12B - Blood Therapy
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
Group Testing & Cross Match
Group
Test RBC for antigens (A, B, and Rh) on membranes
Screen
Screen serum for irregular blood antibodies
Cross matching
Check donor’s RBCs and recipient’s serum compatibility
Full cross match can take up to 1.5 hours
Quick match (less sensitive) can be done in 15 – 20 min
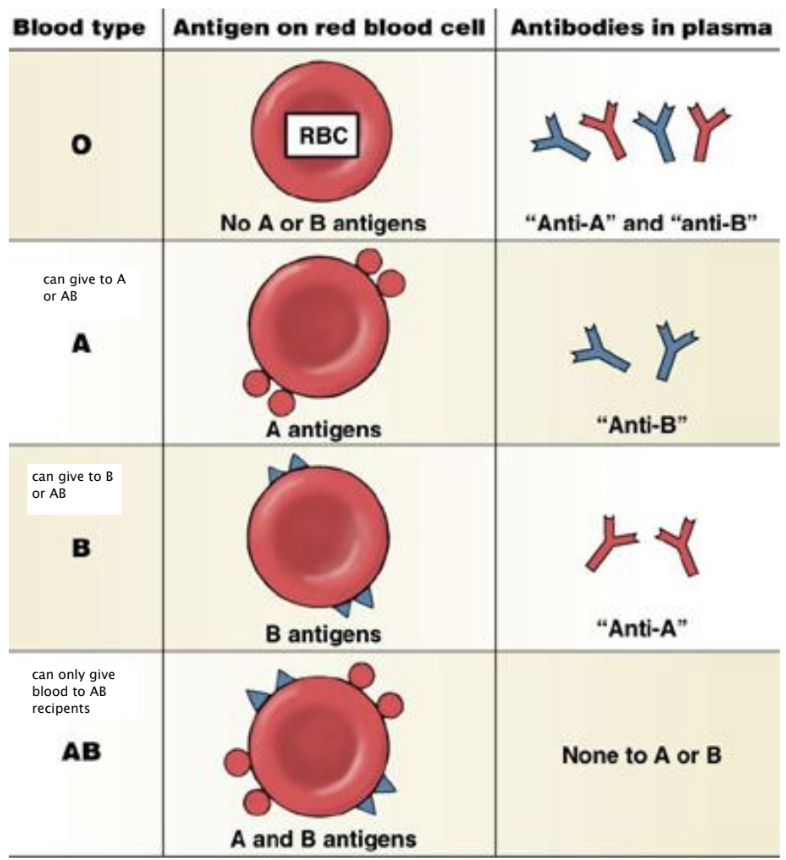
ABO Blood Group
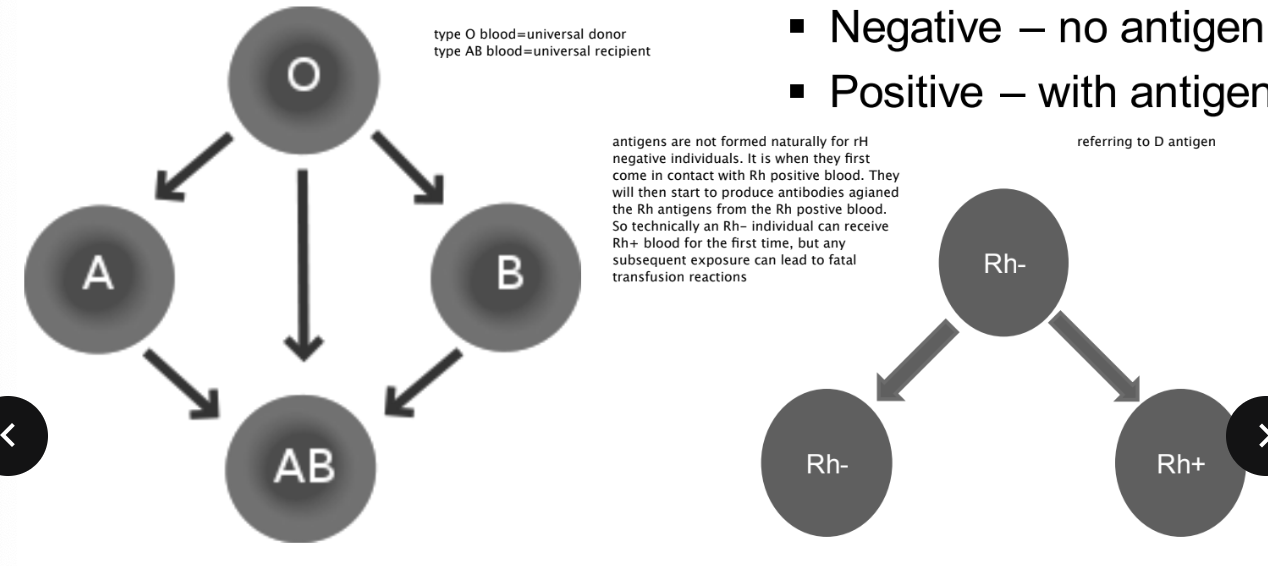
Blod transfusion Compatibility
ABO Blood Group
Rh Blood Group
Negative - no antigen
Positive - with antigen
Blood products
WBC → RBC, Platelets, plasma
Bloof transfusion Equipment
16 – 18 gauge IV (adults)
Y-type blood tubing set with filter (170-260 micron)
flush with Normal Saline
NEVER flush with RL cause it can cause clots
Blood and Fluid warmer
prevent hypothermia
Indication in OR for transfusion
replace blood loss
Maintain adequate oxygen-carrying capacity
Correct coagulation deficits
Replace Blood Loss
Patient can tolerate up to a 30% loss of blood volume if it is replaced with crystalloids or colloids
The difference is what compounds are used to bring the fluid up to the appropriate blood osmotic values
Crystalloids use salt and/or solutions
Colloids use large amount (albumin)
Transfusion of whole blood is rarely used
Packed Red Blood Cells (PRBC) with normal saline is often used as a replacement for whole blood
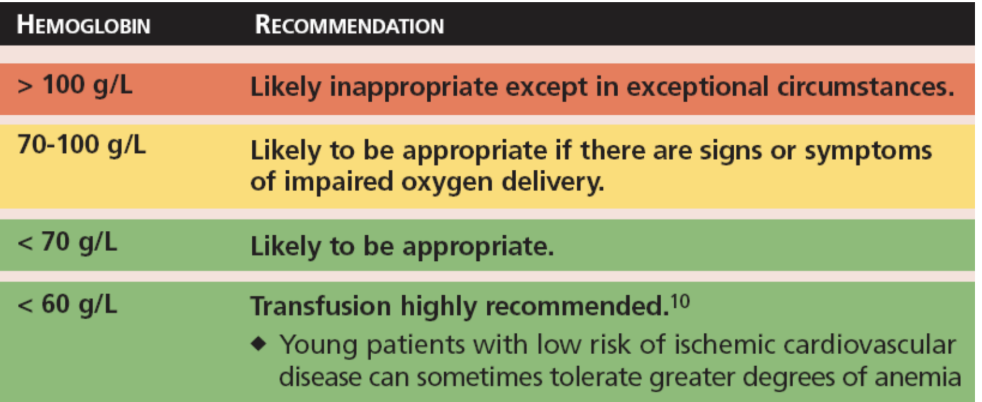
Maintain Adequate Oxygen -Carrying Capacity
monitor oxygenation
monitor hemoglobin value
What to give to Correct Coagulation Deficits
Fresh Frozen Plasma (FFP)
Platelets
Fresh Frozen Plasma (FFP)
Contain all coagulation factors except platelets
Emergent reversal of anti-coagulation therapy such as Coumadin/Warfarin
Platelets
Can be given separately to treat hypocoagulation problems
Thrombocytopenia, impaired platelet function
Risk/ Complications
Transmission of infectious diseases (ex. Hepatitis, HIV, West Nile Virus)
Transfusion-Related Acute Lung Injury (TRALI)
Characterized by noncardiogenic pulmonary edema
Transfusion-Associated Circulatory Overload (TACO)
Hypothermia (core temperature < 35 oC)
Metabolic abnormalities
Transfusion Reactions
Febrile reactions
Allergic reactions
Hemolytic reactions
Febrile Reactions
Fever rarely increases above 38oC
Possible mechanism is a reaction to:
Lysed red blood cells
Donor white blood cells or cytokines
Treatment
slow down infusion rate
Antipyretics
Allergic reactions
hives (Uticaria)
anaphylaxis
Treatment for Hives
antihistamines via IV
Anaphylaxis signs
Hives, dyspnea, hypotension, wheezing, laryngeal and
pulmonary edema, shock
Require immediate treatment for anaphylaxis
Stop transfusion!!!
Epinephrine
Bronchodilators
Antihistamines
Steroids
Circulatory support
Hemolytic reaction
Most serious and life-threatening complication
Result of ABO- and/or Rh-incompatibility
signs of hemolytics reaction
Fever and chills
Chest or back pain
Hypotension and tachycardia
Nausea and vomiting
Skin flushing
Dyspnea
Renal failure
Diffuse bleeding due to Disseminated Intravascular
Coagulation (DIC)
Tx for hemolytic reactions
Stop transfusion!!!
Manage hypotension with fluids, inotropes
Maintain urine output with crystalloids, diuretics
Increase FiO2
Reaction can be delayed if patient has been
sensitized to RBC antigens from previous
transfusion
Autologous Blood Transfusion
Patient can predonate blood prior to a scheduled
procedure for possible transfusion during
perioperative period
Intraoperative blood salvage
AKA: Cell saver
Autologous transfusion can occur during the surgical procedure if blood loss is collected and processed for re-infusion.