(FINAL) CC1 LEC L1.5 Aminoacidopathies & Protein Abnormalities
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
Phenylketonuria (PKU)
Aminoacidopathies: __________
Defect (Enzyme/Gene)
PAH (Phenylalanine hydroxylase) deficiency
Hallmark Clinical Features & Odors
Mental retardation, microcephaly (in infants of untreated mothers).
Tyrosinemia Type 1
Aminoacidopathies: __________
Defect (Enzyme/Gene)
fumarylacetoacetate hydrolase (FAH)
Hallmark Clinical Features & Odors
Cabbage-like odor, jaundice, liver failure, bleeding.
Tyrosinemia Type 2
Aminoacidopathies: __________
Defect (Enzyme/Gene)
Tyrosine Aminotransferase (TAT)
Hallmark Clinical Features & Odors
Photophobia, eye/skin lesions.
Tyrosinemia Type 3
Aminoacidopathies: __________
Defect (Enzyme/Gene)
4-hydroxyphenylpyruvate dioxygenase (HPD)
Hallmark Clinical Features & Odors
Seizures, loss of balance.
Alkaptonuria
Aminoacidopathies: __________
Defect (Enzyme/Gene)
HGD gene (Homogentisate 1,2-dioxygenase)
Hallmark Clinical Features & Odors
Ochronosis: Blue-black pigmentation in cartilage/tendons.
Asymptomatic until 3rd decade.
Urine: Darkens upon standing.
Maple Syrup Urine Disease (MSUD)
Aminoacidopathies: __________
Defect (Enzyme/Gene)
Absence of branched-chain -ketoacid dehydrogenase (BCKDH) complex (BCKDHA, BCKDHB, DBT genes)
Hallmark Clinical Features & Odors
Odor: Maple syrup or burnt sugar (urine, breath, skin).
Lethargy, failure to thrive within a week.
Isovaleric Acidemia
Aminoacidopathies: __________
Defect (Enzyme/Gene)
Isovaleryl-CoA dehydrogenase (IVD)
Hallmark Clinical Features & Odors
Odor: Sweaty feet (due to buildup of isovaleric acid).
Homocystinuria
Aminoacidopathies: __________
Defect (Enzyme/Gene)
CBS, MTHFR, MTR, MTRR, or MMADHC genes
Hallmark Clinical Features & Odors
Lens dislocation (near-sightedness) due to lack of cysteine for collagen. Osteoporosis, mental retardation.
Citrullinemia Type 1
Aminoacidopathies: __________
Defect (Enzyme/Gene)
Argininosuccinate Synthase 1 (ASS1)
Hallmark Clinical Features & Odors
Urea cycle disorder.
Lethargy, vomiting, seizures, coma due to toxic ammonia buildup.
Citrullinemia Type 2
Aminoacidopathies: __________
Defect (Enzyme/Gene)
SLC25A13 gene
Hallmark Clinical Features & Odors
Urea cycle disorder.
Lethargy, vomiting, seizures, coma due to toxic ammonia buildup.
Argininosuccinic Aciduria
Aminoacidopathies: __________
Defect (Enzyme/Gene)
Argininosuccinate lyase (ASL)
Hallmark Clinical Features & Odors
Urea cycle disorder.
Lethargy and unwillingness to eat within first few days of life.
Cystinuria
Aminoacidopathies: __________
Defect (Enzyme/Gene)
SLC3A1 and SLC7A9 genes
Hallmark Clinical Features & Odors
Inadequate renal reabsorption of cystine.
Formation of cystine stones in kidneys, ureters, or bladder.
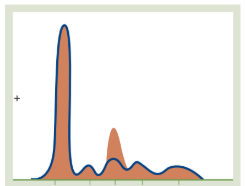
Nephrotic Syndrome
The Pattern: A massive drop in Albumin and a significant spike in the α2-macroglobulin peak.
Why: In kidney disease, the "filter" is damaged. Small proteins like Albumin are lost in urine. The liver tries to compensate by overproducing larger proteins like α2-macroglobulin, which are too big to leak out.
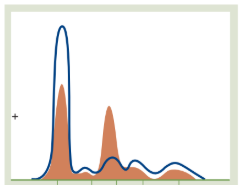
Acute Phase Proteins (Acute Inflammation)
The Pattern: A mild decrease in Albumin and a noticeable increase in α1 and α2 globulins.
Why: The liver ramps up positive acute phase reactants (like Haptoglobin and α1-antitrypsin) during infection or trauma, causing these middle peaks to swell.
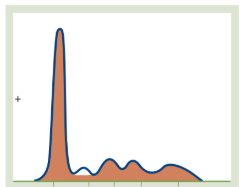
α1-Antitrypsin Deficiency
The Pattern: A complete absence or near-total flattening of the α1 peak.
Why: Since α1-antitrypsin makes up about 90% of the α1 globulin fraction, its genetic absence leaves a visible "void" in the graph. This is often linked to early-onset emphysema or liver cirrhosis.
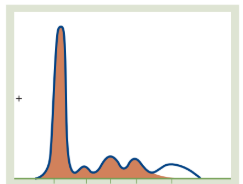
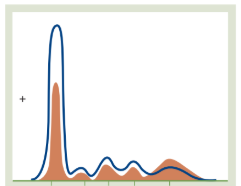
Hypogammaglobulinemia
The Pattern: A very flat or non-existent γ (Gamma) peak on the far right.
Why: This indicates a deficiency in antibodies (Immunoglobulins). This can be congenital or acquired (e.g., due to certain leukemias or immunosuppressive drugs).
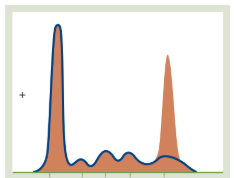
Monoclonal Gammopathy (M-Spike)
The Pattern: A tall, narrow, "church-spire" peak in the Gamma region.
Why: This is a classic sign of Multiple Myeloma. A single clone of plasma cells is pumping out a massive amount of one specific, identical antibody; spike in IgG.
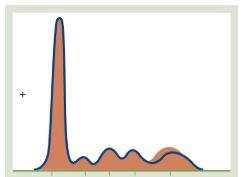
Polyclonal Gammopathy
The Pattern: A broad, "mountain-like" rise in the Gamma region.
Why: Unlike the narrow spike in (E), this shows many different plasma cells are active. This is common in chronic infections, autoimmune diseases (like Lupus), or chronic liver disease.
Severe Hepatic Disease
The Pattern: A significant decrease in Albumin and generally low peaks in the α and β regions.
Why: The liver is the "protein factory." When it is severely damaged, it can no longer manufacture Albumin or the transport proteins found in the α and β zones.
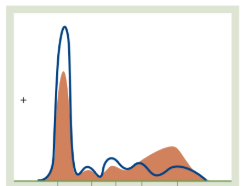
Liver Cirrhosis
The Pattern: A low Albumin peak and a unique "smearing" or "bridge" connecting the β and γ peaks.
Why: This is the diagnostic hallmark of cirrhosis. It’s caused by increased IgA (which migrates between the Beta and Gamma zones), making it impossible to see where one peak ends and the next begins; beta-gamma bridge.
Hepatic Damage
Total Protein (TP): NORMAL or DECREASE
Albumin: DECREASE
Globulin: INCREASE
Key features: Cirrhosis & Hepatitis
Infections
Total Protein (TP): NORMAL or DECREASE
Albumin: DECREASE
Globulin: INCREASE
Key features: Acute & Chronic
Inadequate Diet / Nephrotic Syndrome
Total Protein (TP): DECREASE
Albumin: DECREASE
Globulin: NORMAL
Immunodeficiency
Total Protein (TP): DECREASE
Albumin: NORMAL
Globulin: DECREASE
Dehydration
Total Protein (TP): INCREASE
Albumin: INCREASE
Globulin: INCREASE
Multiple Myeloma
Total Protein (TP): INCREASE
Albumin: NORMAL
Globulin: INCREASE