NR511 Week 5 Common Musculoskeletal Disorders
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
Useful approach in initial pt encounter.
Is the complaint...
Acute or chronic?
Articular or non-articular?
Inflammatory or non-inflammatory?
Localized or systemic in distribution?
Acute pain
<3months, Sharp/throbbing/pulsing/electric/paresthesia/burning in quality, moderate to severe intensity at first that decreases over time, edema that decreases over time, pain disappears once healing is complete, mood does not change pt complaint, pain localized to site of injury, results from specific injury or inflammation
Chronic
> 3 months, pain becomes more generalized than specific, pain patterns shift in location/frequency/intensity/quality, pain does not change with movement/rest/over time. Pain constant rather than intermittent, mood affects pain
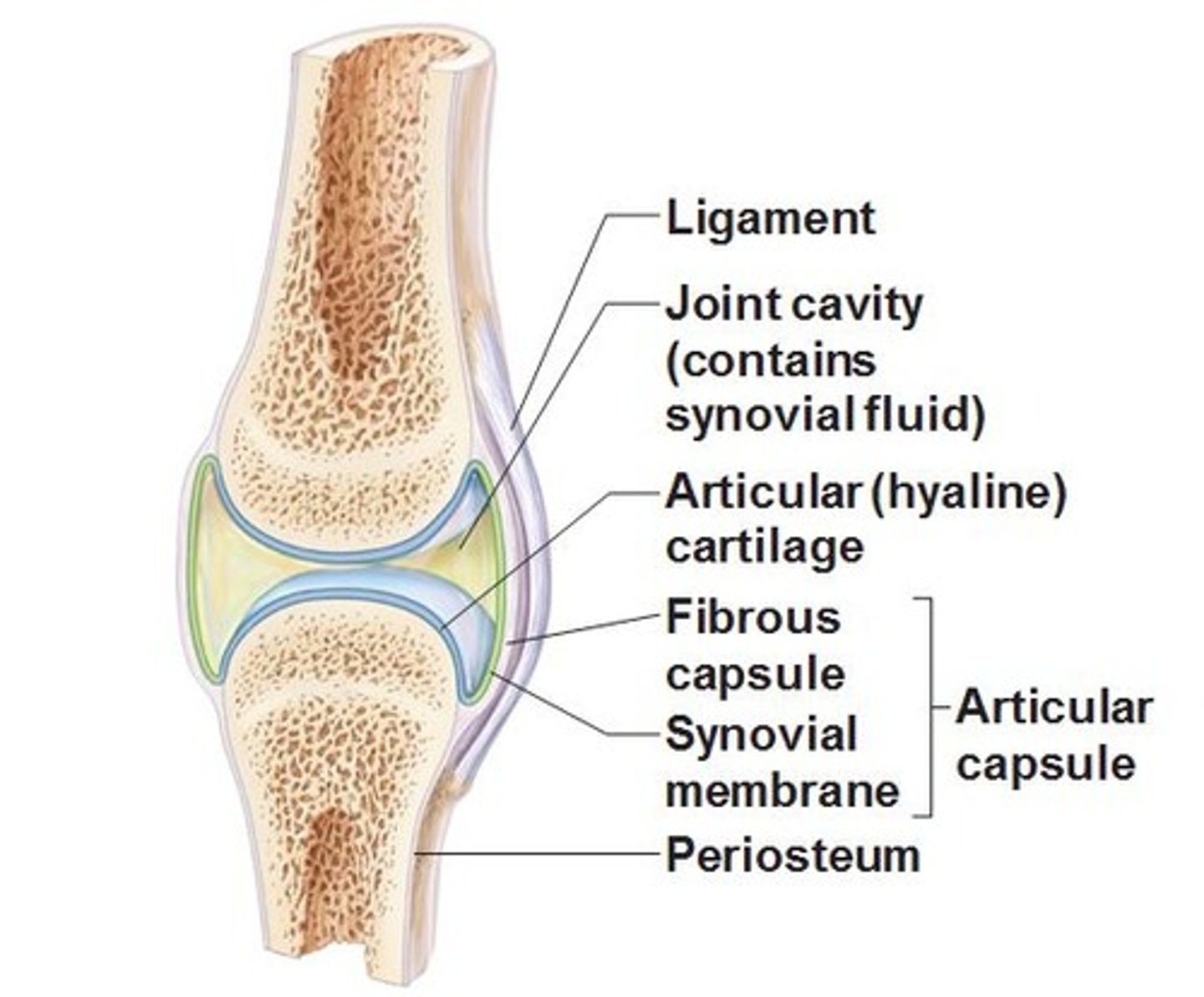
Articular Structures
synovium, synovial fluid, articular cartilage, intraarticular ligaments, joint capsule, juxtaarticular bone
Articular Structure Disorders
Deep or diffuse pain
Limited AROM and PROM on movement
Swelling
Crepitation
Instability
Locking
Deformity
Articular Disorder Classifications (3)
Monoarticular: One joint
Periarticular: Two to four joints
Polyarticular: Four or more joints
Nonarticular structures
Ligaments
Tendons
Bursae
Muscle
Fascia
Bone
Nerve
Overlying skin
Nonarticular structure disorder presentation
Painful AROM but not PROM
Demonstrated point or focal tenderness
Physical findings far from the joint capsule
Unlikely to see crepitus, instability, or deformity
nonarticular disorders are described as either... (2)
Focal or widespread
Inflammatory diseases can be either.... (2)
ideopathic or infectious
4 cardinal signs of inflammation
erythema, warmth, pain, swelling
Systemic signs of inflammation
Fatigue
Weight loss
Morning stiffness
Fever
Elevated ESR
Elevated C-reactive protein
Anemia of chronic disease
Hypoalbuminemia
Thrombocytosis
Non-inflammatory disorders tend to be related to....
trauma (i.e., meniscus tear);
ineffective repair (OA);
neoplasm; and
pain amplification (i.e., fibromyalgia).
Musculoskeletal pain thorough hx
Age
Occupational history
Medications
Leisure activities or hobbies and Family history
Onset with precipitating events
Location including number of joints and distribution
Duration (constant, intermittent)
Characteristics
Alleviating factors
Relieving factors
Severity or limitations of ADLs
Organ systems that may be related to MSK pain
skin (psoriasis), GI tract (inflammatory bowel disease, scleroderma), eye (sarcoidosis), and nervous system (Lyme disease, vasculitis, MS) just to name a few.
MSK physical assessment
Begin by INSPECTING the affected part, observing for side-to side- symmetry
Look for signs of trauma, ecchymosis, erythema, skin lesions, symmetry, edema, etc.
The uninvolved side should be examined initially and compared with the involved side.
palpation to assess inflammation or swollen joints, tender points or trigger points. ROM should be assessed passively and actively.
Acute MSK injuries
SPASM: persistent, painful, and reversible contracture of muscle
STRAIN: muscle injury caused by excessive tensile stressed placed on a muscles resulting in stiffness and decreased function
SPRAIN: stretching or tearing of ligaments that occurs when a joints is forced beyond its normal range.
Sprains
some degree of swelling, pain, and disability
Muscle Cramps
Sudden, painful involuntary contractions lasting a few seconds to several minutes. Muscle cramps are often related to vigorous exercise or during sporting events caused by dehydration but other causes can occur.
Parathesias- what is it?
sensation of numbness or tingling, or paresthesia, may be focal or generalized.
Parathesias Assessment
Patients with paresthesia should undergo a detailed neurological assessment to assess whether sensory or motor deficits are present. Paresthesias are often part of signs and symptoms associated with radiculopathy which is caused by compression of spinal nerve roots
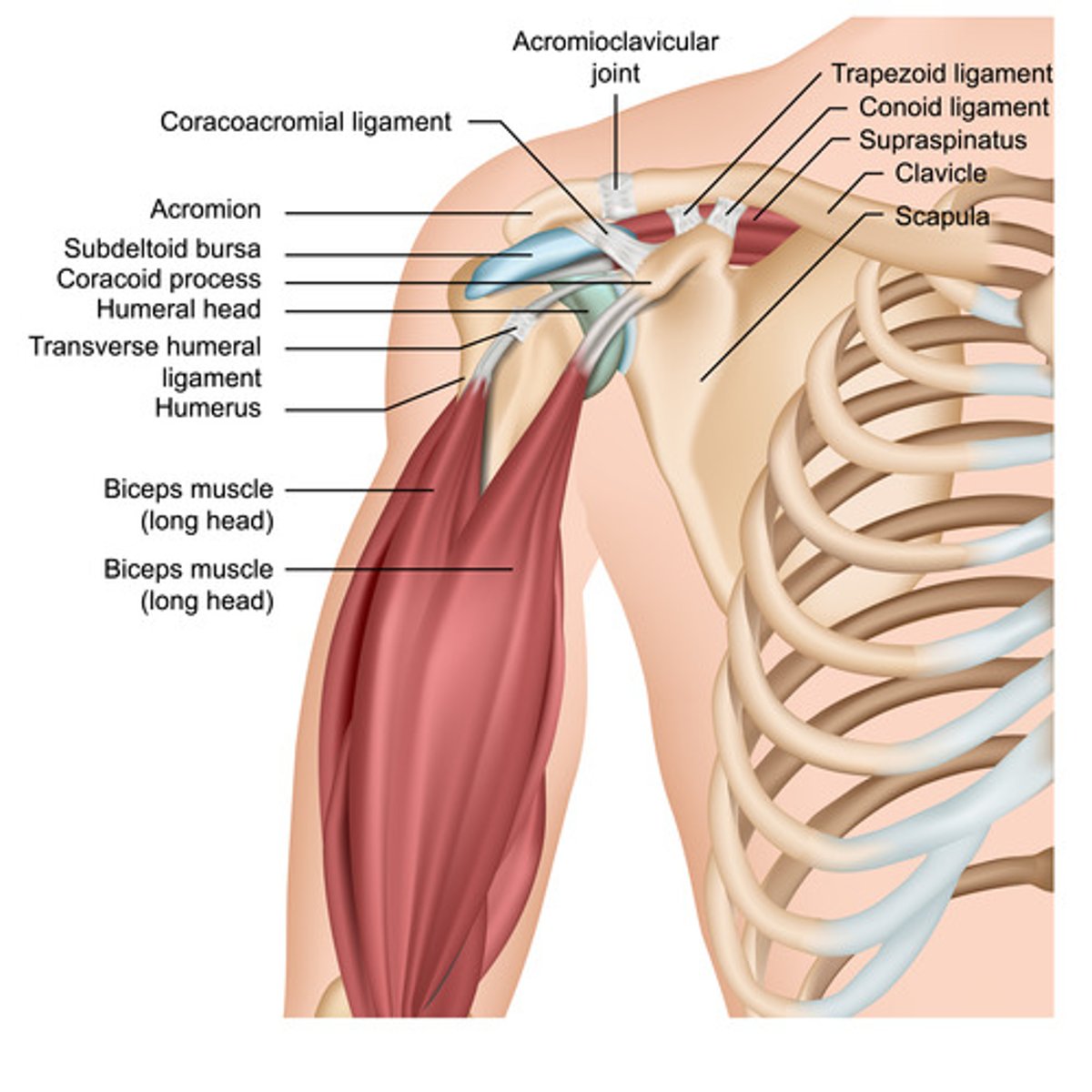
Anatomy of the Shoulder
Physical examination of the shoulder
INSPECTION (Deformity of AC joint, Deformity of the glenohumeral joint, Swelling, Bruising, Scars, Asymmetry),
PALPATION (Palpation should begin over the sternoclavicular joint and proceed laterally along the clavicle to the AC joint, scapular spine—feeling through the superior and inferior angles, cervical and thoracic spinous, and subacromial bursa/tendons.),
ROM (Apley scratch test which measures abduction and external rotation, internal rotation and adduction, Internal/external in flexion, Internal/external in abduction)
Impingement Syndrome- what is it
pathological changes that result when the subacromial bursa and/or rotator cuff becomes inflamed due to compression under the roof of the shoulder joint. The rotator cuff covers the anterior, superior, and posterior aspects of the humoral head and is formed by the coming together of four muscles which assist in elevating the arm.
Impingement Syndrome- Hx & Presentation
gradual onset of anterolateral shoulder pain that is exacerbated by overhead activity. It is sometimes described as a catching sensation. Pain can also radiate from shoulder to elbow.
Impingement Syndrome- Physical
palpation of the greater tuberosity and subacromial bursa commonly will elicit tenderness and crepitus with shoulder motion. On ROM pain will occur with having the patient slowly lower the abducted arm against downward resistance. Neers & Hawkins signs are usually positive.
Impingement Syndrome- imaging
Ultrasound or magnetic resonance imaging (MRI) is not necessary unless pathology is suspected. X-ray is suggested if there is a suspicion of fracture or dislocation.
Impingement testing is best tested by locally anesthetizing the shoulder in the subacromial joint. A referral to orthopedics would be required.If the pain is mostly eliminated and downward resistance is improved then the source is MORE likely to be from inflammation and fibrosis rather than a full blown rotator cuff tear.
Impingement Syndrome- Treatment
Rest, NSAIDs, streching.
If no improvement after 6 weeks an ultra-sound guided peritendinous steroid injection may be tried following by continued stretching. Significant rotator cuff weakness or failure to improve after 6 weeks of rehab (with or without steroid injection) should prompt further evaluation and operative consideration.
Adhesive Capsulitis (Frozen Shoulder)- Hx
tight, painful shoulder joint with idiopathic loss of both active and passive ROM. Patients aged 40-60 years old are more likely to be affected and those with diabetes (especially Type I) is the MOST common risk factor. Individuals without predisposing factors should be investigated for the possibility of underlying organic or neoplastic disease. Underlying conditions related to frozen shoulder include: Parkinson's, stroke, tumors and cervical disk herniation, to name a few. Recuperation can take 6 months to 24 months. Over the course of time, there is decreasing discomfort associated with increasing improvement in function.
Adhesive Capsulitis (Frozen Shoulder)- physical assessment
Loss of active and passive ROM
Pain and tenderness with motion at deltoid insertion
May also have diffuse tenderness over the shoulder
Adhesive Capsulitis (Frozen Shoulder)- Imaging
AP & axillary x-rays of the shoulder to ensure smooth, concentric joint surfaces with intact cartilage space and also to rule out other pathology such as osteophytes, calcification and tumors. If radiographs are normal, other studies such as CT, MRI, and arthrography are rarely indicated but would typically be done by orthopedics.
Adhesive Capsulitis (Frozen Shoulder)- Tx
moist heat, and non-narcotic analgesics. Physical therapy to restore function is recommended but patient should be advised that a long recovery time is possible. If there is no improvement after 6-12 weeks, a referral to orthopedics is warranted.
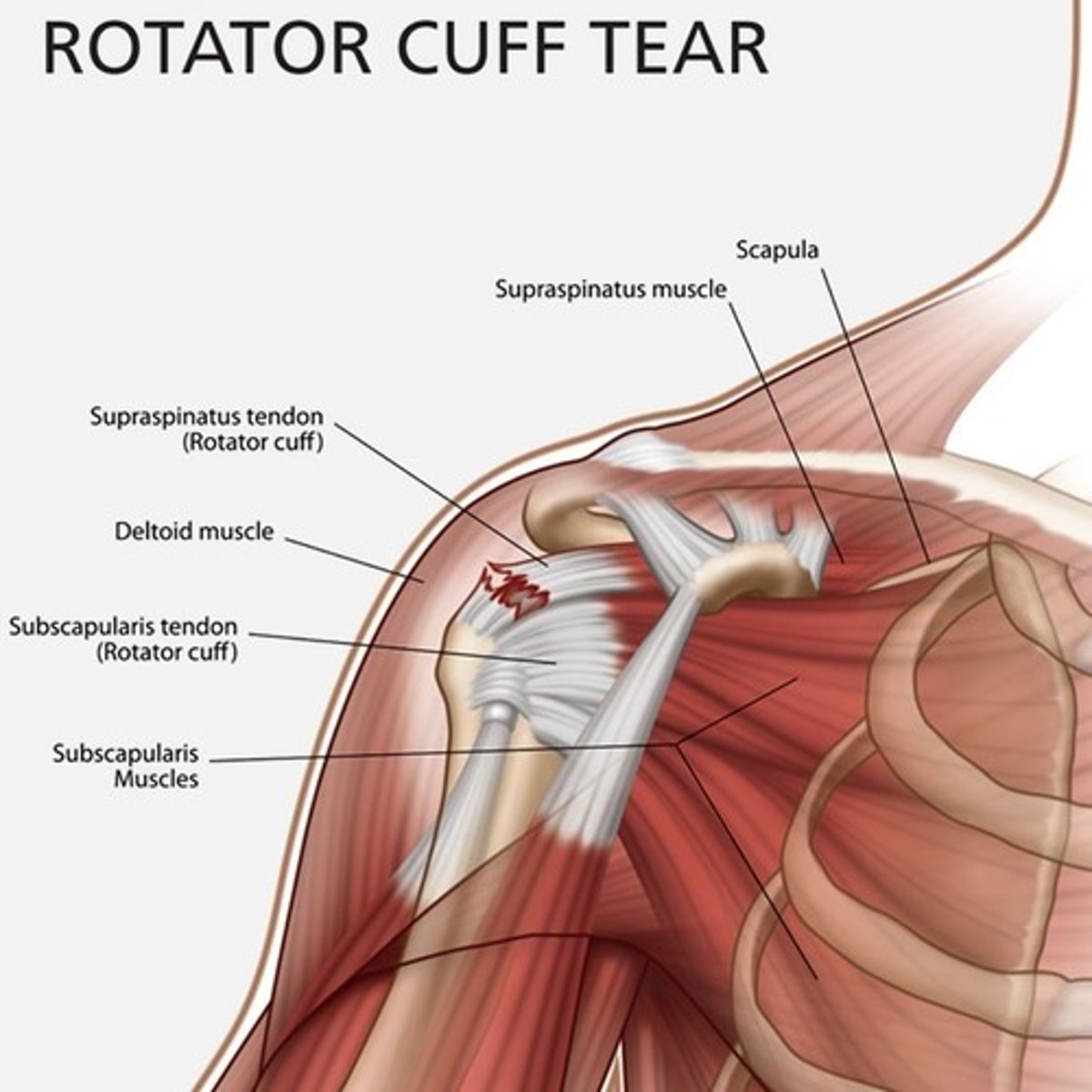
Rotator Coff Tears- how/who it occurs in
secondary to trauma, degenerative changes, mechanical impingement and/or altered blood supply to tendons over time. Spontaneous, full-thickness rotator cuff tears occur typically in patients older than 50 and the supraspinatous tendon is most often affected. When a rotator cuff tear occurs in individuals under 40 years, it is usually because of aggressive physical injury and repeated trauma
Rotator Coff Tears- Hx
The patient often reports lateral deltoid pain with weakness or decreased ability to abduct the arm. Pain is often worse and night and patients will report moderate to severe pain trying to scratch the back.
Rotator Cuff- imaging
MRI, ultrasound, and MR arthrography
Rotator Cuff tx
small, symptomatic tears and would include ice, NSAIDs, PT with stretching and strengthening along with restrictions on overhead lifting.
Refer to ortho if injury not responsive to tx. May require sx repair
Rotator Cuff Physical Exam
A suspected rotator cuff tear is confirmed by performing the "drop arm" test (examiner abducts the patient's shoulder to 90 degrees and instructs the patient to lower the arm slowly. If the arm drops to the side rapidly, the test is positive.
Acromioclavicular (A/C) Sprains- what is it/who is it mostly seen in/how does it occur
result in pain in the clavicular area after direct trauma or excessive pushing/pulling of the upper extremity. A/C sprains are commonly seen in young males and are typically associated with a fall while the arm is abducted causing trauma to the A/C joint; it can occur though from indirect trauma.
Acromioclavicular (A/C) Sprains- hx
Patients will often report pain on adduction or abduction past 90 degrees.
Acromioclavicular (A/C) Sprains- physical exam
Point tenderness over A/C joint, swelling and possible deformities may be seen.
Acromioclavicular (A/C) Sprains- imaging
X-rays can be performed to assess A/C distance. Normal acromioclavicular distance 1-3 mm, but distance shrinks with age. Compare X-ray with uninjured side.
Acromioclavicular (A/C) Sprains- tx
The types I & II injuries are treated non-operatively with 1-3 weeks of NSAIDs and sling.
Type III injuries controversially trend toward non-operative management.
Types IV, V, & VI injuries typically are treated surgically.
Elbow
The elbow is a hinge joint made up of the humerus, ulna and radius as well as muscles, ligaments and tendons.
Elbow pain-hx
A thorough history is essential along with all extracurricular and occupational activities.
Elbow pain physical
Erythema
Scars
Swelling or fluid accumulation
Atrophy such as muscle wasting
Alignment (Carrying Angle)
Regarding assessment and elbow palpation, the landmarks to look for should include medial/lateral epicondyle, olecranon process, radial head, and the ulnar/radial nerve.
The common tests for the elbow include:
valgus stress test; and
varus stress test.
Elbow pain ROM
When it comes to elbow ROM, the angles are crucial numbers.
The flexion should be between 140-150 degrees.
Extension 0-5 degrees.
Pronation 90 degrees.
Supination 90 degrees.
medial epicondylitis-what is it/presentation
Golfers elbow
Pain is often sharp in the medial epicondyle and radiates down the arm from the inside of the elbow. Pain occurs upon extension of the wrist or supination of the forearm such as when gripping, twisting, or flexing at the wrist. There may be weakness in the hand or wrist as well or numbness and tingling in the ring and little fingers.
Epicondylitis imaging
not necessary unless ruling out other dx
Lateral Epicondylitis- what is it/presentation
Tennis elbow
Pain is often sharp in the lateral epicondyle and radiates from the outside of the elbow and down the forearm. Pain occurs upon extension of the wrist or supination of the forearm such as when gripping and twisting. There may be weakness in the forearm or a weak grip.
Epicondylitis (medial/lateral) Tx
avoid or alter activities responsible for symptoms such light duties or work restriction. Treatment depends on the stage of healing of the damaged soft tissue.
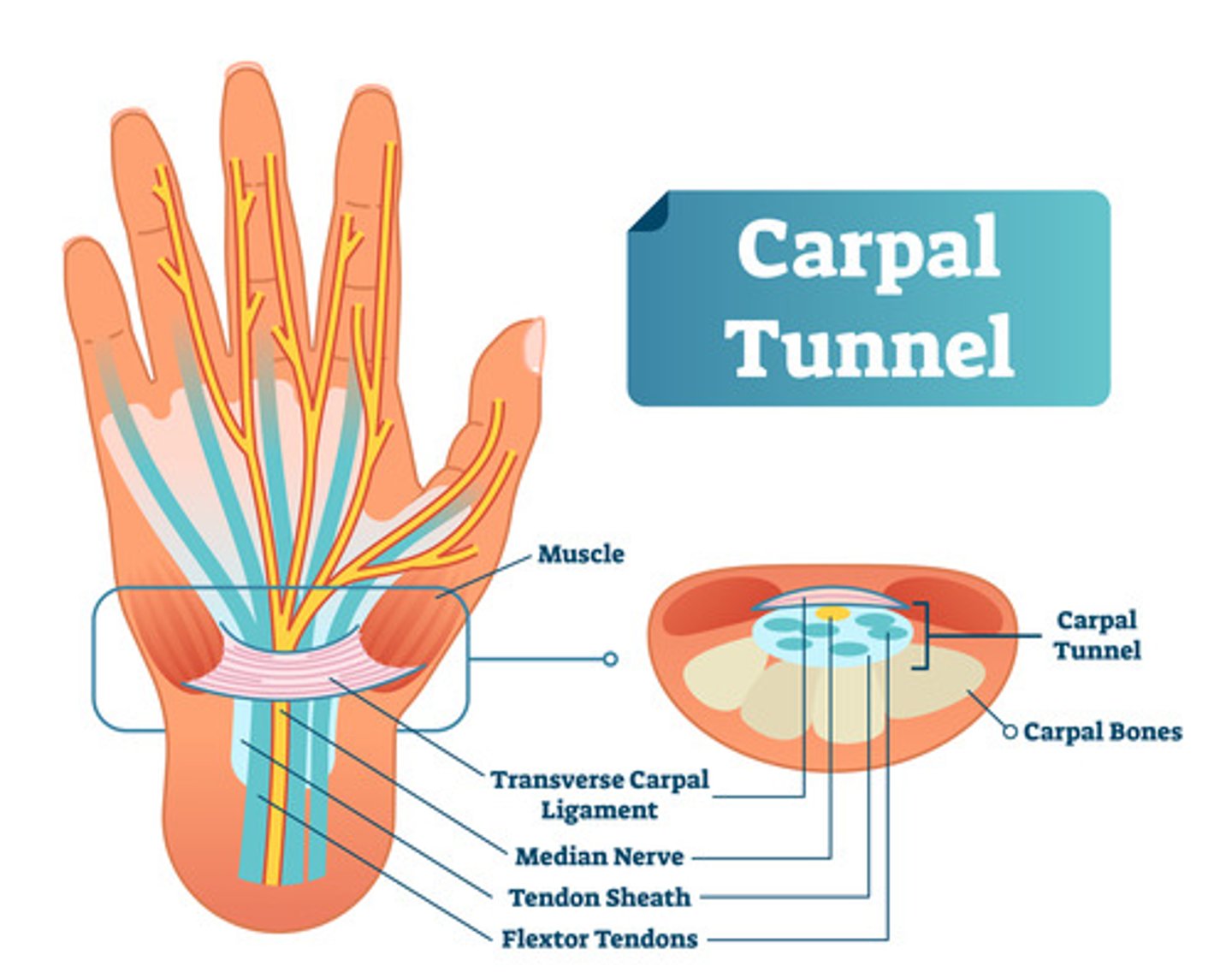
CARPAL TUNNEL SYNDROME (Median nerve entrapment)- how it occurs, what is it, common cause
occurs when the median nerve, which runs from the forearm into the palm of the hand, becomes constricted. The carpal tunnel is a narrow passageway of the ligaments and bones at the base of the hand that houses the median nerves and the tendons that bend the fingers. The median nerve provides feeling to the palm side of the thumb and to the index, middle, and ring fingers but not to the little finger. A common cause of CTS is repetitive activity with the hands that cause irritated tendons, causing compression of the median nerve.
CARPAL TUNNEL SYNDROME (Median nerve entrapment) HX
burning, tingling, or numbness of the hand and fingers, especially the thumb, middle, and index fingers. Symptoms usually start gradually, and the HALLMARK sign is nighttime awakening with numbness and tingling or feeling the need to "shake out" the hand or wrist because of numbness. This is because most of us sleep with our wrists flexed
As the condition progresses, symptoms may occur during the day, and weakness ensues, making it difficult to grasp small objects or perform manual tasks. In untreated cases, the muscle at the base of the thumb loses innervation and atrophies.
CARPAL TUNNEL SYNDROME (Median nerve entrapment)- physical exam
assessment for deformity or atrophy. Palpation for tenderness as well as testing of upper extremity strength, sensation, reflexes and ROM. A Phalen's and Tinel test should also be performed.
In the Tinel's test, the provider taps over the median nerve of the affected wrist. The test is positive if tingling occurs in the affected fingers.
Phalen's maneuver, or wrist-flexion test, involves having the patient pressing the backs of their hands and fingers together with their wrists flexed as far as possible, ideally 90 degrees. The test is positive if tingling or numbness occurs in the affected fingers within 2-3 minutes (it may not happen immediately).
CARPAL TUNNEL SYNDROME (Median nerve entrapment) Dx
clinical diagnosis with attention to occupational and leisure activities.
CARPAL TUNNEL SYNDROME (Median nerve entrapment) TX
nocturnal wrist splints that extend the wrist upwards, taking pressure off the tunnel.
NSAIDs
Pregnancy related CTS usually resolves after delivery. Corticosteroid injections are not recommended in the treatment of CTS over the concern of scarring of nerve and infection
The presence of thenar atrophy or unresolving symptoms with conservative treatment warrant a referral for surgical intervention.
DEQUERVAIN'S TENOSYNOVITIS- what is it, tendons involved, cause, most common risk
inflammation of tendons on the side of the wrist at the base of the thumb. These tendons include the abductor pollicis brevis and flexor pollicis brevis tendons. These tendons pass through a tunnel located on the thumb side of the wrist. Any swelling of the tendons results in increased friction and pain with certain wrist movements. Like CTS, de Quervain's tendinosis may be caused by repetitive movements but is also associated with pregnancy and rheumatoid disease. It is most common in middle-aged women.
DEQUERVAIN'S TENOSYNOVITIS-hx
pain felt over the thumb side of the wrist that may travel up the forearm. The pain is worse when forcefully grasping objects or twisting the wrist. A catching or snapping sensation may be felt when moving the thumb
DEQUERVAIN'S TENOSYNOVITIS- physical assessment
assessment for deformity or atrophy. Palpation for tenderness as well as testing of upper extremity strength, sensation, reflexes and ROM should be assessed. Phalen's and Tinnels tests should be done to rule out CTS.
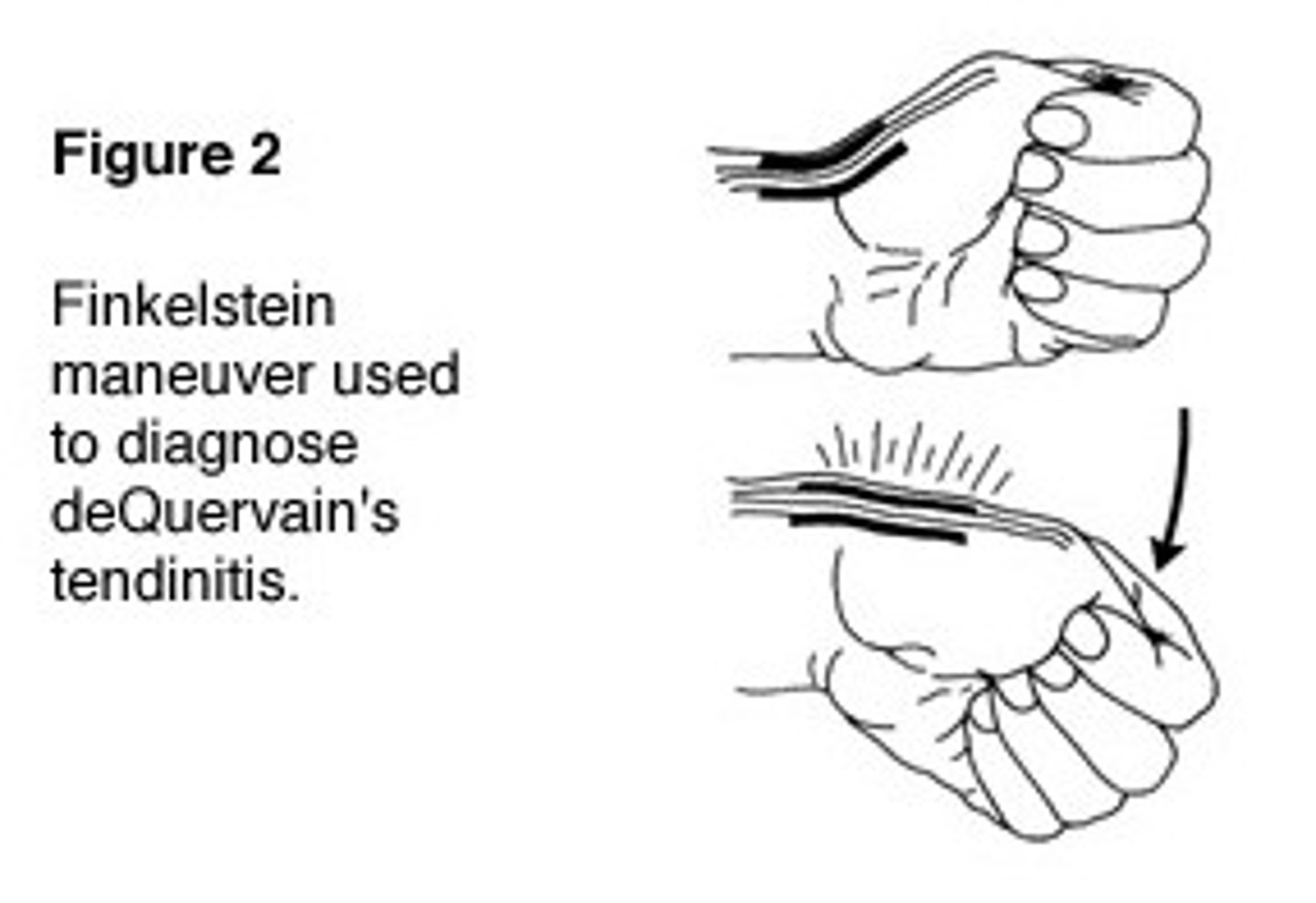
The confirmatory test for DQS is the Finkelstein test. The Finkelstein test is performed by having the patient place their thumb against their hand, making a fist with the fingers closed around the thumb. The patient then is asked to bend the wrist forward toward the little finger. The test is positive if pain is reproduced over the tendon on the thumb side of the wrist.
DEQUERVAIN'S TENOSYNOVITIS Dx
Based on H&P
DEQUERVAIN'S TENOSYNOVITIS TX
plints to rest the wrist and thumb, NSAIDs, and avoiding aggravating activities for 6-8 weeks.
Referral to ortho if symptoms do not improve
Trigger finger (jersey finger)- what is it, most common risk
condition where the tendons in the fingers or thumb are inflammed, making it difficult for the finger to slide through the tendon sheath. Any finger can be affected, although it most commonly occurs in the middle and ring fingers. Trigger finger limits finger movement, and when the patient tries to straighten the digit, it will lock or catch before popping out straigh and often involves a disruption of the FDP tendon near the DIP joint. Trigger finger may be idiopathic or associated with RA and diabetes. It is more common in women than men and occurs most frequently in people between the ages of 40-60.
Trigger finger (jersey finger) Dx
Testing is not needed, but in some cases, the provider may choose to perform AP/lateral/oblique X-rays to rule out other pathology.
Trigger finger (jersey finger) Tx
local anaesthetic and corticosteroid injection into the tendon sheath plus modification of activities for 4 weeks. An orthopedic referral is warranted for this procedure. If conservative treatment fails, surgical correction to release the tendon may be necessary.
Trigger finger (jersey finger) hx
Patients typically report pain and catching when they flex the finger.
Trigger finger (jersey finger) Physical assessment
Physical exam reveals tenderness in the palm at the level of the distal palmar crease, usually overlapping the MCP joint. A nodule might be palpable. The finger will lock when the patient flexes or extends the finger and is almost always painful.