RNSG 1538- Exam 1
1/43
Earn XP
Description and Tags
Reproduction
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Pathophysiology
what is the formula for Naegel’s Rule
current month - 3 months + 7 days
Pathophysiology
According to GTPAL, what is considered a viable pregnancy
when fetus is 22 weeks or older
(G) | Gravidity = |
(T) | Term = |
(P) | Preterm Births = |
(A) | Abortion = |
(L) | Living Children = |
(G) | Gravidity = all pregnancies (miscarriages, current pregnancy and abortions included) |
(T) | Term = term births (37 weeks and above) |
(P) | Preterm Births = pregnancies that ended where the fetus was greater than 20 weeks, but less than 37 weeks completed |
(A) | Abortion = abortion or miscarriages prior to 20 weeks |
(L) | Living Children = all living children 5 |
Manifestations
what are the presumptive signs of pregnancy
Presumptive (Subjective signs)
Amnorrhea
Nausea
Vomiting
Fatigue
Breast tender
Urinary frequency
Hyperpigmentation
quickening (not a positive sign of pregnancy) → it can be gas
Manifestations
What are the probable signs of pregnancy
Probable Signs of Pregnancy
Softing of the cervix
Chadwick’s sign - blue cervix
Hagar signs
Positive pregnancy test → to check for increased levels of HCG levels
Uterine enlargement
Manifestations
What are the positive signs of pregnancy
Positive Signs (only providers can diagnose pregnancy)
Ultrasound
Associations of fetal heart tones
Palpitations of fetal movement
Complications
How is Gestational Hypertension defined
Gestational Hypertension
Greater than 140 /90 after 20 weeks of pregnancy
Can cause pre-term labor
Complications
What manifestations care indicative of pre-eclampsia
Pre-eclampsia
Elevated BP
Proteinuria (+3 or >)
Severe headache
Can cause pre term labor
Manifestations
A nurse is assessing a 2nd trimester patient and observes bright red blood. The patient reports no pain
Vaginal Bleeding, decreased fetal movement, cramps in the 2nd Trimester
Indicate placenta previa
Placenta previa is painless and there is bright red blood
Emergency c-section needs to be done
Nurse Interventions
A nurse is caring for a patients who reports intense pain and dark red blood leakage. What should the nurse do first?
Rationale:
Assess via an ultrasound
Rationale:
S/S indicate placenta abruption. The baby is being cut off from O2. A C-section must be done. Late decels appear on the FHR
Diagnostic
A pregnant person is being educated on how weeks gestation is determined. What can the nurse tell the patient
measuring from the symphysis pubis to the uterine fundus gives an estimate of gestational age
cm = gestational weeks
Diagnostic
What is the relationship between Rh Factors and Pregnancy
Mom is RH negative and Dad and baby is RH positive → up to 20 weeks or less gestation, the mom’s body can kill the baby and cause an abortion. → future pregnancies will be at risk of death due to the antibody build up.
Diagnostic
In the intrapartum phase of pregnancy, what is the
Normal heart rate:
Tachycardia:
Bradycardia
The heart rate in relationship with contractions
Normal: 110-160
Tachycardia: >160 for 10 mins
Bradycardia: <110 for 10 mins
Nurse Interventions
A nurse observes the FHR monitor and observes uterine tachysystole. What should the nurse do first
Rationale:
stop IV oxytocin
Rationale:
when there is 5 or more contractions in 10 mins. it can lead to fetal distress and low O2
Nurse Interventions
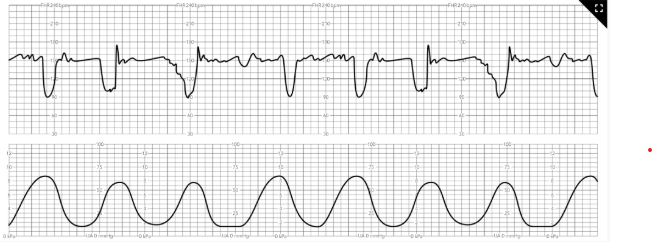
A nurse notices the FHR strip. What should the nurse do first
Rationale:
Place mother in the left lateral position
Rationale:
The strip shows variable decels. the cord is being compressed. O2 needs to be restored
Nurse Interventions
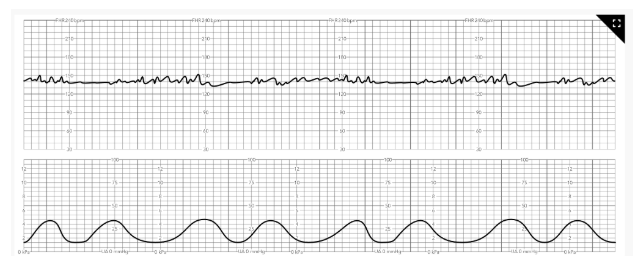
A nurse notices the FHR strip. What should the nurse do first
Rationale:
Nothing theses are normal FHR. These are called accelerations
Nurse Interventions
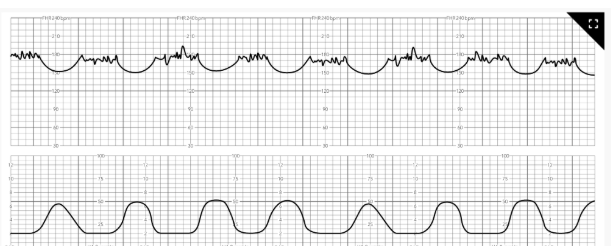
A nurse notices the FHR strip. What should the nurse do first
These are late decelerations. The placenta is not getting enough O2. An emergency C section is needed
Nurse Interventions
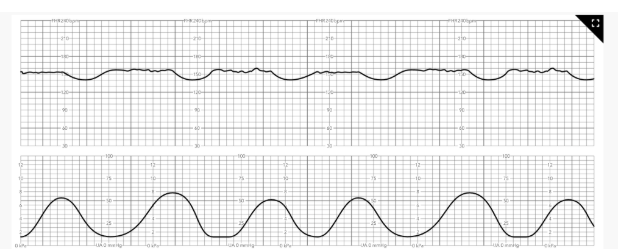
A nurse notices the FHR strip. What should the nurse do first
Nothing. These are early decels. The head is just compressing the placenta
Nurse Interventions
A patient is showing signs of pre-eclampsia. What should the nurse do
take vitals (BP)
Get a urinalysis
assess strength
place the TOCO machine below the fundus
place an ultrasound in-between the babies shoulder blades
Treatment
Metformin →
Terbutaline →
Betamethasone →
Treatment
Metformin → used to prevent miscarige
Turbutoline → to stop the contractions in pre-term labor
Betamethasone → if the baby is born pre term >34 weeks → helps with lung maturity
Treatment
A nurse is explaining when a mother with get the RhoGAM shot. What should the nurse say
Rationale:
RhoGAM shot
Will be given between 26 - 28 weeks and again 72 hours after delivery
Rationale
to reduce future pregnancies of death due to the antibody build up.
Name: Magnesium Sulfate Class: CNS Depressant MOA: Nurse Consideration:
|
Name: Magnesium Sulfate Class: CNS Depressant MOA: increasing the levels will sedate mom and reduce the risk of seizures Nurse Consideration:
|
Nurse Education
A nurse is educating a patient about fetal movement during pregnancy. What can the nurse explain to the patient
Movement of the Baby → educate that baby can be felt around 16-20 weeks gest. And is called quickening and can be felt in the second trimester
Pathophysiology
Primagavida-
Multipera-
Granmultiperida-
False contractions-
Lightning-
Bloody show-
Quickening-
Primagavida- first pregnancy
Multipera- multiple birth under 20 weeks
Granmultiperida- has had many children
False contractions- braxton hicks
Lightning- happens at 38 weeks → baby is settling and getting ready to be delivered.
Bloody show- cervical mucus acts as protective plug (happens around 38 weeks) → baby ready to be delivered
Quickening- first movement of baby at 16-20 weeks
Pathophysiology
Explain the first stage of labor (include cm dilation)
First Stage (Latent) “Cervical Dilation phase” (Active) Contraction occurs at the fundus | Dilation size: 4-6 cm Dilation size: 6-10 cm |
Pathophysiology
Explain the third stage of labor
Third Stage “Placenta stage” | Delivery of the placenta Starts: birth of the baby Ends: delivery of the placenta |
Pathophysiology
Explain the second stage of labor (include cm)
Second Stage “Pushing stage” | Dilation size: full dilation (10 cm) (the baby is pushed out and baby is born) Starts: baby is pushed out Ends: delivery of baby |
Pathophysiology
Explain the fourth stage of labor
Fourth Stage Recovery stage | Moms vitals stabilize
|
What are the most ideal fetal positions a fetus can be in to have a successful delivery
ROA- Right occiput anterior / LOA- Left occiput anterior
The baby’s face is facing towards the spine of mom
The most optional → ensures a smoother delivery
At what station must the fetus be at for optimal delivery
Zero Station = the baby is engaged (good) → the baby is born in seconds
+5 = the head is crowning
The higher the baby, the longer mom has to push
If the head is higher than 0 station there is a risk for cord prolapse
Nurse Interventions
A patient comes into the ED and has ruptured membranes. What should the nurse do to protect the mom and the baby
Rationale:
Place on monitor (fetal scalp electrode)→ to see how baby responded to rupture → the longer mom is ruptured and not delivered the risk for infection rises → c-section has to be done if infection occurs (24 hrs post rupture)
Monitor for temperature
Check every 2 hours
Mom feels warm
Reposition mom → movement can help promote baby to move into the correct position
Assess mom’s GTPAL → The more babies she has had, the easier it is to determine how smoothly the delivery will be
Admin Oxytocin for a poor dilation ( aka augmented labor) → to help move along the labor
Place mom in froggy position or lower the bottom of the bed → open up the pelvis to help with delivery
Complications
Why is fetal distress a complication during birth
Fetal distress
Will show fluctuations from the baseline. The heart rate starts to drop and doesn't come back up → leads to a late decel → emergency c section needed
Complications
A nurse is caring for a patient with a prolapsed cord. What interventions should the nurse perform
Prolapsed Cord
Medical emergency
Remove pressure from the cord
Knee chest position or Trendelenburg position → moves uterus to the side to relieve compression
Give O2 → compression of the head → low o2 to baby → poor perfusion
Complications
A nurse is helping deliver a baby. The nurse notices that the arm is coming out of the vaginal canal. What interventions should the nurse do
Shoulder Dystocia → it can break the baby’s clavicle
Shoulder stuck under the symphysis pubis
An emergency
Mc Roberts Movement- legs are held to help move the babies shoulder
Suprapubic Pressure- nurses hands over the suprapubic area
C-section needed if all measures fail
Treatment
A nurse is helping a patient during the active stage of labor. The patient is given anesthesia. The patient started to push. What interventions should be done and why
Anesthesia Epidural
Given in the active stage of labor
Epidural shuts off when it's time to push → so mom can feel contractions
A 500-1L of Normal Saline Bolus given prior to epidural → epidural can cause hypotension → leads to poor perfusion of baby
Left lateral position with wedge → to relieve support on vena cava and improve blood flow and hypotension
Pathophysiology
What are differences between vaginal blood loss and c-section
vaginal- 500 ml
C-section- 1000ml
Early Postpartum Hemorrhage-
Late Postpartum Hemorrhage-
Early Postpartum Hemorrhage- within 24 hours of birth
Late Postpartum Hemorrhage- 1-2 weeks after birth OR 3-6 weeks after birth
Nurse Interventions
A nurse is caring for a post partum patient and wants to know how much blood the patient lost. What can the nurse use to calculate the loss
Measured in grams (1gram of weight = 1 ml of blood)
All blood soaked material - dry pre-weighed material = quantified blood loss amount → this assessment helps nurses determine normal signs of bleeding or potential hemorrhage
Nurse Interventions
A nurse is helping a postpartum patient. What interventions can the nurse do to to reduce the risk of hemorrhage
Massage the Fundus of the uterus and track the amount of blood loss
2 hours post birth, admin Oxytocin IV after the placenta is delivered → detachment of the placenta leads to an increase in blood loss.
Do not give the oxytocin until after the placenta had come out → oxytocin will cause uterus to contract and prevent the placenta from being delivered
Nurse Interventions
A nurse is helping a postpartum patient.
What interventions can the nurse do to to reduce the risk of hemorrhage when the uterus is boggy upon assessment
where is the uterus located
Location: halfway between the umbilicus and the symphysis pubis MIDLINE
Position: non dominant hand at the pubic symphysis and dominant hand right under umbilicus → massage will help expel as much blood as possible via
If the uterus is boggy, you must massage the fundus→ causes contractions → reduce blood flow
Nurse Interventions
A nurse is caring for a post partum patient. Upon assessment the nurse notices that the fundus is not midline
what us suspected
what interventions can the nurse perform to have the fundus midline
The fundus is not in the midline position → she has a full bladder → it makes it hard for the uterus to contract
Assist her to the bathroom → to empty the bladder and return the fundus to midline position
Use a foley catheter if mom cant get up to urinate
Do another fundal massage
Assessment of Lochia Days | |
Days 1-3 | |
Days 4-10 | |
Days 11-21 |
Assessment of Lochia Days | |
Days 1-3 | Lochia Rubia
|
Days 4-10 | Lochia Psorosa
|
Days 11-21 | Lochia Alba
|
Nurse Interventions
A nurse is caring for a post partum patient. Upon assessment the patient states i have not bled for a week and now im bleeding really bright red blood. What should the nurse do
If the mother has not had lochia bleeding for a week, then begins to bleed bright red, she needs to go to the emergency room → she is either hemorrhaging or have retained placenta
Know the amount
Scant
Moderate
Copious
Assess for clots (golf size or bigger) → she is either hemorrhaging or have retained placenta
Oxytocin →
Methergine →
Nurse Considerations:
Hemabate
Nurse Considerations:
Cytotec
Tranexamic acid (TXA)
Oxytocin → first line drug postpartum
Methergine → the second line drug given if they can't use Oxytocin
Nurse Considerations:
Contraindicated for patients with hypertension
Hemabate
Nurse Considerations:
Contraindicated with asthma pts
Cytotec
Tranexamic acid (TXA)
Keeps the clots bunched together → to prevent the hemorrhage