Lung Tumours
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
Haemoptysis
Cough up blood
Name 5 Differential Diagnoses that can have haemoptysis
1. Lung cancer
2. Infection with virulent organism e.g. TB
3. Abscess
4. Bronchiectasis
5. Fungal infection
6 Differential Diagnoses for for non-resolving consolidation on CXR
1. Non-compliance with medication
2. Pneumonia d/t drug-resistant organisms
3. Pneumonia d/t unusual organisms e.g. TB, fungal
4. Atypical or viral pneumonia
5. Abscess
6. Underlying tumour
5 Differential Diagnosis for a peripherally located mass on CXR
Benign tumour (neoplasm) e.g. hamartoma
Carcinoid tumour
Primary lung cancer
Metastatic cancer
Abscess/organizing inflammation
What is required to make a Primary Lung Carcinoma diagnosis
CXR
CT (inc. PET CT)
Tissue required - biopsy
How is a lung biopsy obtained
Bronchoscopy/EBUS (Bx/aspirate)
CT guided biopsy
Smokers have a ___ fold increase in mortality by 70 yrs
20-fold ↑
Risk of lung cancer goes back to baseline how long after quitting smoking
10 yrs
What % of smokers develop lung cancer
11%
What gases are in tobacco smoke & which of them are carcinogens
CO, Nitrogen dioxide, Hydrogen cyanide, Formaldehyde
Formaldehyde is a carcinogen
Where are most of the carcinogens in tobacco smoke
Particles: 3,000 chemicals (43 known carcinogens)
Name 8 Smoking-related cancers
Mouth
Larynx
Pharynx
Lung
Oesophagus
Pancreas
Bladder
Kidney
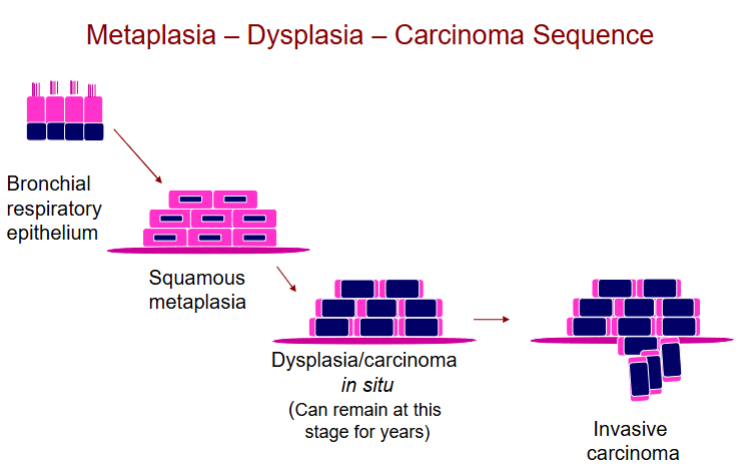
Smoking is associated with the development of what kind of carcinoma (what cell type)
Squamous Cell Carcinoma (SCC)
What are the cell changes that happen to lead to carcinoma due to smoking
Exposure to what 3 types of radiation are risk factors for lung cancer
Radon (synergistic with smoking; 25 fold inc. risk)
Uranium
Ionizing radiation (Hiroshima and Nagasaki)
Asbestos exposure leads to a what fold increased risk of lung cancer in:
Non smokers
Smokers
Non-smokers: 5-fold ↑ risk
Smokers: 50-90 fold ↑ risk
What is the general time between exposure to asbestos and the development of cancer (ie latent period)
10-30 years
Tumours arising centrally will present with what 3 main symptoms, why?
haemoptysis; cough; wheeze - due to bronchial obstruction
What fraction of tumours arising centrally involve 1st, 2nd, 3rd order bronchi
2/3rd
Tumours arising centrally are generally what cell type cancers (2)
SCC (Squamous Cell Carcinoma) or SCUC (Small Cell Undifferentiated Carcinoma)
In what layer of the lung do tumours arising centrally in lung cancer usually grow
Grow along the airway beneath the mucosa (submucosally)
Tumours arising centrally can be complicated by what 4 conditions
pneumonia, abscess, atelectasis, bronchiectasis
Symptoms of someone presenting with tumours Arising Peripherally, & why
Present late (less bronchial obstruction)
Present with cough, pleural irritation (from pleural extension), effusion
Where do Peripheral Tumours arise
1/3 arise in alveoli or terminal bronchioles
What cancer type is associated with Peripheral Tumours
adenocarcinomas
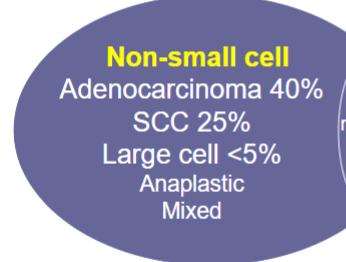
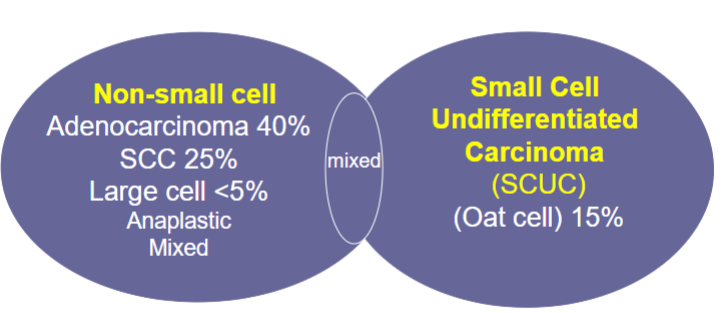
Name 5 types of non-small cell lung cancer
Small Cell Undifferentiated Carcinoma (SCUC) is aka what
Oat cell carcinoma
is Non-small cell carcinoma / Small Cell Undifferentiated Carcinoma (SCUC) more common
Non-small cell
Options for treatment for Non-small cell carcinoma
Surgery & RT & chemotherapy
Options for treatment for SCUC
Chemotherapy & RT
Match to Squamous Cell Carcinoma / Adenocarcinoma
More common in females ♀
More common in males ♂
More common in smokers
More common in non smokers
Peripherally located (mostly)
Usually express lung-specific marker (TTF1+)
Express cytokeratins & transcription factors specific for the histological type, but not specific for lung origin
Squamous Cell Carcinoma:
More common in males ♂
More common in smokers
Express cytokeratins & transcription factors specific for the histological type, but not specific for lung origin
Adenocarcinoma (AC)
More common in females ♀
More common in non smokers
Often peripherally located
Usually express lung-specific marker (TTF1+)
What do you see in Squamous Cell Carcinoma histology
Keratin/Intercellular Bridges
What 5 mutations are associated with SCC
Loss and deletions on ch 3, 9; 17
p53 mutations
Loss of Rb
FGFR1 amplification (increased growth)
EGFRvIII mutation
How are driver mutations found
Genomic testing:
Next generation sequencing (NGS)
RT-PCR
IHC
ISH
What do you see in Adenocarcinoma histology
Gland formation seen
Does SCC or AC present with metastases more
Adenocarcinoma (AC)
Where in the lung would you find the Lepidic Subtype of AC
Peripheral location
Grows along pre-existing structures/septae
Lepidic Subtype of AC structure
Single or multiple coalescing nodules
Origin type II pneumocytes, clara or bronchiolar cells
Lepidic Subtype of AC can mimic what other condition radiologically
Mimic pneumonia radiologically
There are Different subtypes of AC. Does mucinous have a good/bad prognosis
Mucinous has excellent outcome
2 main driver mutations associated with lung AC
KRAS
EGFR
True/False In AC, somatic changes are usually mutually exclusive
True - if you have 1 mutation, you won’t have another
How are EGFR mutation ACs treated (agent type & drug name)
EGFR inhibitors - erlotinib
How are EML4‑ALK / ROS1 rearrangement ACs treated (drug name)
Crizotinib
Is Small Cell Undifferentiated Carcinoma associated with smoking
Yes
Where Central/Peripheral is Small Cell Undifferentiated Carcinoma (SCUC)
Central or peripheral
SCUC presents early/late with/without metastases
Presents late with metastases
SCUC presents histologically with what
Large pleomorphic nuclei
Scanty cytoplasm
Crush artefact
Neuroendocrine differentiation of SCUC is done with what stains
H&E and IHC
What info helps us decide on TNM Staging
Imaging CT, XRay, MRI, PET, RI bone scan, US of brain, chest, abdomen and bones
Pathology (if tissue sampled and post surgery)
Lung cancers are most commonly diagnosed at what stage
Stage IV
What % of lung cancer is suitable for surgery
20%
What’s the % 5-year survival if lung cancer is localised
50% 5-year survival if localised
What’s the % 5-year survival overall
18%
Which has a better prognosis: non-Small Cell carcinoma / SCUC
non-Small Cell carcinoma
Average survival of how long for SCUC
2-9 months - most are metastatic at presentation
Which of these spreads (non-localised) 1st:
Adenocarcinomas
SCC
SCUC
SCUC

Lung also has CK20
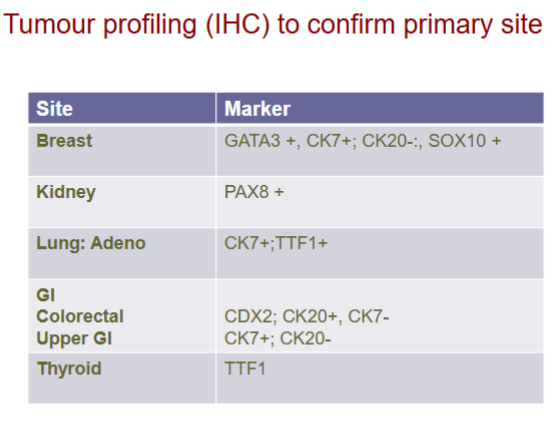
Problem with imaging of cancer with TTF1 marker cancers
Thyroid appears normal on imaging
(TTF1 → Thyroid cancer)
Lung Cancer can directly spread to where
- Regional nodes
- Pulmonary artery
- Regional organs/structures: e.g. pericardium, mediastinum, superior vena cava , cervical sympathetic ganglia (Horner’s syndrome)
Lung Cancer directly spreading to which regional structure is considered an emergency
Superior vena cava!!
What would be a sign that lung cancer spread to the SVC
Engorgement of the jugular veins
Lung cancer can spread through the blood to where
Adrenal, liver, brain, bone, breast
What is Paraneoplastic syndrome
An effect that is not explained directly by the presence of tumour or by secretion of substances native to the organ from which tumour arose (generally caused by substances the tumour secretes)
Common hormonal association with SCC
PTH (Parathyroid Hormone)
2 Common hormonal associations with SCUC
ADH
ACTH
Paraneoplastic effects of ADH with lung cancer
Hyponatraemia
Paraneoplastic effects of Parathormone with lung cancer
Hypercalcaemia
Paraneoplastic effects of ACTH with lung cancer
Cushing’s syndrome
Paraneoplastic effects of Calcitonin with lung cancer
Hypocalcaemia
Paraneoplastic effects of Gonadotrophins with lung cancer
Gynaecomastia
Paraneoplastic effects of Serotonin with lung cancer
Carcinoid syndrome
6 Common primary tumours that metastasise to the lung
Breast
Renal
Prostate
Oesophagus
Testicular tumours
Sarcomas
Malignant Mesothelioma is common/rare
Rare
Malignant Mesothelioma is cancer where caused by what (2)
Arises from mesothelial cells
Related to Asbestos exposure & smoking
Name a benign tumour
Hamartoma
Hamartoma are found how?
Incidentally - they don’t cause issues so generally found by accident
Hamartoma are generally found more in adults/children
Adults
Hamartoma structure
Mixture of mesenchymal tissue native to lung (smooth muscle, cartilage, fat) with entrapped bronchial glands
Hamartoma is found centrally/peripherally
Usually peripheral
With what form of testing are Hamartomas usually identified
Radiological features usually specific
(If not, biopsy may be necessary)
Name a neuroendocrine lung tumour
Carcinoid lung tumours
In what age group are Neuroendocrine tumour most common
< 40 yrs
Are Lung carcinoid tumours malignant
Has low-grade malignant potential
Possible risk of Lung carcinoid tumour
Carcinoid syndrome (rare)