Neuro Exam 3 - Old Material
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
define neuroanatomical diagnosis
neurolocalization of a specific lesions rather than medical diagnosis of overall disease
discuss central and peripheral lesions
central - involve the brain and/or spinal cord
peripheral - elsewhere
discuss focal, multifocal, and diffuse lesions
focal - lesion affects one area; that is, all clinical signs can be explained by a single, localized lesion; ex. IVDD
multifocal - affect 2+ areas that are not anatomically adjacent; ex. HBC with brain trauma and peripheral nerve damage
diffuse - affect a large continuous area; ex. toxin ingestion may result in diffuse nervous system involvement (tremors, seizures, mentation changes, dyspnea, etc.)
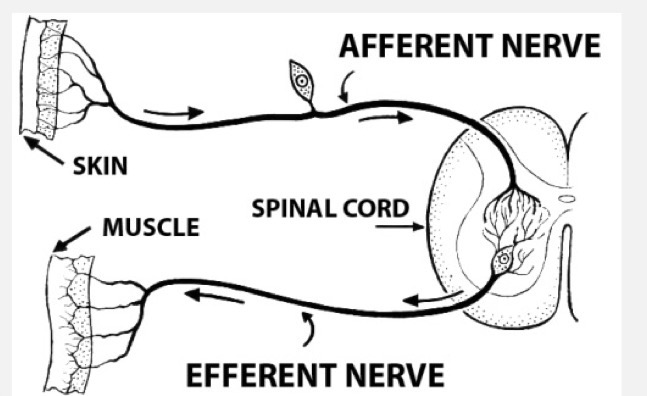
recognize that lesions of the nervous system interrupt pathways; demonstrate understanding of this concept
interruption of a pathway will result in loss of motor or sensory function below that point
CNS vs. PNS vs. ANS
CNS - central nervous system - those parts that are housed within the axial skeleton (brain and spinal cord)]
PNS - peripheral nervous system - spinal nerves and cranial nerves, (nerves from anatomy)
ANS - autonomic nervous system - includes both CNS and PNS structures; can be subdivided into sympathetic and parasympathetic
motor vs. sensory
motor / efferent - impulses carried from the CNS to the periphery
sensory / afferent - impulses carried from the periphery to the CNS
somatic vs. visceral
somatic - impulses carried to or from the skeletal muscle, skin, bones
somatosensory - sensation of pain, temperature, touch, proprioception
somatomotor - motor to skeletal muscle
visceral - impulses carried to and from smooth muscle, cardiac m., glands
viscerosensory - visceral pain (organ distension, traction, ischemia) and monitoring of homeostasis (blood pressure, pH, pO2, pCO2)
visceromotor - autonomic responses
neurons vs. neuroglia
neurons - possess membranes that can generate electrical impulses and transfer impulses to adjacent nerve cells, somatic structures, and visceral structures at synapses
neuroglia - neural support cells, which account for 90% of the total number of nervous system cells
discuss mentation / sensorium
a descriptor of level of consciousness and reaction to external stimuli
the client’s observations are very important here; they have a better understanding of their animal’s normal behavior and are more likely to notice subtle changes
additionally, patients often behave quite differently at the clinic than they do at home
possible mental states: BAR, QAR, depressed, obtunded, stupor, coma, demented
understand the continuum of mentation
BAR / QAR →
depressed / lethargic / sedate →
obtunded →
stupor →
coma
BAR / QAR
bright alert responsive
quiet alert responsive
depressed / lethargic / sedate
less active than normal
normal response to stimuli
obtunded
decreased responses to stimuli
stupor
only responsive to deep pain stimuli
coma
no response to any stimuli
demented / disoriented / delirium
unusual responses to stimuli, restlessness, apparent confusion
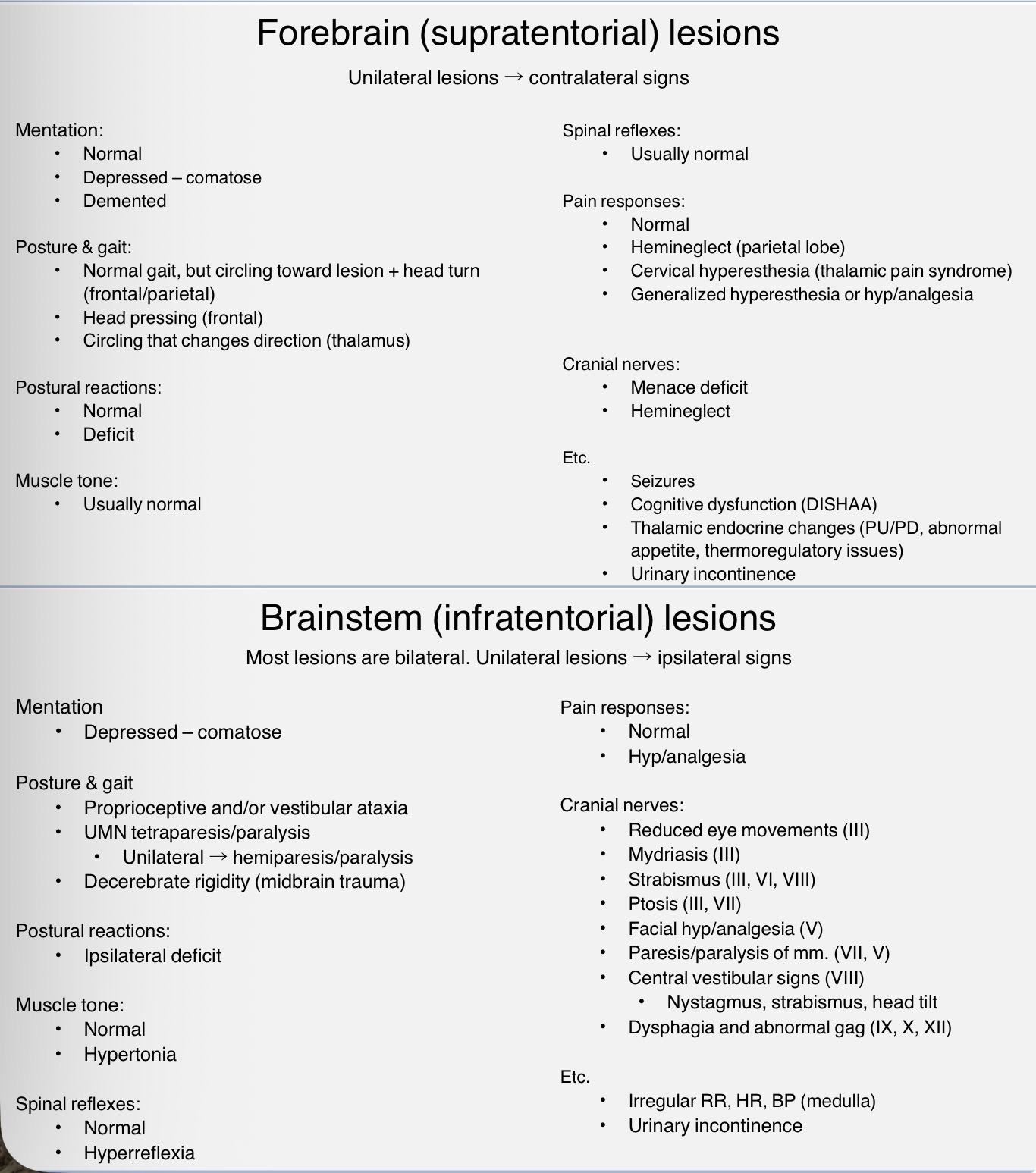
list lesions that can affect mentation
forebrain
cerebrum (particularly frontal / parietal lobes or the limbic system
thalamus
brainstem (specifically the reticular formation
list lesions that do not affect mentation
spinal cord
neuromuscular disease
cerebellum (with no additional cerebral involvement)
discuss why decreased mentation doesn’t always mean neuro disease
it is important to note that a patient may have decreased mentation because they don’t feel well; for instance, a patient with a high fever will be lethargic
additionally, a recumbent animal does not necessarily have altered mentation; for instance, a patient with a cervical spinal cord lesion can be recumbent with normal mentation
discuss signs of damage for frontal lobe
adversive syndrome
wide, propulsive circles toward lesion
head deviated toward lesion (head is turned, not tilted)
usually no ataxia, paresis, or paralysis
normal → obtunded, or demented
personality changes (often aggression)
compulsive activity
delays in onset of movement
lack of conscious perception of touch and pain
head pressing
discuss signs of damage for parietal lobe
adversive syndrome
wide, propulsive circles toward lesion
head deviated toward lesion (head is turned, not tilted)
usually no ataxia, paresis, or paralysis
normal → obtunded, or demented
personality changes (often aggression)
compulsive activity
delays in onset of movement
lack of conscious perception of touch and pain
hemineglect
discuss signs of damage for temporal lobe
there is a great deal of decussation in the pathway between the spiral organ and the temporal lobe
because of this, damage to one temporal lobe will not cause deafness
discuss signs of damage for occipital lobe
cortical blindness (PLR intact)
in humans, damage to the visual association cortex is documented to lead to visual hallucinations
discuss signs of damage for piriform lobe
damage to both sides results in loss of olfaction
list the brain regions which constitute the brainstem
mesencephalon (midbrain)
metencephalon (cerebellum and pons)
myelencephalon (medulla oblongata)
unilateral lesion → ipsilateral signs
explain why brainstem lesions are often severe
a lesion of the midbrain or pons can stop the ascending fibers of the ARAS from reaching the thalamus, which can result in coma
a lesion of the medulla can effect the reticular formation, including the cardiovascular and respiratory centers; this is generally fatal
in cases of brainstem trauma, recovery is rare; those animals who do recover will suffer neurological deficits
discuss the ascending reticular activating system
input to the ARAS comes from all modalities (except proprioception) and from every segment of the spinal cord (via spinoreticular tract) and brainstem
special senses
touch
pain
these neurons synapse in the reticular formation; RF neurons synapse on the thalamic nuclei; from here, there are projections to all parts of the cortex
ARAS: sensory neurons → RF → thalamus → internal capsule → cortex
functions of reticular system:
regulation of consciousness and alertness
sensory modification
regulation of muscle tone
contains central pattern generators for voluntary and involuntary actions
regulation of ANS
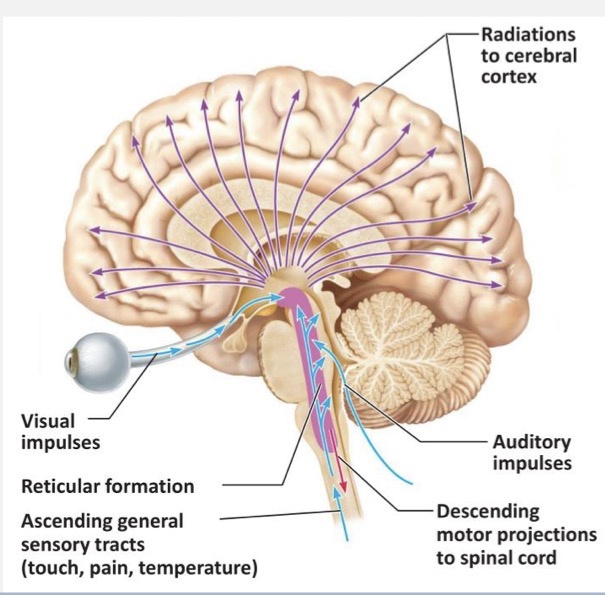
summarize the function of the ascending reticular activating system in relation to regulation of consciousness and alertness
sensory inputs travel cranial to the reticular formation, then thalamus, and then activate areas of the cerebral cortex
ex:
your dog is sleeping peacefully, you open a bag of treats, suddenly your dog is awake
auditory stimuli goes not only to auditory cortex, but to the reticular formation
the ARAS activates the entire cortex, thus allowing your dog to be awake and alert
without a reticular formation, the cortex doesn’t respond to sensory inputs
localize a brain lesion when given a list of clinical signs
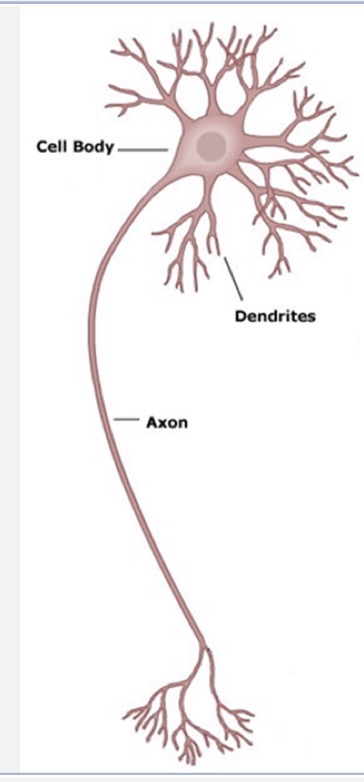
soma
cell body
contains organelles and cytoplasm
receives signals from adjacent axons
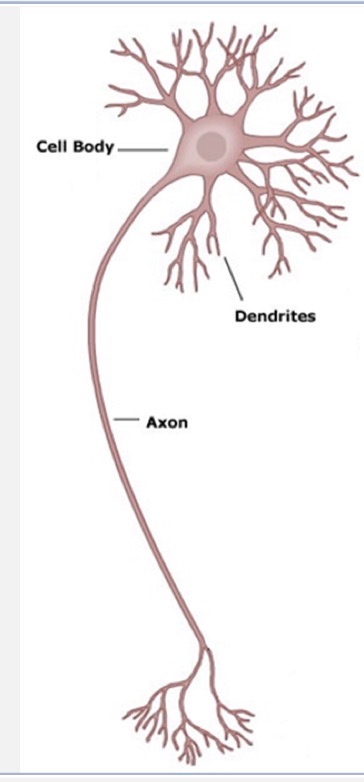
axon
sends and receives signals
each neuron has a single axon which can have many branches
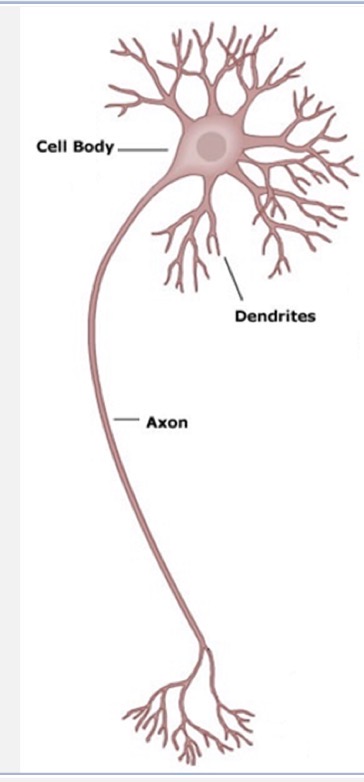
dendrite
receive signals
remainder of the neuronal processes
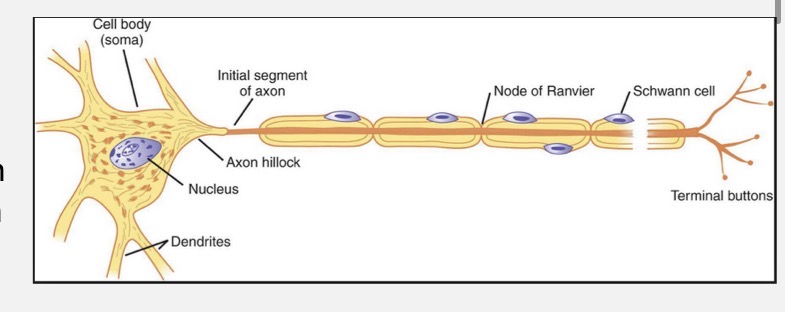
myelin sheath node / node of ranvier
gaps between myelinated segments
nuclei
collection of nerve cell bodies in the CNS
ganglia
collection of nerve cell bodies in the PNS
tract
bundle of nerve fibers in the CNS
nerve
bundle of nerve fibers in the PNS
list the types of traumatic peripheral nerve injury
compression - most severe is crushing
traction - most severe is avulsion
laceration - most severe is complete transection
ischemia - most severe is total loss of blood flow
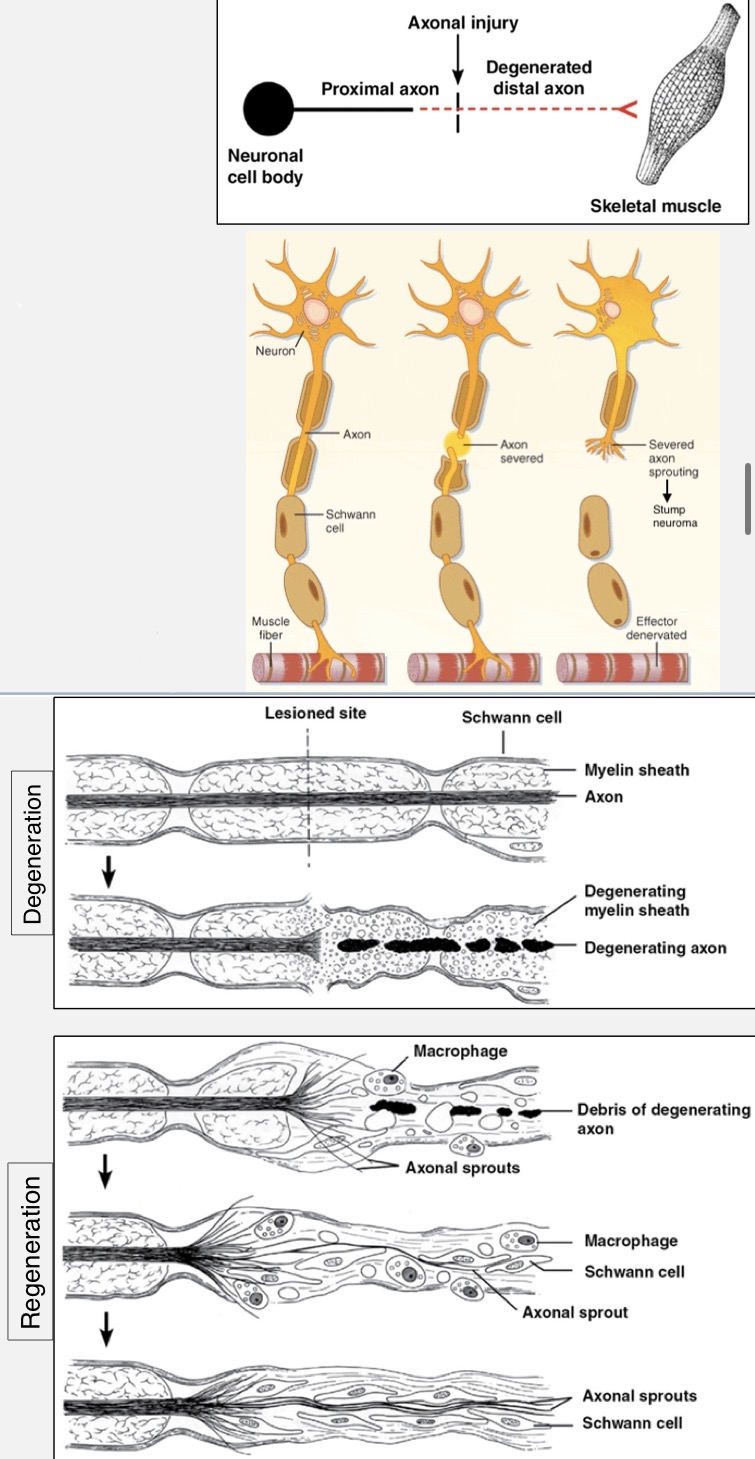
explain what occurs upon axonal and general neuronal injury in the PNS
when an axon is completely severed, we refer to the portion with the cell body as the proximal segment and the isolated portion as the distal segment
proximal segment undergoes some degeneration, then it may:
regenerate (1-5 mm/day) to original or different synapse site
lead to neuronal death
become the site of neuroma formation
distal segment undergoes Wallerian degeneration (total degeneration) because protein synthesis occurs at the soma
myelin requires contact by axon to remain intact, so it too degenerates
schwann cells may remain intact or degenerate over time
damaged neurons can regenerate back to their original site if the cell body survives and the regenerating axon can make contact with distal schwann cells (which secrete chemotropic factors)
factors that decrease likelihood of functional nerve regrowth:
damage near the soma
severe and/or crushing injury
misalignment of segments
scar tissue formation
old age of patient
CNS vs. PNS axonal injury
PNS axons are more likely to heal than CNS because:
in CNS, the entire neuron is likely to die with axonal damage
more efficient phagocytosis and debris removal in PNS
schwann cells are better equipped to re-myelinate than oligodendrocytes
PNS axons have endoneurium which guides the proximal segment toward the distal segment
explain what occurs upon axonal and general neuronal injury in the CNS
location of injury is important:
superficial - fibroblasts in meninges synthesize collagen
deep - proliferation of astrocytic processes; not as effective as fibroblasts
CNS injury commonly results in degeneration and necrosis of neurons:
space-occupying lesions - hemorrhage, abscess, tumor → compressive
lesions which impede blood flow - cardiac arrest, hypovolemic shock, thrombosis → ischemic
other - infection, toxins, trauma, nutritional deficiencies
the BBB protects the CNS from initial infectious insult; however, once infected the brain lacks efficient mechanisms to combat spread and damage
axonal injury in the CNS typically results in wallerian degeneration, as well as degeneration of the entire neuron
those neurons that do survive will typically only regenerate a few millimeters, at which point synapses with adjacent neurons can occur
cases of functional recovery after CNS lesions typical involve compensatory adaptations by other neural networks, rather than a regeneration of damaged neurons
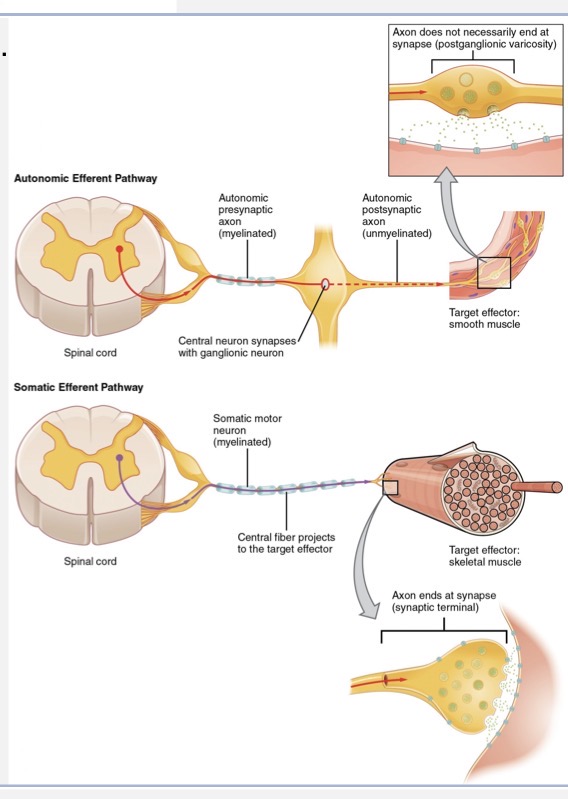
name the types of synapses (electrical, chemical) and what structures can receive a presynaptic terminal (neuron, skeletal muscle, smooth muscle, cardiac muscle, glandular cell)