Ectopic Pregnancy
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Definition
Implantation of the fertilised ovum on a tissue other than the normal endometrial lining of the uterus.
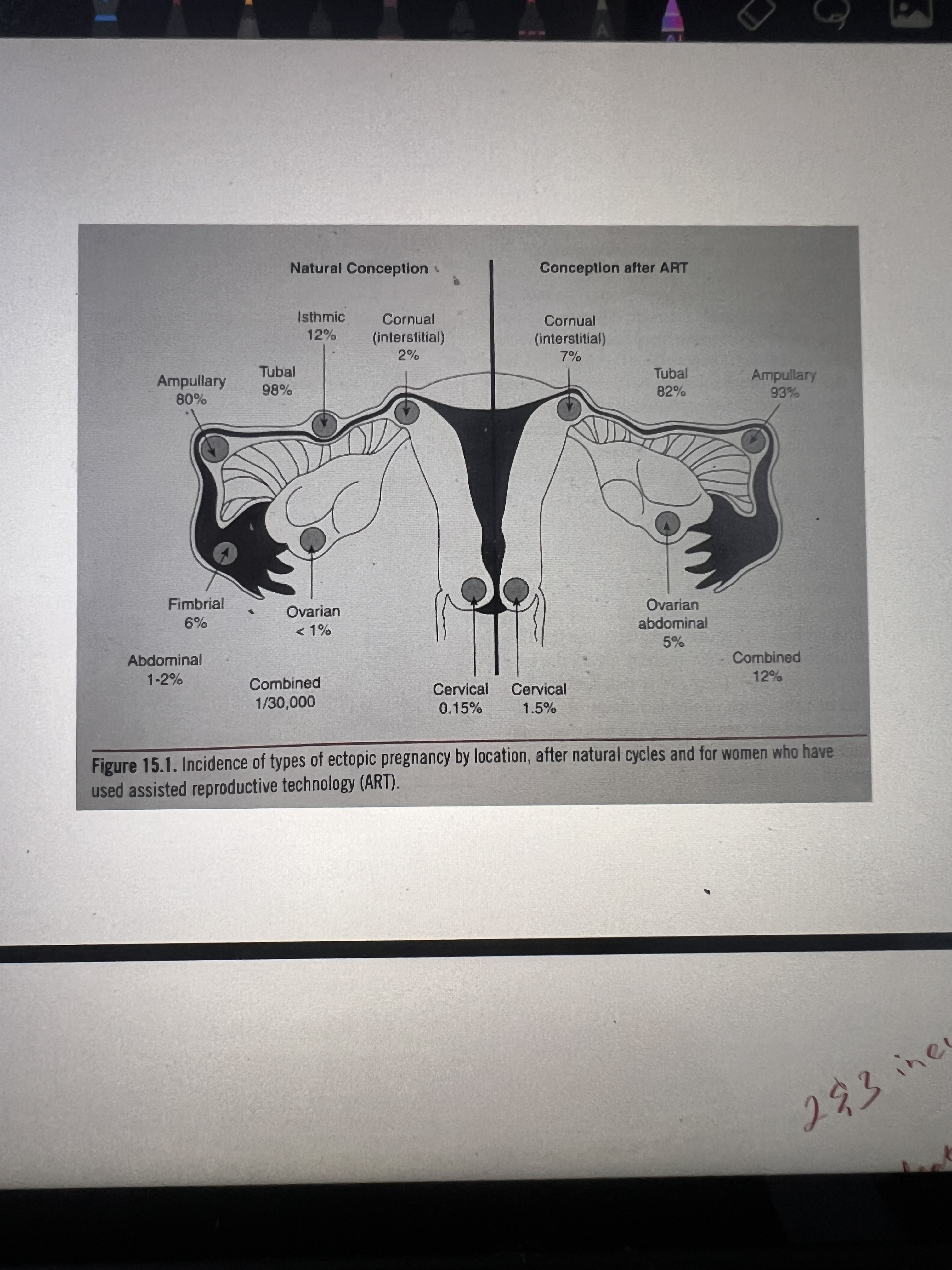
Classification
Risk factors
Previous ectopic pregnancy (? 10 – fold↑)
•PID, salpingitis (Chlamydia and Neisseria gonococcus)
•Previous tubal surgery.
•Age(women 35 -44 years 3x more than women 15 -24 years).
•Assisted reproductive technology like IVF and GIFT when multiple embryos or gametes are implanted into the uterus or the fallopian tubes.
•Heterotopic pregnancy.
Progesterone – only IUCDs: decrease the motility of the fallopian tube
•Previous hx of uterine synechiae
•Salpingites isthmica nodosa
Ovulation induction or ovarian stimulation.
• Recurrent appendicitis
• Cigarette smoking
• in utero exposure to Diethyl stilbesterol
Symptoms
•Pain(abdominal/pelvic, generalized or localized, unilateral or bilateral, radiating to shoulder epigastrium or back)
•Amenorrhoea
•Syncope
•Dizziness
•Pregnancy symptoms 10 – 20 •Nausea 15
•Urge to defecate(blood collection in POD presses against rectum)
• bleeding per vaginum as spotting for up to 10days
•decidua cast shedding
•diarrhea
•jaundice
Triad of symptoms
Abdominal pain
Amenorrhea
Abnormal vaginal bleeding
Signs
varies from asymptomatic
to severe pallor and shock(cold clammy extremities, weak rapid pulse, decreased bp)
Diffuse or localized abdominal mass,supra pubic tenderness,
CET,
adnexal mass
Uterine softening and slight increase in size
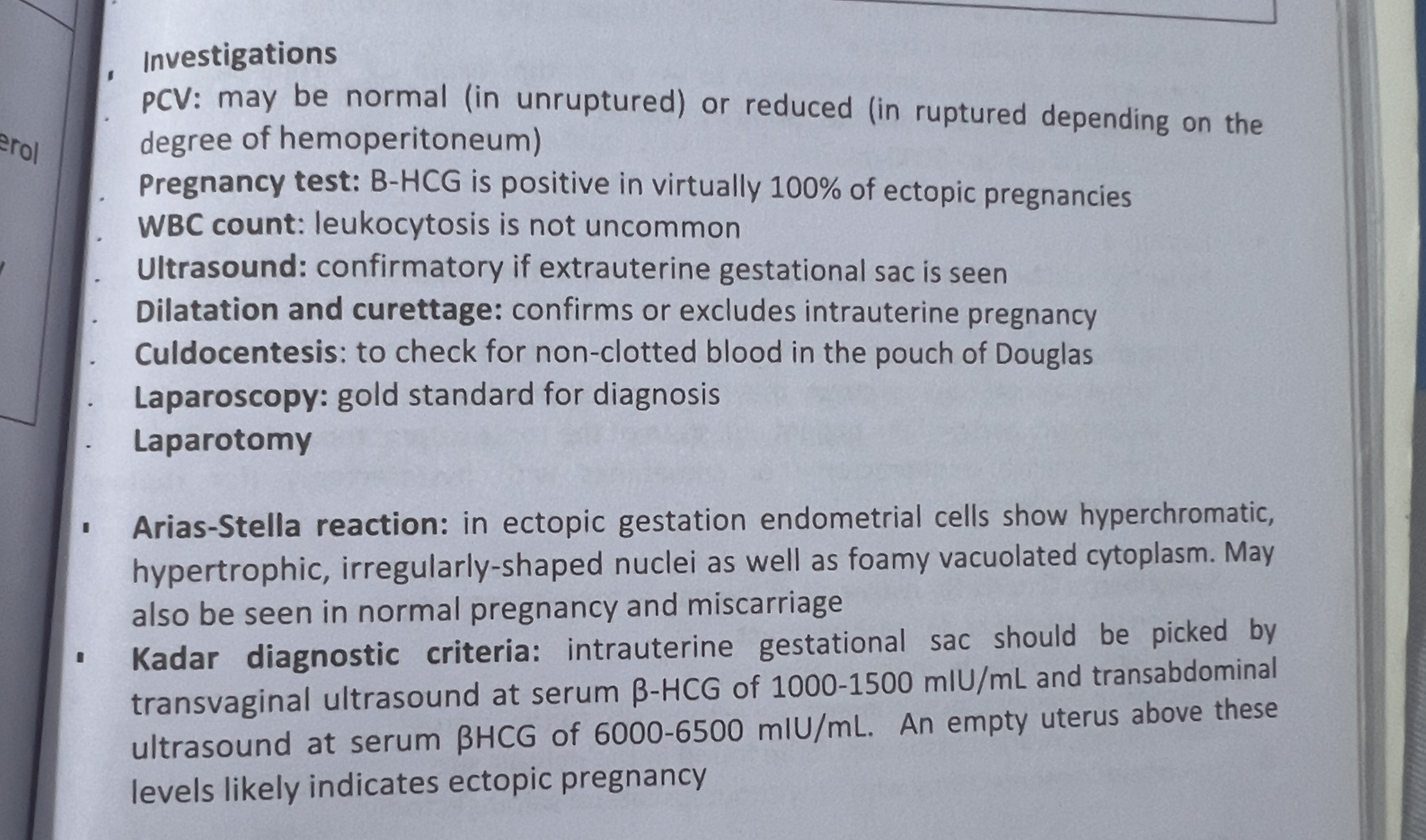
Investigations
EUCr: to check baseline kidney function in case surgery is needed
Blood group and xM: in case transfusion is necessary
time of rupture
Isthmic: 6-8wks
Ampullary: 8-12wks
Interstitial/cornual:12-16wks
DISCRIMINATORY LEVEL
OF BHCG
Significance of above
What is it called?
>6,500 miu/ml –gestational sac should be seen for transabdominal scan.
•> 2,500 miu/ml for trans vaginal scan.
Bhcg levels above discriminatory zone with empty uterus suggests ectopic pregnancy.
Kadar diagnostic criteria
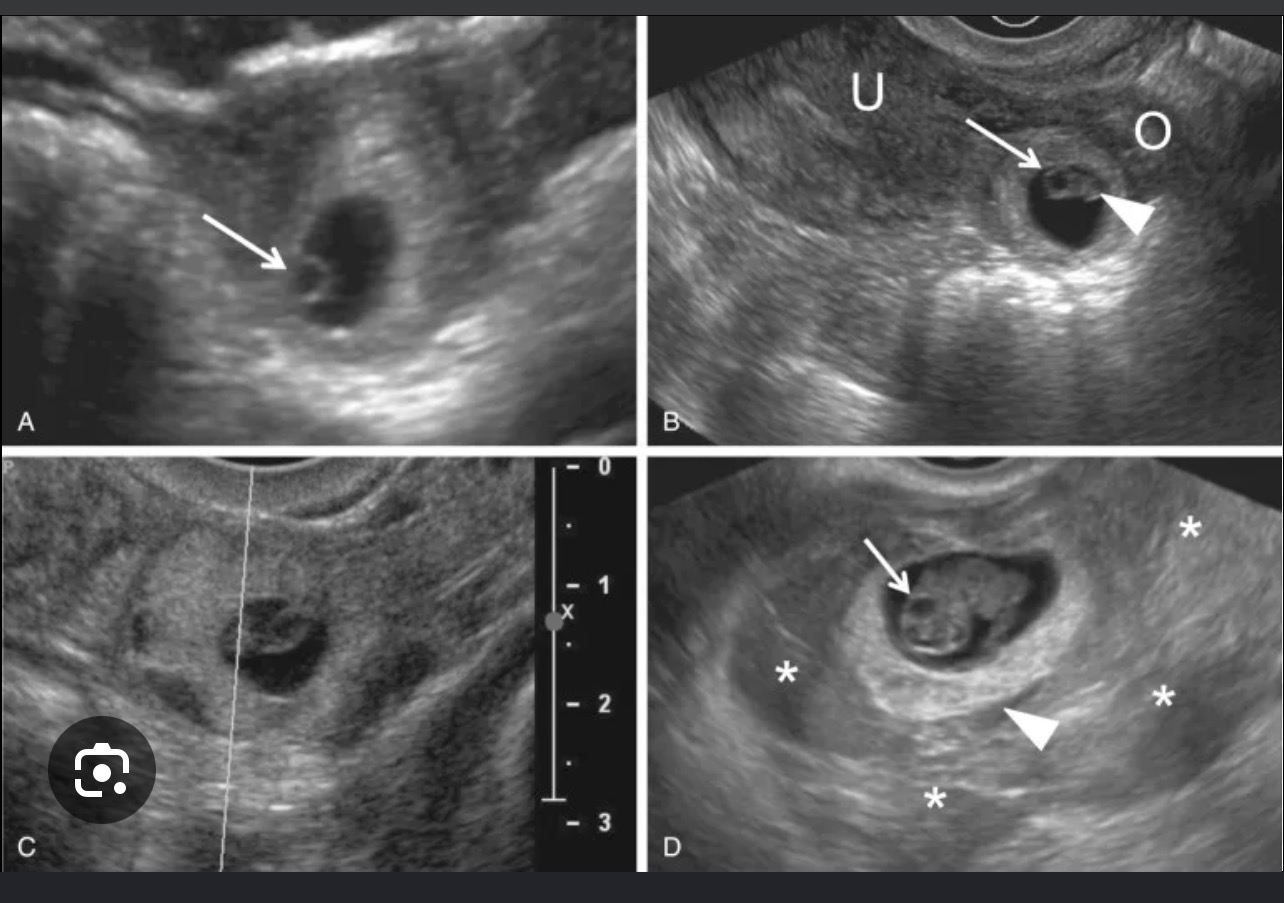
U/S findings for ectopic pregnancy
Unilateral mass
•Fluid in the pouch of Douglas
•Absence of a well-defined gestation sac/fetus in the uterus.
•Presence of fetal cardiac
U/S findings for ectopic pregnancy
Unilateral mass
Extrauterine gestational sac with/ wO live embryo(bagel’s sign)
•Fluid in the pouch of Douglas
•Absence of a well-defined gestation sac/fetus in the uterus.
•Presence of fetal cardiac
Treatment modalities for unruptured
Treatment for Ruptured
Expectant mgt
Surgical mgt
Surgically administered medical mgt
Medical mgt
Resuscitation
Definitive treatment(laparotomy and salpingectomy)
Indications for expectant mgt
•no sign of intra uterine Pregnancy
•Falling BHCG levels at 2-day intervals
•<4cm diameter of ectopic preg
•No sign of rupture or active bleeding.
• hemodynamically stable
•
Substances used for SAM
Drugs used for medical mgt
Systemic methotrexate 1mg/kg body wt IM
Actinomycin D
Mifepristone
Contra Indications for medical treatment
Haemodynamic instability
•Free fluid in POD or pelvic pain
•Known sensitivity to methotrexate
•Non – compliant patient
•˃3.5cm diameter with positive fetal heart motion.
•Liver, pulmonary and renal diseases, peptic ulcer patients
•Immunodeficiency
Indications
Clinically stable
Ectopic mass <3.5cm without cardiac activity
HCG is positive after salpingotomy(persistent ectopic pregnancy)
Absence of contraIs
Surgical treatment and surgical procedures
Laparotomy or laparoscopy
Linear salpingotomy: the procedure where the pregnancy is removed from the tube through an incision on the antimesenteric border
Prevention
•Comprehensive education: •Effects of sexually transmitted diseases, smoking, drug use and douching, unsafe sex
•During preconception counseling, the woman can be screened for predisposing factors to ectopic pregnancy
•reminded again of the signs and symptoms of ectopic pregnancy.
••Before any reproductive procedure, such as tubal ligation, the woman should be informed of the increased risk of ectopic pregnancy.
Spiegelberg’s criteria for ovarian pregnancy
Treatment?
Fallopian tube on the affected side is intact
The gestational sac must occupy ovarian position
The sac must be connected to the uterus by the utero ovarian ligament
Ovarian tissue must be identified histologically in the wall of the gestational sac
Oophorectomy with/ without ipsilateral salpingectomy
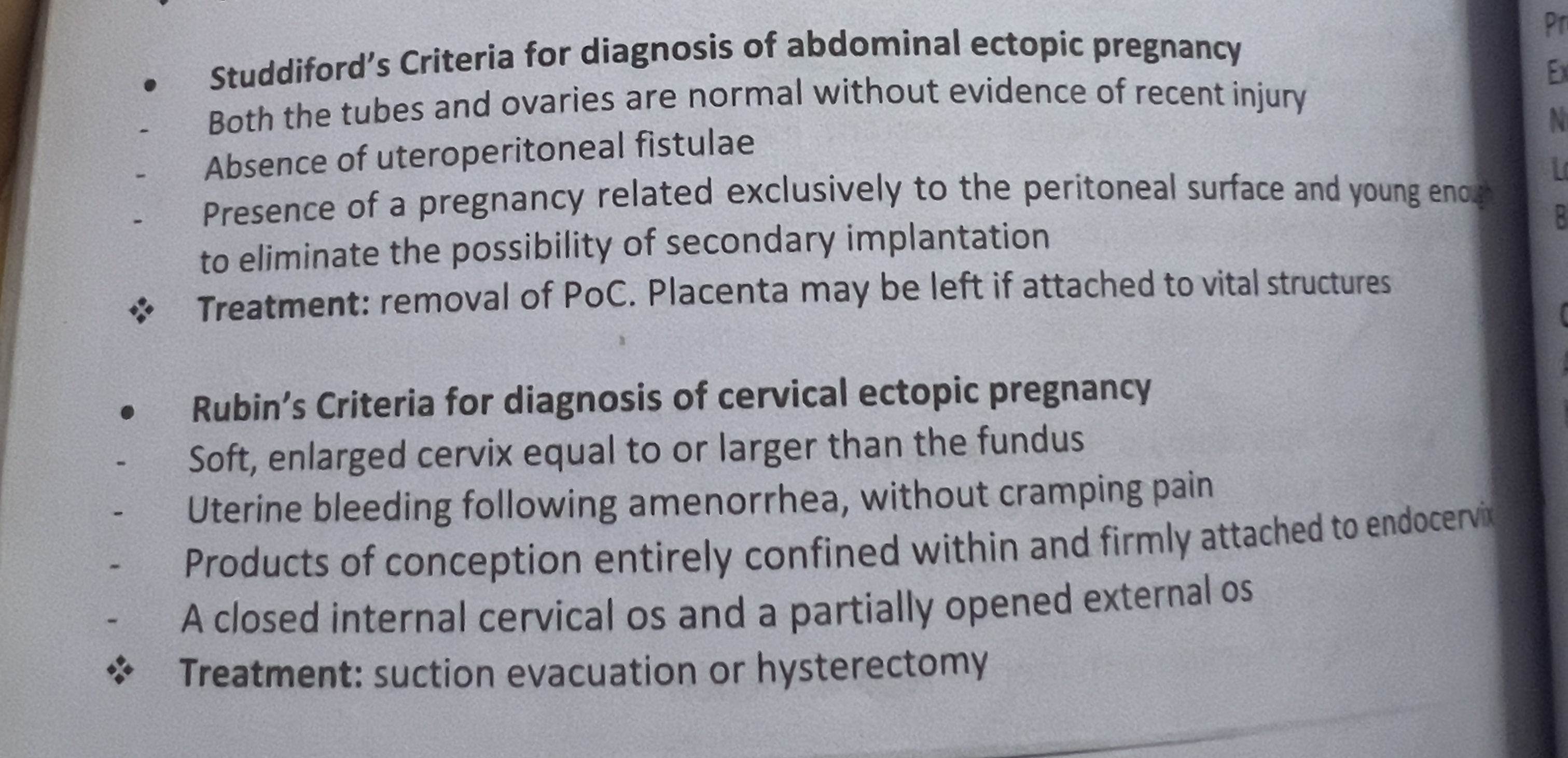
Studdiford criteria
Rubin’s criteria