Combined Exam 4 CLin med
1/640
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
641 Terms
117
To date, _________ countries worldwide have reported at least one XDR-TB case.
No
have most pts with MDR-TB have had a previous TB infection?
Drug-Resistant Tuberculosis
-any isolate that is resistent to one of the first-line TB drugs
Multidrug-Resistant Tuberculosis
-isolate resistant to at least Isoniazid and Rifampin
Extremely Drug-Resistant Tuberculosis (XDR-TB)
isolate resistant to at least isoniazid, rifampin, and fluoroquinolone + aminoglycoside or capreomycin or both
Totally Drug-Resistant Tuberculosis (TDR-TB)
isolate resistant to all first and second line TB drugs
• R - Rifampin (RIF)
• I - Isoniazid (INH)
• P - Pyrazinamide (PZA)
• E - Ethambutol (EMB)
first line agents against TB
-Spontaneous chromosomal mutations at a predictable low frequency.
-poor adherence bc of difficult regimens
-Monotherapy or improper drug prescriptions
-drug supply runs out or is of poor quality
how does TB drug resistance occur?
Drug-resistant TB
can occur when the drugs used to treat TB are misused or mismanaged.
Multi-Drug Resistant Tuberculosis (MDR-TB)
At risk:
• Previously treated for TB, esp if tx was inadequate or inappropriate
• When drug supply runs out or is of poor quality
• Pts infected in countries w/ high rates of resistance
• Adherent pts who are not responding to standard empiric therapy
• Close contacts of drug-resistant TB
• Drug susceptibility screening at start of Tx
• Check for resistance on those failing to improve on appropriate regimen
• Rescreen pts failing drug regimens for HIV+
what should you do for Multi-Drug Resistant TB (MDR-TB)?
Russian, Eastern Europe, China and
India
XDR-TB has its highest prevalence where?
Extremely Drug-Resistant Tuberculosis (XDR-TB)
-more associated with HIV+ status
• HIV-infected patients are more likely to have problems with malabsorption, altered drug metabolism, or drug interactions due to concomitant ART.
• This can lead to acquired drug resistance because of inadequate anti-tuberculosis drug levels and increased selection for mutations.
Xpert Ultra
technology that could replace conventional culture as primary TB diagnostic tool
Primary Ciliary Dyskinesia (PCD)
-Autosomal Recessive
• Results from absent or disordered ciliary movement
• Most commonly due to defect in dynein arm which provide energy via
ATPase
Primary Ciliary Dyskinesia (PCD)
• Recurrent otitis media, sinusitis and bronchiectasis
• 50% are associated with Kartagener syndrome
• Situs inversus
• Chronic sinusitis
• Bronchiectasis
• Males are infertile due to immotile sperm
• Chronic untreated infections lead to bronchiectasis
Primary Ciliary Dyskinesia (PCD)
Primary Ciliary Dyskinesia (PCD)
• Confirmed by electron microscopy of respiratory cilia
• Obtained by scraping/biopsy of respiratory epithelium
• Measurement of nasal NO (nitric oxide) is used as a screening tool (Will be low or absent)
• Pressure equalizing tubes for chronic otitis
• Sinus surgery although questionable benefit
• Chest physiotherapy
• Treatment of recurrent bacterial infection
treatment of Primary Ciliary Dyskinesia (PCD)
Hemoptysis
Coughing up blood or blood in the presence of sputum
Pulmonary Hemorrhage
bleeding from intrathoracic source
Hemoptysis
Refers to expectoration of blood originating from the lower respiratory tract
children usually swallow their sputum
why is hemoptysis rare in children?
Pulmonary Hemorrhage
Hemoptysis is a sign of ______________________________
Pulmonary Hemorrhage
Pulmonary Hemorrhage
Causes of _____________________:
• Pulmonary embolism
• Arteriovenous (AV) malformations
• Iatrogenic
• Congenital heart defects
• Pulmonary hypertension
• Infection
• Autoimmune disorders
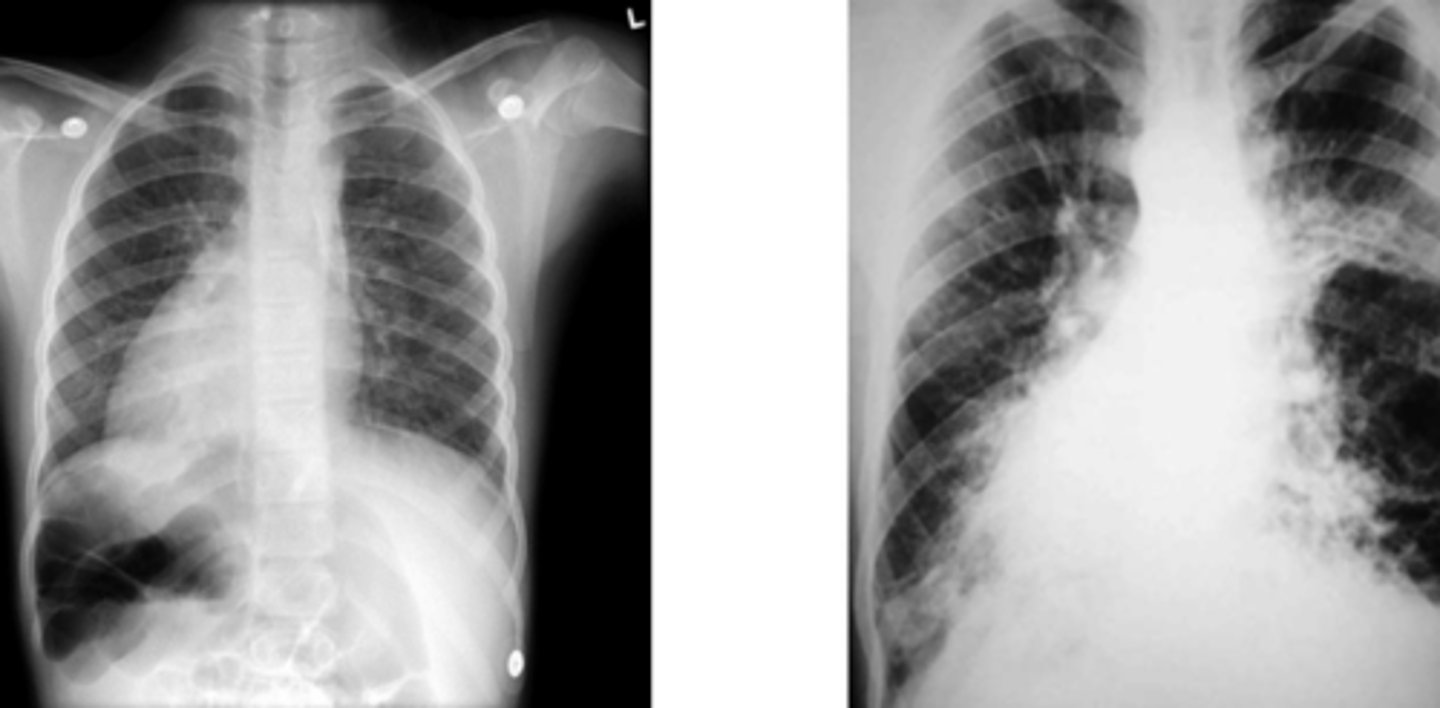
Bronchiectasis
_______________________ can cause hyperplasia, tortuosity and dilation of bronchial arteries which can erode or rupture and bleed
Pulmonary Hemorrhage
• Cough
• Wheeze
• SOB
• Pallor
• Fatigue
• Cyanosis
• Fever
• Bubbling sensation in the chest
• Increased work of breathing
Hematemesis
-acidic, coffee-grounds, contains food material
-unless massive bleeding and then may be bright red
Hemoptysis
alkaline, frothy, bright red or rust color
Pulmonary Hemorrhage
• Fever
• Weight loss
• Choking episodes
• Family illnesses
• Recent trauma
• Travel
• Hx of chronic lung disease
• Hx of congenital or rheumatic
heart disease
• Chest pain
• Calf pain
• Drug use
• Hematuria
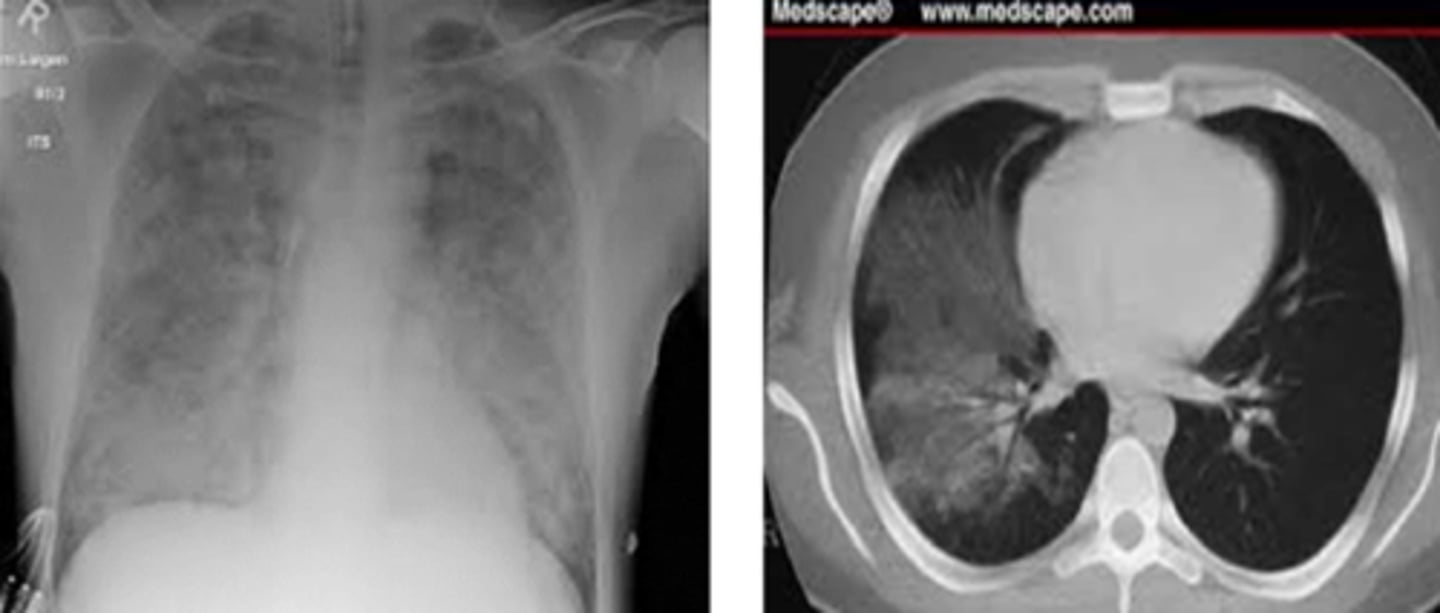
Pulmonary Hemorrhage
• Local or diffusely decreased breath sounds, cyanosis, and crackles on auscultation
• Dullness to percussion
• Calf tenderness
• Clubbing
• Murmur
• Pallor
• Bruising or bleeding gums
• Signs of trauma
• Thorough oral and nasopharynx exam
• CBC, ESR, coags (PT, PTT, INR)
• Sputum culture
• Urinalysis
• ANA and evaluation for rheumatologic disease
• Sweat chloride test
What labs/tests would you order if you suspect Pulmonary hemorrhage
• Consider nasopharyngoscopy
• CXR, CT, CT angiogram, bronchoscopy, echocardiogram
diagnostic studies for pulmonary hemorrhage
• Supportive care: Supplemental O2 & blood transfusions
• Mechanical ventilation with PEEP to tamponade bleeding
• Bronchoscopy with balloon catheter, iced saline lavage
• Embolization for bronchial arterial bleeds
• Identify underlying cause and treat
treatment of pulmonary hemorrhage
Pertussis
• Caused by Bordetella Pertussis, gram negative bacillus
• Incubation period is 6 days
• Classically called whooping cough
Pertussis
• A vaccine preventable disease
• Countries such as United Kingdom and Japan had shown increase when the vaccination rates declined
• High mortality rate is associated with infants who are not completely vaccinated
-Catarrhal Stage
-Paroxysmal Stage
-Convalescent Stage
the three stages of pertussis
Catarrhal Stage
What stage of Pertussis?
• Non specific symptoms like low grade fever and nasal secretions for 1-2
weeks
Paroxysmal Stage
What stage of Pertussis?
• Coughing in paroxysms during expiration which lasts for 2-4 weeks
• May have cyanosis, apnea, and choking during paroxysms
• Post-tussive emesis common
• Between fits children appear well and are afebrile
• Characteristic whoop sound with the cough
Convalescent Stage
What stage of Pertussis?
• Gradual resolution of symptoms in 1-2 weeks
• Coughing decreases but can persist for months
Apnea
in a neonate, ________________ can be the first presenting sign of pertussis
• PCR and nucleic acid amplification for the organism
• Lymphocytosis
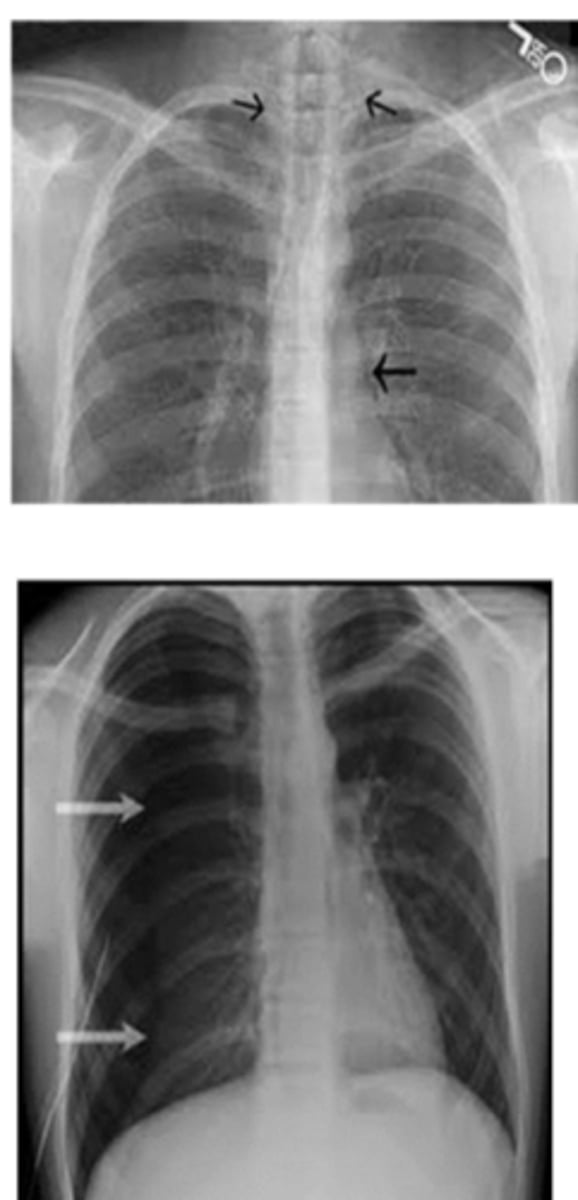
• Chest X ray findings
• Perihilar infiltrates
how to diagnosis pertussis?
Antibiotics:
• Azithromycin, Clarithromycin
• Erythromycin is avoided due to association with pyloric stenosis
Treatment for Pertussis
give macrolide and booster DTap if last dose was more than 3 years ago
Post-exposure prophylaxis for pertussis (under 7)
give macrolide and Tdap if not previously received
Post-exposure prophylaxis for pertussis (greater than 7)
Pertussis
• Apnea
• Hypoxia
• Seizures
• Encephalopathy (permanent disability)
• Secondary bacterial infections
• Strep pneumonia, Haemophilus influenza, Staph aureus
• Pneumomediastinum
• Pneumothorax
• Retinal hemorrhages
• Epistaxis
• Hernias
Pertussis
-2, 4, 6, and 15 months
-between 4-6 years
When do you give DTaP vaccine?
11 years; 10 years
Tdap is given at ___________ and every ___________ as a booster
27-36 weeks gestation
if pregnant and previously fully vaccinated, when do you give Tdap vaccine?
Bronchiolitis
• Viral respiratory infection
• Leading cause of hospitalizations in
infants
• Associated with respiratory tract
inflammation with airway
obstruction with cellular debris and
mucus plugging leading to poor air
exchange
• Can be life threatening
• Very contagious
• Spread by respiratory droplets
Bronchiolitis
Etiologies of ______________________:
• RSV*
• Adenovirus
• Parainfluenza virus
• Rhinovirus
• Influenza virus
• Human Metapneumovirus
• Coronavirus
• Prematurity
• Chronic lung disease
• Congenital heart disease
• Neuromuscular disorders
• Immunodeficiency
high risk groups for bronchiolitis
Bronchiolitis
• 50% of children under the age of two experience _________________________
• Peaks between 2-6 months
• Typically seen during Dec to March
Bronchiolitis
• Rhinorrhea
• Cough
• Raspy breathing
• Low grade temperature
• Apnea
• Intercostal, subcostal or supraclavicular retractions
• Diffuse wheezes/crackles
• Grunting
• Cyanosis
Bronchiolitis
• Mild leukocytosis
• Viral Culture (typically not done unless really ill)
• Venous, Capillary, Arterial blood gas
• Hyperinflation of lung fields
• Respiratory monitoring (Pulse ox)
• Oxygen to keeps sats > 92%
• Antipyretics
• Hydration
treatment of bronchiolitis
Warn parents that symptoms usually worsen days 3-5 and then improve
what should you tell parents when explaining treatment for Bronchiolitis?
Monthly Palivizumab, RSV monoclonal antibody vaccination
prevention of Bronchiolitis
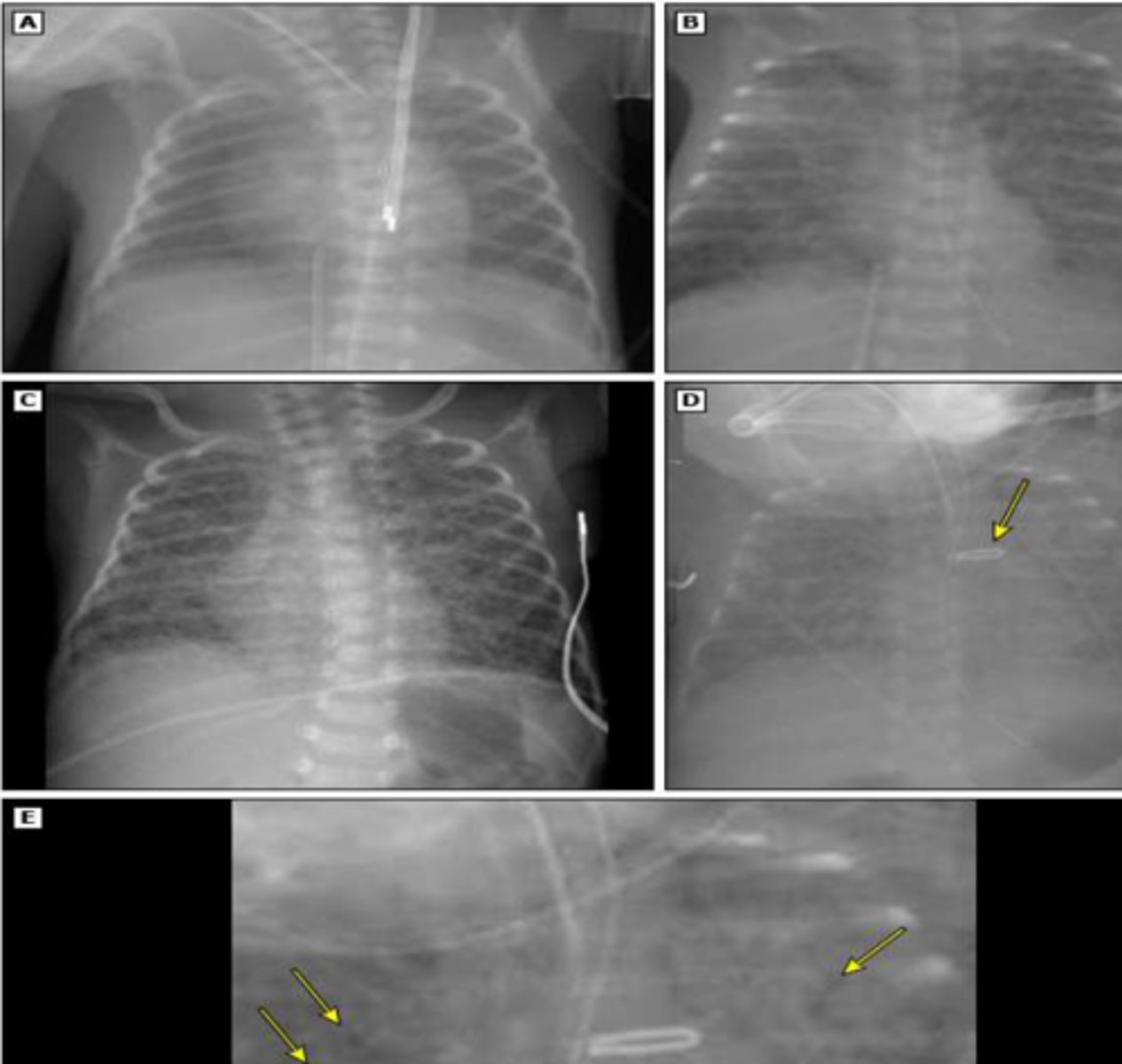
Respiratory Distress Syndrome (RDS)
Also known as hyaline membrane disease
Respiratory Distress Syndrome (RDS)
-occurs at the onset of breathing due to an insufficiency of pulmonary surfactant
• Surfactant is produced starting at 20 weeks gestation by the type II cells
• Increases and starts maturing around 32-34 weeks gestation
• Prenatally the Lecithin/Sphingomyelin ratio is a good predictor of lung maturity (> 2:1 ratio)
Respiratory Distress Syndrome (RDS)
Pathophysiology:
1. Decreased surfactant
2. Pulmonary artery vasopasm
3. Atelectasis
4. More perfusion than ventilation
5. pulmonary shunting/hypoxemia
6. Increased atelectasis decreases lung compliance
7. retractions
8. Hypercapnia, acidosis, hypoxia
Respiratory Distress Syndrome (RDS)
• Cyanosis/ Hypoxemia
• Tachypnea
• Nasal flaring
• Intercoastal or subcoastal retractions
• Grunting
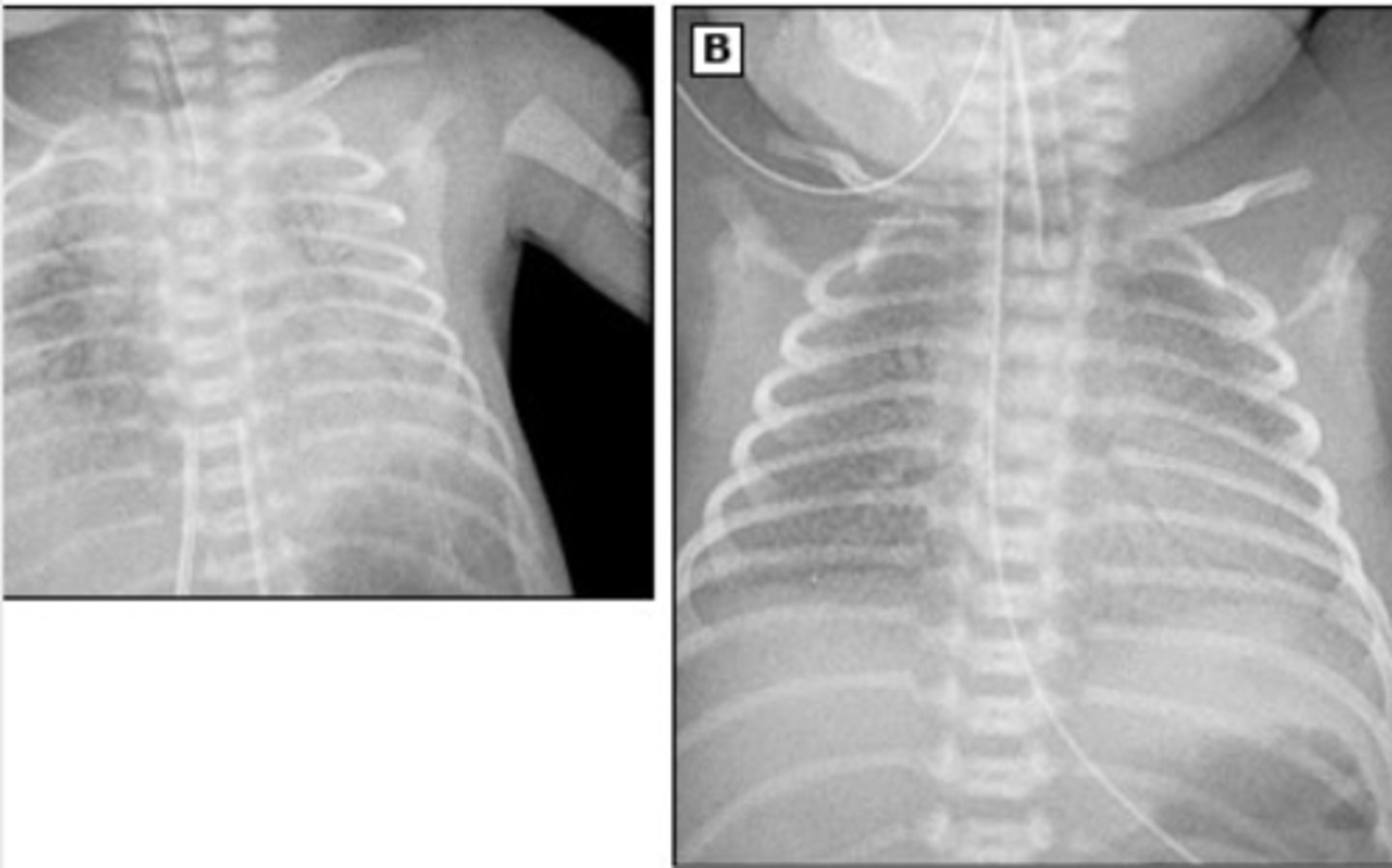
Respiratory Distress Syndrome (RDS)
Imaging shows characteristic low lung volume and diffuse reticulogranular ground glass appearance with air bronchograms
• Administration of betamethasone in mother's who are at risk for premature
delivery
• Intratracheal administration of exogenous surfactant
• Supported ventilation
• Antibiotics: Ampicillin/Gentamicin
treatment for RDS
• Bronchopulmonary dysplasia (BPD)
• Pulmonary air leaks
• Retinopathy of prematurity
complications of RDS
Bronchopulmonary Dysplasia (BPD)
• Condition of chronic lung disease due to disruption of pulmonary development and injury in preterm infants
• Infants with lung disease of prematurity who require supplemental oxygen >28 days
Bronchopulmonary Dysplasia (BPD)
• Grunting
• Nasal flaring
• Retractions
• Should be suspected in neonates who are still requiring oxygen even after
their due date
Bronchopulmonary Dysplasia (BPD)
• Pulmonary
Hypertension
• Cor Pulmonale
complications of BPD
• Ventilation
• Surfactant
• Nitric Oxide
• Corticosteroids
• Supportive: Feeding, Hydration,
Nutrition
treatment of BPD
Pneumonia
• Infection and inflammation of the lung parenchyma associated with infiltrates on CXR
• Patients often present with fever, cough, dyspnea
• Physical exam may reveal decreased breath sounds, crackles (rales), tachypnea, and respiratory distress
Pneumonia
Diagnosis is suggested by:
• Infiltrates on CXR (usually interstitial for viral and lobar for bacterial)
• Elevated WBC count (lymphocyte predominance for viral, neutrophil for bacterial)
Maternal Flora (Group B Strep) (S. pneumoniae)
etiology of pneumonia in neonates (0-3 months)
Viral Respiratory Infections
etiology of pneumonia in children 3 months to 5 years
Atypical Organisms (M pneumoniae and
Chlamydophila pneumonia)
etiology of pneumonia in school aged children (>5 yrs)
Mycoplasma pneumoniae
leading cause of bacterial pneumoniae in school aged children and young adults
-Antibiotics (if bacterial)
-Oxygen and Fluids
treatment of pneumonia
Common cold
• Acute rhinitis with variable degrees of pharyngitis
• Fever is "low grade"
• Most common acute illness in industrialized world
6
OTC cough & cold medicine not
recommended for children < ______ years old
Zinc
-alternative therapy for common cold
-esp lozenges can reduce severity and duration of cold
-may lead to permanent anosmia intranasally
-Zinc
-Vitamin C
-Echinacea
-Nasal Saline
alternative therapies for common cold
Pharyngitis
-sore throat, particularly when swallowing
-fever, headache, or malaise
-swollen glands, or anterior neck pain
-nasal congestion, coryza, hoarseness, sinus discomfort or tenderness, ear pain, or cough
Pharyngitis
Physcial Exam:
-pharyngeal erythema
-tonsillar hypertrophy
-possibly purulent exudate
-anterior cervical lymph nodes are typically tender and enlarged
-palatal petechiae
-NSAIDs/Acetaminophen, Lozenges,
• Steroids (controversial)
treatment for Pharyngitis
• Coxsackie A virus (CAV)
• Herpes simplex virus (HSV)
• Epstein Barr Virus (EBV)
viruses that can cause exudative pharyngitis
• GAS
• Mixed anaerobic
• Corynebacterium diptheriae
bacteria that can cause exudative pharyngitis
Corynebacterium diptheriae
bacteria associated with a gray pseudomembrane
• Adenovirus (AdV)
• Influenza
• Rhinovirus (HRV)
• Coronavirus (CoV)
viruses assoc with non-exudative pharyngitis
Acute Bronchitis
acute respiratory disease with severe and prolonged cough that continues after other signs and symptoms of the acute infection have subsided
Acute Bronchitis
-sputum, fatigue, chest discomfort, sore throat, mild myalgoa, NO (or low grade) fever
-Cough often lasts 14-21 days
-Adenovirus (AdV)
-Rhinoviruses (HRV)
-Coronaviruses (CoV)
-Metapneumovirus
-Parainfluenza virus
-Respiratory syncytial virus (RSV)
-Influenza
common causes of acute bronchitis
• Direct damage to the respiratory mucosa
• Release of inflammatory substances
• Increased production and/or decreased clearance of respiratory secretions
• Stimulation of airway irritant receptors
why do we cough?
Pertussis
______________ is the only indication for antibacterial agents in the treatment of acute bronchitis.
-Dectromethorphan
-Guaifenesin
-Bromhexine
-Dexbrompheniramine/Pseudoephedrine
non prescription oral medicines that may improve acute cough
Reye's Syndrome
why do you NOT give aspirin to children with a viral infection?
Reye's Syndrome
• Acute noninflammatory encephalopathy and fatty degenerative liver failure
-mitochondrial injury resulting in dysfunction that inhibits oxidative phosphorylation and fatty acid beta-oxidation in a virus-infected, sensitized host
Influenza-like Illness (ILI)
• Fever, chills, severe fatigue, myalgia, respiratory symptoms
• Systemic symptoms appear first & then respiratory symptoms predominate over the next week
Influenza, Adenovirus, Parainfluenza, RSV
causative agents of influenze-like illness