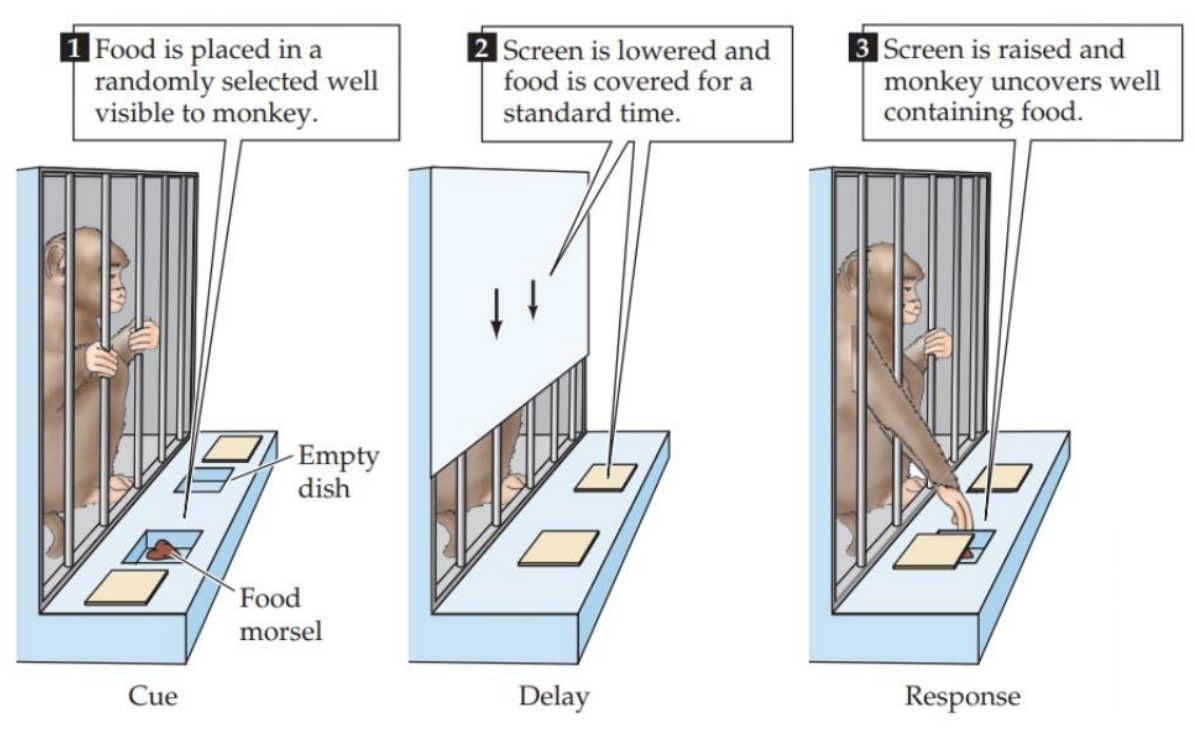
WM test – monkeys (L02)
mild food deprivation leads to strong motivation to perform for food
then shown two wells, one is empty, the other food
wall is lowered over cage and wells are covered → in order to remember where food is, monkey must maintain mental representation of its location
this is delay period across memory assays (period where original stimulus removed and monkey can’t see it, so representation is maintained)
then leave time for response phase
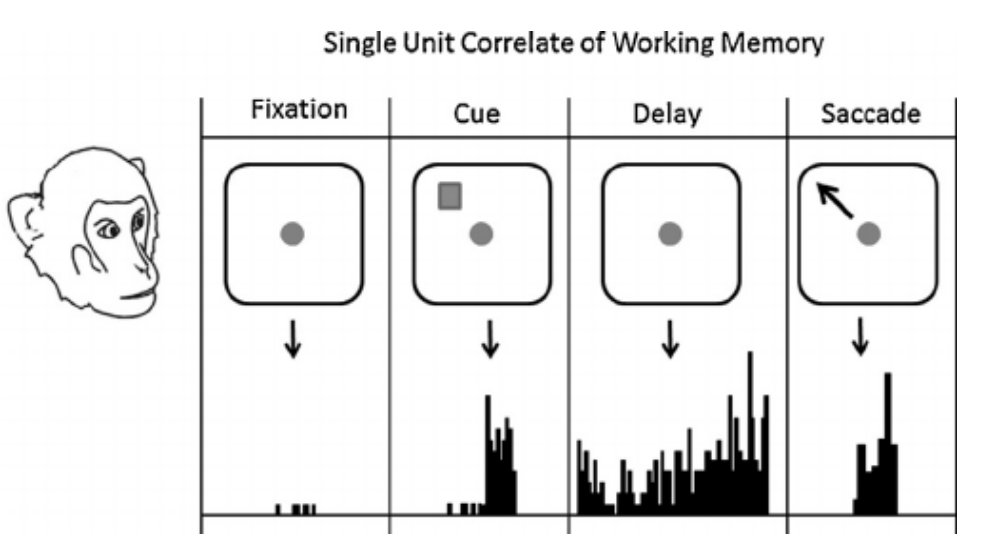
Task-relevant PFC neurons
To complete the task, the animal must maintain a representation of the stimulus (food in well) and focus on the goal (point to well) during delay
PFC neurons might fire during the delay period (task-relevant neurons) and such cells could be responsive to NA stimulation*
there is representation of information in its absence (during delay period) that allows this task to work
PFC neurons still fire even when visuals are removed (they are responsive to NA signals)
How does NA affect memory? Does NA make memory better or worse?
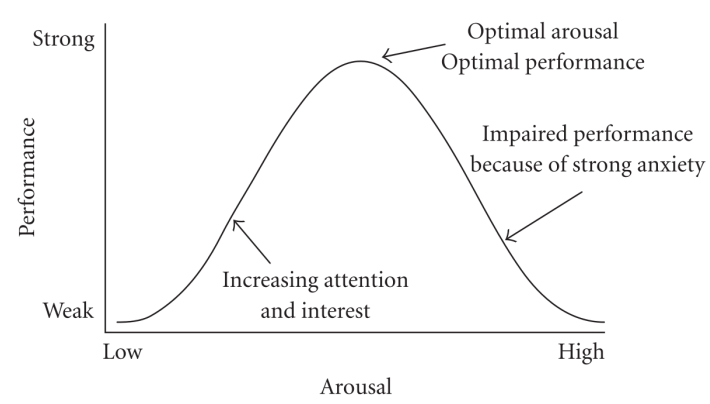
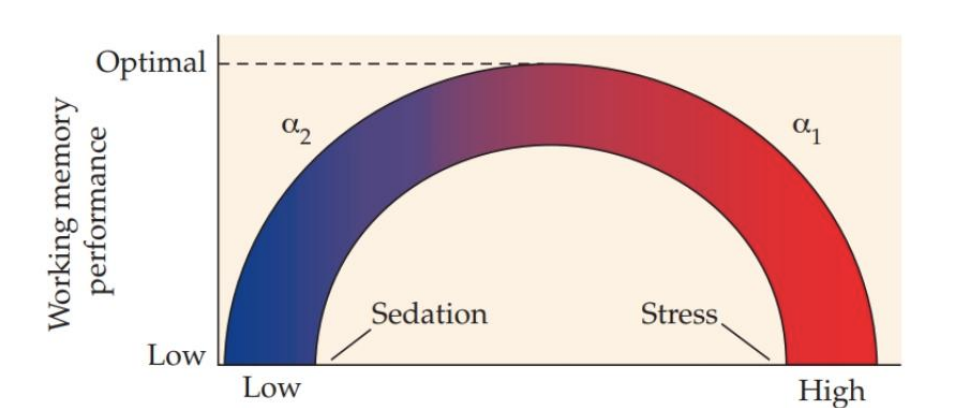
WM and NA and Yerkes Dodson Theory
NA levels vary (e.g. during states of stress/arousal)
In humans and animals, very low and very high NA levels are associated with impaired WM
Moderate NA levels appear to be optimal for WM
If this relationship sounds familiar, it should – you have seen it before!
Inverted U-shaped relationship between arousal and performance also appears to exist for WM
WM + the PFC
The bell shape may be due to receptor affinity
Only weak α2 at low NA levels; strong α1/α2 at very high NA levels
Targeting adrenergic receptors to treat cognitive dysfunction (with aging, in ADHD)1-3 ; many studies focusing on guanfacine
concentration variation matters bc it reflects a pattern + receptor activation
in certain individuals, drugs may be helpful bc they push them closer to a sweet spot where' there’s the right proportion of activation of a1 and a2 receptors
Role in asversive/emotional memories
Memories of arousing experiences tend to be stronger*
We are more likely to remember major events (which are arousing) and major details of these events
Enhanced memory for arousing experiences might involve adrenergic signaling and the amygdala
Amygdala damage impairs fear conditioning
β-adrenergic antagonists in the amygdala impair fear memories
β3-KO mice also show impairments, results in β1/ β2 KO mice more complex
NA signaling may play role in aversive memories
disrupt such signaling in animals w damage to amygdala → we don’t see such strong memories + no fear conditioning
Therapeutic relevance
β-adrenergic receptor blocker (propranolol) in PTSD
Exposure after trauma may lower risk (inconsistent)
If used during memory reactivation, may reduce symptoms
α1R blocker prasozin used to treat nightmares in PTSD
altering emotional character of traumatic memory may be useful in PTSD → target neural basis of memory (target with antagonist + treatment during memory → improvement over time)
study where those who got into accidents got surgery with anesthetic compounds had lower PTSD risk → perhaps the drug affected the likelihood of PTSD
Adrenergic theory of cognition
Many different theories
Effects of NA on memory and attention (psychological processes) are likely the result of effects of NA on neuronal function (physiological processes)
Roles of adrenergic signaling in cognition might exist due to many effects, including energy metabolism, synaptic plasticity + gain control
NA signaling does not just facilitate memory → it may have a role in energy metabolism indirectly, or facilitating synaptic plasticity, gain control (doesn’t just contribute to neural activity)
not as fleshed out theories though
Adrenergic signaling + mood
Many mental health disorders are related to stress
risk of Anxiety, depression and post-traumatic stress disorder goes up w more stressful life events
As part of the effects of stress might be due to NA, ADR and cortisol levels, modulating signaling may be therapeutic
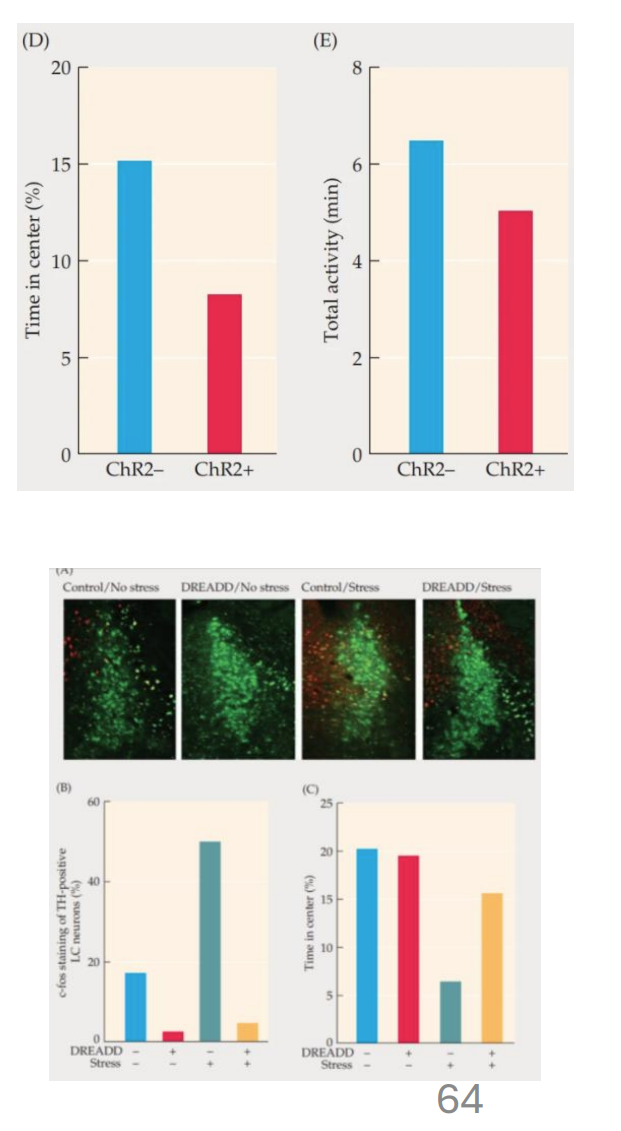
1 – Anxiety
LC activity likely contributes to the anxiety of stress (due to being primary source of noradrenergic signaling)
Activating the LC (e.g. w/optogenetics study) increases anxiety-like behavior in the EPM (see L03)
less active LC cells would show less anxiety
Reduced LC activity with therapeutic drugs (e.g. benzodiazepines, SSRIs and MAOis in some cases)
2 – Depression
Mixed evidence for lower NA levels in depression
Decreases in NA release (also other NTs) (i.e. with reserpine) are associated with depression-like behavior
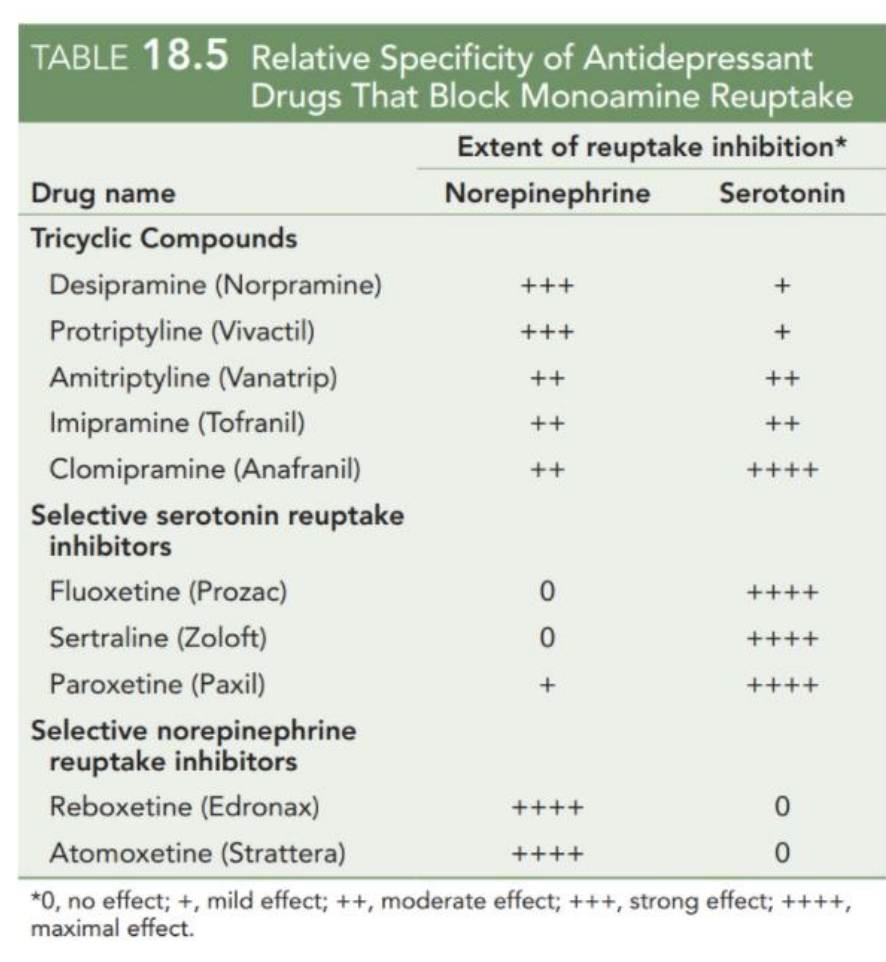
Many antidepressants affect NA metabolism and transport
MAOis + SSRIs
every signaling compound associated w depression in some way
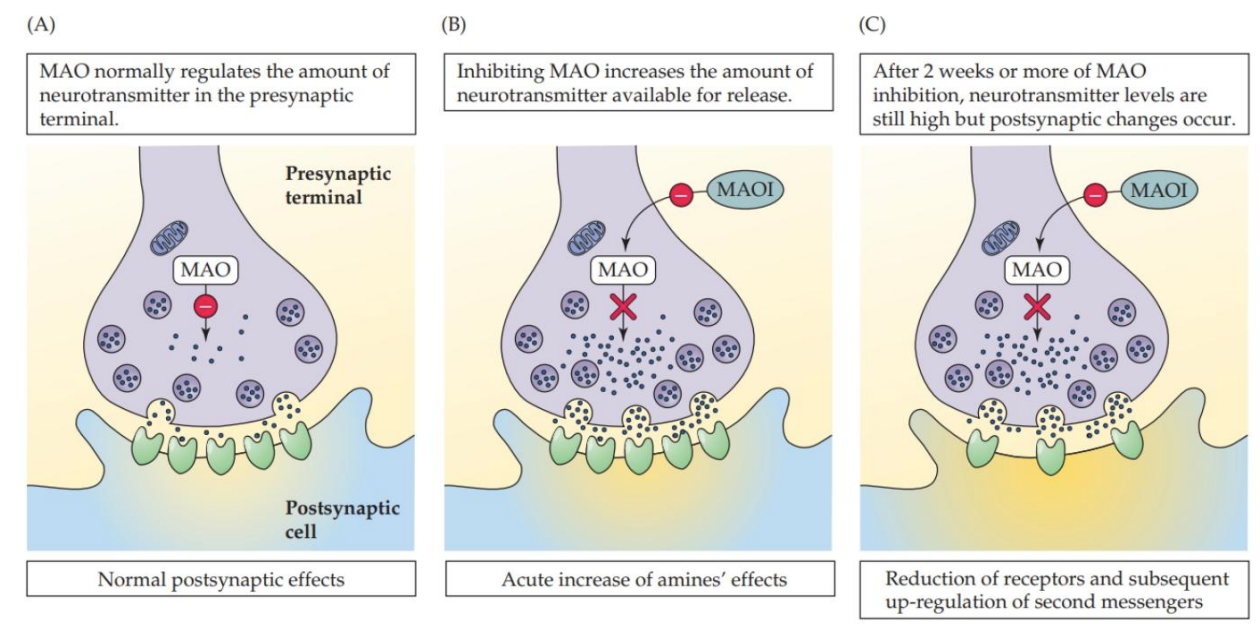
MAOIs + depression
Antidepressant action may require long-term adaptations that take place over several weeks
antidepressants don’t work right away but may involve long-term changes in NS
why not right away - because they slowly change your brain
MAOi → less metabolism → more monoamines → less receptors***
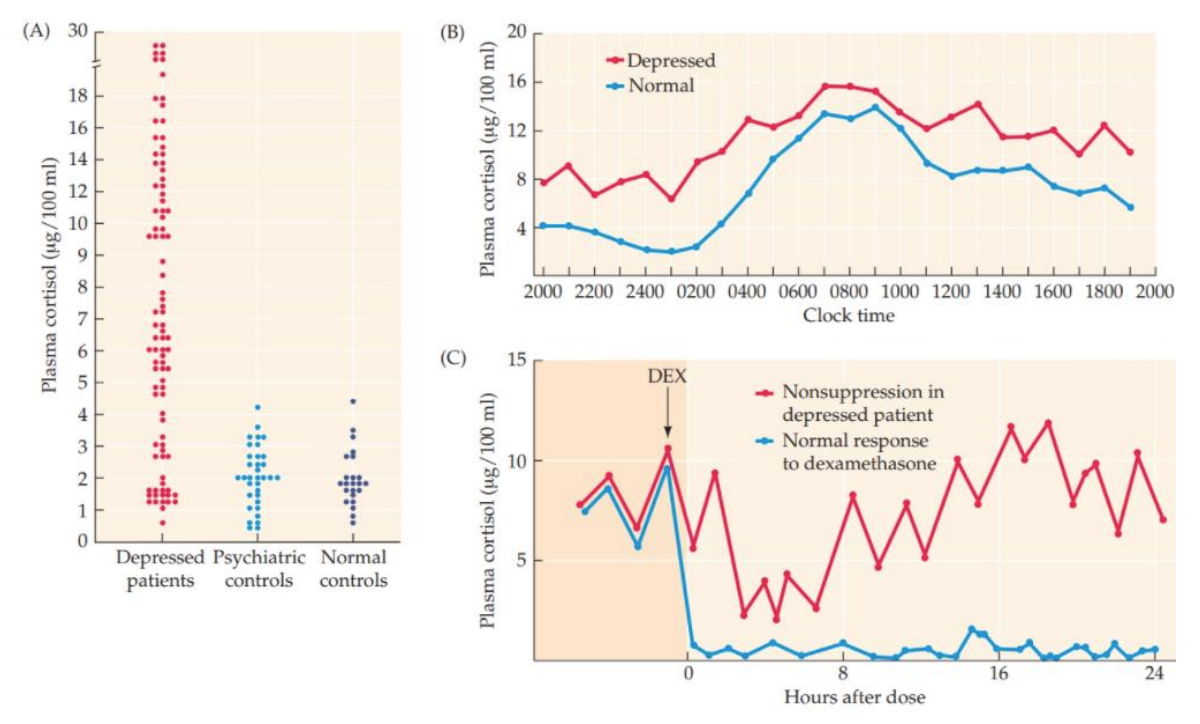
Role of cortisol in depression
higher cortisol associated w depression
can be on exam → describe the association of all NTs with depression
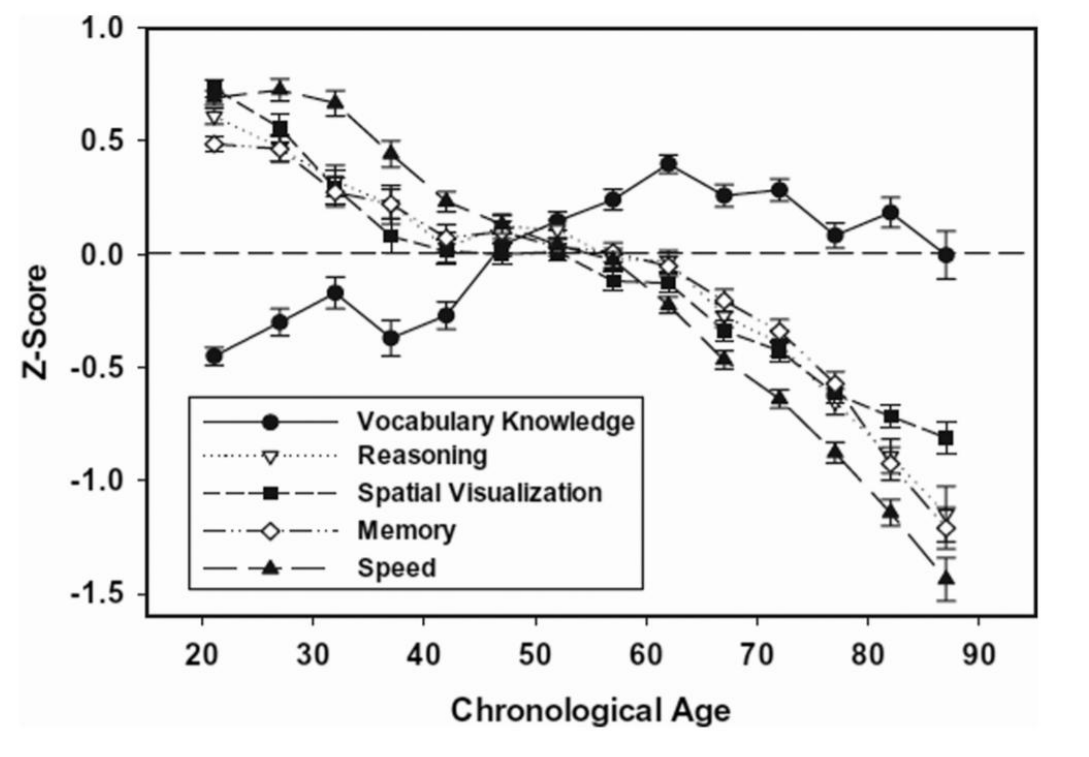
Memory, cognition and aging
cognitive peak likely to come earlier in life
why? noradrenergic changes
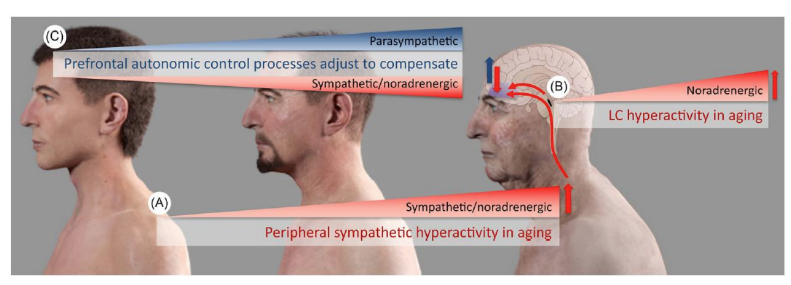
NA system in aging
Early studies suggested a loss of LC neurons w/aging
NA levels are lower with age
These changes may contribute to age-related cognitive decline + disorders such as Alzheimer’s Disease (AD)
Targeting adrenergic signaling may help with cognitive decline and apathy in AD (more on this later)
not usually done, but notably for ADHD where we use drugs to affect noradrenergic signaling to enhance cognition
With aging
Increase in positive emotions + decrease in negative emotions → due to NA signaling
Original theories proposed a role for cognitive control + more
Recent studies propose changes in the CNS (i.e. in the LC) contribute
theory = different mechanisms for cog control develop as you age → how you experience emotions become different