Pulp Therapy of Immature Permanent Teeth
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
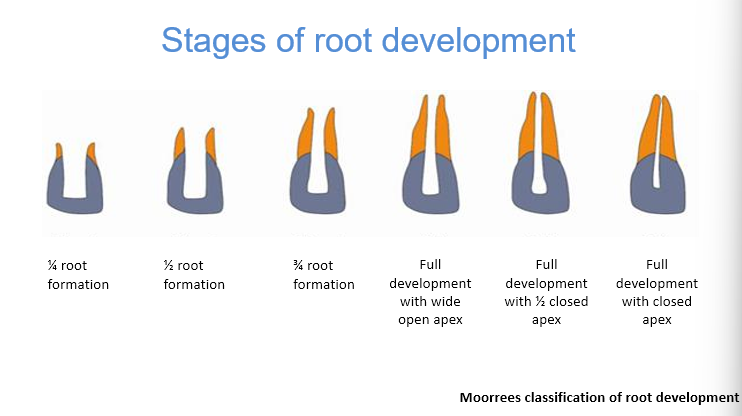
What are the stages of root development according to the moorrees classification of root development
¼
½
¾
full development of the root with wide apex opening
full development with ½ closed apex
full development with closed apex
below stage 6 is immature
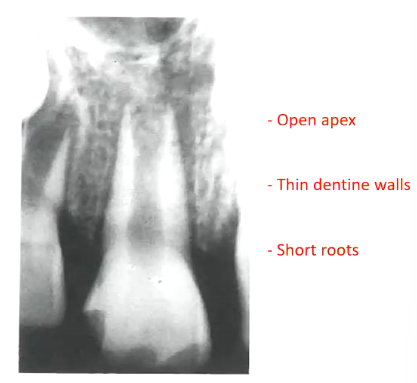
Immature vs mature teeth roots
Immature:
Shorter roots (tooth cannot withstand a lot of force, stage 1 and 2 may not be suitable for any pulp therapy)
Wide open apex (allows more blood to enter roots - better healing, also nothing stopping extrusion of material)
Thin dentine walls (affects the prognosis of tooth, trauma may fracture the tooth in the future when treating immature teeth)
Mature:
Closed apex
Long root
Thin dentine walls
prognosis of pulp healing and why?
obturation ease
crown root ratio
strength of root
immature vs mature teeth?
Immature:
Better prognosis of pulp healing - good blood supply (wider apex)
less favourable crown root ratio
difficult to obturate
week root - increase fracture risk
Mature:
not as good prognosis of pulp healing - less bloody supply
better crown root ratio
easier to obturate
stronger root
What are aims of pulp therapy in immature permanent teeth? (4)
Preserve the vitality of the pulp or part of the pulp (to let the root continue growing - thicker walls, narrower canals)
Continuation of root development and root apex formation - (Apixogenesis - do pulp therapy so tooth can continue growing - apex close)
Induce of a natural apical barrier - (Apexification - we fix it)
Placement of an artificial barrier at the root apex
Apexogenesis is for which type of teeth, vital or non vital?
Vital teeth, so apexification the tooth can no longer grow to maturity as the pulp is dead
What are 4 procedures that fall under Apexogensis for vital teeth?
Indirect pulp capping
Direct pulp capping (not primary teeth anymore, can put CaOH no longer any resorption)
Cvek pulpotomy (remove 2-3 mm of the pulp if there is any infammation)
Conventional pulpotomy (removing whole coronal pulp)
these keep the vitality of the teeth so that the root development process can continue to maturity
these procedures rely on good bloody supply from the apex
What are 2 pulp procedures for non-vital teeth in apexification?
Inducing a calcified barrier at the apex:
1. Natural barrier with CaOH dressing (irritate bone on top of apex and body will lay down cementum like tissue to close apex artificially - body makes the barrier)
2. Artificial apical barrier with MTA cement - (we put the barrier)
Pulp revascularisation (regenerate the pulp)
Definition of Apexogenesis? again what 4 procedures does this include?
Vital pulp therapy procedure performed to encourage physiological development and formation of the root end
indirect and direct pulp capping, partial pulpotomy (cvek), conven pulpotomy
Rationale for vital pulp therapy - Apexogenesis? (3)
Continuation of root development needs an normal healthy pulp
Pulp of immature teeth has a better repair potential (blood supply)
poor long term prognosis of endodontically treated immatuer teeth (most will fracture - you want thicker walls, closed apex )
What is a Cvek pulpotomy/partial pulpotomy?
A procedure in which the inflamed pulp tissue beneath an exposure is removed to a depth of 1-3mm or more to reach the deeper healthier tissue
What is the rationale behind a cvek pulpotomy (2)?
Based on the observations from Mjor and Townstad - dental pulp is usually inflamed only to a depth of 2 mm
removing the infected part of the pulp and leaving the healthy part will stop the spread of the inflammation and encourage physiological development and formation of the tooth

What procedure does this child require?
Partial pulpotomy
What materials can be used here for partial pulpotomy? (4)
Non setting CaOH (opposite to primary teeth where it causes resorption)
MTA (stronger bridge, easire to handle, seal - discolouration - tooth goes grey not ant and expensive)
Biodentine
whiet MTA - still causes discolouration
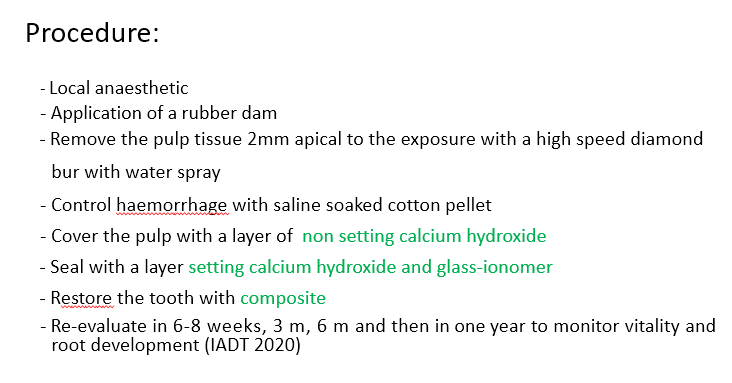
What is the procedure of a Cvek pulpotomy in immature teeth?
if the bleeding doesn’t stop then you need to go deeper , then complete pulpotomy
setting is hydrophobic, non-setting is hydrophilic and so stays on the pulp
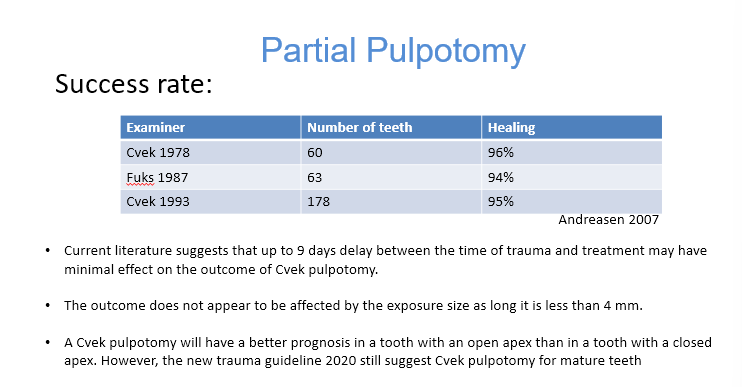
Success rates of cvek pulpotomy?
management of traumatic injury due to procedural error:
what do you do if there is saliva contamination (1)
when there is no saliva contamination (4)
proceed for partial pulpotomy if saliva contamination
if no saliva contamination:
Direct pulp capping with CaOH/MTA/Bio-dentine:
1. irrigation
2. stop bleeding (if bleeding does not stop then proceed for partial pulpotomy)
3. Place non setting Caoh/MTA/biodentine
4. Seal with GIC and restore
Remember no MTA in anterioir teeth
What is apexification?
A method of inducing a calcified barrier at the apex of a non-vital tooth with incomplete root formation by the use of CaOH as a canal medicament
you change the CaOH every few months
What is the rationale behind apexification (2)
Wide funnel shaped canals make endodontic treatment in immature teeth difficult
An apical barrier is needed against which a root canal material can be packed
Why is CaOH used in apexification? (2)
high pH - bactericidal
zone of liquefaction and coagulation necrosis - cementum like structure formed acting like a calcific barrier
Disadvantages to using CaOH? (2)
Concerns about long application of CaOH may result in weakening the dentine walls and increase the risk of root fracture
it is a long procedure that requires patients compliance and high cost
2 indications and contraindications in apexification?
Immature tooth and non vital - indications
vital tooth, very short roots
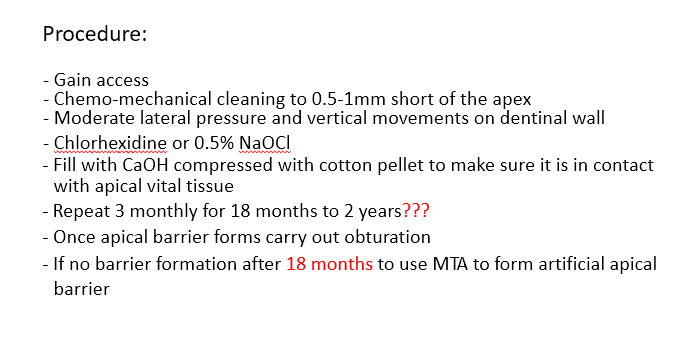
What is the procedure for apexification?
chlorhexidine - material of choice for children
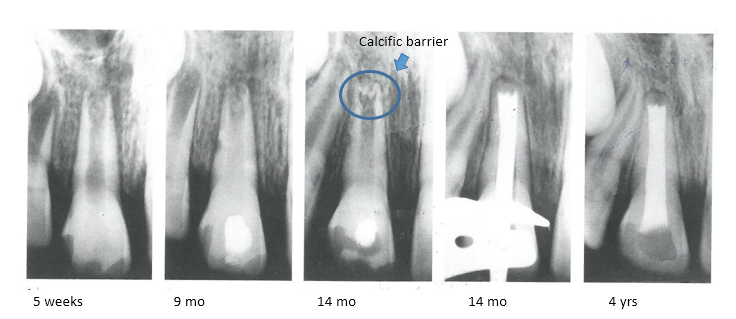
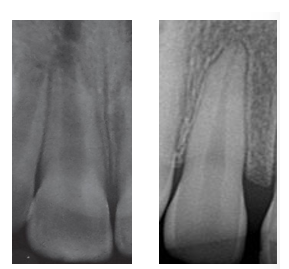
What are these series of radiographs showing?
the calcific barrier forming overtime and then oburation
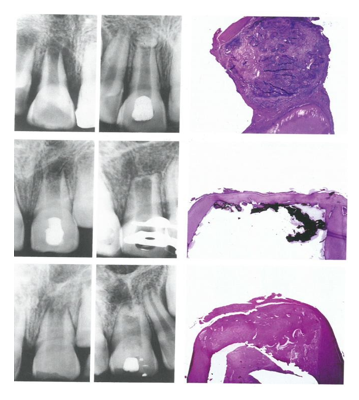
What is this image showing?
different forms of hard tissue barriers
histologically all were cementum like
can be a ball on top, tin wall, rough
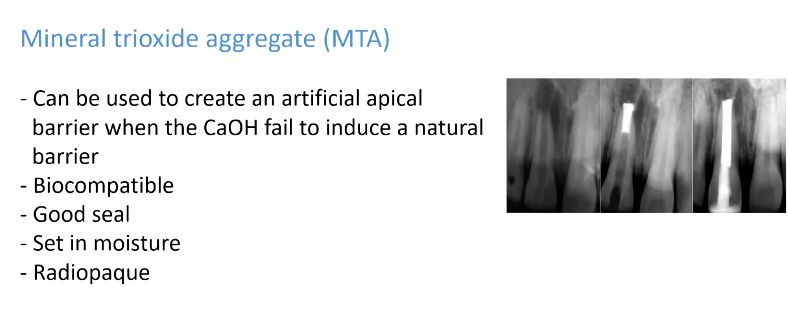
When is MTA used?
some adv?
long to wait 2 years
5 mm of MTA then the root filling material
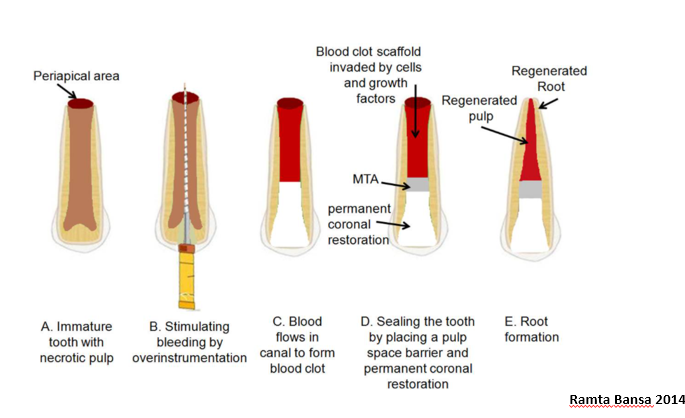
What is regenerative endodontic technique?
(non vital tooth - want the root to grow more as its short or walls too thin for better prognosis so you regenerate pulp inside canal to continue tooth growing)
Treatment procedure designed to replace damaged pulp tissue with viable tissue which restores the normal function of the pulp-dentin structure
after regenerative endodontic treatment, continued root development and hard tissue deposition on the dentinal wall can occur under ideal circumstances
What are indications for regenerative pulp procedure? (4)
Tooth with necrotic pulp and immature apex
Pulp space not needed for post/core final restoration
compliant patient/parent
patient not allergic to medicaments and antibiotics necessary to complete procedure
Generally what happens in the first and second visit?
First visit:
Disinfection of the canal using non setting CaOH or tri antibiotic paste (TAP) (ciprofloxacin, metronidazole, minocycline (part of the tetrac)) or double antibiotic paste (DAP) (ciprofloxacin/metronidazole)
second visit:
create intra-canal bleeding to form scaffolding for the pulp repair/regeneration
What happens in the first appointment in more detail?
What happens in the second appointment in more detail?
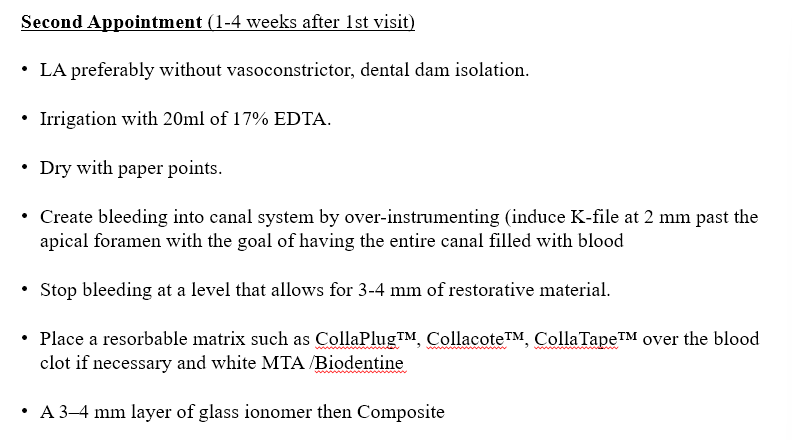
image for better visualisation: