Female Reproductive System
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
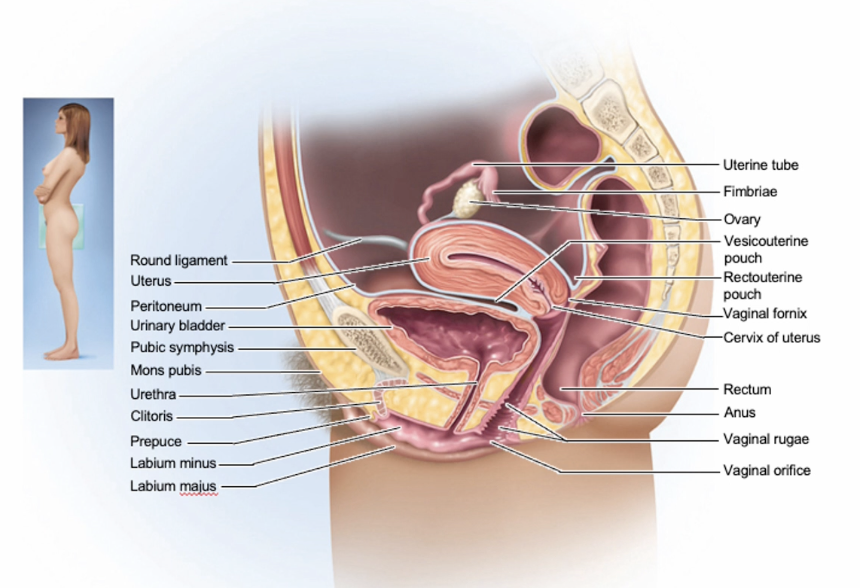
Where does fertilization commonly take place?
Within the ampulla of the fallopian tube → takes around 5-6 days to travel through the isthmus to the uterus, then implanting if fertilizing.
Puberty
begins at age 8-10 for most girls
triggered by rising levels of GnRH which stimulate anterior lobe of pituitary to produce FSH and LH
requires sufficient leptin (fat percentage) to happen
Thelarche: development of breast
Pubarche: appearance of axillary and pubic hair with apocrine sweat glands/sebaceous glands, libido
driven by androgens from ovary and adrenal cortex
Menarche: first menstrual period ~12
Female hormones secreted cyclically and in sequence
Ovarian cycle vs Uterine cycle
Ovarian → changes in ovary during and after maturation of oocyte
Uterine → preparation of uterus to receive fertilized ovum
if implantation does not occur, stratum functionalis is shed during menstruation
Aging female reproductive cycle
Hormone directed sexual characteristics start to develop at puberty
Reproductive cycle occurs once/month from menache until menopause
fertility declines with age
menopause is cessation of menstruation with fewer than 1000 follicles to stimulate hormone secretion and low estrogen and progesterone cause atrophy in the uterus and breasts and vagina
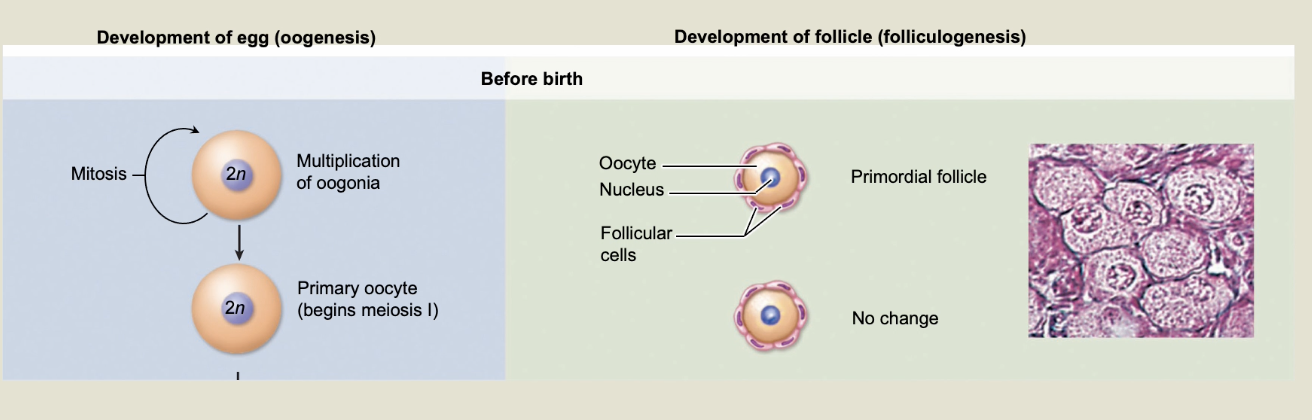
Oogenesis
mitosis of oogonia before birth
6-7 million oogonia reduced to ~2 million primary oocytes by atresia
By puberty ~ 200,000 primary oocytes remain
Only 400~ secondary oocytes ovulated
meiosis I completes just before ovulation
secondary oocyte completes meiosis only if fertilized
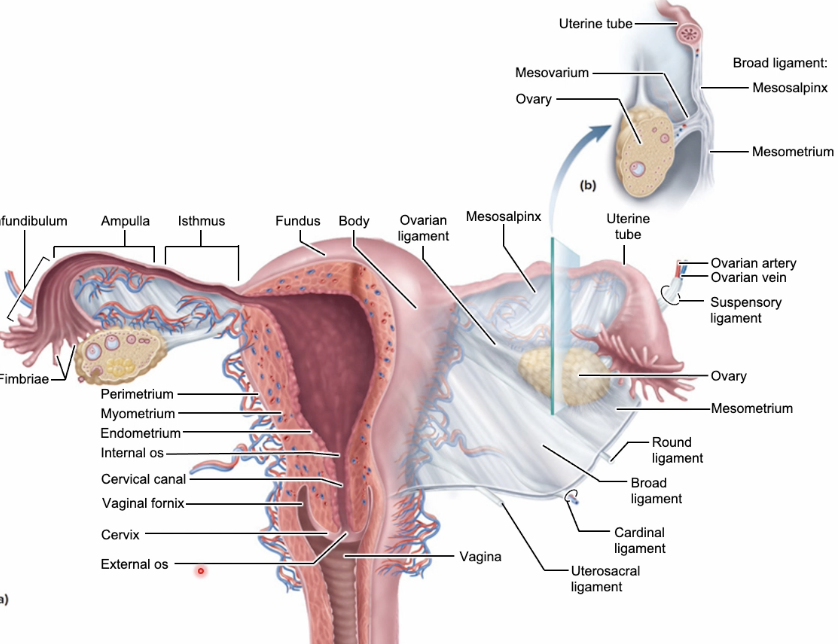
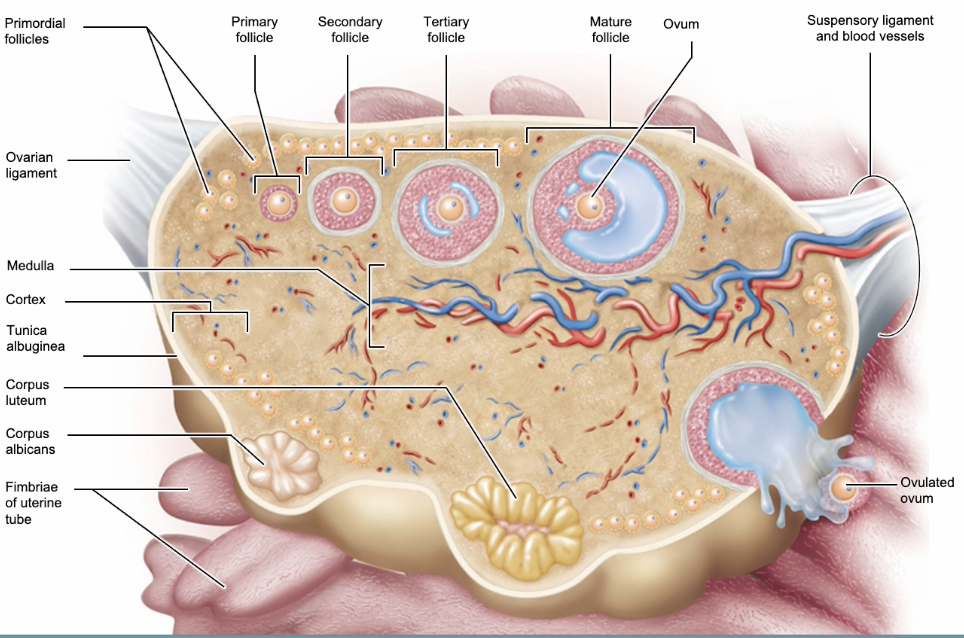
Folliculogenesis
As oogonia become primary oocytes, primordial follicles develop
cohorts of 1-2 dozen primordial follicles recruited each month
recruitment turns follicles into primary follicles with granulosa cells
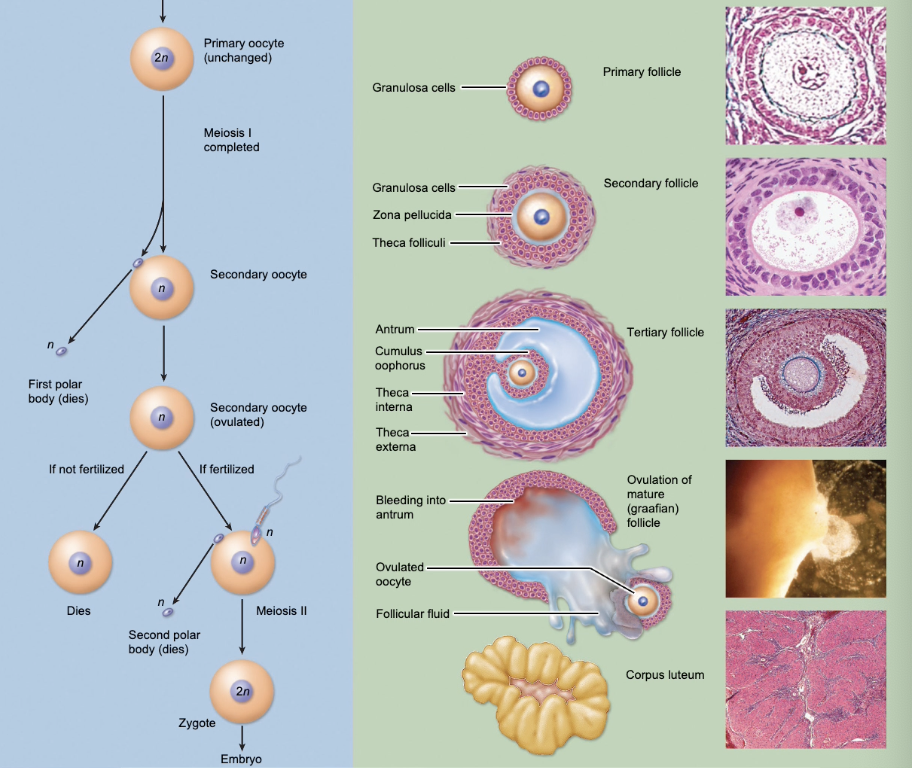
primary follicles develop into secondary follicles
thecal cells convert cholestrol into androgens (LH) and granulosa cells convert that into estrogens (FSH)
tertiary follicles are antral follices which develop follicular fluid, corona radiata, and cumulus oophorus
mature follicle is ovulated
granulosa cells: convert androgens into estrogen under influence of FSH
theca cells: convert cholesterol into androgens under influence of LH
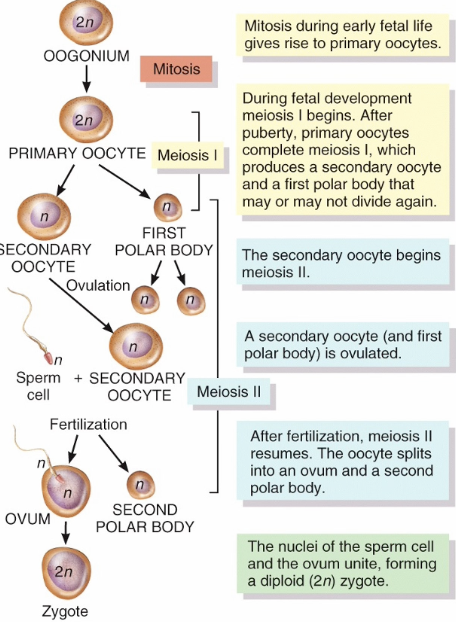
Oogenesis steps
Oogonium (2n) undergoes mitosis to create a primary oocyte (2n).
Primary oocyte goes through meiosis I to create secondary oocytes.
It produces a haploid secondary oocyte and a haploid first polar body (degenerates and is reabsorbed).
the secondary oocyte is formed before ovulation and is arrested in meiosis II until fertilized.
After ovulation, if sperm is present and fertilization takes place, the secondary oocyte continues into meiosis II.
Only secondary oocytes undergo meiosis II.
An ovum and second polar body form. The ovum becomes a diploid zygote when it unites with the sperm.
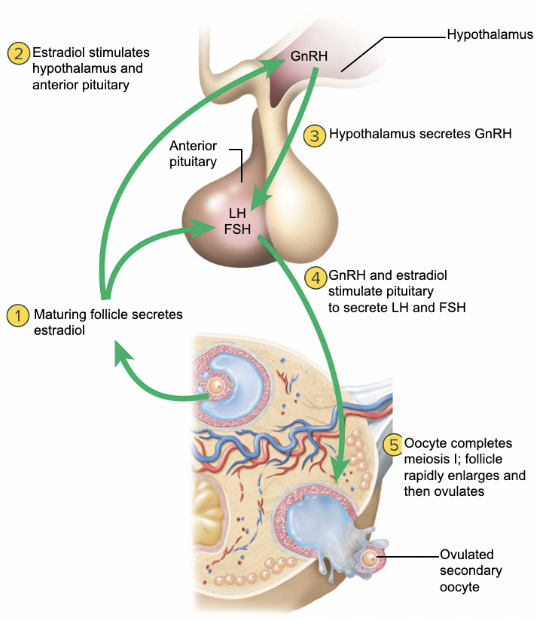
Hormonal regulation of the sexual cycle
GnRH controls the female reproductive cycle
stimulates anterior pituitary to secrete FSH and LH
FSH initiates growth of follicles that secrete estrogen → estrogen maintains reproductive organs
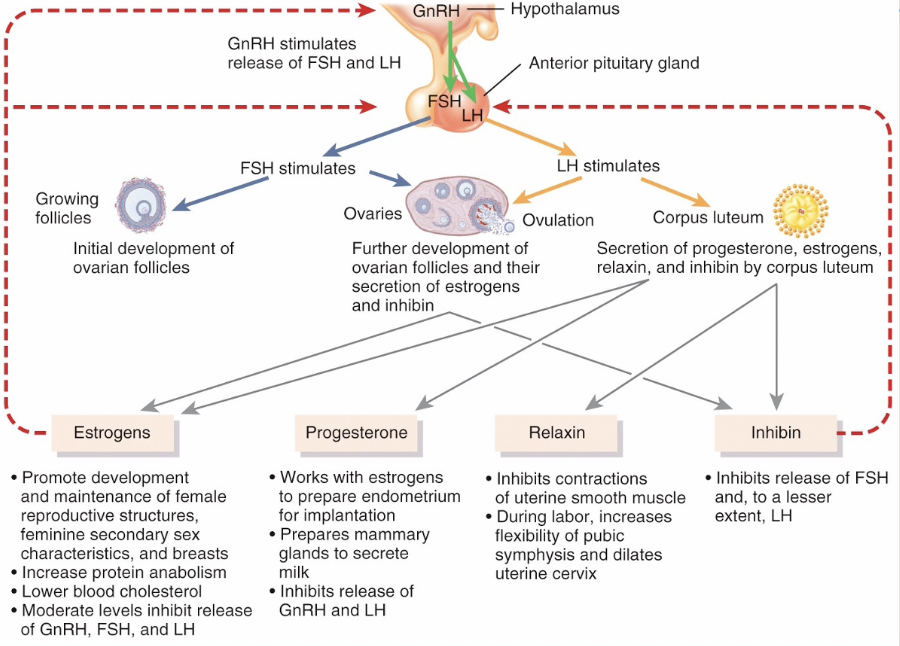
LH stimulates ovulation and promotes formation of the corpus luteum which secretes estrogens, progesterone, relaxin, and inhibin
progesterone prepares uterus for implantation and the mammary glands for milk secretion
Relaxin facilitates implantation in the relaxed uterus
Inhibin inhibits the secretion of FSH
Hormonal Regulation Chart
Sexual cycle
averages 28 days but ranges 20-40 days
Hormone cycle produces hierarchy of control
hyopthalamus → pituitary → ovaries → uterus
Follicular phase (2 weeks)
menstruation occurs during first 3 to 5 days of cycle
uterus replaces lost endometrium and follicles grow
Luteal phase (2 weeks)
corpus luteum stimulates endometrial thickening
endometrium lost again if pregnancy does not occur
Ovarian cycle and Menstrual Cycle
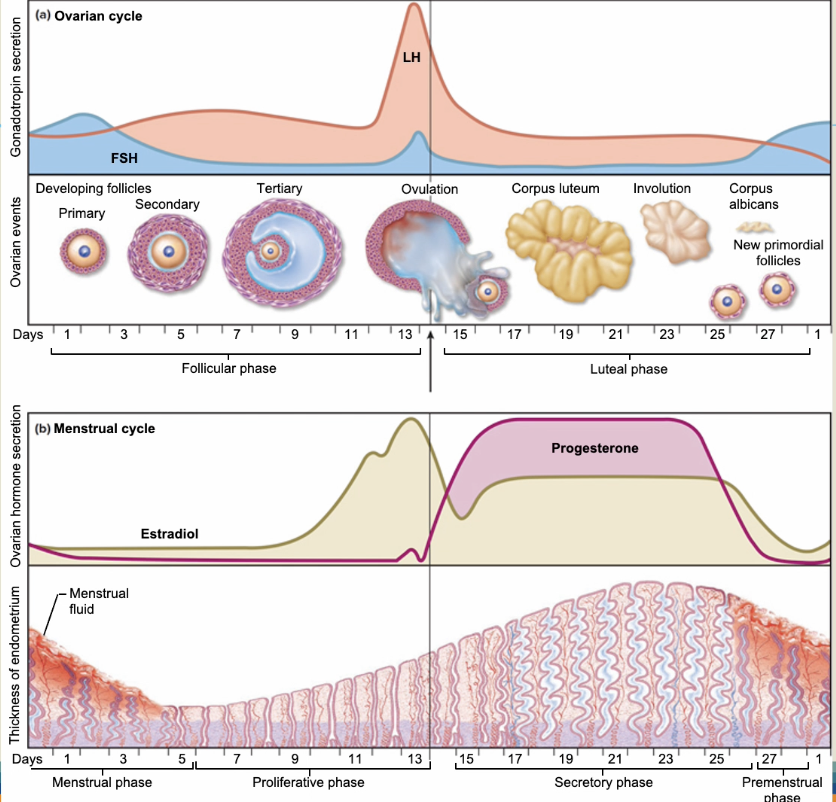
Estrogen
Released by: the ovaries or corpus luteum
Dominates the proliferative phase where it builds the endometrium
promote development and maintenance of female reproductive structures, feminine secondary sex characteristics, and breasts
Increases protein anabolism
lowers blood cholesterol
moderate levels inhibit release of GnRH, FSH, and LH
Low Estrogen Levels → Stimulates GnRH and FSH
Low estrogen occurs at the very start of the menstrual cycle (during menstruation), because the previous cycle's corpus luteum has just degraded and stopped producing hormones.
Because there is almost no estrogen in the bloodstream, the "brakes" on the brain are completely removed → The hypothalamus freely releases GnRH which commands the anterior pituitary to secrete FSH → FSH is needed to recruit immature ovarian follicles and start the next cycle
Big idea: Low estrogen stimulates (GnRH and FSH)
Moderate Estrogen Levels → Inhibits FSH and Stabilizes LH
As those new cohort of follicles grow, their granulosa cells begin secreting estrogen. By the mid-follicular phase, estrogen reaches moderate, steady levels.
Moderate estrogen binds to estrogen receptors on the hypothalamus and pituitary. It signals the brain to dial back FSH production → Method used to select the dominant follicle which will have the most FSH receptors, meaning it can survive on lower amounts of FSH
The smaller, less-developed follicles are starved of FSH and wither away, ensuring that usually only one egg matures.
Big Idea: Moderate estrogen levels inhibit FSH
High Estrogen Levels → Stimulates a Massive LH & FSH Surge
By the end of the follicular phase, that single dominant follicle grows massive and becomes an estrogen-producing powerhouse, driving blood concentrations to peak levels.
When estrogen passes a high threshold and stays there for at least 36 to 48 hours, it activates the hypothalamus → Triggers the dumping of GnRH → creates the explosive LH surge (and a smaller FSH bump) and forces ovulation.
Big Idea: High estrogen stimulates FSH and LH surge to trigger ovulation
Progesterone
Dominates the secretory phase
Stops the growth (proliferation) → alters the endometrium to secrete more glycogen, proteins, and lipids to welcome an embryo.
Prepares mammary glands to secrete milk
Inhibits release of GnRH and LH → no more making new follicles if there is an ovulated follicle that can become fertilized
Tells spiral arteries to stop contraction → more blood flow
Proliferation
Endometrium grows thicker
Relaxin
Inhibits contractions of uterine smooth muscle
Increases flexibility and dilates cervix during pregnancy
Inhibin
Inhibits release of FSH and to a lesser extent LH
It is secreted by the granulosa cells of the developing ovarian follicles (and later by the corpus luteum)
inhibin acts directly and exclusively on the anterior pituitary. It tells the pituitary to stop secreting FSH, without affecting LH or GnRH → allows for dominant follicle to grow
Ovarian cycle
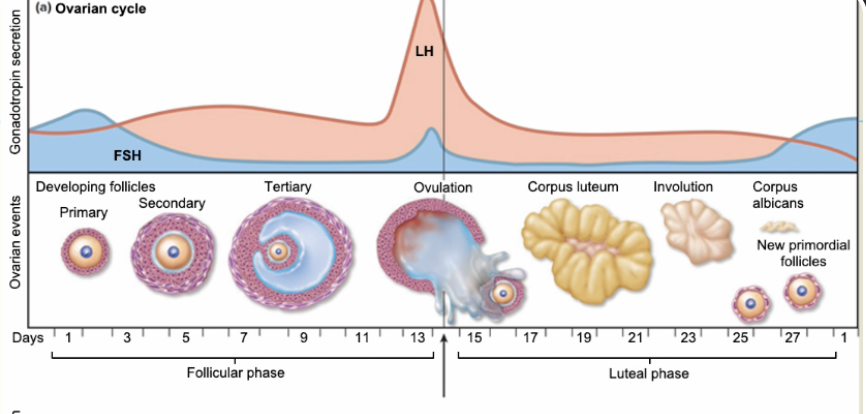
Follicular phase:
2 weeks
menstruation occurs during first 3-5 days of cycle due to low progesterone
grow a mature egg and rebuild the uterine lining.
Steps:
The hypothalamus starts releasing GnRH, which signals the anterior pituitary to secrete FSH → FSH travels to the ovaries and "recruits" a small cohort of about 15–20 immature follicles to begin growing
Next, granulosa cells surrounding the eggs start producing moderate levels of estrogen and inhibin to turn down FSH and pick the dominant follicle (most FSH receptors
The dominant follicle releases massive amount of estrogen which then passes a threshold and triggers hypothalamus to release burst of GnRH
Pituitary becomes hyper-sensitive to to GnRH → triggering the explosive LH surge (alongside a smaller bump in FSH).
Luteal Phase
2 weeks
The corpus luteum forms after ovulation → immediately starts pumping out massive amounts of progesterone and moderate amounts of estrogen → progesterone brings more nutrients and vascularization to the endometrium
Keeps ovaries suppressed by telling brain to stop GnRH, FSH, and LH release
endometrium lost again if pregnanacy does not occur
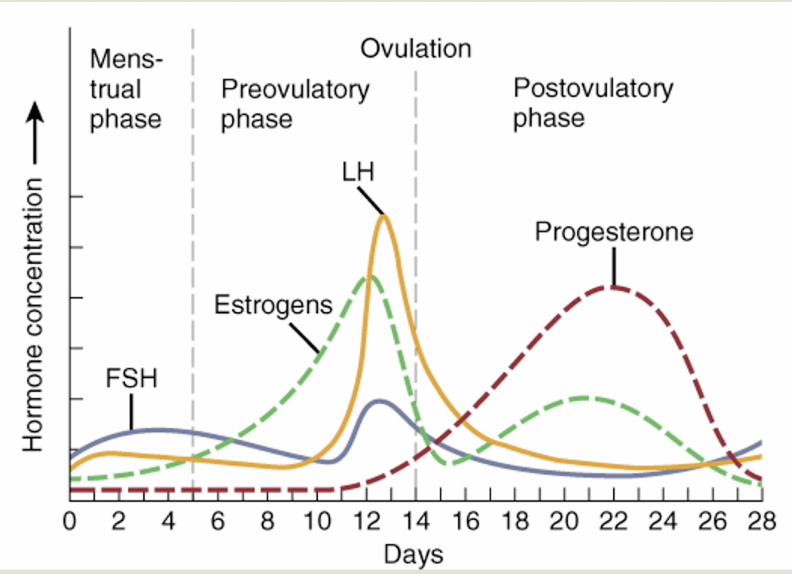
Menstrual Cycle
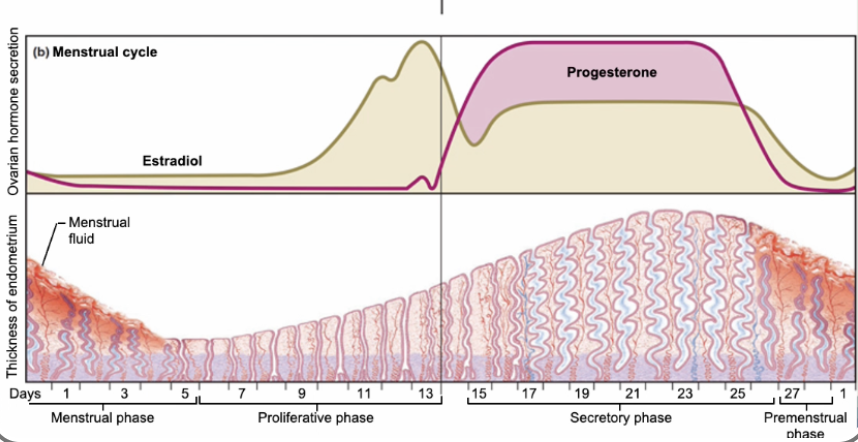
Menstrual Phase:
Lasts for 5 days
In ovary:
20 follicles that began to develop 6 days before are now beginning to secrete estrogen
fluid if filling the antrum from granulosa cells
In Uterus:
declining levels of progesterone cause spiral arteries to constrict → stratum functionalis layer of endometrium is sloughed off due to necrotizing
Preovulatory phase:
lasts from day 6-13
In ovary (follicular phase):
follicular secretion of estrogen and inhibin has slowed secretion of FSH
dominant follicles survive to day 6
by day 14, dominant follicle has been selected and matures
increased estrogen levels by dominant follicle trigger the secretion of LH by anterior pituitary
In uterus (proliferative phase):
increasing estrogen levels have repaired and thickened the stratum functionalis to 4-10mm in thickness
Ovulation → caused by elevated estrogen levels that stimulate release of GnRH which stimulates anterior pituitary to release LH (surge)
Postovulatory Phase:
Lasts 14 days
In the ovary (luteal phase)
if fertilization did not occur, corpus albicans is formed
as hormone levels drop, secretion of GnRH, FSH, and LH rise
If fertilization did occur, developing embryo secretes HCG which maintains health of corpus luteum and its hormone secretions
In the uterus (secretory phase)
hormones from corpus luteum promote thickening of endometrium to 12-18mm
form more endometrial glands and vascularization
if no fertilization occurs menstrual phase will begin
LH
Made in the anterior pituitary and stimulated by GnRH released by hypothalamus
LH binds to specific cells in the ovaries called theca cells on the outer layer of follicles → stimulates conversion of cholesterol into androgens → which granulosa cells will use FSH to convert into estrogen
As the dominant follicle matures, it pumps out massive amounts of estrogen. Once estrogen levels cross a high threshold for 48 hours, it triggers an explosive, 10-fold spike in LH release from the pituitary gland—the LH surge
Preovulatory phase
From Day 6-13
In the ovary (follicular phase)
follicular secretion of estrogen and inhibin has slowed secretion of FSH
dominant follicles survives to day 6
by day 14, mature follicle has enlarged
increasing estrogen levels trigger LH secretion
In the uterus
Amenorrhea
absence of menstruation
dysmenorrhea
pain associated with menstruation