Quiz 2 process and skills (copy for help)
1/149
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
150 Terms
Using countertransference for insight- CO is disengaged
Might come to realize that the client is highly disengaged emotionally... They intellectualize & don’t really talk about their central concerns...
Using countertransference for insight- CO is highly empathetic
Might feel urged to reassure clients a lot & validate them... Might overestimate how much they are helping or connecting with the client & stop checking in or evaluating progress.
Interpretations
Goes beyond the client’s words that are overly stated & presents:
-New meanings
-Reasoning or explanations
-Context for understanding thoughts, emotions, behaviors
-Problems presented with new perspective
Interpretations and empathic conjectures
Names the confusing experience
•Decrease distress over confusion (why do I do this?)
•Gives conceptual framework for clients to try on & see if it brings them clarity
•Offers a rationale for behavior, thoughts, emotions – normalizes it
Helping stone for clients
•Helps clients with lower emotional intelligence or self-awareness
•Provides a spark or launching point to explore further
•Ensure you give power back to clients by letting them mold your interpretation (“Or something like that, you tell me.”)
Using Reflections to Highlight Meaning
Clients speak without realizing what they’re implying
In this case, use reflections to pull forward underlying emotions or meanings to build awareness
Grounds for Interpretation
Themes
Patterns
Connections
Defenses
Conflicting or Puzzled Reactions
Examples – Past Influences Present
•“Last week, you mentioned that your relationships drift apart after a month or so, and today we’ve explored your past experiences of rejection and betrayal of close friends. I wonder if you break up with romantic partners so that you don’t have to risk intimacy and getting hurt.”
Examples – Defense mechanisms
•“As a child, you learned to not draw attention to yourself because that drew ridicule from others. Now, I see you receding to the background with your friends. Is this attempting to preserve the relationship? Protect you from harm? How does your withdrawal function in your relationships?”
Using Therapeutic Control
1.*Leans forward, raising a hand for attention. “Can we slow down a bit? I think we’re touching on something important.”
2.“Hold on a moment. If you’d be so kind, I’d like your help with something. I’m noticing that I’m struggling to get on the same page with you. How do you feel?”
Immediacy
•Self-disclosure of personal reactions or perceptions
•Directing client’s attention to what they think/feel in the moment
•Process Statements: Asking how the client perceives the counselor right now OR asking clients how they think the counselor is perceiving them (in the moment)
•Drawing Parallels
Immediacy examples
•“Sometimes, I feel like we don’t get anywhere useful in here, like we’re not digging deeper into your experiences.”
•“What do you notice your mind doing right now?”
•“I wonder how do you feel about being assigned to me as your counselor?”
•“You mentioned not feeling heard by anyone. I wonder, how do you feel in here with me?”
Insight Stage Caveats
Not Wanted?
•Not all clients are looking for insight.
•May just want a relaxing space to share whatever they want.
•May just want coping skills, no deep insights
“Perfect Insight”
•Therapists place too much pressure on self to find the perfect insight.
•Working harder than the client (lack of collaboration)
•Power Over vs. Power With
Cultural Misses
•Cultural differences or misunderstandings
•Imposing values
•Forgetting to explore culture (lack of attending to culture)
Excitement & Momentum
•Getting useful insight should be a boost – giving momentum to change.
•Therapists can be overly excited by finding insight that they MISS clients (too far ahead)
3 questions clients need to answer after seeing a path for change-Used to Assess Readiness for Change
“Can I do it?”: Do I have the Ability?The Time?The Knowledge The Resources to Change?
“Will this work?” Will this help me achieve my goals? Will it result in lasting change?What would stop me?
“Is it worth it?” Is reliving trauma to heal worth the pain? Is admitting my flaws going to be worth it in the end?
Ask Clients their Current Understandings...Collaboration with Clients is Key
•Let them summarize & cement the insight.
•Let them give voice & express the insight, heighten the emotionality of it.
•Let them own it.
Confrontation and resistance
in the middle of difficulty, lies opportunity, for there is no progress without honest confrontation
Confrontation & Challenging
Come alongside clients to help them see:
1) unhelpful thoughts or emotions
2) discrepancies & contradictions
3) rigid behavioral patterns keeping them stuck
4) Defense mechanisms
assessing questions
1.What is the client not willing to acknowledge?
2.What’s their hard to swallow pill?
3.What hope are they clinging to, despite what their experiences are telling them?
4.What are they avoiding?
5.How are they keeping themselves ignorant?
6.What feels disjointed, not integrated? Overly simplistic & lacking nuance?
Doors clients do not want to open
1.Their father/mother cannot provide the nurturance they seek
2.Anxiety & depression will likely not go away for forever
3.They are non-consciously contributing to their problems
4.More coping skills won’t heal the deep pain inside
5.Forgiveness is the path to healing, not resentment
6.you cannot heal trauma without feeling it’s effects
Kinesics:
Arm/Leg movements
Emblems:
Substitutes for words (wave)
Illustrators:
Accompany Speech (measuring a fish)
Regulators:
Monitor the conversation flow (head nod
Adaptors:
Habitual acts, often done non-consciously (head scratching)
Exploration to Insight: Cognitive Focus
-Looking to slow down the process
-Help clients think through their situations gain objective explanations
-Give opportunity to talk about the different pieces in warm, nonjudging relationship
-Sift through information, looking for connections and new meanings
Exploration to Insight: Emotion Focus
-Looking to slow down the process
-Help clients acknowledge & express their emotions à creates personal involvement & responsibility in clients
-Give opportunity to talk about painful experiences in warm, nonjudging relationship
-Unaccepted feelings often “leak out”, sometimes in destructive ways.
Confrontation gives ____
clients clarity, And it helps reduce the incongruence between the experience and the outward communication
when you should challenge a client
•When it would increase awareness that relates to therapeutic goals
•When client awareness is lacking, and this is an obstacle for growth
when you should not probably challenge a client
•When it’s more about you than the client - stems from your own bias, history, defensiveness, etc.
•It’s not therapeutically relevant or would be a hard shift in the therapeutic agenda.
•Don’t have rapport yet or would set up a major power struggle.
Clients are likely to be ____
“resistant” & express some form of “resistance”
Defining Resistance
1) Any covert or overt opposition to the therapist, counseling tasks, or goals (internal view of resistance)
2) A negative relational dynamic that chafes or disconnects the client & therapist (interactional view of resistance)
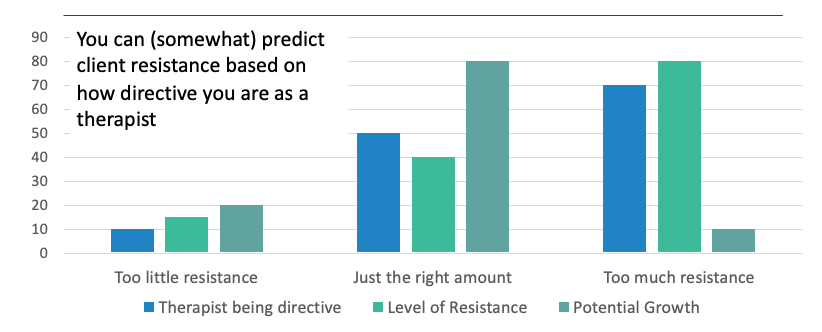
Moderate levels of direction & resistance is best
Understanding Resistance
1.If we feel stuck – where are we suppose to be going?
2.What’s our goal again? Would the client agree this is our goal? Is this goal made clear to both of us? Could we both articulate this goal?
3.is the problem reframed into a SOLVABLE problem?
1.Person, Place, & Time Specificity?
2.“Don’t want to be anxious” – not solvable
3.“Stay calm & be assertive when talking to my boss about my schedule” – a solvable problem b/c it specifies Person, Place, & Time.
IS THIS AN EMOTIONAL RAW SPOT? AM I IRRITATING THAT RAW SPOT? HOW COULD I PROCESS OUR INTERACTION?
Explore the Resistance with Clients
1.Are the pathways forward scaring the client? Viewed as “too painful to go on”? Does the client fear…
1.They won’t be able to function?
2.They won’t be able to stay safe (suicidal ideation)?
2.When we talk of change, is there an unprocessed emotion attached to the change? Are my actions irritating that emotional raw spot?
3.What’s the function of the resistance? Is there a pattern of this?
Possible sources of resistance
-Fear of failure, pain, abandonment, etc.
-Transference (therapist represents a conflict – enacted with passive-aggressive resistance)
-Client fees shamed b/c they haven’t been able to resolve their problems
-Client is exhausted (psychological fatigue)
Personality disorders (enjoy manipulation)
Resistance as Cultural Resiliency
A struggle to connect could be related to cultural differences.
Resistance may actually be a form of cultural resiliency that has protected the client from discrimination, helped them endure, coping mechanism.
If suspected – broach culture.
“Sometimes, I struggle to connect or feel like I’m on the same page with you, and I wanted to check in about that. Specifically, I’m wondering if this may be related to me being a white male. What are your thoughts?”
Resistance as Cultural Resiliency pt 2
1.Note: the field has moved away from suggestions of broaching culture with simple acknowledgements of seemingly phenotypical differences (e.g., I’m White – you’re Black, what do you think about that?)…
2.…or highlighting similarities… the main suggestion now is to dive deeper into your intersecting cultural identities (and the client’s) – connecting this to experiences of power, privilege, & oppression.
Addressing Resistance
1) Play dumb – clients can’t resist if there’s nothing to push against.
- What are your reasons for drinking? <makes case>
- I don’t know of anything that could replace the benefits of drinking <client explains all the issues drinking causes>
2) Tap on client values & the emotional energy needed for the motivation to change
- Empathic reflections
- Exploring underlying values for the change
3) Go back & connect more with the client’s perceptions
- What are other people doing to the client? How are they treated?
- What unreasonable demands are placed on them? How are they made to feel?
NOTE: empathize with clients but don’t collude & co-create a sense of victimhood
4) What’s their experience telling them?
- Have you been successful?
- Is that narrative about yourself helpful in motivating you to change?
Addressing Resistance (poorly)
1) Being the change expert – clients will resist.
- What are your reasons for drinking? <makes case>
- Drinking has a list of consequences therapist presents info <client says, “yeah, but…”>
More quick tips
NO EXCESSIVE QUESTIONING
•Empathic reflections > Questions
•Dialogue without questions.
•Reflect the underlying emotions or unmet needs
•Reflect the values of the client
TREAT RESISTANCE WITH RESPECT
•Can’t argue or convince a client to change.
•Respect & understand the reason they are resistant to opening the door, getting started, or staring TRUTH in the face.
FOCUS ON DETAILS
•Details of a client’s situation create options for new action
•Process a client’s situation from a depth that has yet to be explored.
•Express less expertise the more resistance you encounter.
Common Insight Obstacles
1. The unreliable client
2. Client who rejects every coping skill & solution
3. Too talkative (surface level)
4. The client who blames everyone else
Confronting Unreliable Clients
How it looks: They are late, don’t follow up on homework, cancel last minute, etc.
-Establish a clear policy. Be transparent about the actions YOU will take if client is unreliable. Include informed consent on consequences, as well as explore the benefits of sticking it out.
-Stick to your established boundary. Enforce the rule. Clients do better when they perceive value in the session time.
-Be kind and assertive. Speak with sympathy and stand your ground.
Confronting Clients who Reject Solutions
How it looks: Rebuff every suggestion for coping skill, say they’ve tried that already (and it didn’t work), like to talk a lot & complain frequently
-Reframe the resistance as a stage of change. They are contemplating the idea of change & not ready to make changes just yet.
-Set realistic expectations. Instant transformation is a myth. Most of the work happens between sessions. There are ups & downs.
-Address the underlying emotions of change. Speak to the fear, the despair, the missing out on life, the shame of not being able to change…
Confronting Too Talky clients
How it looks: Conversation is mostly absent of emotion, lots of story-telling, surface-level insights
-Meet client where they are at. Adjust your therapeutic ambition. They may not be ready for deeper insights. This can still be meaningful to them
-Try being more vulnerable. Role-model self-disclosure of vulnerable emotions, then turn it to the client.
-Re-examine the goals of therapy. Take therapeutic control & share your insights about how therapy is going. Is this the kind of therapy they want? Or is there more to explore & they need to be pushed?
Confronting clients who blame everyone
How it looks: Exasperated with others, shift blame, vent a lot, make excuses for their behavior, low insight
-We all do it. Acknowledge that this is uncomfortable & that we all universally lean toward easy explanations vs. hard looks at ourselves.
-Unveil the impact. Keeps client stuck. Erodes the trust others have for the client (when they always blame others). Protects them from pain.
-Slow, small steps. Guiding clients to be more introspective requires finesse. Use curiosity often à “I notice that” or “I’m curious about”
THE JOURNEY OF INSIGHT
•Focusing on influencing skills of:
•Interpretations & Metaphors
Which can “map out possibilities for change
WHY INFLUENCE CLIENTS?
influencing skills (top of triangle)
•Info Giving
•Directives (take a breath, tell me more, slow down)
•Interpretations & reframes
•Self-disclosure & feedback
•Challenging
Responding skills (middle of triangle)
•Summarizing & Paraphrasing
•Reflections & Questions
•Encouraging client observations
•Minimal encouragers
Attending skills (bottom of triangle)
•Vocal tone & Pacing
•Verbal Following & Tracking the story
•Culturally appropriate eye contact
•Open, approachable body language
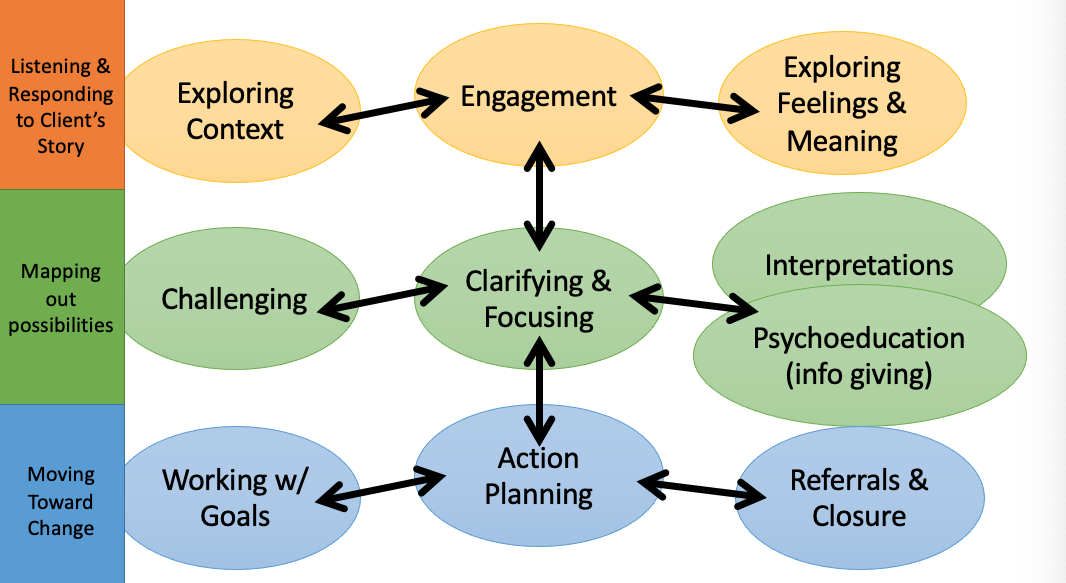
flow chart
INTERPRETATIONS (POSSIBLE EXPLANATIONS)
•Interpret TOGETHER
•Offered vs. Given
•Clients trust you
•High levels of experiencing
•Give new energy & grounds for exploration
VARIATIONS OF INTERPRETATIONS
•The Connector – How does [Point A] relate to [pattern]
•Reframes
•Self-disclosure + “How does that relate to you?”
•Metaphors with a meaning + “How does that relate to you?”
•THE CONNECTOR
•“In this discussion about your continuous frustration & forgiveness of your partner’s drunkenness, I find myself reflecting back to how this relates to your continuous frustration and hurt with your father, namely the lack of nurturance there. Is this a coincidence or something to explore further?”
VARIATIONS OF INTERPRETATIONS
•THE REFRAME
•“Apart of me sees that forgiveness is totally healthy in a relationship. But, that’s with the understanding that the relationship itself is healthy. In your case, I’m wondering if forgiveness actually keeps you stuck in an unhealthy relationship.”
VARIATIONS OF INTERPRETATIONS
•THE SELF-DISCLOSURE
•“Awhile back, I learned something about myself that might relate. I realized a friendship I had was lop-sided. I was frequently disappointed, frustrated… and then I realized I didn’t want to let go of the friendship because of two reasons. One, I had been raised to never give up on someone. And two, I didn’t have anyone else like this friend and I was scared ofbeing lonely. Is there something similar going on here, or am I way off?”
FRAMEWORKS & EXPLANATIONS
•Cultural & Social
•Biological & Medical
•Developmental Stage
•Existential & Spiritual
•Past influencing Present
•Counseling Theories
•Defense Mechanisms
CULTURAL & SOCIAL
•Minority Stress Theory – Understanding internal psychological distress as a product of external discrimination & marginalization
•Recognizing messages around masculinity & femininity as influencing behavior (fit this box & feel distress if you don’t)
Developmental Frame-interpretations
“See if this helps makes sense of things. You’re 19-years-old, in a new place, living independently for the first time. Seems to me like a prime spot for exploring who you are & what kind of adult you want to be. I mean, those are some lofty questions to answer! What if your anxiety, though unpleasant, is largely connected to answering these big questions about yourself and who you want to be?”
Biological Frame
“Anxiety shows up in the body, right? It’s a rapid heartrate or racing mind or sweaty palms. All normal physiological systems. Except, your body seems really skilled at sending your system into a state of anxiety, right? It’s like your body learned to be uptight as its baseline. So, I wonder if we might look to soothe your body’s system so as to help it relearn to relax? We work to master physical control over your body in order to ease the anxious thoughts. What do you think?”
Past Connections Frame
“You say depression has been around most of your life, and you’ve also mentioned long-time struggles with family. I wonder if some part of you internalizes the pain from family or maybe it manifests inside you as this heaviness… And, now, as you grow more aware, you have this opportunity to feel the heaviness more than you could as a child.”
Defense Mechanism Frame
•“I wonder if the more adaptive coping strategy, for a child with little experience, was to sort of repress the darkness or quiet the pain inside by not paying too much attention to stressors, like your family. Now, I wonder if that coping strategy, the push it all down, is what keeps you in the dark about why you’re struggling or why you are feeling down and struggling. In other words, the coping of your past is no longer the answer for today’s struggles.”
PITFALLS OF INTERPRETATIONS
•Helper is afraid or lacks confidence in self
•Helper stays too shallow
•Forgets to be empathic & keep the client involved
•Client isn’t ready or doesn’t want insight
•Biased, stuck in 1 perspective or theory
INTERPRETATION GUIDES
•Who is the expert with the “correct” explanation?
•Who is doing the work?
•Does the interpretation land with the client?
•Does the interpretation add new energy or progress?
METAPHORS
•Creatively capture a client’s experience
•Provide an easily accessible lens to see treatment directions
•Can be co-created or offered
metaphors to use
•Jelly-bean jar & relationships
•The captain who doesn’t want to repair the hull
•Quicksand
•Passengers on the bus
•Movie screen & Banjo surprise
THE CAPTAIN & THE HULL
There was an old ship on the sea when, suddenly, it smashed into an iceberg out of nowhere. The hull was damaged, and the ship took on freezing water. The crew moved fast, patched the damage quickly, albeit with a thin & temporary barrier.
Luckily, it held long enough for them to get to a random port. However, once docked, the captain refused to inspect the ship’s damage. They ignored their crew’s pleading & didn’t make any repairs. They said, “The damage is beneath the surface, just where I like it.”
The crew begged their captain to reconsider, noting they would soon sail for more icy waters and would need a restored hull. The captain ignored them & set sail. Again, they hit another iceberg. The crew patched it up quickly, & the ship crawled back to the same port they’d left previously. Again, the captain refused to look at the damaged hull beneath the water’s surface.
The story continues on in this way, and the ship is never able to reach its final destination.
•
What’s your take-away from this story?
IMMEDIACY QUICK REVIEW
•Brings counseling content or process into the here & now, increasing everyone’s focus on the immediate experience & process occurring in the present moment.
•Can be a powerful invitation extended to the client to mindfully look at what’s going on 1) within them or 2) between them and the counselor.
•Could be a disclosure of helper’s feeling/reactions or sharing a hunch of what the client may be feeling in the moment (possibly linking it to the client’s issue).
Immediacy can:
•Increase client awareness of their experience
•Address unhelpful relationship patterns & interactions between client & counselor
•Strengthen the therapeutic relationship
•Contribute to change by heightening emotions, increasing ownership of experience, etc.
“I notice that you haven’t looked at me all session which is leaving me feeling rather shut out. It
feels as if you want to stop me getting too close… I wonder if that’s how it feels to you?”
Rx Process Statements
•Invites the client to share feelings about the therapeutic relationship.
•“I wonder what reactions you had to the session today?”
•“How do you feel like this conversation is going?”
Sharing Reactions
•Helper shares their feelings in the moment, usually following up with an inquiry about how the client feels.
•“I’ve been feeling a little stuck. How do you feel about our progress?”
•“Just sitting with that story, I feel a powerful sadness. How are you feeling right now?”
Drawing Parallels
•Helper wonders out loud whether the client has reactions to them that are similar to outside rxs.
•“You mentioned no one seems to get you. I wonder if you might be saying that I don’t really understand you.”
WHEN TO USE IMMEDIACY?
Promote Depth & Insight
•Heighten emotions by having clients mindfully contact them in the moment
•Increase the vulnerability (and thus the potential growth) of the relationship
•Give clients a moment to pause & reflect a slow, mindful awareness that promotes insight
Address a stuck point or obstacle in the relationship or counseling process
•Client is resistant, defensive, evasive, etc.
•You feel frustrated, drained, or bored… and realize you’re in a power struggle
•Ruptures, lack of trust, boundary issues
•Any negative relational dynamic
WHY IMMEDIACY?
•Increases the intensity of experiencing thoughts/emotions by focusing on the moment.
•In turn, this enhances relationships & insight.
Clients need to ______ which comes from________of an experience. This makes clients_______in changing their experience vs. passive victims of their pain.
own their experience (I feel X); awareness + verbalization; active agents
IMMEDIACY LETS YOU EXPLORE THE METAPHOR
Cl says, “I didn’t realize how far away your office was.”
- Are they telling you, via metaphor, how far away & foreign treatment seems to them?
- At an intrapsychic level, is “trouble finding parking” really abouthow they have trouble allowing themselves to settle down & settle in to the idea of coming to therapy?
SIDE NOTE: SHOULD YOU EXTEND A SESSION FOR A LATE CLIENT?
•Do you have other appointments afterwards?
•“Everyone gets 1 pass, but it’s not something I do in general.”
•“I end on time. It indirectly conveys the ground rules that I have time set aside for them to use as they see fit – supporting a boundary.”
•If you extend time without comment – does it convey the message that “if they arrive late, the hour will be extended”? How does that play out across sessions?
WHY NOT IMMEDIACY?
•Helpers get nervous about making clients angry, upset, etc.
•Helpers don’t trust their gut feelings
•Helpers use immediacy for the wrong reasons or use incorrectly:
•To reassure themselves that they are doing a good job (poor reason)
•Using “should” statements vs. phrasing things tentatively
CASE STUDY
•Session transcripts analyzed, research team watched the videotape of the sessions
•17 sessions total, $5 a session (later therapist proposed they be “done with paying”)
•Post-therapy interview, client said, “It was wonderful because I felt like Dr. W really took out the time to understand me [and]. . .the issues that I was going through. It was really helpful because I had a different therapist before and you could just tell that they weren’t interested in what I was dealing with. So he wanted to get to the core of the issue. So, that’s what made it special to me.”
•Client disclosed how her father had beaten her brother so badly that he was totally paralyzed, dying years later. Cl said her mother overtly expressed loving her brother more than her (said Cl was too dark-skinned & didn’t want her).
•Client was deeply wounded, yet highly resilient, motivated, & eager to be involved in therapy (took notes in session, requested more directive & problem-solving therapist)
•First 10 sessions = warmth & understanding. Sessions 11-13 = progress stalled (Dr. W less attuned to Cl, often redirecting session to his goal of Cl seeking employment, surface-level work – Cl became more passive in response). Session 14 – new progress made after collaborative spirit was reestablished.
PROCESS DATA IN CASE STUDY
Very active
•Therapist averaged 44% of words spoken in transcript.
•56 events of immediacy in 17 sessions (about 3-4 per session)
•More intense immediacy exchanges came in later sessions, many events were brief check-ins
12 immediacy categories
1.Reinforced client for what she did (24 events)
2.Wanted to collaborate w/ client (13)
3.Inquired about Cl’s reactions to therapy (11)
4.Reminded Cl it’s okay to disagree w/ him (9)
5.Said he was glad to see Cl (8)
6.Talked about boundary or fee (8)
7.Inquired about possible problems in rx (7)
8.Drew parallels in rx (7)
9.Disclosed immediate feelings of closeness (7)
10.Affirmed/Shared Cl’s pain (6)
11.Reinforced Cl for disagreeing with him (4)
12.Gave client a gift (4)
RESULTS OF IMMEDIACY? case study
•After Session #14, therapist (and those watching the tape) thought a rupture could still be present.
•Therapist wanted to express he was reliably present – in contrast to Cl’s mother.
•The relationship was never deeply processed past this – but the effects were a much more productive following session, with client disclosures that showed increased comfort.
•It’s possible she never felt a rupture, but it’s also possible that she couldn’t admit to anger b/c of her difficulty with confrontation or that the word “withdrawal” was too strong for her.
ACTION STAGE
•After exploration, ideally after insight too (now we know what we gotta do)
•No action = continued dysfunction (won’t get better on its own)
•However – if in crisis – immediate action is required.
ACTION WORK = BEHAVIORAL WORK
•Watch out! Pesky thoughts & sticky emotions will STILL linger.
•So, sometimes, action work = working on how we’ll pivot away from these “obstacles” with healthy coping methods.
•Less feel, more do. (But decide TOGETHER)
FOCUS ON OVERTBEHAVIORS
•Things you can see someone do (visible changes)
•Things you can do in the present moment & current situation (do them today/this week)
•Specify the behavior & relate it to a clearly defined goal.
Example: I will get up at 8am MWF, go jogging for at least 20 minutes, with the goal of increasing my distance each day in order to be healthier.
ACTION STAGE GOAL – NEW BEHAVIOR
•Thoughts/Cognition Target?
—Thought records, self-compassion statements
•Deep Pain/Trauma Target?
—Journaling, Life narrative, Share in a group
•Self-Soothing of Emotion?
—Distraction & Grounding, Positive imagery
•Familial & Relational Targets?
—Ritual of connection, Letter of appreciation
•Empowerment?
—Join an advocacy group, Attend a pride march
•Positive Psychology/Meaning?
—Gratitude journal, Reconnect with nature/spiritual side
Identify new behaviors to try out – which changes depending on what our main “target” area is
POSITIVE ACTIONS > POSITIVE THINKING
•Identify a current challenge
•Write how you feel about it
•Find 1 thing going right with this challenge.
•Hidden opportunities?
•Grown closer to others?
•Proud of yourself for communicating about it? Or glad others take it seriously (even if not resolved yet)?
YOU SHOULD BE MORE ACTIVE, DIRECTIVE, OR PRESCRIPTIVE
•Suggest an adaptive behavior
•“Let’s see, I’ve got some ideas, then I’d like to hear what you’re thinking. I was thinking…”
•Modify a behavior
•“Sounds like you had the right idea, but it fizzled out. I wonder if, next time, we might…”
BE A COACH (NOT A FIXER)
•Facilitate the planning, don’t make the plan for them.
•Help them figure out how to implement the plan (when, where, how) – don’t set it up for them.
•Check in – “How confident do you feel in carrying out this plan?”
•“What would get us off track?”
•What’s our motivation for when we don’t “feel like doing it”?
4 TYPES OF ACTION
Behavior Change
Relaxation & Soothing
Rehearse a social skill
Decision making
Behavior Change
With specific problem in mind, explore the idea of action change, previous attempts, & generate new options. Evaluate how it goes, adjust as needed.
Plan my time, feels like a drag, tried planners B4, haven’t tried “chunked” time
Relaxation & Soothing
Healthy coping skills, psychoeducation, practice them in-session to translate them outside of session – align with values
Deep breathing, self-care, grounding, exercise
Rehearse a social skill
Describe a specific social or communication problem, role-play back & forth to evaluate effectiveness, brainstorm degrees of communication or boundaries, provide a role model example
Try being assertive to me… (provide feedback & then demonstrate)
Decision making
Identify issue, list values & rate their importance, determine options along a continuum, commit (verbalize & write down), empathize with future self
Do I go straight into PhD program? Or take a year off?
NORMALIZE TRIAL & ERROR
•Ditch what doesn’t work, everyone’s got to find their own & unique collection of tools
•Improvement is ups AND downs
•Discuss a “not yet” mindset
•Emphasize empathy & support in cases of “relapse” & “struggles to change”
Reflect: How has changed looked in your life? Continuous improvement? Gradual or rapidly?
Exploration Foci:
•What’s the smallest step we can take?
•How do they feel about transition & change?
•What’s worked in the past?
•What’s an obstacle we can anticipate & plan for?
Insight Foci:
•What’s maintaining the symptoms & “stuckness”?
•How does their past failures impact them now?
•Whose “voice” is louder when they begin to change?
COMMON PITFALLS Action stage
•Moving too quickly to action or being too rigid
•Not realizing you sound like the expert that’s telling the client what they need to do…
•Not bold enough to nudge clients to make changes or not being supportive/encouraging
•Too invested in the client changing à why do you think this a pitfall?
SESSION STRUCTURE
•It’s the way you want to start/end sessions.
•It’s the gameplan for how the middle part looks like (e.g., teaching skills, lots of listening, more directive) & the approach you take.
•It’s looking at the opportunity to get to know one another (Who shares? Is it mutual? What’s okay to ask about?)
PLANNING YOUR COUNSELING SESSION – EARLY SESSIONS
•Connect & build strong trust
•Develop a set of hunches about how the client functions, feels, thinks – working hypotheses
•Develop an agreed upon goal & interventions
•Decide on the framework for future work
WHAT’S OUR WORK GOING TO LOOK LIKE?
•Decide how active everyone will be. Give space? Is gently pushing & influencing okay?
•What’s the focus of our therapy? What’s “off the table” or “not the priority right now”?
•How do we check-in & give feedback to each other?
•How do you feel supported? What are you looking for in a counselor? How could we better use our time?
•How much to push? How much to assign “therapy tasks” outside of session?
PITCH THEM AN IDEA
•I listen, empathize, & give you space…
•I’m active, collaborative & focused on developing your tools for managing stress…
•<Insert metaphor for therapy here>
•We keep it light… we delve deeper into painful histories… we focus on present struggles… we cry… we laugh… we do quick mood checks… we open session wherever you like… we focus on specific issue…
Give them options. Come to an agreement about a general framework.
Assessing & Preventing Suicide
Biological, Sociological, & Psychological explanations of Suicide
Biological - certain Mental Health Diagnoses associated with increased risk (e.g., schizophrenia has 5-10% of people go on to complete the act of suicide)
Sociological – Ex. transgender folks have massively increased risk of suicide in comparison to cisgender folks
Psychological – Ex. adverse childhood events (trauma) is associated with increased risk
Suicide is the leading cause of death for
young men & 3rd most common cause of death for middle aged men (though they have the highest frequencies of suicides, especially in the Western world).
Self-harm & Suicidal ideation are
not the same, but self-harm does elevate the risk of acting on suicidal thoughts at some point in their life.