Liver Transplants (Ch. 20)
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
OPTN (Organ Procurement and Transplantation Network) states that 1 donor can save up to __ lives
8
indications for liver transplant (MC and 2nd MC?)
severe liver disease
drugs
hepatitis C, B, and autoimmune hepatitis
cirrhosis (MC reason)
ETOH (2nd MC reason)
hepatocellular carcinoma
sclerosing cholangitis
hemochromatosis
Wilson’s disease
nonalcoholic steatohepatitis
Budd Chiari syndrome
biliary syndrome
biliary disease
biliary atresia
alagille syndrome
primary sclerosing cholangitis
liver disease symptoms
jaundice
fatigue
weight loss
ascites
black stool
itching
bleeding in stomach
confusion
nausea
loss of appetite
?? delete hepatic encephalopathy causes…
confusion from liver disease
disorientation
altered mental status
minimally responsive
contraindications
severe irreversible illness
widespread cancer
HIV/AIDS
active/uncontrolled infection
severe pulmonary HTN
active ETOH/substance abuse
poor social support
MELD and PELD
MELD (Model for End-Stage Liver Disease) and PELD (Pediatric End-Stage Liver Disease) are scoring systems
prioritize patients on liver transplant waiting list
predicts likelihood of waitlist mortality (death without a transplant within the next 3 months)
who performed the very first liver transplant? and when?
Dr. Thomas Starzl on March 1, 1963
first 5 transplant recipients died within 23 days
1967: first successful liver transplant performed by Dr. Starzl
pt. survived 1 year due to recurrent HCC
1989: first living donor liver transplant performed
cadaveric liver transplant procedure (pt. 1)
liver can be preserved between 8-12 hours on ice
donors and recipients are rechecked to verify a match
tissue and blood match
“mercedes sign” (across chest)
diseased liver is detached from its surrounding structures, and the major blood vessels are clamped and ligated
vessel alterations
anastomosed or trimmed down to size
if donor vessel is too short, an iliac artery or iliac vein graft may be used to extend it
iliac vein graft: conduit b/w recipient SMV and donor PV
iliac artery graft: conduit b/w recipient infrarenal AO and donor HA

anastomosis increases risk of what?
stenosis
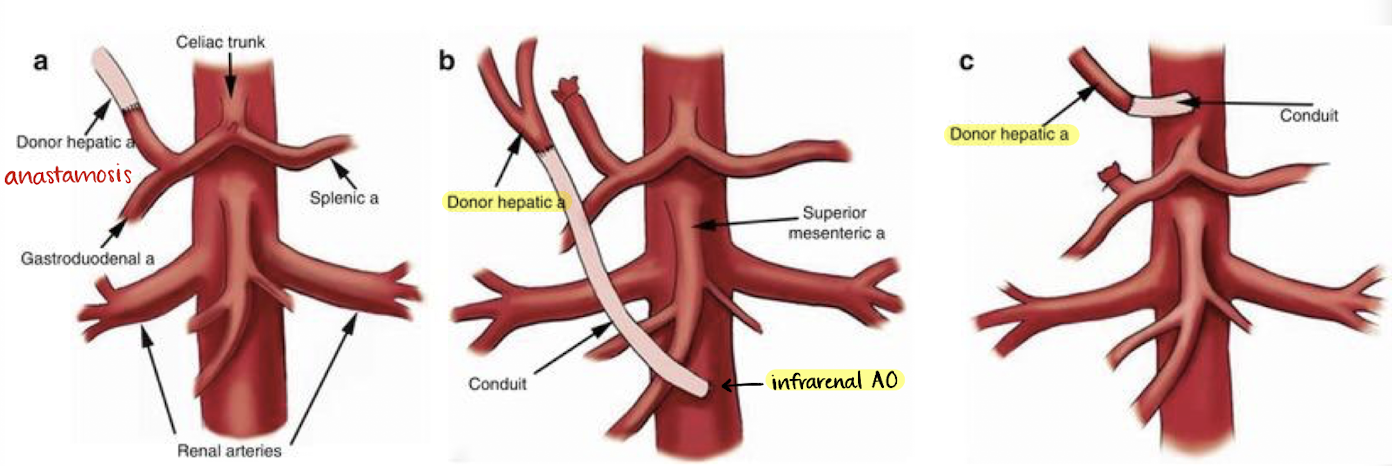
why is a conduit used in B and C?
the donors’ vessel was too short to anastomosis to the receipts’
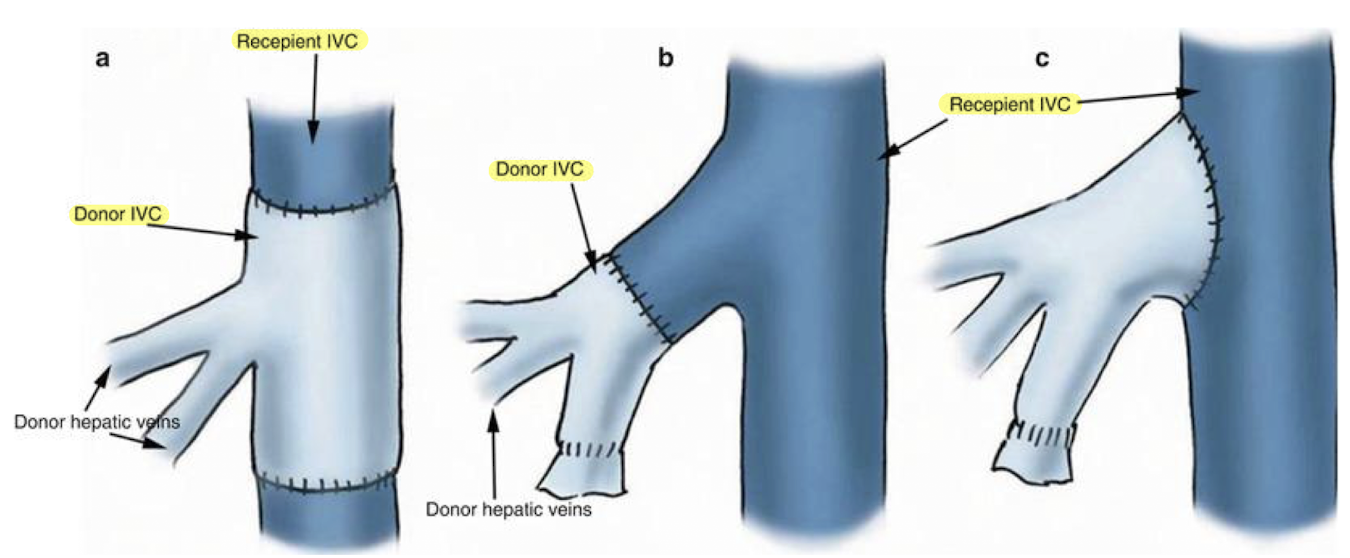
cadaveric liver transplant procedure (pt. 2)
donor IVC and recipient IVC are connected using a “piggyback” technique
donor IVC sewn end to side or within the recipient IVC)
(ANNOTATE: “IVC/IVC anast”)
end to end portal anastomosis
end to end common hepatic artery anastomosis
CBD is anastomosed
cholecystectomy is done on donor liver
sonographer should image the fossa (follow main lobar fissure—from MPV to the GB neck)
surgical drains may be placed in right and left subhepatic spaces and secured to the skin with sutures
a living donor liver regenerates to more than ___% of its original volume
85
living donor liver transplant procedures
RLL donated to a recipient; will vary (surgical report)
“mercedes sign,” vessels clamped and ligated
vessel alterations
anastomosed or trimmed down to size
iliac vein graft: conduit b/w recipient SMV and donor PV
iliac artery graft: conduit b/w recipient infrarenal AO and donor HA
living donor liver transplant procedure
end to end HV and IVC anastomosis
end to end PV anastomosis
end to end HA anastomosis
end to end duct anastomosis
drains placed posterior to liver and inferior to incision
US evaluation of liver transplant
smooth, homogeneous, and moderately echogenic
usually performed immediately post-operatively, day 1, 3, and 5, 7
document date of transplant (body can reject transplant in 10 days)
know the type of liver transplanted!!
refer to surgical report and/or previous images
assess size, echogenicity, contour, biliary tree, and vasculature
biliary stents may be present
any masses, fluid collections, or ascites present?

PW Doppler evaluation of liver transplant
evaluate for thrombus or stenosis
waveforms should fill the spectral window
PVs
HAs
HVs
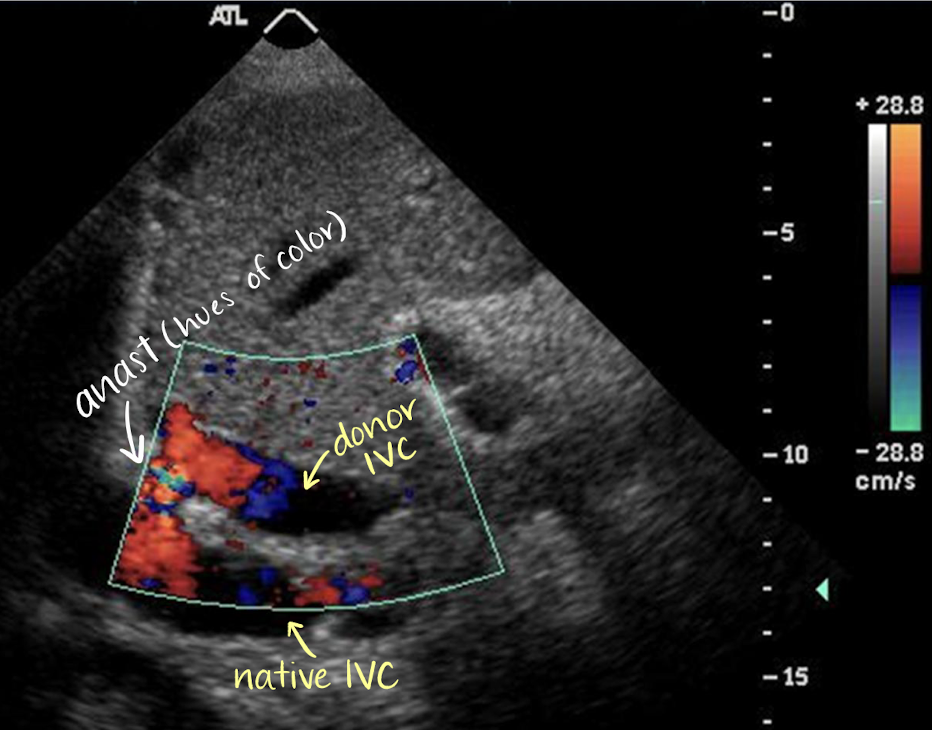
IVC/IVC anastomosis (deceased donor)
HV/IVC anastomosis (living donor)
velocity should never double.trimple at various locations
if stenosis detected, PW Doppler at and after narrowing (highest velocity)
transplant portal veins
hepatopedal (red)
continuous flow with minimal respiratory changes
<125 cm/s for PV transplant
normal PV velocity is 20-30 cm/s in native liver
above the baseline flow
Doppler at, above, and below the anastomosis
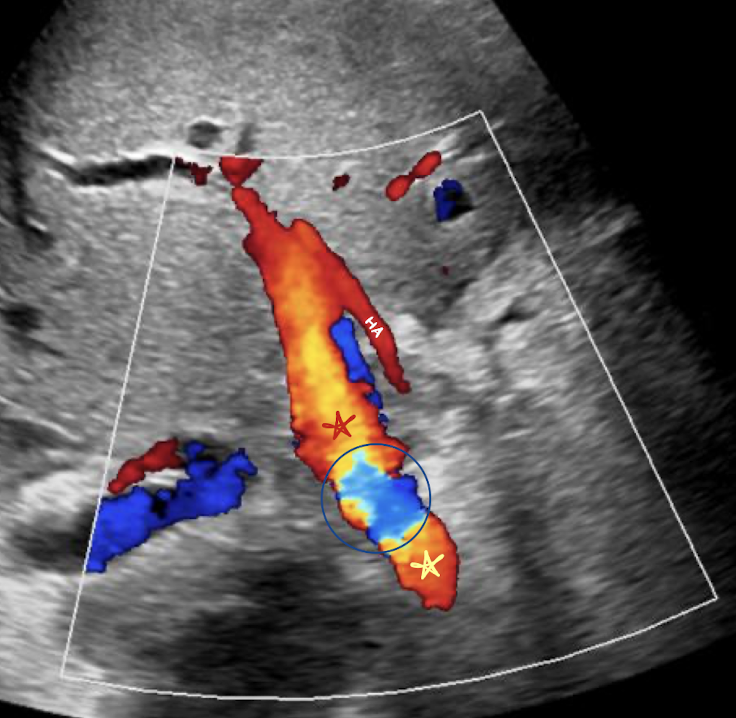
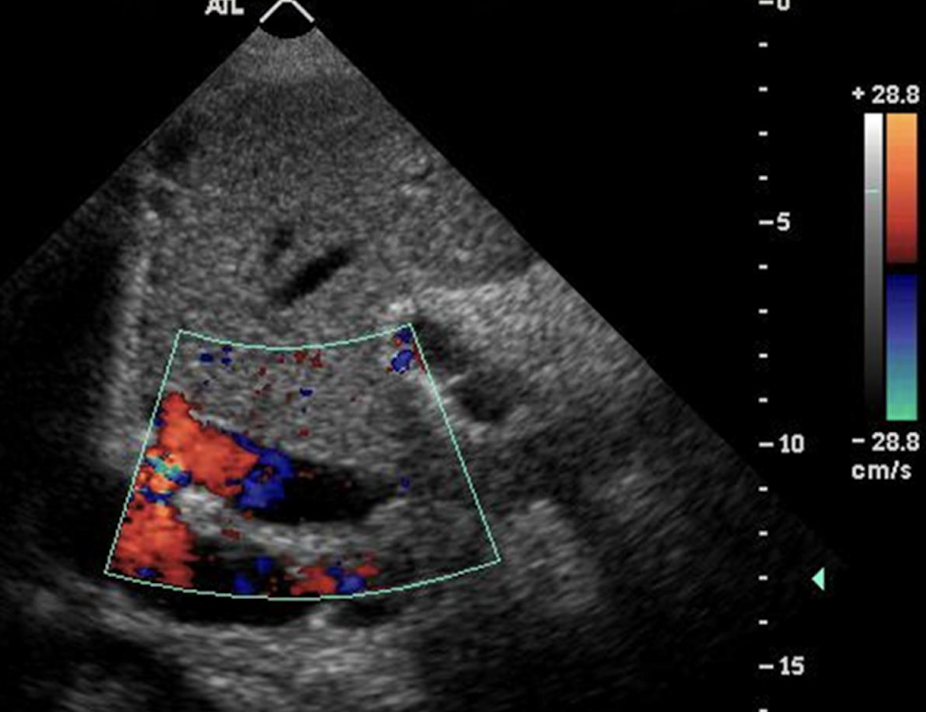
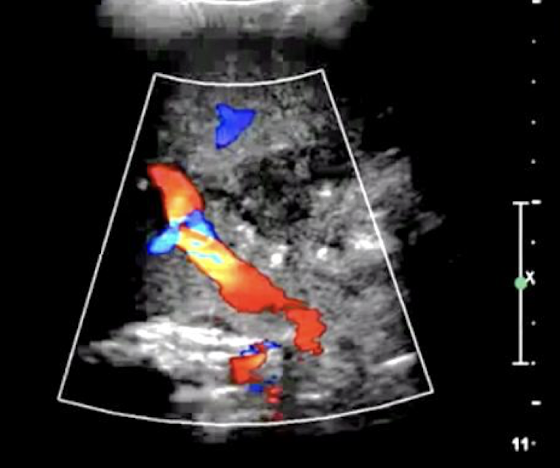
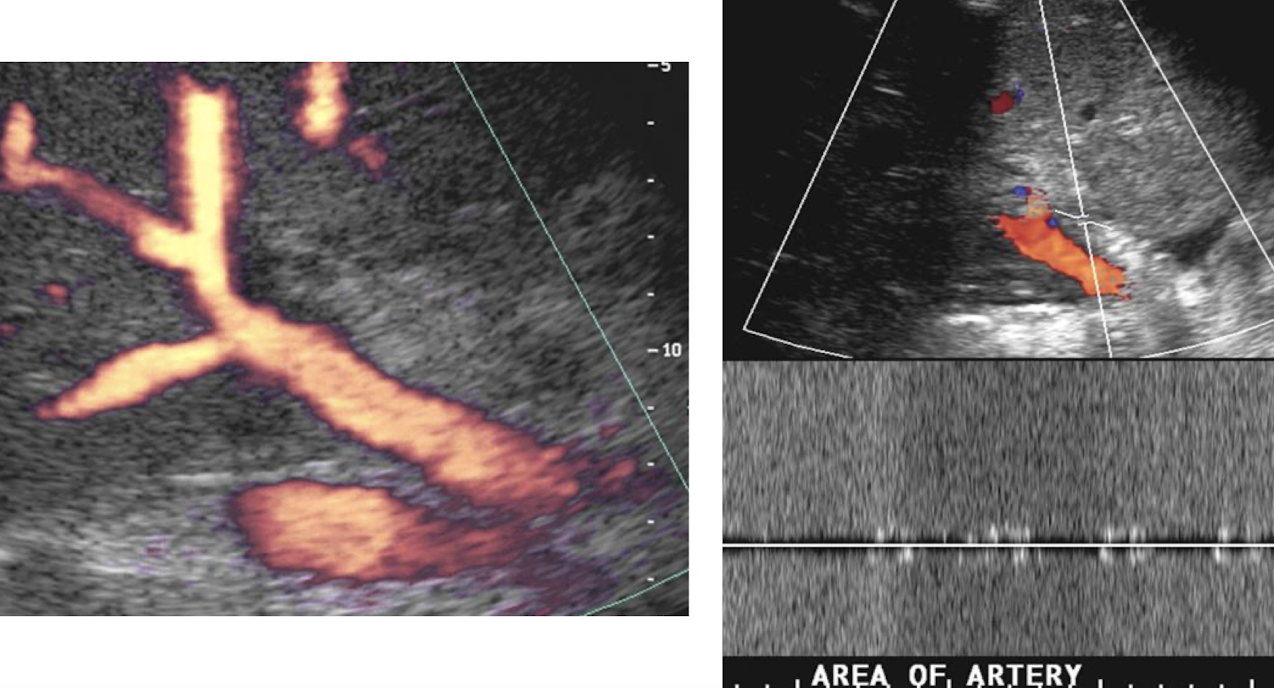
what does the red star represent? blue circle? yellow star?
red star: post PV anastomosis
blue circle: at PV anastomosis
site of anastomosis (hues of color)
yellow star: pre PV anastomosis
**velocity should not be double or triple anywhere
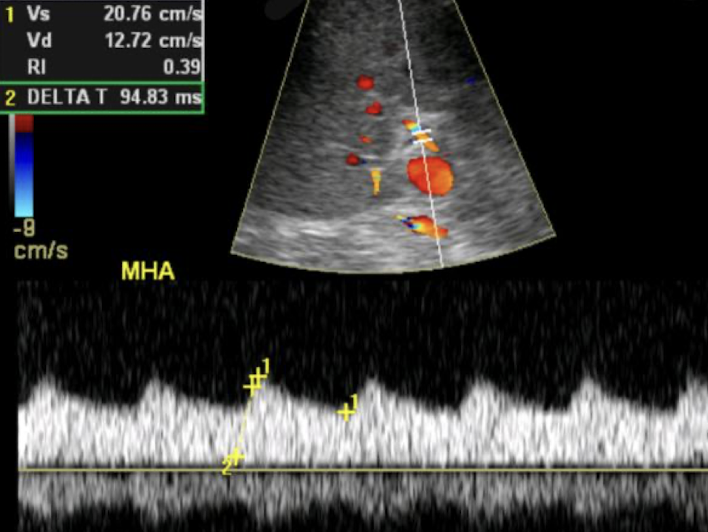
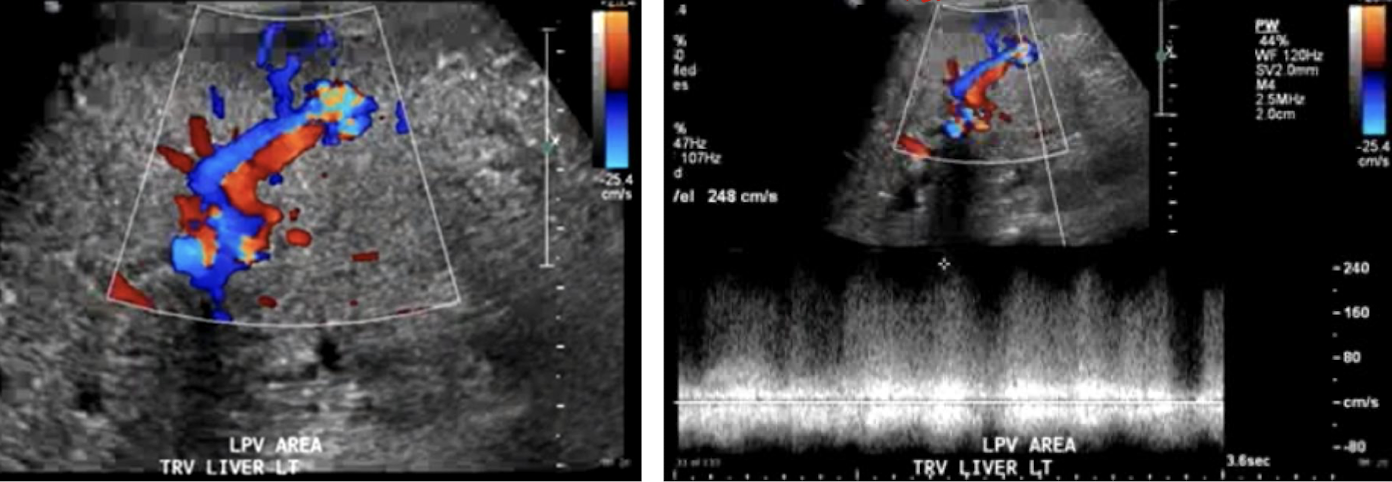
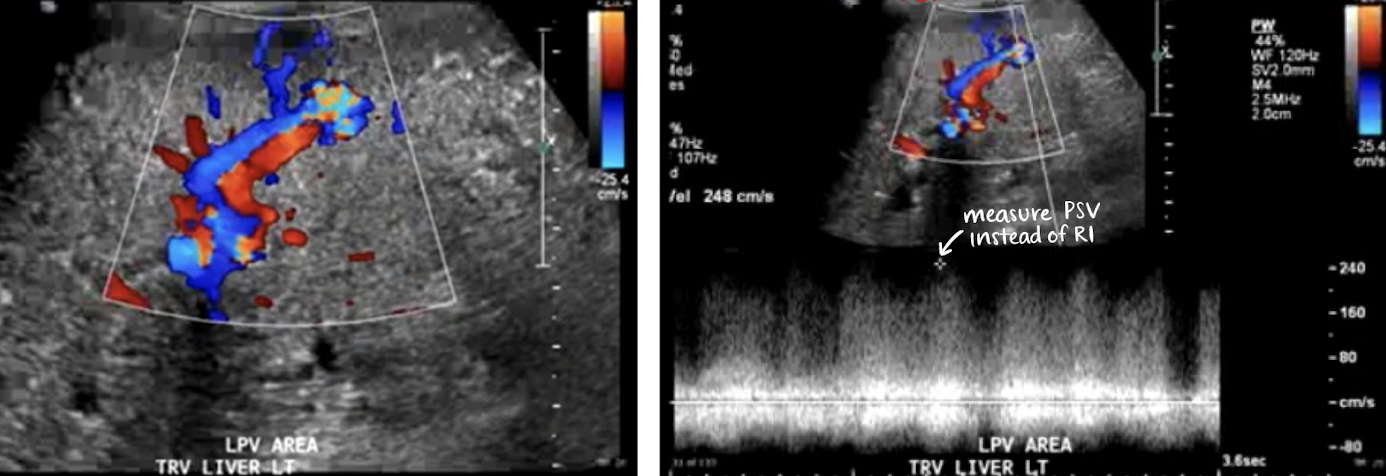
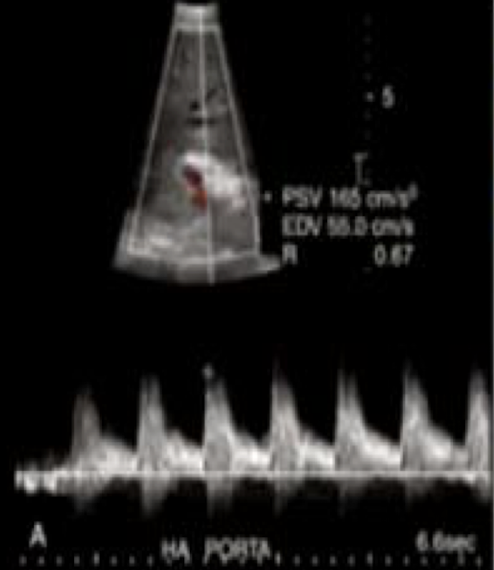
transplant hepatic arteries
resistive index of transplant HA:
normal RI (documented for each HA): between 0.50-0.70
abnormal RI: 0.80—could indicate rejection, but 0.80 is normal immediately post-op b/c of edema
low RI indicative of proximal stenosis
high RI indicative of rejection or hepatic venous congestion
rapid upstroke with continuous diastolic flow above the baseline
velocity less than 200 cm/sec
low resistive waveform—with high diastolic component

is this normal or abnormal RI for transplant HA?
normal
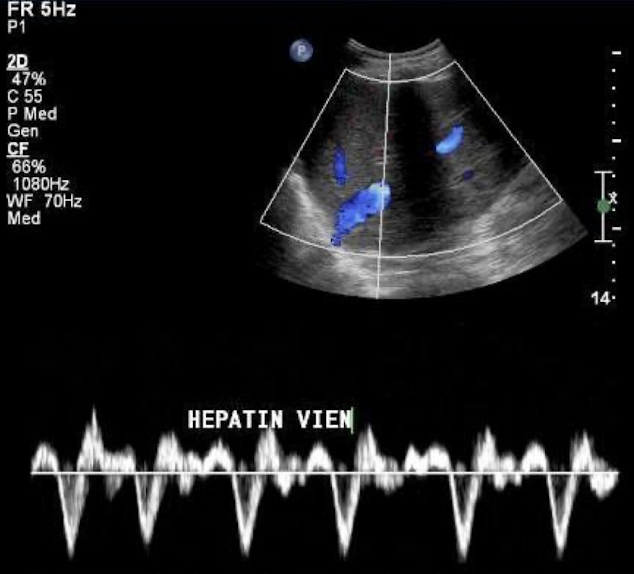
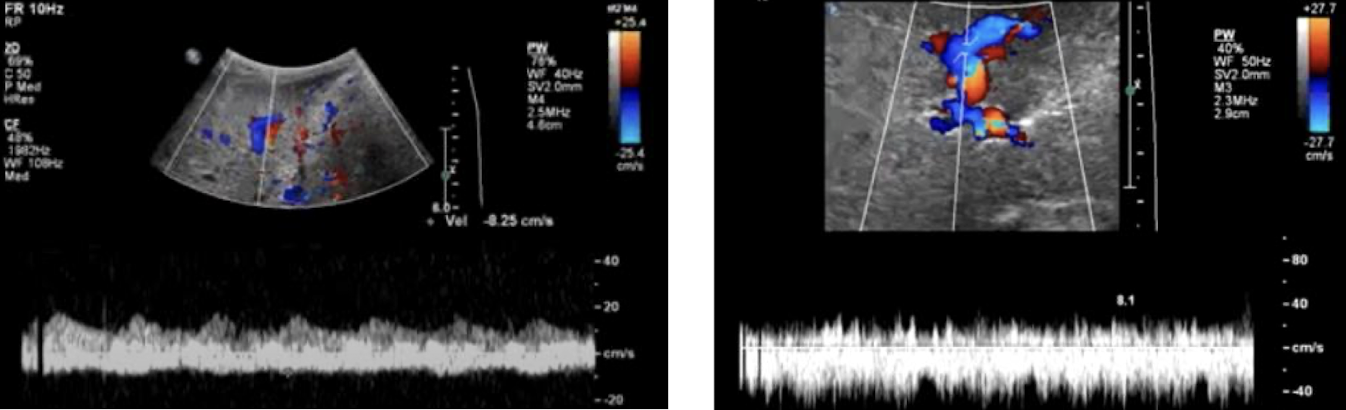
transplant hepatic veins
hepatofugal (blue)
phasic bidirectional flow—indicated by “to-fro” sign
LHV more pulsatile due to proximity to heart (common)
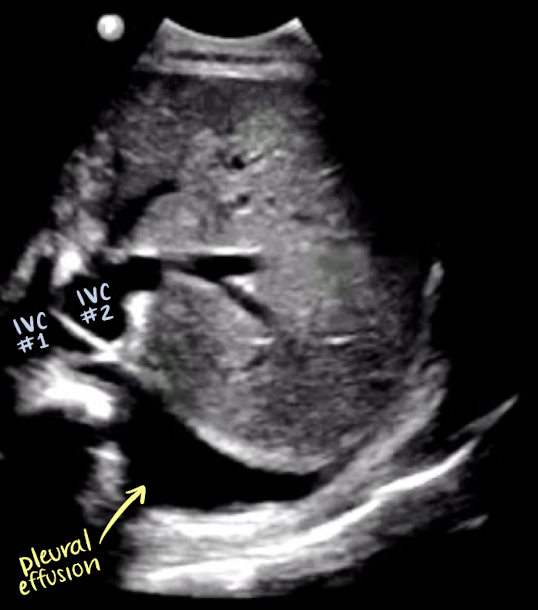
transplant IVC/IVC anastomosis
identified by aliasing
phasic and bidirectional flow
donor/txp IVC is always closer to the liver
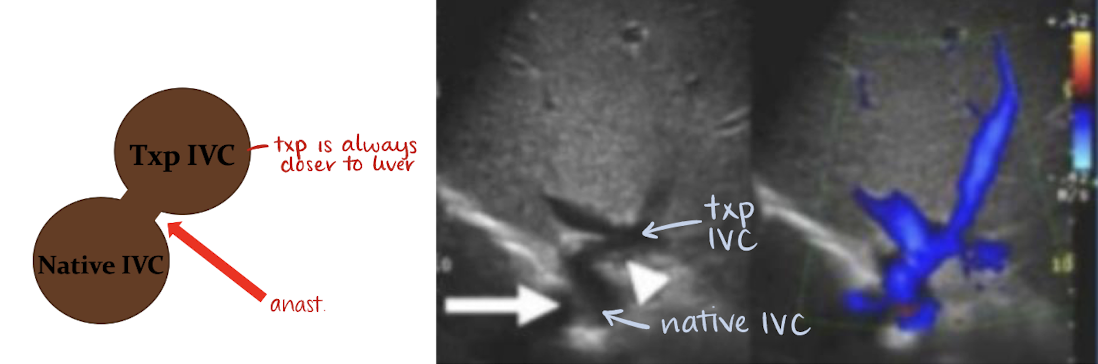
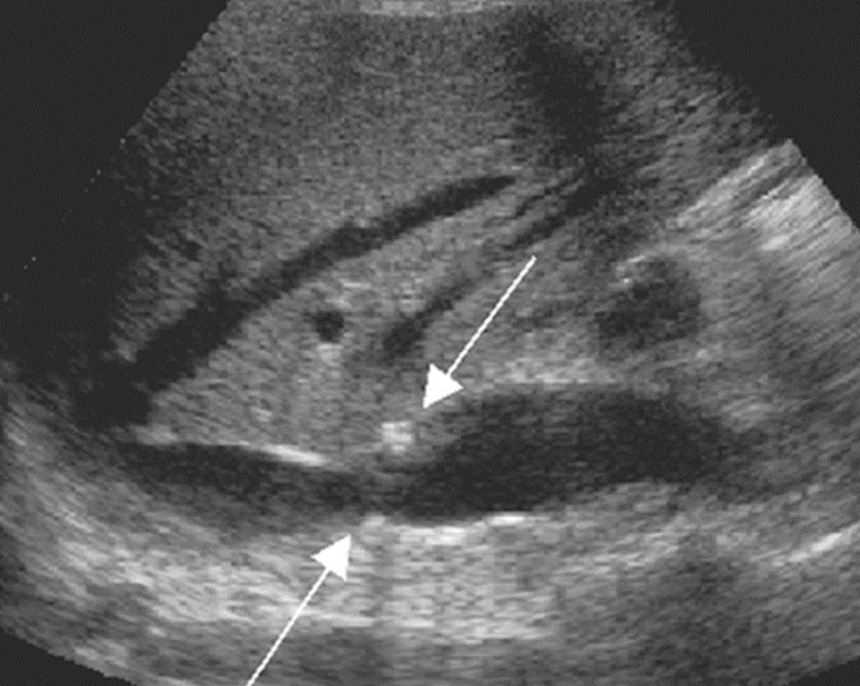
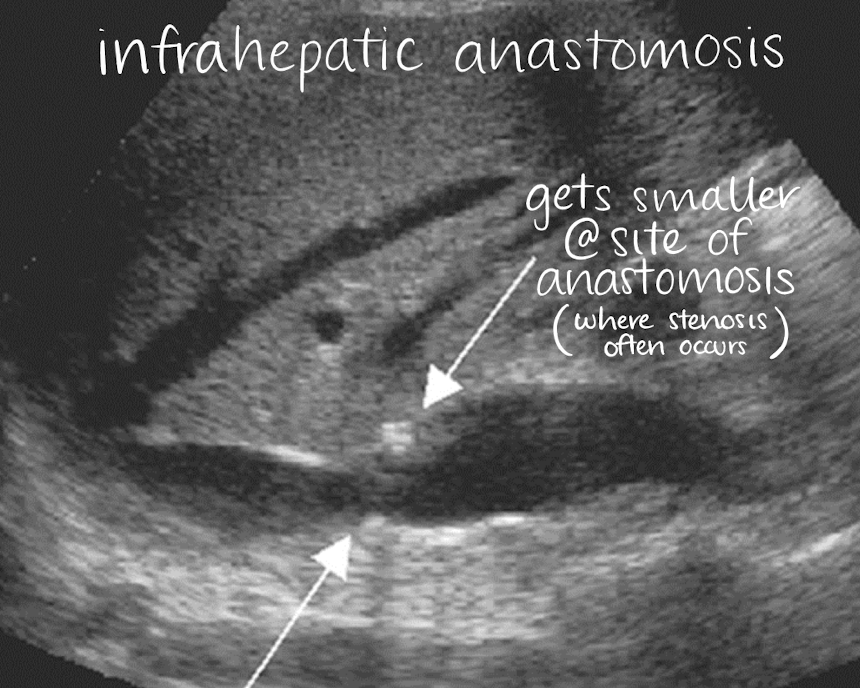
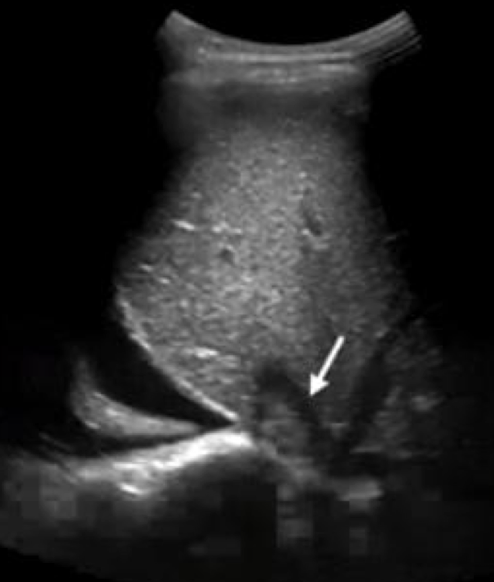
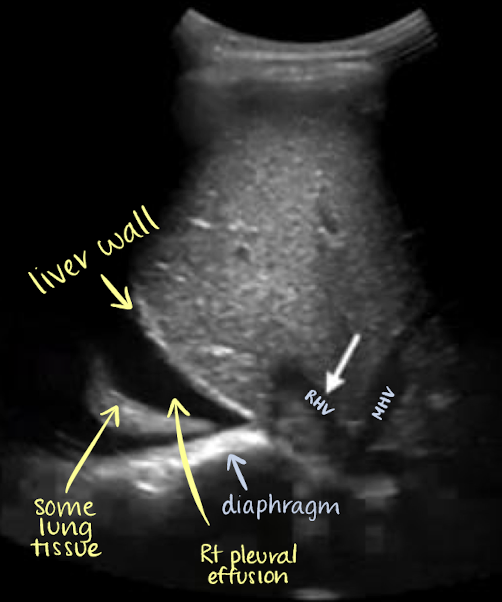
what is this showing?
infrahepatic anastomosis (below HV)
what is this showing?
postoperative imaging
flow is IMPORTANT!!
edema
can cause little to no diastolic flow and inc. RIs
fluid collections and hematomas are common
sequential evaluations to document dec. in size
within the first 2 weeks
what does increase of fluid collection post-op indicate?
active bleeding; therefore, look at previous images to ensure measurement is accurate
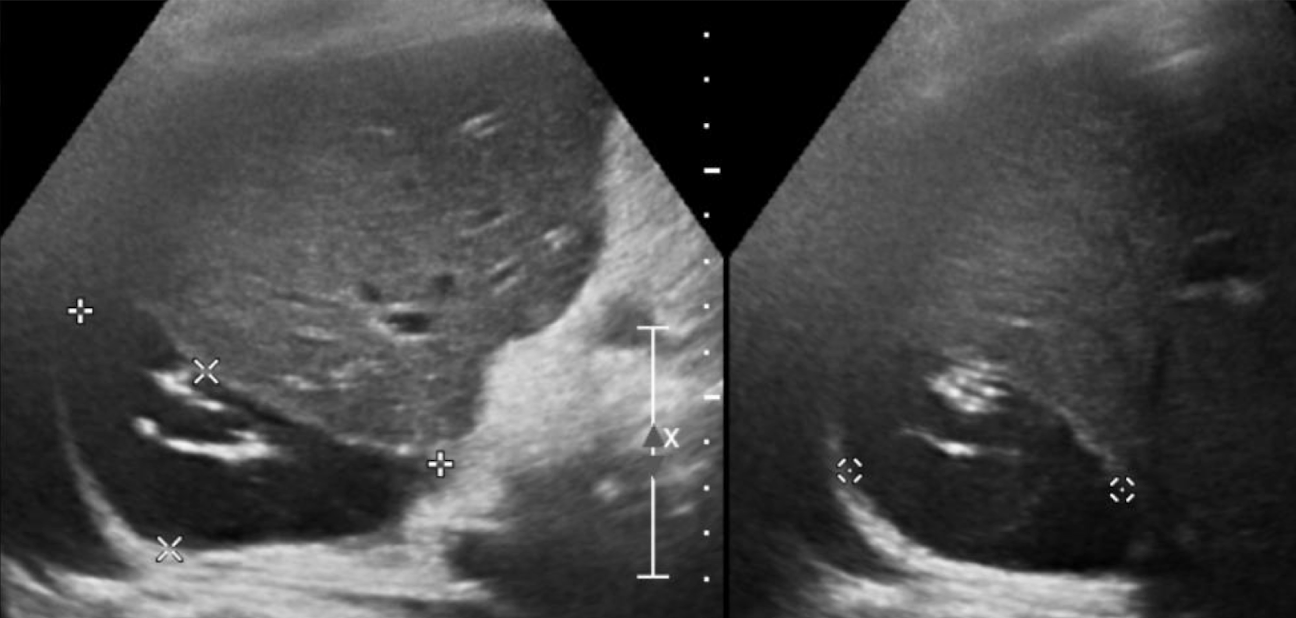
what is this showing? (3 options)
fluid collection
hematoma (if solid components within)
abscess (gas/dirty shadowing; reverberation artifact)
with abscess, pay attention to HAs—check if its patient because they’re correlated
liver transplant pathology: rejection
acute, within first 10 days of transplantation
chronic, develops over time and causes fibrosis
S/S:
RUQ pain
fever
tachycardia
hepatomegaly
ascites
elevated LFTs
encephalopathy
liver transplant pathology: infection and abscesses
thick walls
poorly defined borders
complex
gas bubbles
liver transplant pathology: HV and IVC thrombosis and stenosis
no Doppler flow
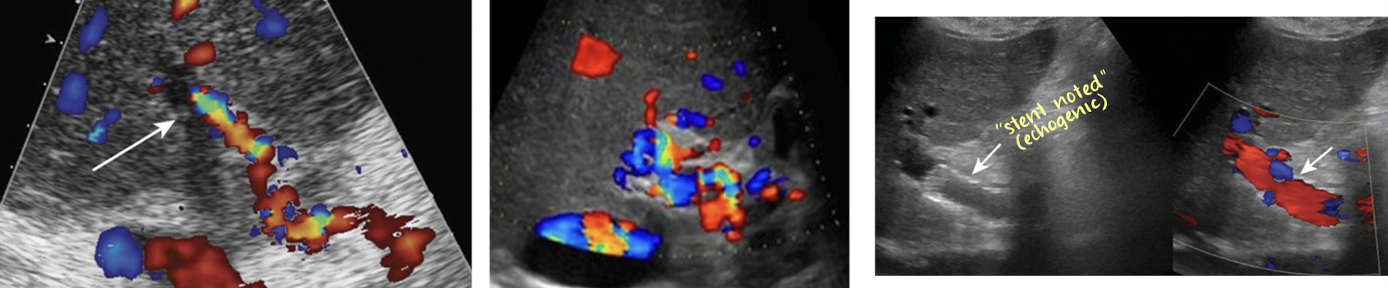
stent placement
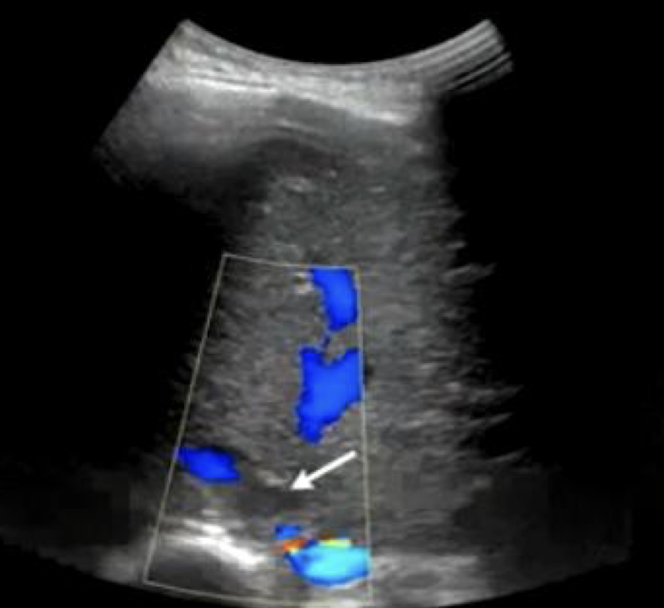
what is this showing?
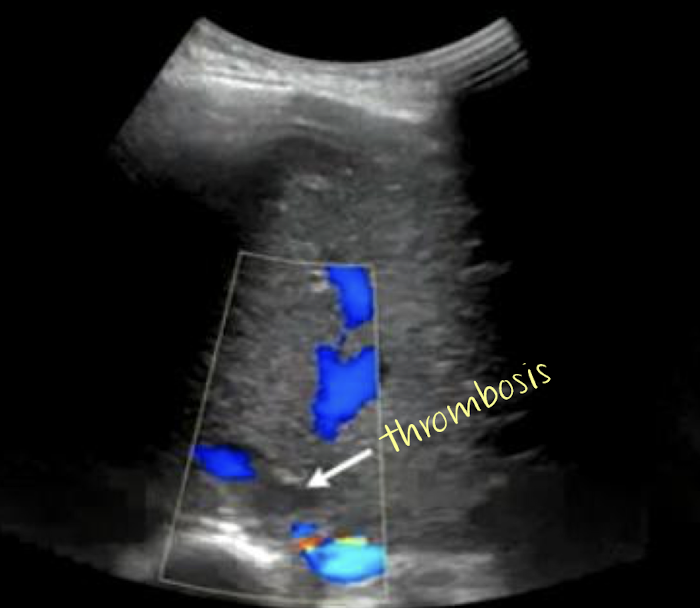
what is this showing?
liver transplant pathology: PV thrombus and stenosis
fresh/new thrombus appear echogenic; old thrombus appears anechoic
if thrombus has no Doppler flow, it is occlusive
occluded PV → cavernous transformation
stent placement
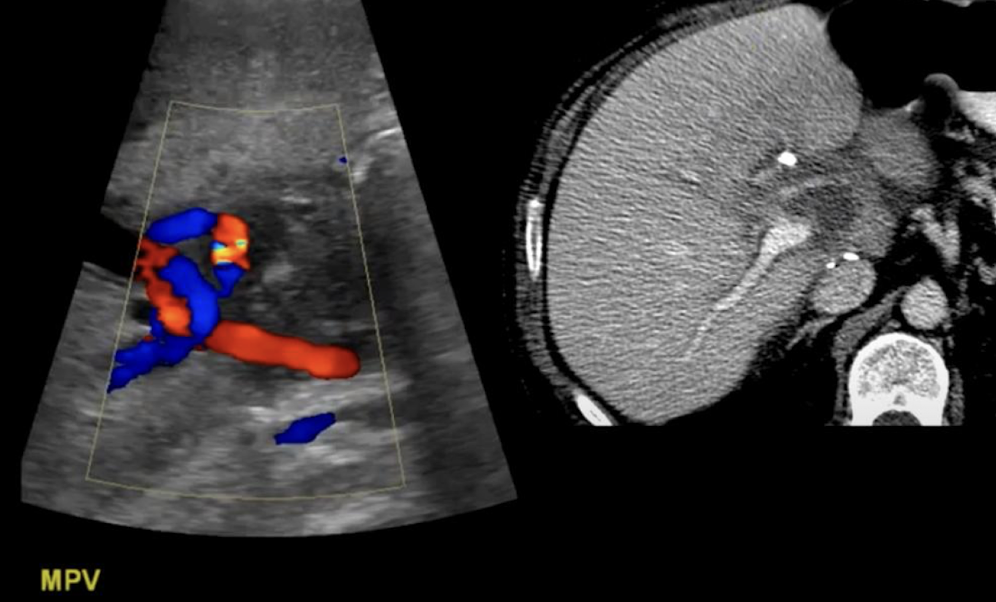
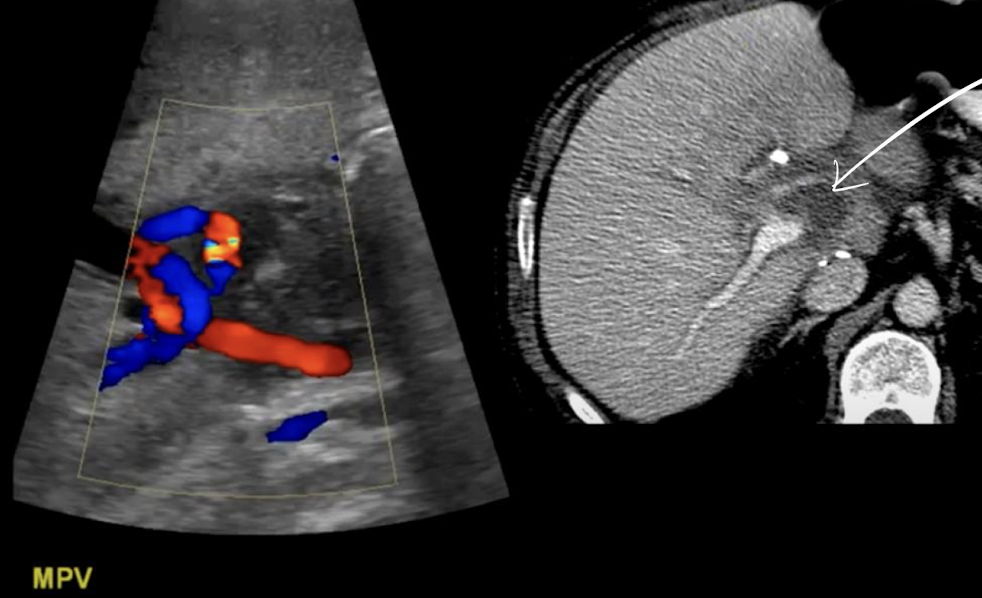
liver transplant pathology: hepatic artery stenosis
aliasing and turbulent flow
RI less than 0.50
velocity >200 cm/s
tardus parvus waveform
present distally to stenosis (very slow upstroke to peak)
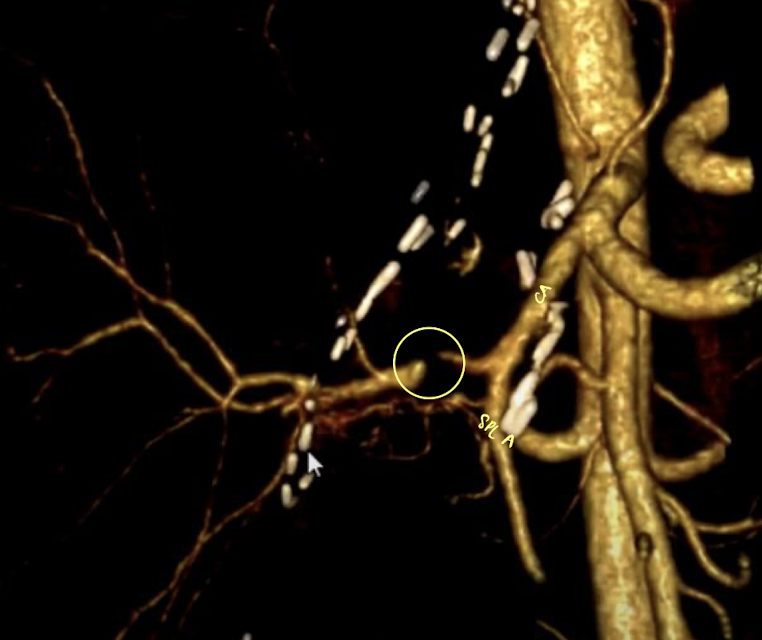
what is this CT showing?
HA stenosis—stenotic region is very thin

what do you see?
other liver transplant pathology (pt. 1)
HA thrombosis
MC vascular complication of liver transplant
leads to biliary ischemia
absence of color and no flow on spectral Doppler
HA pseudoaneurysm
biliary complications
obstruction from stricture at the anastomosis or from ductal stone
fluid collections
seromas (near perihepatic space and near vascular and biliary anastomoses sites)
lymphoceles, bile leaks, and bilomas
ascites (resolved within 7-10 days)
what is this showing?
HA thrombosis..
what should sonographer do to prove HA thrombosis
turn up PW gain to see noise
should confirm no flow to prove HA thrombosis
what is this showing? (in HA)
HA pseudoaneurysm
what is this showing?
biloma
bile leak
round
complex
in GB fossa
other liver transplant pathology (pt. 2)
hepatocellular carcinoma metastatic disease
recurrence of HCC seen in 40% of cases
hepatitis C recurrence
reinfection occurs in nearly all patients
20% develop cirrhosis within 5 years of transplantation
controversial
PV gas and bowel ischemia
if PV gas seen beyond post-op state=poor prognosis
high mortality rate of 75-90%
SONO:
echogenic foci flowing through the vein (gas within vascular system) on grayscale or entire liver parenchyma (severe cases)
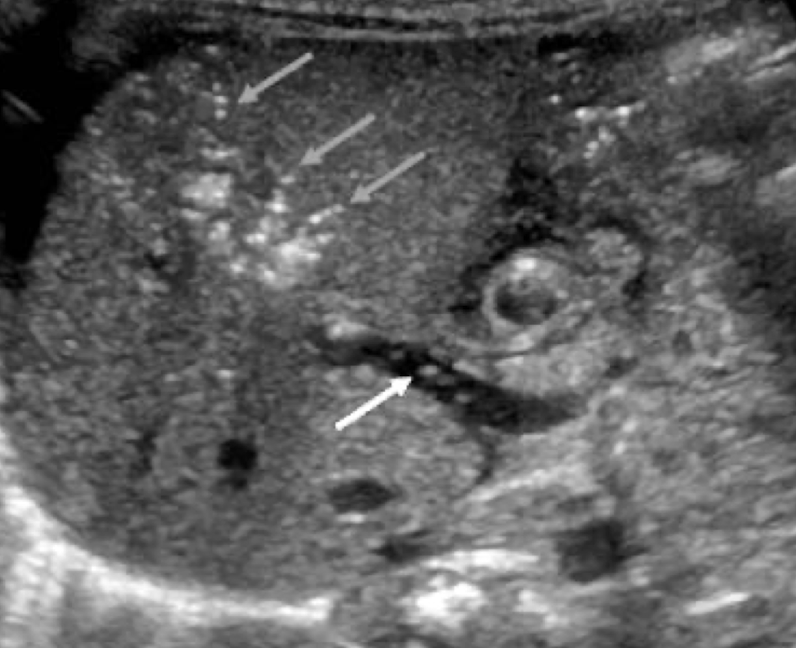
what is this showing?
portal venous gas
**emergency is air bubbles are mobile
liver transplant pathology: posttransplant lymphoproliferative disorder (PTLD)
most severe complications found in solid organ and stem cell transplantation
caused by chronic use of immunosuppressant medication
masses caused from Epstein-Barr virus (EBV)
liver transplant pathology: benign findings
cysts
hemangiomas
pneumobilia
fatty liver and focal sparing
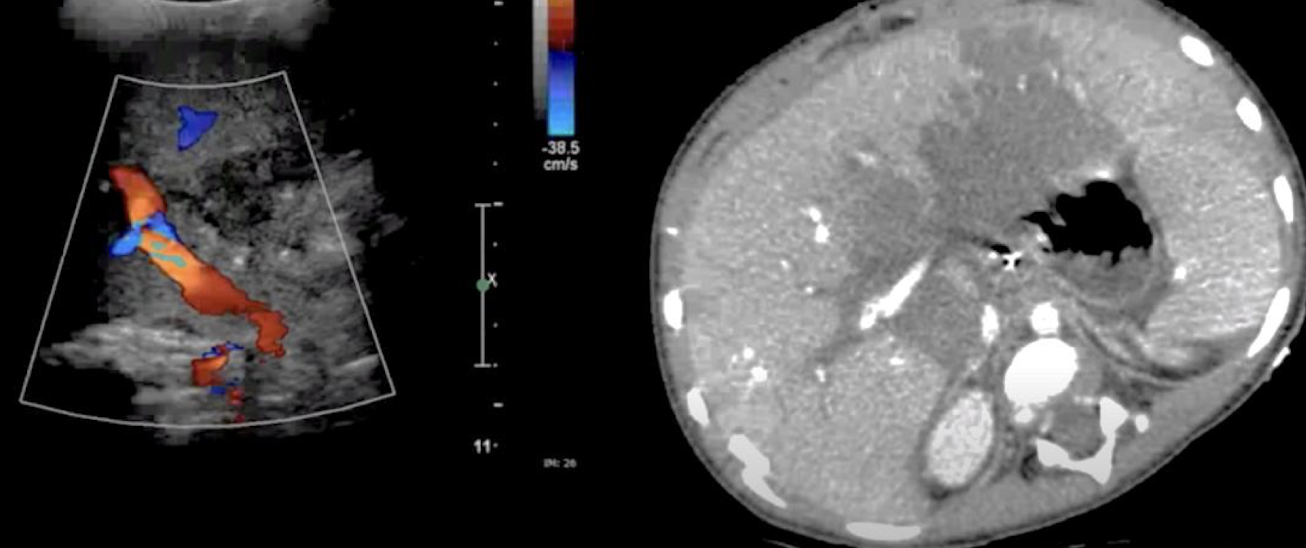
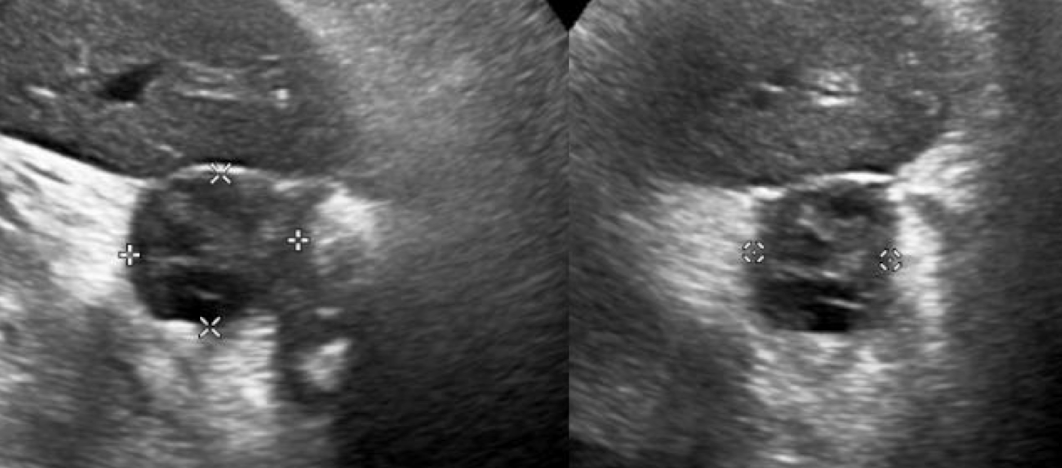
what is this showing?
posttransplant lymphoproliferative disorder (PTLD)
hypoechoic area on CT
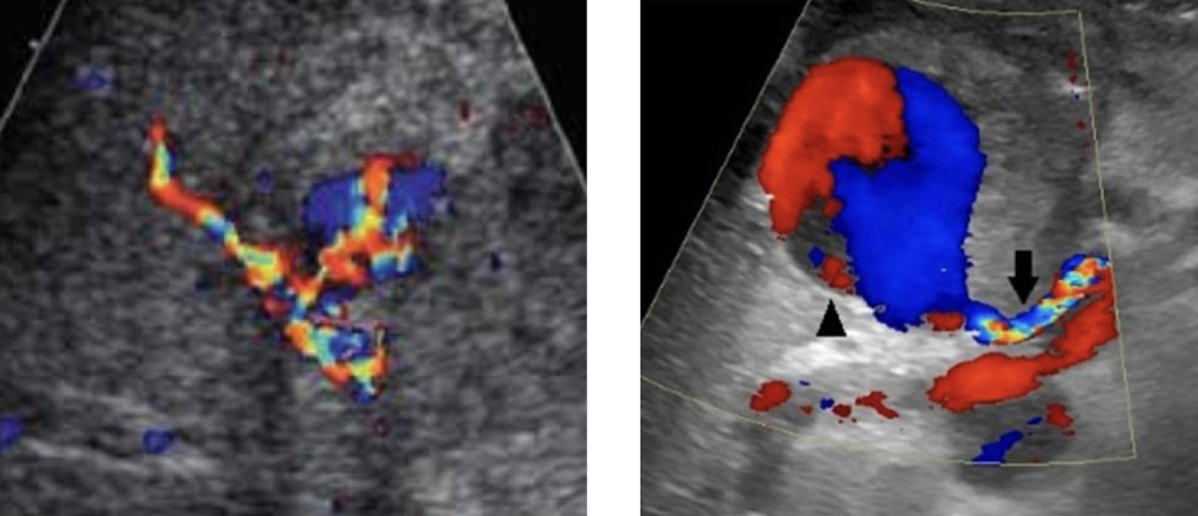
what do you see?
AV fistula
may be from biopsy
aliasing—arterial and venous waveform shown
difficult to distinguish
mosaic waveform
velocity >200 cm/s
what do you see?
tardus parvus arterial and venous waveform
Doppler all around
cine
AV fistula
normal vs abnormal HA RI waveform?
normal: 0.5-0.70
brisk upstroke
slow end diastolic component
abnormal: >0.80
PV RI waveform
continuous forward flow
minimal respiratory alterations

HV RI waveform
to-fro flow
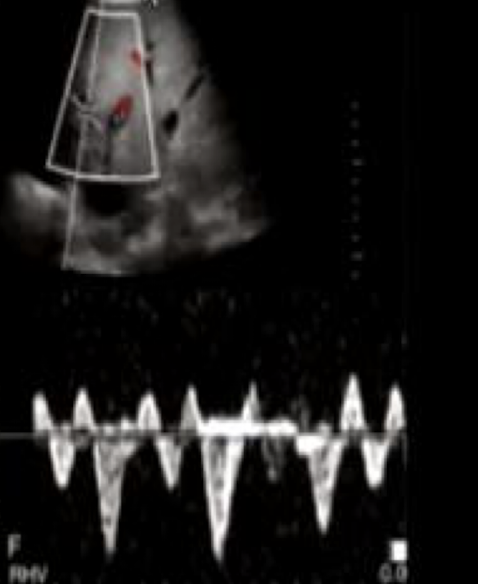
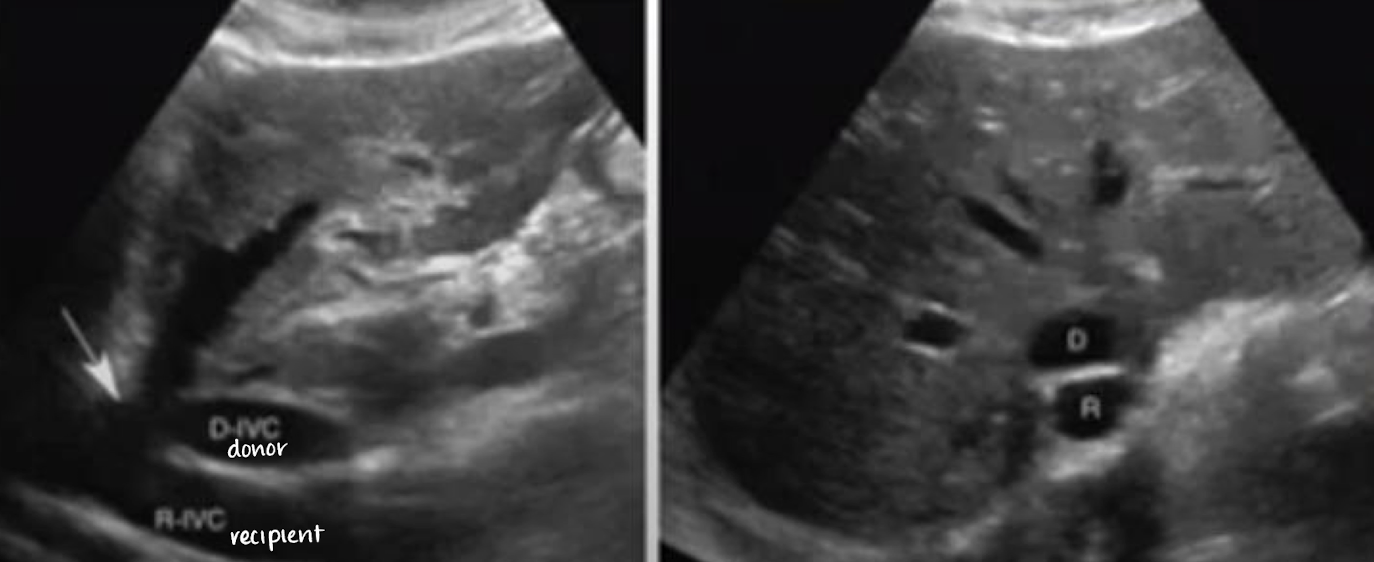
would this be from a living or deceased donor?
deceased donor
**write “IVC to IVC anast”
liver can be preserved for how many hours on ice?
8-12 hours
what is the “mercedes” sign?
scar left from liver transplant
from bilateral subcostal skin incisions that extend to the midline up to xiphoid process