PHR 948 - Block 2: COPD
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
COPD
chronic obstructive pulmonary disease
- obstructive disorder
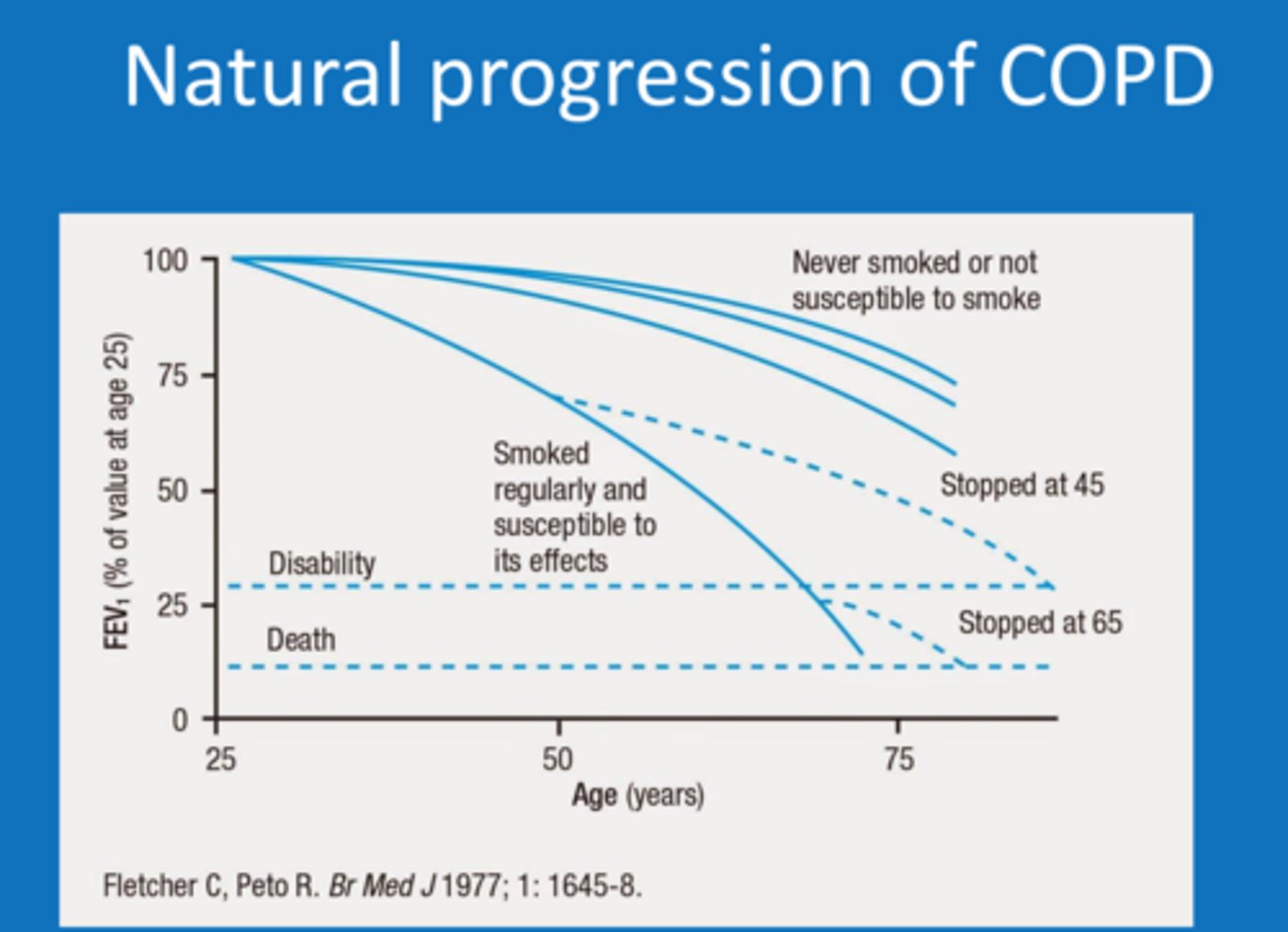
- chronic, progressive, & incurable disorder causing severe breathing difficulties
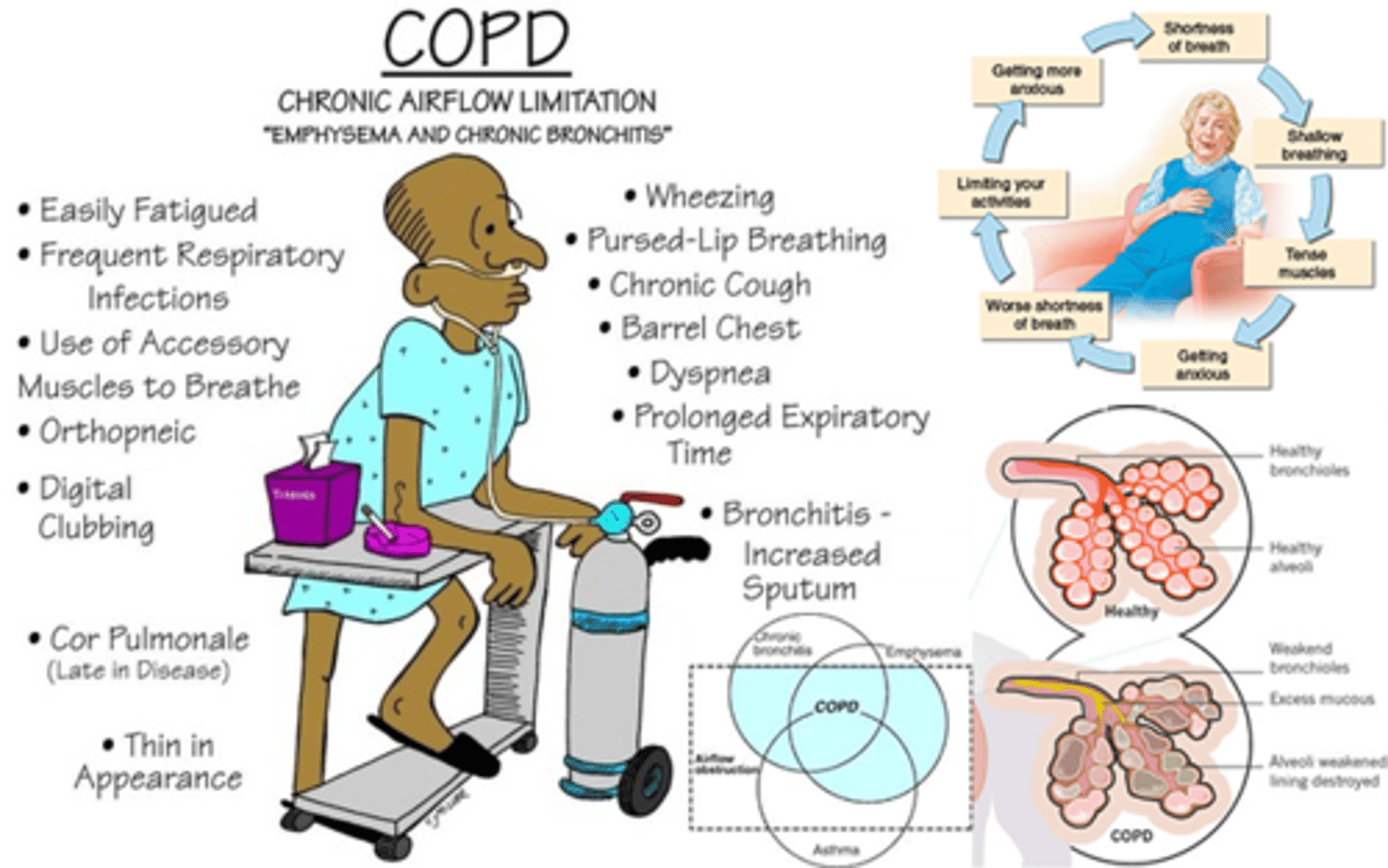
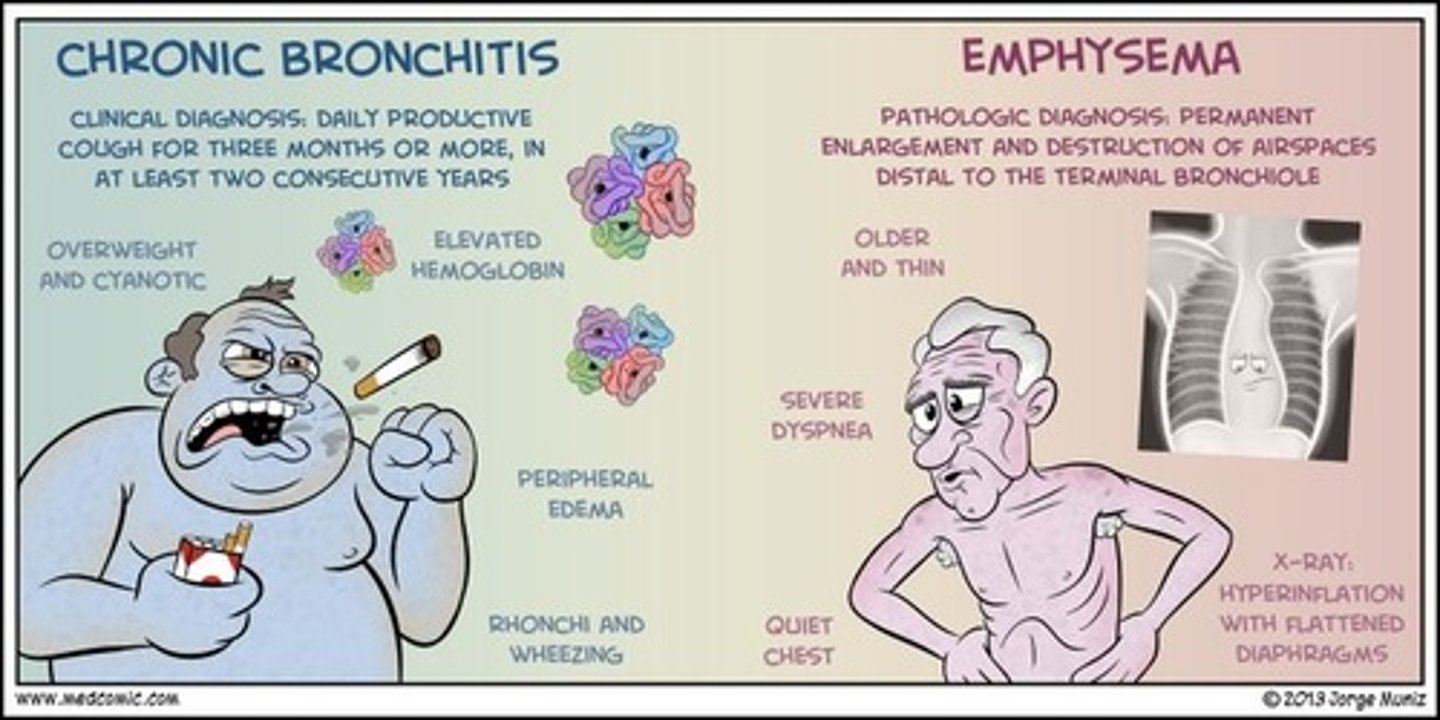
2 pathophysiologies of COPD
1. small airway disease
- chronic bronchitis
- airway inflammation, airway fibrosis, luminal plugs, increased airway resistance
2. parenchymal destruction
- emphysema
- loss of elasticity at alveoli, leading to air trapping
COPD exacerbations
sudden worsening in respiratory symptoms
- increased dyspnea, coughing, wheezing, changes in mucus productions, fatigue
- usually occurs after exposure to triggers or respiratory viruses
- requires additional treatment beyond the normal maintenance medications to improve
- lung functions typically worsens for good after a relapse
global initiative for chronic obstructive lung disease (GOLD)
annual guidelines for COPD
diagnosing and classifying COPD
diagnosing
- look at clinical presentation, symptoms, history, risk factors
- rule out other causes
- spirometry
classifying
- use symptom rating score
- exacerbation/ illness history
- spirometry
- GOLD grade and GOLD ABE group
COPD symptoms
- dyspnea
- chronic cough
- may or may not have mucus production
- recurrent wheeze
COPD risk factors
- tobacco smoking, current or history
- household and outdoor pollution/ occupational exposures
- genetics (alpha-1 antitrypsin deficiency)
- abnormal lung development
- low birth weight/ prematurity
- childhood respiratory infections
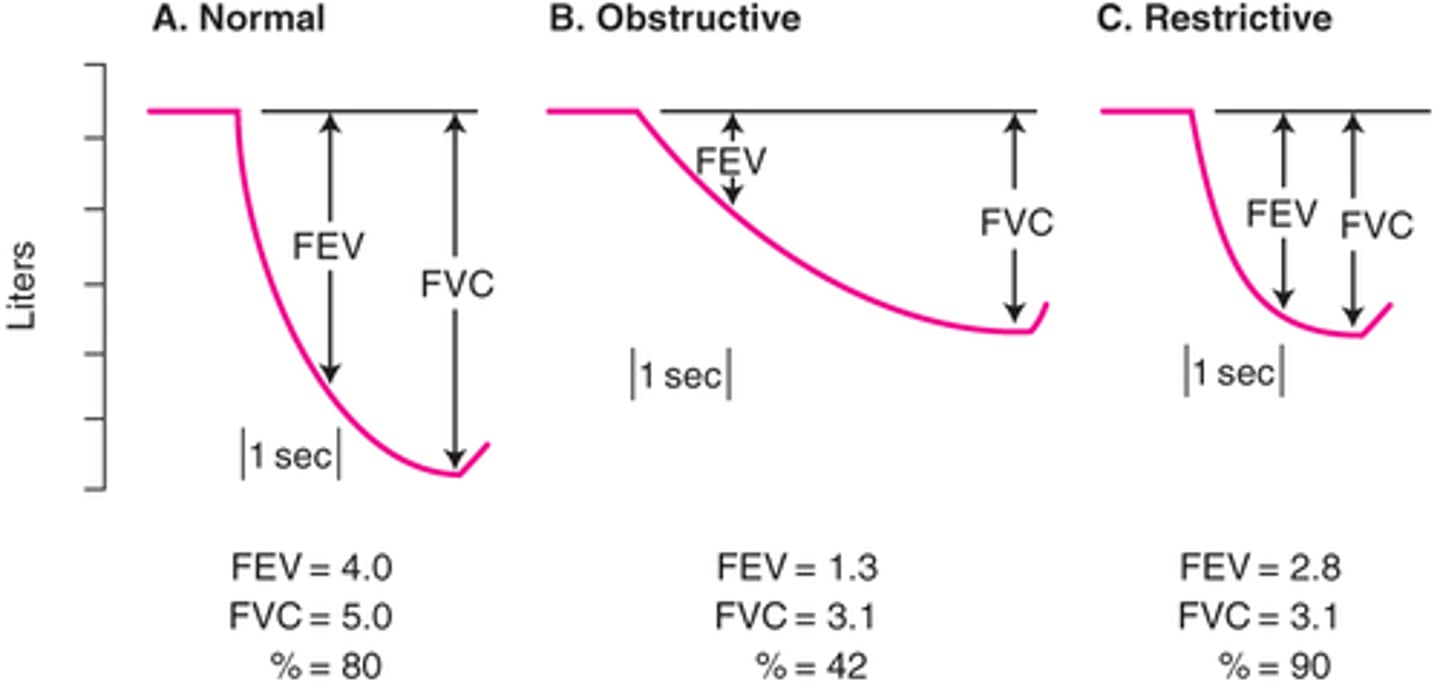
spirometry
(pulmonary function tests)
- should be performed AFTER administering a short acting bronchodilator (albuterol)
- look at FEV1/FVC ratio
> if less than 0.7 = COPD diagnosis
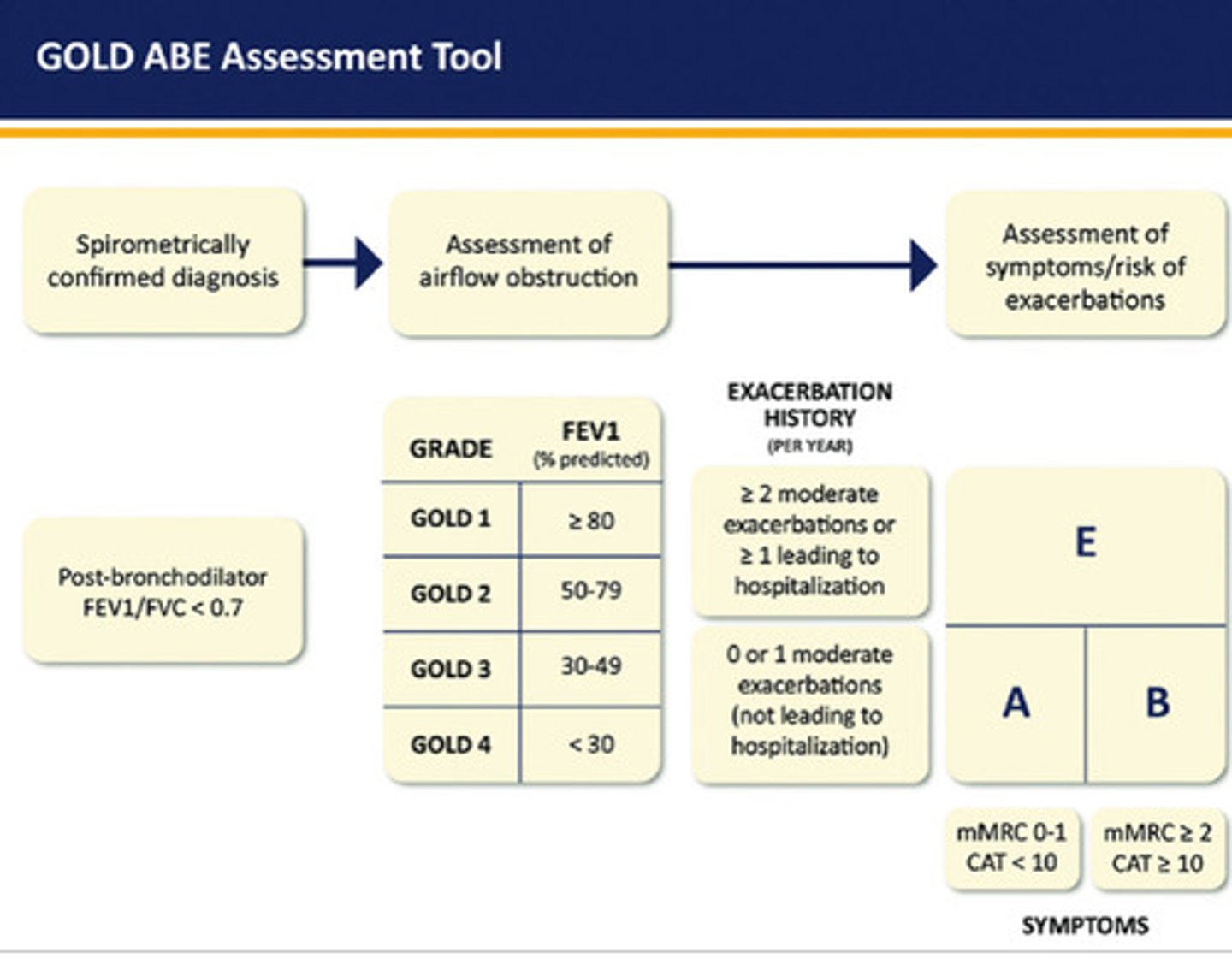
GOLD classification of COPD
GOLD grade
- GOLD 1 (mild): FEV1 ≥ 80% of predicted
- GOLD 2 (moderate): 50% ≤ FEV1 < 80% of predicted
- GOLD 3 (severe): 30% ≤ FEV1 < 50% of predicted
- GOLD 4 (very severe): FEV1 < 30% of predicted
GOLD ABE group
- A: no moderate/ severe exacerbations in the previous year
> mMRC 0-1 or CAAT <10 (use worst of the two)
- B: no moderate/ severe exacerbations in the previous year
> mMRC ≥ 2 or CAAT ≥ 10
- E: one or more moderate/ severe exacerbations in the previous year
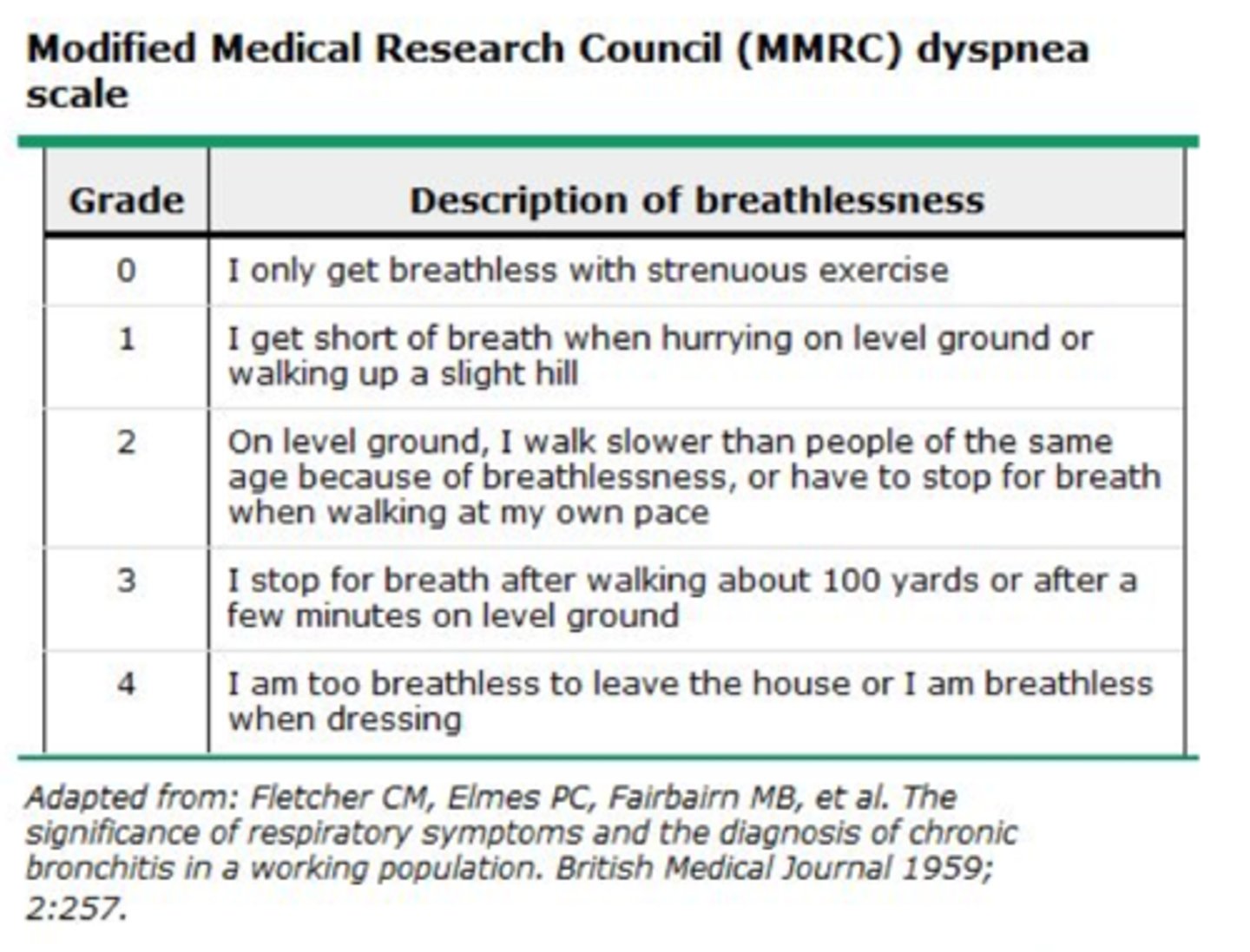
symptom rating scales
mMRC (modified medical research council dyspnea score)
CAAT (chronic airways assessment test)
- quantifies the severity of symptoms
- obtained at each visit
- used in the ABE tool to classify disease severity (for patients without exacerbation in the last year)
COPD pharmacologic therapy overview
- bronchodilators & anti-inflammatories
bronchodilators: beta 2 agonists (SABA/ LABA), muscarinic antagonists (SAMA/LAMA), or a combo of these two
anti-inflammatories: ICS, chronic macrolide, PDE inhibitors, IL-4 inhibitors
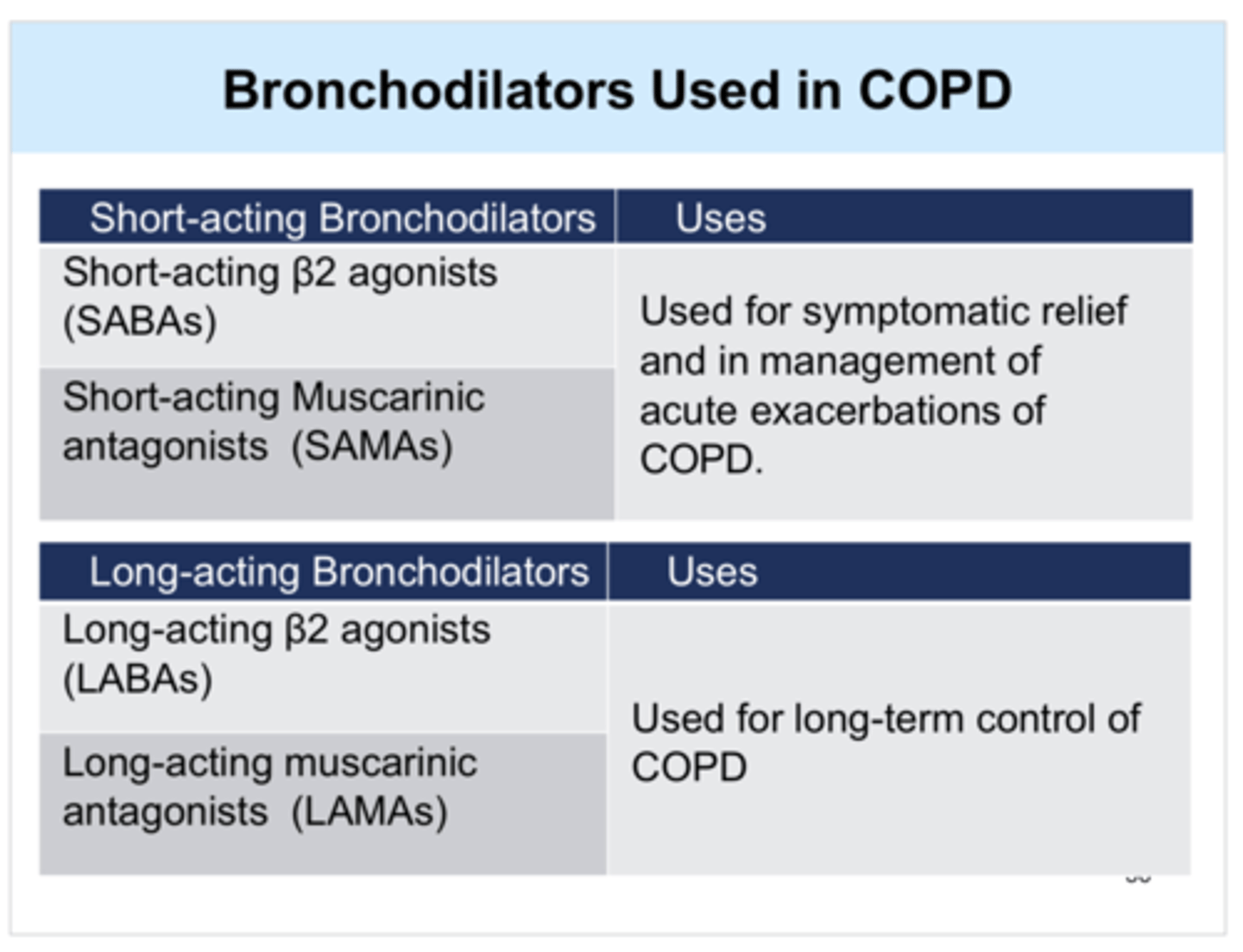
bronchodilators for COPD
beta 2 agonists and muscarinic antagonists
- 1st line treatment for most people
- improves FEV1, improves symptoms, and reduces exacerbations
- long-acting agents are preferred for chronic maintenance
> short-acting agents may be used in addition for rescue therapy
for monotherapy
- LAMA > LABA for exacerbation reduction
- LAMA = LABA for symptom reduction and FEV1 improvement
- LAMA + LABA > monotherapy for all outcomes
inhaled corticosteroids (ICS) in COPD
do NOT use alone in COPD, it increases mortality
- can decrease exacerbations, but no impact on dyspnea
- increases the risk of pneumonia, especially in severe disease
- if patient has blood eosinophils < 100 cells/mcL, little to no benefit from ICS is expected
- if a patient has co-occuring asthma, ALWAYS use an ICS in treatment regimen
ICS place in therapy
use strongly favored if:
- history of hospitalization(s) for exacerbations
- 2+ moderate exacerbations of COPD per year
- blood eosinophils 300+
- history of or concomitant asthma
use favored if:
- 1 moderate exacerbation of COPD per year
- blood eosinophils 100-300
against use if:
- repeated pneumonia events
- blood eosinophils <100
- history of mycobacterial infection
ICS + LABA in COPD
not preferred in most patients
- still used commonly though bc providers are used to this
- if indicated, use triple therapy (LAMA + LABA + ICS)
> triple therapy is superior for reducing exacerbation, improving lunch function and symptoms
phosphodieserase (PDE)
- PDE-4: breaks down cyclic AMP, regulates airway epithelial cell inflammation
- PDE-3: breaks down cyclic AMP and GMP, regulated airway smooth muscle cells (bronchoconstriction/dilation)
- inhibitors of PDE-3/4 increase cAMP and CGMP = decreases inflammation and induce bronchodilation
PDE-4 inhibitor
roflumilast (Daliresp)
- indicated in patients with: severe-very severe COPD (FEV1 <50%), chronic bronchitis features, history of exacerbations requiring hospitalization or treatment with a steroid +/- antibiotic
- can reduce exacerbation frequency and improve lung function, but does NOT decrease symptoms
- ADE: neuropsychiatric effects (anxiety, depression, sleep disturbances), weight loss, GI effects
PDE-3/4 inhibitor
ensifentrine (Ohtuvayre)
- only approved in the US
- unclear place in therapy
- can increase FEV1
- ADE: bronchospasm, psychiatric effects, suicidality, UTI, back pain
chronic macrolide therapy
azithromycin 500 mg three times weekly chronically
- used as an anti-inflammatory, not for antimicrobial
- most beneficial in former smokers with exacerbations despite appropriate inhaled therapy
IL-4 and IL-13 inhibitor
dupilumab (Dupixent)
- SQ injection
- can reduce exacerbations and improve lung function in patients with: chronic bronchitis features, history of 2+ exacerbations per year despite triple therapy, GOLD 2-3, and blood eosinophil count of 300+
IL-5 inhibitors
mepolizumab (Nucala)
- SQ injection
- can reduce exacerbations in patients with: COPD, 2+ moderate exacerbations or 1 severe exacerbation despite triple therapy, GOLD 2-4, and blood eosinophil count of 300+
benralizumab (Fasenra)
- not recommended, no change in exacerbations
COPD non-pharm therapy
- risk factor reduction and trigger avoidance
> smoking cessation!!!!
- vaccinations
- pulmonary rehabilitation (groups B and E only)
pulmonary rehabilitation
- an education and exercise based program to increase awareness of how to exercise or perform everyday activities with pulmonary limitations
- recommended for patients in group B and E
- benefits: reduces symptoms, decreases days hospitalized, increases physical activity & exercise tolerance, improve daily life, and improve emotional health
COPD treatment initiation
- all COPD patients should have a short acting bronchodilator for rescue
> SAMA, SABA, or combo
> if on LAMA, do not give them a SAMA
use ABE to determine initial therapy
A: bronchodilator
B: LABA + LAMA
E: LABA + LAMA + consider ICS if high eosinophils (300)
COPD treatment adjustment
exacerbations:
- if on a LABA or LAMA, increase to combo therapy
- if blood eosinophils high (100-300), consider triple therapy with ICS
- if pt still has exacerbations, consider roflumilast, azithromycin, or biologic
persistent dyspnea:
- if on a LABA or LAMA, increase to combo therapy
- if pt still has dyspnea, consider: switching devices, non-pharm treatments, other causes
classifying COPD exacerbation
mild:
- dyspnea VAS <5
- RR < 24 breaths/min
- HR <95 bpm
- resting O2 sat ≥92% and ≤3% change from baseline
- CRP <10
> treatment: increased use of short acting bronchodilators
moderate: (3+ of these)
- dyspnea VAS ≥5
- RR ≥24 breaths/min
- HR ≥95 bpm
- resting O2 sat <92% or >3% change from baseline
- CRP ≥10
- hypoxemia or hypercapnia
> treatment: increased use of short acting bronchodilators, oral corticosteroids, maybe antibiotics
severe:
- moderate plus new onset of hypercapnia (PaCO2 >45 mmHg) and acidosis (pH <7.35)
where to treat an exacerbation
ambulatory:
- mild exacerbation, minimal comorbid involvement
- cooperative pt, good home support
hospitalization:
- respiratory failure signs/ symptoms
- failure to respond to initial medical management
- serious concomitant comorbidities
- insufficient home support
ICU:
- persistent/ worsening hypoxemia or hypercarbia despite ventilator
- worsening mental status change
- need for invasive mechanical ventilation
- hemodynamic instability
measuring exacerbation severity
- dyspnea visual analog scale (VAS)
- labs: respiratory rate, heart rate, O2 sat, CRP, arterial blood gas
oral corticosteroids in COPD exacerbation
prednisone 40 mg QD x5 days
- no taper needed (unless HPA axis suppression signs)
- can consider budesonide nebulized if contraindications to OCS
antibiotics in COPD exacerbation
cardinal symptoms to support antibiotic use:
- increased sputum purulence (more pus = more yellow)
- increased sputum volume
- increased dyspnea
- patient requires mechanical ventilation
- to assess sputum changes, rely on patient
common pathogens: H. flu, strep. pneumo, moraxella, atypical organisms (mycoplasma, chlamydophila)
empiric antibiotics:
- macrolide (azithromycin)
- tetracycline (doxy)
- beta lactams (amox/clav, amp/sul, 2nd-3rd gen cephalosporin)
- respiratory FQ (levofloxacin, moxifloxacin) ONLY if severe AND pt has beta lactam allergy
exacerbation follow up
- follow up within 1-4 weeks
- ensure appropriate response to therapy
- evaluate maintenance therapy
- assess non-pharm interventions (vaccines, smoking cessation, pulmonary rehab)