Complex patient
1/199
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
200 Terms
what is lipohaemoarthrosis
presence of blood and fat in a joint cavity that nearly always signals an acute intra-articular fracture
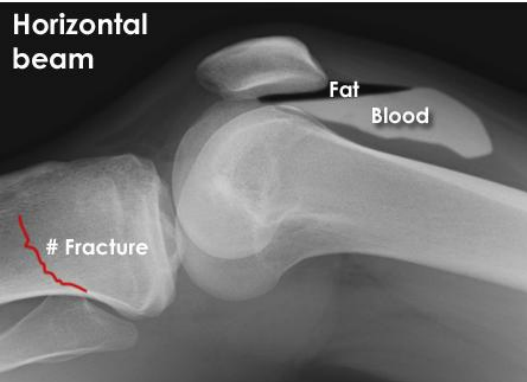
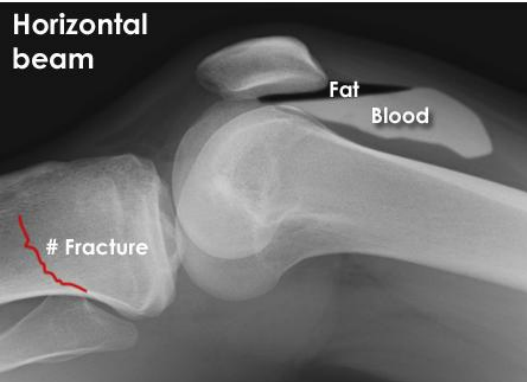
you examine this x-ray and identify a fracture as well as associated blood and fat in the joint cavity, what is this phenomenon called
Lipohaemoarthrosis
posterior fat pad is visible on a lateral xray of elbow, identify this phenomenon, why it occurs and what is likely to also be found on xray
Positive sail sign
Visible posterior fat pad occurs when joint effusion (from injury) fills olecranon fossa, psuhing the posterior fat pad out and making it visible
A fracture is likely to be found if there is +ve sail sign
Describe traumatic fracture and provide example
Fracture caused by abnormal force e.g. MVA, fall
Describe pathological fracture and provide example
Fracture in bone weakened by disease e.g. osteoporosis, tumor
Describe periosthetic fractures
Fracture at the point of weakness around a prosthetic implant or prior ORIF
Describe open/compound fractures and an associated risk
Broken bone pierces skin, high risk of infection
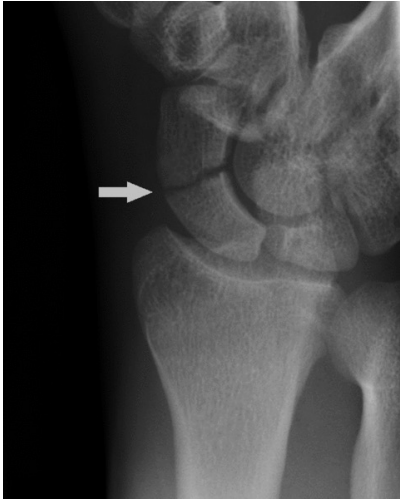
Describe buckle/torus fractures and how they occur
compressive forces cause one side of bone cortex to buckle and bulge outward and other side remains intact


describe what the arrow is pointing at and how it occurs
torus/buckle fracture whereby compressive forces cause one side of bone cortex to buckle and bulge outward whereas the other side remains intact
describe greenstick fractures and how they occur
bending forces cause bone cortex to fracture on one side
Identify the 3 types of simple fractures
Spiral, oblique, transverse
Identify the 2 types of wedge fractures
Intact wedge, fragmentary wedge
Identify the 2 types of comminuted/multifragmentary fractures
Intact segmental, Fragmentary segmental
Scaphoid fracture
-most common MOI
-clinical finding
FOOSH + tenderness over asb
note a specific scaphoid view is required xray
Colles fracture
-Describe what occurs
-Most common MOI
-Clinical finding
-Common associated fracture
Transverse + partial fragmentation of distal radius that angles dorsally
FOOSH
Dinner fork deformity due to dorsal angulation of radius fragment
Associated transverse fracture of ulnar styloid

Describe what happens in a monteggia fracture
Fracture of proximal ulna + disclocation of radial head

Describe what occurs in a galeazzi fracture
Fracture of distal radius + disruption of distal radio-ulnar joint (DRUJ)

You examine an xray and find a fracture of the distal radius, what structure should you also examine for damage/pathology
Distal radio-ulnar joint (incase of galeazzi fracture)
You examine an xray and find a fracture of the proximal ulna, what structure should you also examine for damage/pathology
Radial head (incase of radial head dislocation in a monteggia
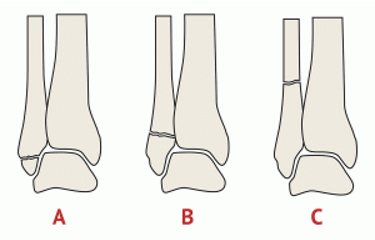
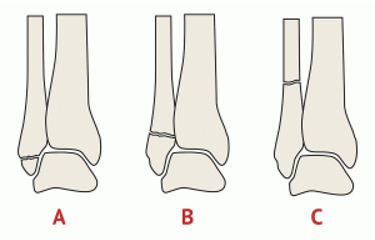
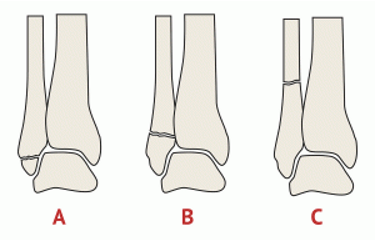
Describe what findings we would see in an ankle fracture with a grade A Weber classification
Fracture distal (below) to syndesmosis
Syndesmosis intact
Deltoid ligament intact
Usually stable
Describe what findings we would see in an ankle fracture with a grade B Weber classification
Fracture AT the level of the syndesmosis
Syndesmosis intact or partially torn
Deltoid may be torn
Variable stability
Describe what findings we would see in an ankle fracture with a grade C Weber classification
Fracture proximal (above) syndesmosis
Syndesmosis disrupted
Deltoid/medial malleolus involved
UNSTABLE - needs ORIF
you examine an xray and find an ankle fracture proximal to the syndesmosis
-what structure(s) will we most likely see damage involved in, as well (other than syndesmosis)
-can we expect this pt ankle to be stable or unstable? Is any specific treatment required?
We can expect medial malleolus or deltoid ligament to be involved
Unstable - requires ORIF
Identify the weber classification of ankle fracture given the following description - fracture distal (below) to syndesmosis, syndesmosis intact, deltoid ligament intact, usually stable
Weber A
Identify the weber classification of ankle fracture given the following description - fracture AT level of syndesmosis, syndesmosis intact or partially torn, deltoid ligament may be torn, variable stability
Weber B
Identify the weber classification of ankjle fracture given the following description - fracture proximal (above) to syndesmosis, syndesmosis disrupted, deltoid ligament or medial malleolus involved, UNSTABLE (ORIF)
Weber C
identify the structures affected in a trimalleolar ankle fracture
medial and lateral malleolus, posterior malleolus (distal posterior tibia)
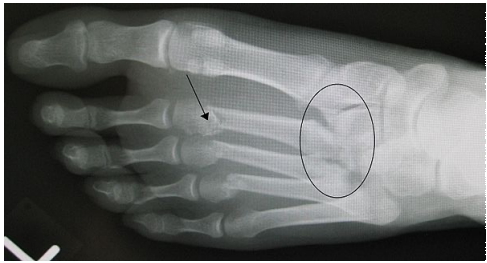
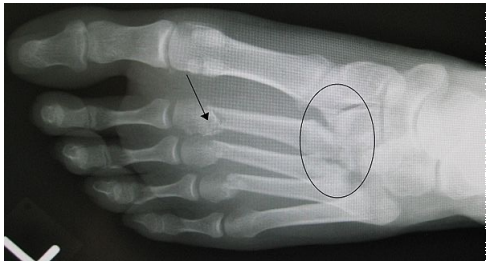
Describe what occurs in a jones fracture and what specific imaging is needed to detect it and distinguish from lateral ankle sprain
Fracture of diaphysis of 5th metatarsal, AP/Oblique/Lateral foot views with foot fully dorsiflexed required

Identify what part of the 5th metatarsal is affected in a jones fracture
Diaphysis

what xray sign can we see in lisfranc injuries
gap between base of 1st and 2nd proximal metatarsals

Pt presents with pain and swelling over midfoot and bruising on sole of foot following a fall from height, what is your primary hypothesis for diagnosis without imaging
Lisfranc injury
Pt presents with pain over midfoot after dropping a couch on foot whilst moving house, upon xray inspection you find a gap between base of 1st and 2nd proximal metatarsals, what is your primary hypothesis for diagnosis
Lisfranc injury
What specific xray view is most specific for detecting lisfranc injuries
weight bearing AP view
Identify the most common MOI for fracture of 5th metacarpal and describe why this occurs
Punching with closed fist places big axial load on metacarpal head causing transverse (most commonly) fracture of metacarpal shaft/head

describe what ACTIVE movement would be lost in someone who has suffered mallet finger
DIP extension

describe what ACTIVE movement would be lost in someone who has suffered mallet finger and describe why this occurs
Hyperflexion injury at DIPJ avulses the extensor tendon attachment from dorsal base of distal phalanx, causing loss of DIP extension

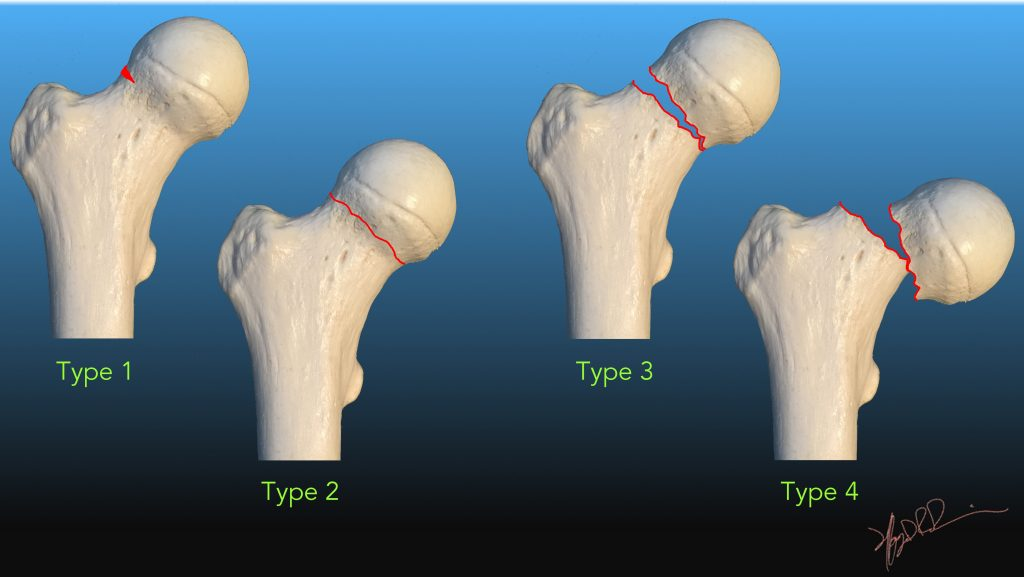
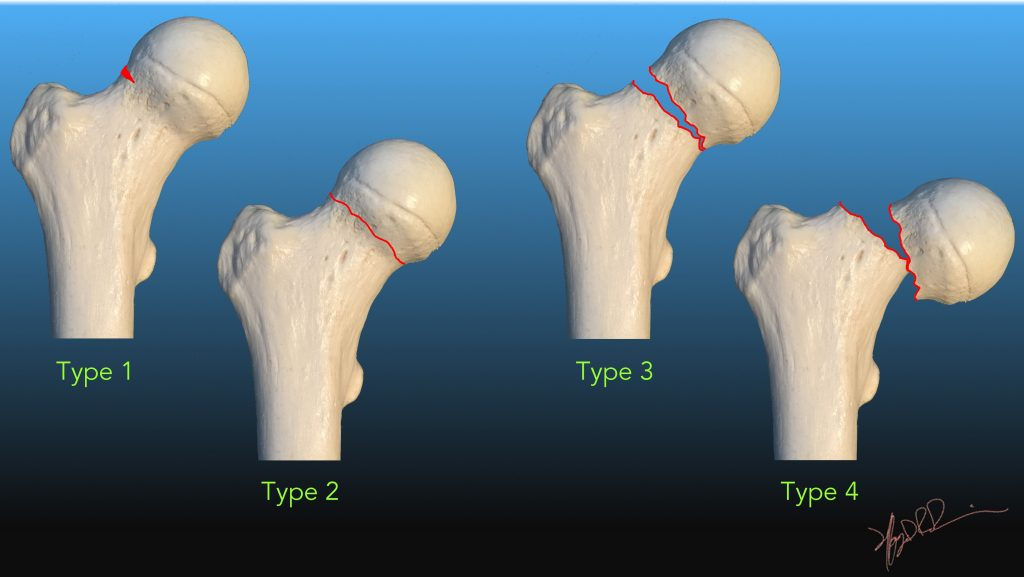
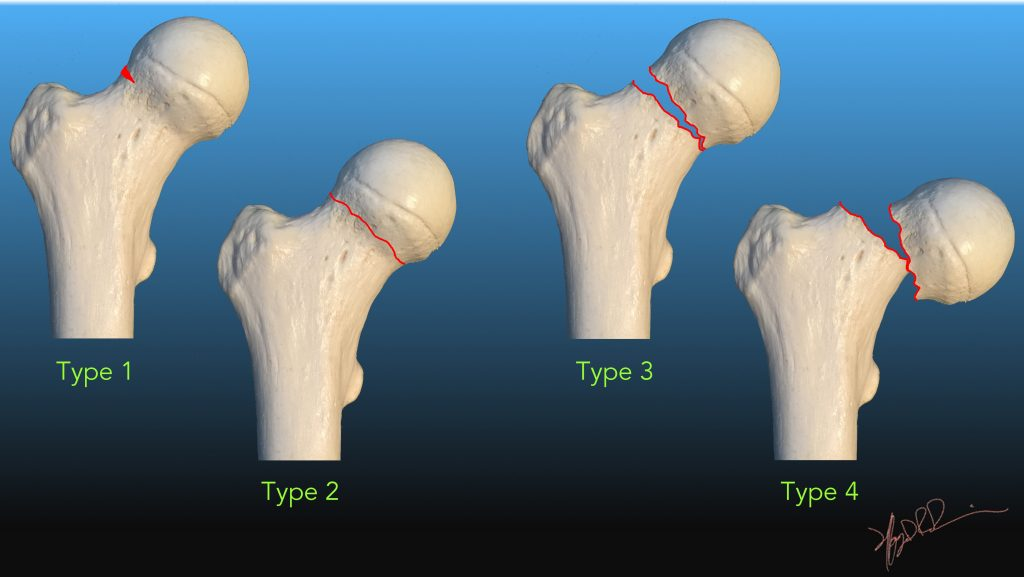
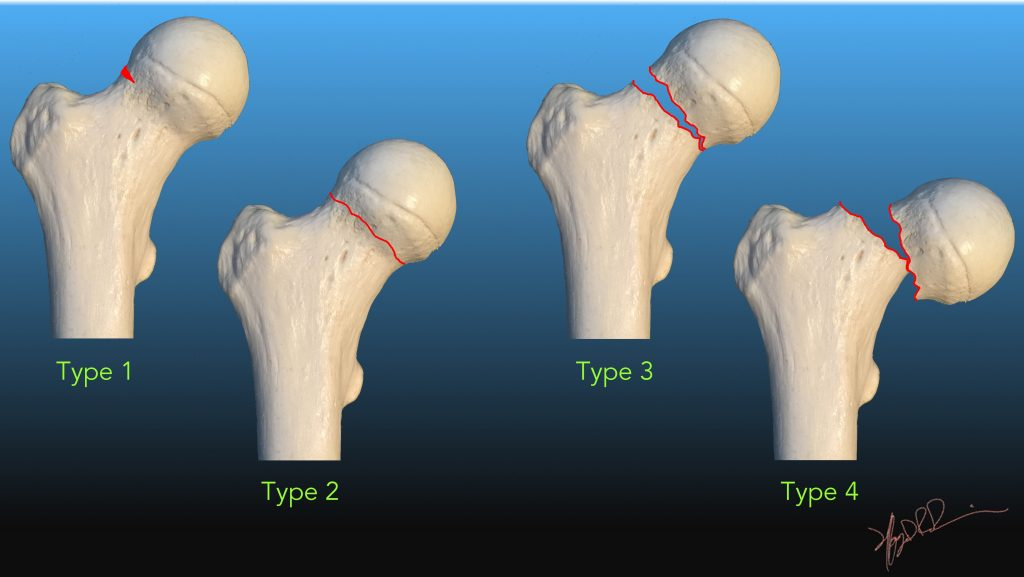
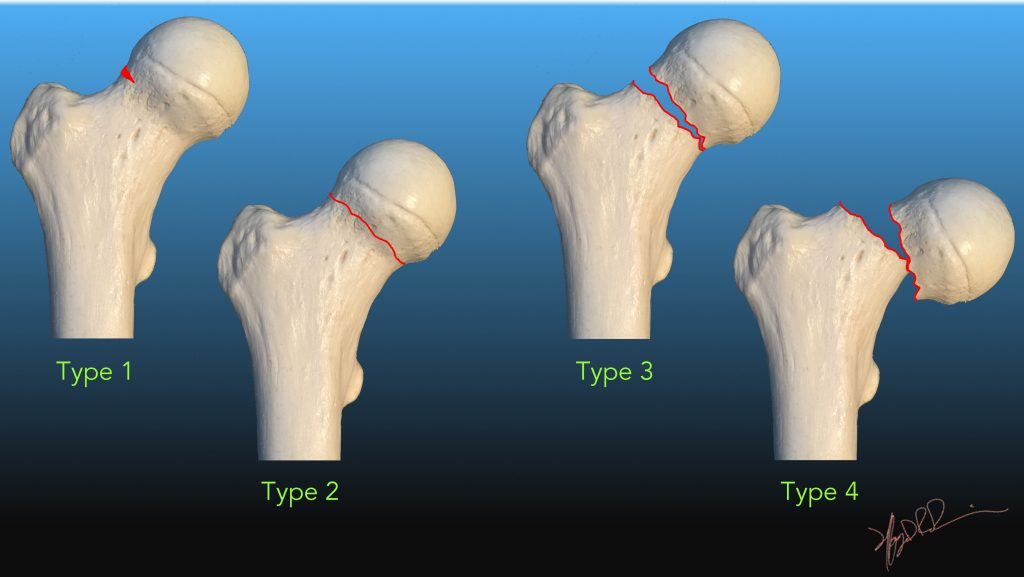
Describe subcapital/intracapsular hip fractures
Fracture at or just below the femoral head
Describe subtrochanteric/extracapsular hip fractures
Fracture between greater and lesser trochanters, outside the capsule
Describe subtrochanteric hip fractures
Below lesser trochanter
Which garden classification of intracapsular hip fracture has BEST prognosis and describe it
Garden 1 - Incomplete/impacted fracture, facilitates vascular regrowth
Which garden classification of intracaspular hip fracture has WORST prognosis and describe it
Garden 4 - Complete, full displacement greater than 50%, bone ends fully seperated, highest AVN risk
Describe Garden 1 Intracapsular hip fractures
Incomplete/Impacted, bone ends impacted into eachother, best prognosis, facilitates vascular regrowth

Describe Garden 2 Intracapsular hip fractures
Complete/non-displaced, fracture line complete but minimal bone end shift, less stable but good prognosis
Describe Garden 3 Intracapsular hip fractures
Complete, partial displacement less than 50%, vascular compromise likely, worse prognosis
Describe Garden 4 Intracapsular hip fractures
Complete, full displacement greater than 50%, bone ends fully seperated, worst prognosis, highest AVN risk
What are the 3 clinical rules for dislocation/fracture
ALWAYS reduce the dislocation
ALWAYS check neurovascular status before AND after reduction
ALWAYS obtain post redcution xrays to confirm satisfactory position
In displaced garden 3/4 fractures, what surgical management is indicated
Hemiarthroplasty, THR
Recall ALL of the ottawa ankle rules
Tenderness over posterior edge or tip of medial or lateral malleolus
Tenderness over navicular
Tenderness over base of 5th metatarsal
Inability to weight bear
Recall ALL of the ottawa knee rules
Age 55 or older
Unable to flex knee to 90deg
Unable to weight bear
Point tenderness at proximal fibular head
Isolated point tenderness of the patella
Identify the 6 core cardiorespiratory problems
Type 1/2 respiratory failure
Increased WOB/breathlessness
Sputum retention
Loss of volume
Pain
Reduced exercise tolerance
What should be included when educating a patient pre-operation, what should we also demonstrate to the patient
Role of physio
Expected post op experience
Effects of surgery
Early mobilisation
Pain relief importance
Demonstration of breathing exercises, circulation exercises, supported cough, bed mobility/transfers, post-op exercises
When performing a circulatory assessment how do we conduct a DVT screen
Assess the patients calf for swelling, redness, localised pain/tenderness, increased temperature, positive Homans sign (calf pain on passive ankle DF)
What would we see in a positive Homans sign and what does it test for
Calf pain on passive ankle dorsiflexion, tests for DVT
note low sens and spec, often false positives
If a patient has had spinal/epidural anesthetic used during their surgery/operation, what assessment is required and what should be included?
Neurological assessment - hip, knee, ankle strength and sensation
Identify some patient related risk factors for post-op complications
Smoking Hx
Age >60
Obesity (BMI >27)
Immobility
Pain
Medications
Identify some procedure related risk factors for post-op complications
Location - upper abdomen or thorax
Prolonged anesthesia >180mins
Emergency vs Elective surgery
Identify the most common post surgical complication and describe it
Atelectasis - collapse of avleoli, up to 10-15% of lung tissue can collapse within 15min of sedation
Clinical signs of post-surgical atelecatasis
Reduced PaO2, reduced lung compliance, reduced FRC
Non-productive cough, tachycardia, tachypnea, wheeze, chest pain
Changes on CXR, auscultation and percussion
Clinical signs of post surgical chest infection
SpO2 less than 90% on 2 consecutive days
Temperature >38 deg after day 1 post-op
Productive sputum
Abnormal breath sounds on auscultation
WCC raised
Infiltrates/consolidation on CXR
Opiod/narcotic analgesia side effects and mx for each one
Drowsiness/reduced respiratory drive - requires supplementary O2
Nausea/vomiting - managed with antiemetics
When should physiotherapists plan treatment times for post operative patients
Around analgesic onset
Identify benefits of early mobilisation
Prevents immobilisation effects
Increases minute ventilation
Increases cardiac output
Maintains muscle strength
Provide an example of how we can gradually progress mobilisation in stages
e.g. stage 1 - in bed exercises
Stage 1 - Breathing and circulation exercises in bed
Stage 2 - Sit out of bed (legs over edge, then chair)
Stage 3 - Walk short distances with appropriate aid
Stage 4 - Self care (hygiene, dressing)
Stage 5 - Progressive distance, stairs, independence
When should we commence mobilisation of patient
As soon as pt is haemodynamically stable
Identify some factors to consider before mobilising a pt
Incision location and type
Level of pain and adequacy of analgesia
presence of adverse effects (dizziness, N&V)
Attachments (IV lines, drains, catheters, O2)
Assistance available vs required
Equipment available (walking aids, chairs)
Pre existing conditions and premorbid mobility level
Identify the dislocating location for a posterior THR approach
Flexion >90deg, adduction past neutral, IR past neutral (or combined)
Identify the dislocating location for a anterior/anterolateral THR approach
Forced extension; flex or ext with Add+ER
THR post-op management (day 0, 0-1, 1-2, 2)
Day 0 - circulorespiratory exercises, hip ROM and quads (hip flexion limited to 90deg), IRQ, bridging/bed mobility
Day 0-1 - FWB, mobilise via unaffected side, rollator initially
Day 1-2 - Sitting, allow 30mins initially, progress as tolerated
Day 2 - Progress ROM/strength, balance ex, progress aid to 4WW/crutches/SPS, stairs, car transfer
*Discharge target day 3-5
Recall hip precautions post THR (lifelong; strict first 12 weeks)
No hip flexion beyond 90deg
No adduction past neutral
No IR past neutral
Do not sit in low chairs or cross legged
Do not lie on affected side
Do not squat or bend from hips
No twisting on affected leg in standing
No driving for 6 weeks until cleared by surgeon
Identify possible post-operative complications of THR
Dislocation, DVT, infection, component loosening
Identify possible peri-operative complications of THR
scaitic nerve damage (foot drop), poor acetabular positioning, acetabulum/femur fracture, excessive blood loss
Describe what occurs in a hip arthrodesis
Fusion of femur and pelvis at 15-20deg flexion, neutral abduction and rotation
Describe what occurs in a Girdlestones procedure (excision arthroplasty)
Surgery that removes femoral head and neck, results in limb shortening
Describe what occurs in a birmingham hip resurfacing and advantages of this procedure
Metal cap replaces femoral head and metal cup for acetabulum, preserves femoral head/neck, less bone resection, good long term outcomes
Physio Mx for a menisectomy
FWB, rapid rehab = ROM, SLR, IRQ, limit walking to manage swelling
Physio Mx for a meniscus repair
PWB or NWB on crutches, ROM, IRQ, SLR, manage swelling
Advantage of meniscal repair > menisectomy
Preserving meniscus reduces OA risk
Physio Mx for a ACL reconstruction
Surgeon dependent, usually FWB, clsoed chain exercises for 3months, no open chain for 6-12 weeks
Identify 4 types of ACL grafts that can be utilised for reconstruction
Synthetic (LARS), allograft (cadaveric), hamstring autograft, patellar tendon autograft
Advantage/Disadvantage of synthetic (LARS) grafts for ACL reconstruction
Adv - quicker return to sport
Disadv - no significant diff at 24 months, history of failures
Advantage/Disadvantage of allograft (cadaveric) grafts for ACL reconstruction
Adv - no donor site pathology, shorter op, replaced by new tissue
Disadv - rejection risk, rupture risk (esp donors >30-35yrs old)
Advantage/Disadvantage of hamstring autografts for ACL reconstruction
Adv - good strength, no anterior knee pain
Disadv - elastic creep leads to slightly lax graft
Advantage/Disadvantage of patellar tendon autografts for ACL reconstruction
Adv - strong, replaced b new tissue
Disadv - anterior knee pain, donor site pathology
What is the gold standard procedure for severe knee OA
total knee replacement
discharge criteria for those in rehab for TKR
SLR with <5deg lag, >/= 90deg flexion, stairs, independent HEP, target day 3-5
what procedure is used for those with medial tibiofemoral OA with varus/valgus deformity
High Tibial Osteotomy (HTO)
Describe what occurs in a HTO
Bone is divided and repositioned to align tibia and femur to distribute laod more evenly
TKR post-op management (Day 0 and 1 exercises, Day 0-1 mobility, Sitting, goals)
Day 0 ex - circulorespiratory exercises
Day 1 ex - Quads, active/assisted knee flexion (aim 90deg), IRQ, SLR
Day 0-1 mobility - FWB/WBAT, out of bed on unaffected side, progress rollator to crutches
Sitting - day 1-2, 30 min initally, apply ice
Goals - Knee flexion >90deg, extension 0deg, SLR, HEP independence, stairs
Clinical features of a displaced NOF#
pain, limb shortened and externally rotated, unable to WB
Clinical features of an undisplaced NOF#
pain, no limb orientation change, sometimes can WB, harder to detect may need MRI/CT/bone scan
Physio Mx for #NOF
Mobilise day 1 (generally WBAT unless young pt <65)
Easily fatigued (focus on functional activities only)
Analgesia pre mobilsiation, appropriate walking aid, miminise bed rest but ensure adequate rest time
Exercises similar to THR (Circulo-respiratory exercises, hip ROM & quads (hip flexion limited to 90°), IRQ, bridging/bed mobility) however, consult with nursing staff/surgeon
What 2 diagnostic features are ALWAYS present in psot operative delirium
Decreased attention
Disorganised thinking
Identify diagnostic features of post operative delirium
Decreased attention, disorganised thinking (always present)
Rambling/irrelevant/incoherent speech
Decreased consciousness, hallucinations/misinterpretations, disturbed sleep cycle, memory impairment, disorientation to time/place/person
Physio Mx for ankle fractures
NWB, moonboot day 1 if swelling allows, elevate 10 days, IRQ, SLR, hip/knee flexion, hip abd/add
Identify 3 TSJR indications
Hard to control pain, esp if affecting sleep/ADLs
Posterior humeral head subluxation
Glenoid cartilage degeneration (preferred over hemi for OA)
Identify 5 contraindications for TSJR
Insufficient glenoid bone stock
Rotator cuff arthropathy
Irrepairable rotator cuff
Deltoid dysfunction
Active infection
Identify 4 reverse TSJR indications
Cuff tear arthropathy
Rotator cuff insufficiency
Anterior-superior escape
3 or 4 part fractures
Identify factors in a pt that would make a reverse TSJR appropriate (not indications)
Low functional demand
>70yrs old
Sufficient glenoid bone stock
Must have working deltoid muscle
Must have intact axillary nerve
Why must someone have a working deltoid muscle to be an appropriate candidate for reverse TSJR
Deltoid is the main muscle for movement post-op, hence must also have workign axillary nerve
Post-op physio for TSJR
Circulation ex, mobilise out of bed day 1
Shoulder immobiliser sling until week 6
No WB through shoulder, no lifting
Exercises = elbow, wrist, hand + grip, c-spine
PROM = flexion 90deg, ER to 0deg
Progress to ER isometrics
Limit passive ER
IR eccentric and isometric