Chapter 6: Anxiety Disorders
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
anxiety and fear
Anxiety = apprehension over an anticipated problem - future, moderate arousal, adaptive, helps us notice/plan for future threats
small degree of anxiety improves performance on lab tasks, but too much interferes with performance (inverse U-shaped curve)
Fear = reaction to immediate danger - now, high arousal, adaptive, fundamental for "fight-or-flight" reactions, triggers rapid changes in the sympathetic nervous system.
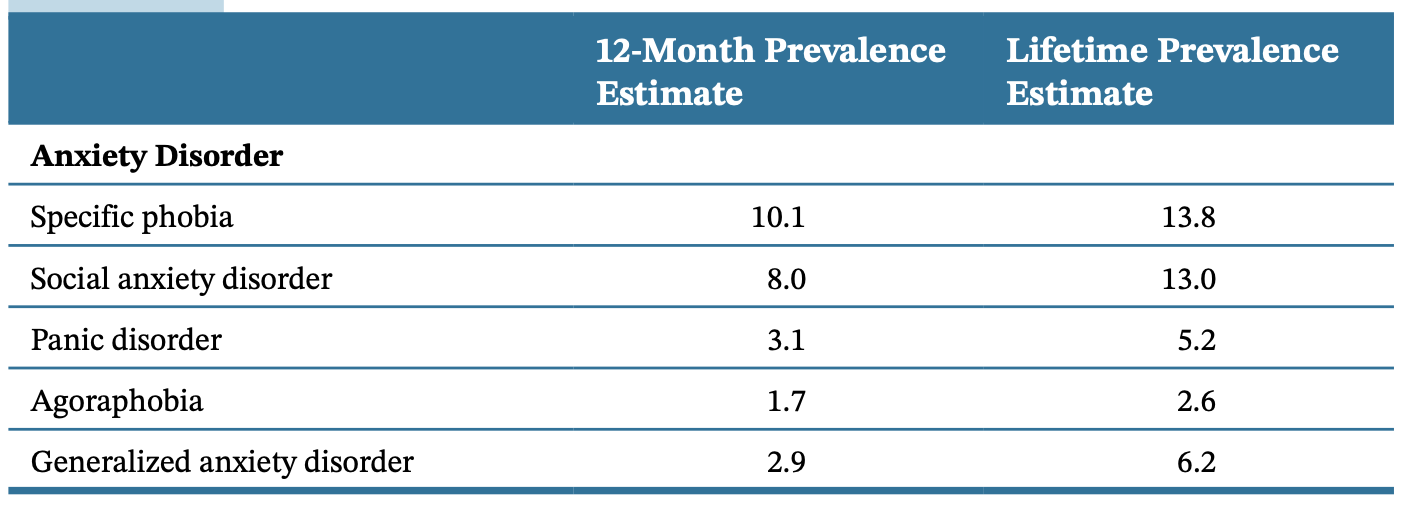
Major anxiety disorders in the DSM-5-TR
specific phobias, social anxiety disorder, panic disorder, agoraphobia, generalised anxiety disorder
Involve excessively high anxiety;
Involve tendencies to experience unusually intense fear (except GAD).
Most common type of psychological disorder: prevalence 28%.
Tend to experience chronic or intermittent symptoms;
Related to medical disability, unemployment, risk of marital discord, risk of suicide attempts, risk of developing medical conditions.
specific phobias
= consistent tendency to experience extreme fear of an object/situation (e.g. flying, snakes, heights). The person recognises the fear is excessive but still goes to great lengths to avoid the feared object/situation.
Two of the most common types are claustrophobia and acrophobia (fear of heights).
A person with a phobia for one type of object/situation is very likely to have a specific phobia for a second object/situation (highly comorbid).
Defining symptoms:
Disproportionate fear consistently triggered by specific objects/situations, typically lasting 6 months or more.
The object/situation is avoided or else provokes intense anxiety/fear.
Types of specific phobias:
Animal (snakes, insects)
Natural environment (storms, heights, water)
Blood, injection, injury: tend to run in families, heart rate slows and possible fainting when facing the fears stimuli.
Situational (public transport, tunnels, bridges, elevators, flying, driving, closed spaces)
Other (choking, contracting an illness, loud sounds, clowns)
Social anxiety disorder
= persistent, unrealistically intense fear of social situations that might involve being scrutinised by/exposed to unfamiliar people.
Deeply concerned that they will do/say something embarrassing and be judged harshly
Intense feelings of shame/humiliation (more chronic than for shy people)
Leads most to avoid social situations.
Most common fears: public speaking, speaking in group settings, meeting new people, talking to people with authority.
May spend days in advance thinking about what can go wrong, then days after feeling ashamed about any small moments that did go badly.
Can range in severity from a few specific fears to a generalised host of fears (the latter are more likely to experience comorbid depression and alcohol use).
At least a third also meet the criteria for avoidant personality disorder (symptoms and genetic vulnerability overlap, but the latter is more severe and pervasive).
Defining symptoms:
Marked and disproportionate fear consistently triggered by exposure to potential social scrutiny.
Exposure to the trigger leads to intense anxiety about being evaluated negatively.
Trigger situations are avoided or else endured with intense anxiety.
Symptoms typically last 6 months or more.
Panic disorder
= recurrent panic attacks that are unrelated to specific situations, and worry about having more panic attacks.
Panic attack = sudden experience of intense apprehension, terror, feelings of impending doom, accompanied by at least four other symptoms:
Physical symptoms: shortness of breath, heart palpitations, nausea, upset stomach, chest pain, feelings of choking and smothering, dizziness, lightheadedness, faintness, sweating, chills, heat sensations, numbness or tingling sensations, trembling.
Depersonalisation (feeling of being outside one's body).
Derealisation (feeling of the world not being real).
Fears of losing control, going crazy, dying.
*People feel an intense urge to flee whatever situation they are in when a panic attack occurs, some people think they are having a heart attack.
*The symptoms tend to come on very rapidly and reach a peak of intensity within 10 minutes.
A panic attack is a misfire of the fear system: sympathetic nervous system arousal at the same level as people facing an immediate threat to life.
Symptoms are inexplicable, so person tries to make sense of them: thinking they are dying, losing control, going crazy -> likely to feel more fear. (90% report these kinds of beliefs)
Defining symptoms:
Recurrent unexpected panic attacks.
At least 1 month of concern about the possibility that more attacks could occur or the possible consequences of an attack, or problematic behavioural changes to avoid attacks or their consequences.
Agoraphobia
= anxiety about situations from which it would be embarrassing or difficult to escape if anxiety symptoms occurred (crowds, crowded places, also trains, bridges, long road trips).
Due to these fears, many are unable to leave their house, or do so with great distress.
Defining symptoms:
Disproportionate and marked fear or anxiety about at least two situations where it would be difficult to escape or receive help in the event of incapacitation, embarrassing symptoms, or panic-like symptoms (being outside the home alone; traveling on public transportation; being in open spaces such as parking lots, bridges, and marketplaces; being in enclosed spaces such as shops, theatres, or cinemas; or standing in line or being in a crowd).
These situations consistently provoke fear or anxiety.
These situations are avoided, require the presence of a companion, or are endured with intense fear/anxiety.
Symptoms typically last 6 months or more.
Generalised anxiety disorder (GAD)
= persistent worry, often about minor things.
Worry = cognitive tendency to chew on a problem and to be unable to let go of it.
Worries of people with GAD are excessive, uncontrollable and long-lasting.
Their worries center on the same threats that worry everyone (relationships, health, finances, daily hassles), but they worry more about these issues.
Worry is accompanied by arousal-related symptoms.
GAD has a major impact on relationships: more likely to report marital distress and an absence of friendships than any other anxiety disorder.
Defining symptoms:
Excessive anxiety and worry about multiple events or activities.
The person finds it hard to control the worry.
The anxiety and worry are associated with at least three (or one in children) of the following:
Restlessness or feeling keyed up/on edge.
Tiring easily.
Difficulty concentrating/mind going blank.
Irritability.
Muscle tension.
Sleep disturbance.
Symptoms are present at least 50% of days for at least 6 months.
Comorbidity of anxiety disorders
More than half of people with one anxiety disorder meet the criteria for another anxiety disorder during their lives.
Also highly comorbid with other disorders: 3/4 of people with an anxiety disorder meet the criteria for at least one other psychological disorder.
60% of people in treatment for anxiety disorder meet the diagnostic criteria for major depression in their lifetime.
OCD also commonly co-occurs with anxiety disorders.
Comorbidity is associated with greater severity and poorer outcomes of anxiety disorders.
Gender differences in anxiety disorders
Women are almost twice as likely to experience anxiety disorders.
Anxiety disorders are related to more functional impairment for women.
Explanations:
Women may be more likely to report symptoms.
Social influences, gender norms: men face more social pressure to face their fears (basis for treatment).
Women experience different life circumstances: more likely to be SAd, may interfere with developing a sense of control over one's environment (having less perceived control over one's environment is a risk factor); men may be raised to believe more in their personal control over situations.
Women show higher neuroticism levels and more biological reactivity to stress (perhaps due to social/psychological influences).
Cultural influences on anxiety disorders
Culture and environment influence what people fear.
Cultural concepts of distress may shape the expression of an anxiety disorder:
In Japan, taijin kyofusho involves fear of displeasing or embarrassing others, fear of making direct eye contact, blushing, having body odour, or having a bodily deformity. Symptoms overlap with social anxiety disorder, but the focus on others' feelings is distinct.
Dhat syndrome in South Asia, involves anxiety or distress attributed to the loss of semen.
Susto in Latin America, involves the belief that a severe fright has caused the soul to leave the body.
The objects of anxiety/fear in these syndromes relate to environmental challenges or to attitudes that are prevalent in those cultures.
Prevalence of anxiety varies dramatically across cultures, ranging from 3-19%.
Cultures differ in variables like stress levels, the nature of family relationships, the presence of war, and the prevalence of poverty:
Countries with recent war or conflict have higher rates of anxiety disorders.
Countries with higher rates of COVID-19 showed greater increases in prevalence of anxiety disorders.
Countries with high income inequality have much higher rates of anxiety.
Cultural attitudes change how comfortable people are in disclosing psychological symptoms.
Influences that increase general risk of anxiety disorders
Cultural and cross-national influences: exposure to war, persecution, income inequality.
Behavioural conditioning (classical and operant conditioning)
Genetic vulnerability
Disturbances in neural activity: amygdala, mPFC, brain regions involved in processing fear and emotion.
Decreased functioning of GABA (gamma-aminobutyric acid) and serotonin; increased norepinephrine activity.
Behavioural inhibition
Neuroticism
Cognitive influences: sustained negative beliefs, perceived lack of control, overattention to cues of threat, intolerance of uncertainty
Fear conditioning
The behavioural theory of anxiety focuses on conditioning.
Mowrer's two-factor model of anxiety disorders suggests two steps in the development of an anxiety disorder:
Classical conditioning: a person learns to fear a neutral stimulus that is paired with an intrinsically aversive stimulus.
Operant conditioning: A person gains relief by avoiding the CS, avoidant response is reinforced and maintained.
Does not fit the evidence very well: many people cannot remember any threatening event that triggered their symptoms, and many who do experience serious threats don't develop anxiety disorders.
Extension to the model explains why some people don't remember any conditioning experience: classical conditioning could occur in different ways (direct experience, modelling, verbal instruction).
Also, some people are more vulnerable to developing anxiety disorders: people with anxiety disorders are more responsive to threats, are slower to extinguish fears once conditioned (also present in offspring).
Research suggests that people with anxiety disorders are particularly sensitive to unpredictable, diffuse or remote threats: neutral predictable unpredictable (NPU) threat task - anxiety disorders are specifically related to increased affective and psychophysiological response to the unpredictable threat condition vs predictable (specific to anxiety disorders, doesn't happen with MDD)
Genetic vulnerability
Heritability of 0.5-0.6 for anxiety disorders
Genetic vulnerability to phobia increases risk for other anxiety disorders
Genetic vulnerability to anxiety disorders (especially GAD) overlaps with MDD
Genetic vulnerability is tied to higher neuroticism (predictor for depressive/anxiety disorders)
Neurobiological correlates
Labelled the fear circuit (bad, also activated during other types of processing, also mood disorders).
Amygdala: assigns emotional significance to stimuli; people with anxiety disorders show greater amygdala activity to angry faces.
mPFC: regulates amygdala activity, extinguishes fear, conscious processing of anxiety/fear, regulates emotions; people with anxiety disorders show less activity in mPFC to threatening stimuli/during extinction of conditioned fear responses.
Connectivity between mPFC and amygdala: pathway inhibiting activity of the amygdala, weaker in people with anxiety disorders.
Bed nucleus of the stria terminalis (extended part of amygdala): cues of threat
Anterior cingulate cortex: allocation of attention, anticipation of threat
Insula: awareness, processing of bodily cues (high arousal involved in threat)
Both higher activity to threat stimulus in anxiety disorders.
Hippocampus: encoding the context in which feared stimuli occur.
Locus coeruleus
Neurotransmitters:
Anxiety disorders linked to disruptions in serotonin levels (modulates emotions and responses to threat).
Changes in the function of the GABA system (modulates amygdala activity and other regions involved in processing threat).
Anxiety disorders related to increased levels of norepinephrine (activates sympathetic nervous system), changes in sensitivity of norepinephrine receptors