Physl 210 B EVERYTHING FOR FINAL EXAM
1/506
Earn XP
Description and Tags
GIT, Respiratory, Renal, Endocrine, Reproductive
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
507 Terms
GIT internal or external
Still considered part of the “external environment”
Main functions of GIT
Digest and absorb important nutrients, minerals and water from “external” environment to internal environment; excrete waste products and protect the host from infection/harmful substances
Upper third of GIT
Made of skeletal muscle (where we can feel swallowing in our esophagus)
Mucosa
Outermost layer of the GIT. Made of 3 sections: epithelium, lamina propria and muscularis mucosa
Villi, microvilli and crypts function
To greatly increase the surface area of the GIT
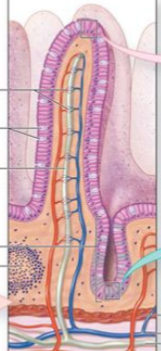
Epithelial layer
Outer part of mucosa. Main barrier for deciding what gets into the basal interior (selective uptake of nutrients, electrolytes and H2O; ensures harmful substances don’t get into the interior). Contains both villi (outward projections) and crypts (inner folds) to increase surface area. Has distinct basolateral and apical sides, helps keep specific transport proteins restricted to their sections (via tight junctions). Replaced every 5 days
Lamina propria
Second layer of the Mucosa; contains the connective tissue and all the important vessels (Blood vessels and capillaries; lymphatic drains (lacteals); nerve fibers and immune/inflammatory cells.

Muscularis mucosa
Third layer of the mucosa, contains the smooth muscle. Not responsible for GIT contraction, may be important for villi movement

Paracellular pathway
Movement of small, water soluble particles through tight junctions located in the epithelial layer
Transcellular pathway
Transport of larger molecules via transport proteins from the lumen to the basolateral surface of the cell
Submucosa
(submucosal) Plexus of nerve cell bodies; also contains connective tissue, blood and lymphatic vessels

Muscularis externa
Thick inner layer of circular muscle, involved in narrowing the lumen (responsible for contractions). Myenteric nerve plexus found here, and thinner outer layer of longitudinal muscle
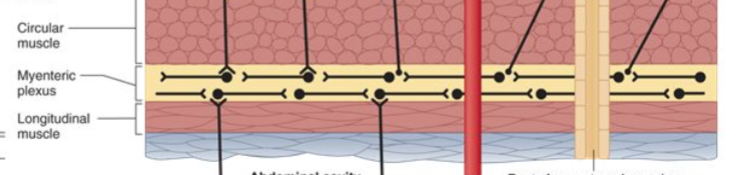
Muscularis externa circular muscle function
Cause narrowing of lumen
Muscularis externa longitudinal muslce function
Shorten tube
Serosa
Connective tissue, encases intestine and forms connection to abdominal wall
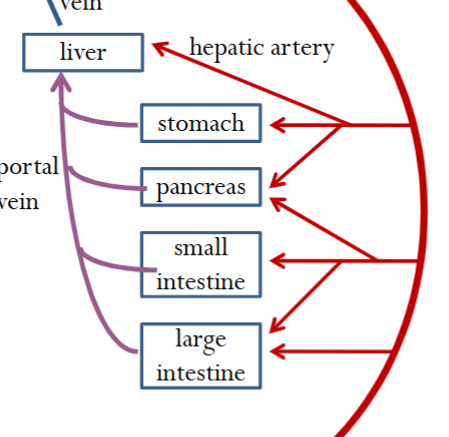
GI blood circulation
Critical for carrying away water soluble absorbed nutrients from GIT to other areas of the body; also secretes hormones into GIT to aid in digestion and breakdown.
Liver blood circulation
75% from digestive organs (blood rich in nutrients and lower in O2) via portal vein; 25% from hepatic artery (oxygenated). Acts as a filter
Regulation of GIT processes
Secretion and motility most important. Governed by the amount and type of contents in GIT.
Intrinsic/enteric GIT regulation
Controls secretomotor neurons. Contained completely within GIT (brain of the gut, as many nerves as spinal cord), functions independently of CNS (involuntary). Uses two nerve networks = myenteric plexus and submucosal plexus
Myenteric plexus
In general, influences smooth muscle (contained in the muscularis externa)
Submucosal plexus
In general, influences secretion (contained in the submucosa)
Extrinsic regulation of GIT
Through autonomic NS (Para and symp); based on hunger, sight/smell of food, emotions. Recall that para allows for digestion and symp stops it.
Hormones of GIT
Released by endocrine cells into the blood. Secretin, Cholecystokinin, Gastrin and Glucose dependent Insulinotropic peptide. All peptide hormones.
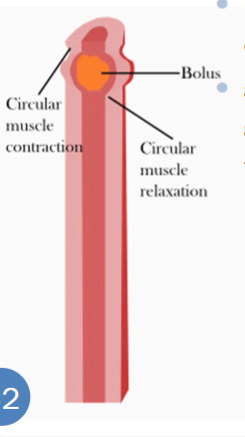
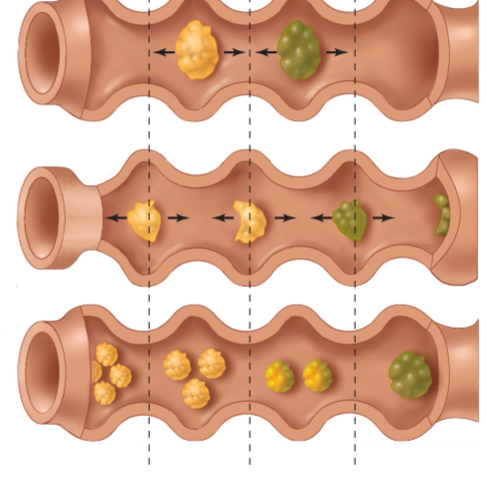
Peristalsis (propulsion)
Contraction and relaxation of the two smooth muscle layers working in tandem to propel food. Longitudinal and circular always doing the opposite of one another. Muscles on top of food contract, muscles below food relax to allow for smooth passage down, towards the anus
Segmentation
Contraction and relaxation of intestinal segments where the contents are not moved forward, but rather bounced around to mix them and further break them down. Slows down transit time to allow for increased absorption and contact with digestive enzymes
GIT pacemaker cells
Located in smooth muscle, constantly undergoing spontaneous depolarization/repolarization cycles (slow waves). These propagate to the muscles via gap junctions. In the absence of stimulus, these do not produce significant contractions. Maintains the frequency of contractions
Contraction of GIT
Occurs when excitatory hormones and NT further depolarize the membrane. The more action potentials fired, the stronger the force of contraction (cannot increase the frequency of contractions, only the force).
Short GIT nerve reflex pathways
local or intrinsic pathways inside the GIT (not involved with CNS). Once hormones reach targets and bind, this is what occurs and how changes propagate.
Long GIT nerve pathways
Extrinsic pathways activated by sight, smell, food etc which relay info to CNS. These then activate the autonomic nerve pathways and got to the GIT.
Cephalic GIT control/stimulation
Receptors here are activated by seeing food, smelling food, tasting food and emotional state etc. Parasympathetic fibers then activate the GI nerve plexi.
Gastric GIT control/stimulation
Receptors here are stimulated by peptides, amino acids, distension. Hormone gastrin regulates this, as well as short/long nerve reflexes
Intestinal GIT control/stimulation
Receptors here stimulated by amino acids, peptides, distension and ___. Long and short nerve reflexes. Hormones CCK and GIP
Hypothalamus GIT functions (Food)
Lateral area responsible for hunger; ventromedial responsible for satiety. Also secretes neuropeptide Y (increase hunger) and melanocortin (decrease hunger)
Orexigenic factors
Ghrelin (Hormone secreted in stomach, causes release of Neuropeptide Y) , Neuropeptide Y (NT in hypothalamus which stimulates hunger - acts on lateral region?)
Anorexigenic factors
Leptin (from adipose tissue), Peptide YY (from intestines), Insulin (from pancreas - makes sense since glucose has to be present), Melanocortin from hypothalamus.
Leptin as an example (when satiated)
When we are intaking lots of food, more fat deposits build up in adipose tissue. These release leptin, which decreases the feeling of hunger (decreases neuropeptide Y release) and increases metabolism (to break down the food present faster).
Leptin unique case (when hungry)
When there is an absence of leptin (due to no fat deposits when food is scarce), the body increases its feeling of hunger and decreases metabolism (so you feel more hungry but can live off of less food for longer).
Regulation of water intake
Done by hypothalamus thirst centre. Main way is through osmolarity changes (even just 1%), particularly after eating a salty meal. Secondary way would be large amounts of plasma lost, if excessive bleeding, vomiting or diarrhea occurs. Dry mouth/throat also cause thirst.
When plasma osmolarity increases (related to thirst)
Osmoreceptors in the hypothalamus thirst centre cause vasopressin to be released (antidiuretic) which causes the kidneys to conserve more water.
When intense plasma loss occurs (related to thirst)
Baroreceptors in the cardiovascular system are stimulated, as well as in kidneys. Production of angiotensin 2 which increases thirst (in animals)
Obesity and Leptin
Originally thought that obese people were those lacking leptin (as shown by some mice studies where leptin is deactivated). However, for most obese people, there is actually a high concentration of leptin present, their body is just not able to recognize it properly (leptin disorder).
Salivary glands
Parotid (serous), submandibular (serous and mucous) and sublingual (mucous). Together produce ~1500mL of saliva per day. ONLY GIT COMPONENT NOT IMPACTED BY HOROMONES
Saliva composition and characteristics
Hypotonic (Low Na and Cl concentration), alkaline (rich in bicarbonate and K+), 97-99% water, digestive enzymes (lipase and amylase), some glycoproteins (mucous) and antimicrobial factors (lysozyme and lactoferrin)
Saliva functions
Begins digestion (slightly - amylase and lipase); antimicrobial properties (lactoferrin and lysozyme); lubricates mouth and food for easier swallowing and speech; buffer action against HCl if vomiting/acid reflux (bicarbonate content)
Acinar cells
Leaky (tight junctions allow ions and water through which makes the initial solution isotonic); ensure the proper proteins are present in the saliva
Myoepithelial cells
The “pump” portion of the turkey baster - push the saliva secreted by the acinar cells into the duct.
Ductal cells
Responsible for reuptake of ions (Na and Cl) which causes the saliva to be hypotonic. Very tight junctions connect these cells, not allowing for any water to leak through.
Salivary digestive components
Amylase, Lipase
Salivary production increased when
Parasympathetic is activated = smell and taste, food, nausea (about to vomit). Causes an increase of blood flow to the glands which enables the high fluid and metabolic requirements needed for increased secretion. Also increases proteins from acinar and myoepithelial cell activity.
Salivary production decreased when
Parasympathetic inactivated = sleeping, tired, fearful, some drugs
Xerostomia causes
Some drugs (inhibit parasympathetic NS), gestational (no salivary glands), autoimmune (Sjogrens), radiation treatment.
Xerostomia side effects
dry mouth, decreased oral pH (increase in tooth decay/bacteria), difficulty lubricating and swallowing food. Treatment = drink water and fluoride.
Esophagus functions and characteristics
Specialized tube which ensures food does not end up in our lungs. Top 1/3 is skeletal muscle (where we can feel ourselves swallowing), the rest is smooth muscle (where peristalsis can take place). Epithelial layer is very thick (20-30 cells), ensures that the rough food particles which the tube is exposed to do not cause damage. Also striated and smooth, which ensures that the food glides down to the stomach.
Esophageal sphincters
One at the entrance just behind the pharynx (skeletal muscle) and one at the entrance to the stomach (smooth muscle). Always closed except when swallowing, burping or vomiting. Ensures that food does not enter the airway (top) and that stomach acid is not able to “backwash” up the tube (bottom)
Heart burn
When stomach acid leaks out of the sphincter into the esophagus and is not properly neutralized. Can be caused by an inefficient sphincter, after a big meal and during pregnancy (lots of pressure on stomach).
Not a major source of absorption
What is NOT one of the functions of the stomach
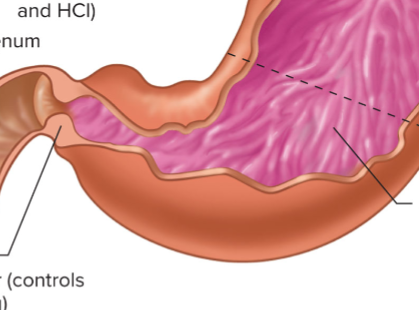
Stomach fundus and body
Top portion; made of thinner smooth muscle layers. Secretes mucus, pepsinogen and HCl
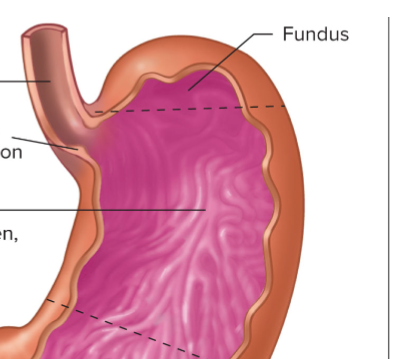
Stomach antrum
Lower portion; made of thicker smooth muscle layers (for mechanical grinding and mixing). Secretes mucus, pepsinogen and gastrin
Major exocrine stomach products
Substances secreted into ducts directly onto epithelial surface: Mcuous (prevent self digestion), HCl and Pepsinogen
Minor stomach secretory products
Intrinsic factor (Vit B absorption), Gastrin (endocrine for HCl production), Histamine (paracrine release for HCl production), Somatostatin (paracrine release for HCl inhibition)
Chief cells (stomach)
Gastric gland cell found all throughout the stomach; secrete pepsinogen
Enteroendocrine cells (G cells)
Gastric gland cell found only in the antrum. Secrete the hormone gastrin into the blood (endocrine)
Enterochromaffin-like cells (ECL)
Gastric gland cell found all throughout the stomach; secretes histamine
D cells
Gastric gland cell found all throughout the stomach; Secretes somatostatin
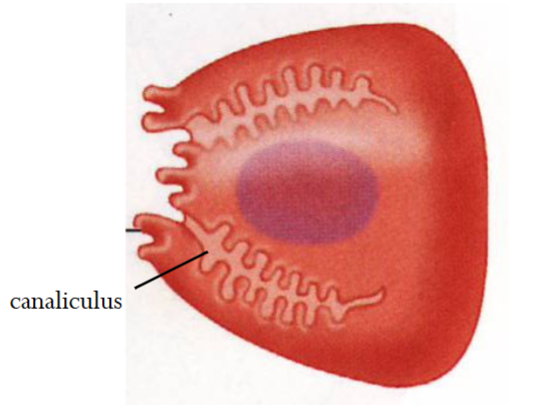
Parietal cells
Found in gastric glands located only in the body/fundus. Produces HCl (and intrinsic factor); impacted by somatostatin, gastrin, Ach and histamine. Contains canalicular structures, which increase cell surface area - can be adjusted in size when active vs inactive.
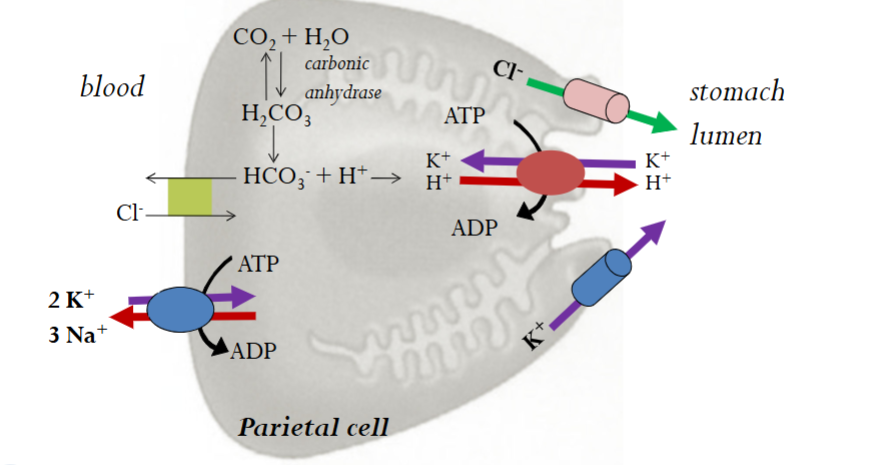
Acidification of stomach lumen steps
Happening in Parietal Cells:
H+/K+ ATPase (pumps K into cell and H+ out to lumen surface - where the H in HCl comes from)
Carbonic Anhydrase (Catalyses the formation of H2CO3 from H2O and CO2 - H2CO3 then dissociates into HCO3 and H+; this is where the H+ is taken from to be pumped out).
Cl-/HCO3- exchanger (secondary active transporter which restores the pH balance of the cell; pushes out basic bicarbonate and brings in acidic Cl - Where the Cl in HCl comes from).
K+ channels (passive diffusion of K out of the cell to restore K balance)
Cl- channels (passive diffusion of Cl out to balance the loss of K ions)
Cephalic stomach phase
Starts when our brain sees, smells or tastes food. Anticipatory and excitatory; travels via the vagus nerve through the parasympathetic system
Gastric stomach phase
Major phase, begins when food reaches the stomach. Excitatory, mainly vai gastrin
Intestinal stomach phase
Mainly inhibitory, due to presence of acid and fat. Secretin, CCK and others secreted to inhibit.
Gastrin impacts (stomach)
Increases the production of HCl. Directly from blood to parietal cell and also indirectly by stimulating endochromataffin-like cells to produce more histamine.
Ach impacts (stomach)
Increases the production of HCl. Directly from the parasympathetic NS to parietal cells and also indirectly via: 1. Negatively stimulates D cells to slow production of somatostatin 2. increases production of gastrin 3. Increases production of histamine
Histamine impacts (stomach)
Increases HCl production by directly stimulating parietal cells
Somatostatin impacts (stomach)
Decreases HCl production (only one that does so in the stomach!). Stimulated by an increase in stomach acidity (more H+). Inhibited by Ach. Directly inhibits parietal cell as well as indirectly inhibits histamine and gastrin release.
Pepsinogen activation and secretion
Secreted by chief cells. Starts off in zymogen form (so as not to degrade cellular proteins) and is then activated by low stomach pH (turns into pepsin). Begins degradation of proteins; irreversibly inactivated once in the small intestine due to pH increase.
Gastric motility
Food stimulates peristaltic waves, weak contractions occur in body, strong contractions occur in the antrum. Pyloric sphincter allows a small, controlled amount of food to leave the stomach and enter the small intestine. The pyloric sphincter then slams shut and forces the food to move back into the main area of the antrum for further breakdown and mixing.
Electrical basis for gastric motility
Pacemaker cells in the smooth muscle spontaneously depolarize and repolarize in slow wave fashion (no contractions). When food is sensed, excitatory hormones and NT released causing contractions. Frequency of contractions is set in stone by pacemaker cells, strength of contraction is proportional to amount of stimulus.
Vomiting Triggers
Ejection of potential pathogens, toxins, when motion sickness occurs, when head injuries occur, when there is an infection/disturbance in the GIT and during specific sights/smells - all of which act on the vomiting centre in the medulla oblongata.
Vomitting steps
Vomiting centre in medulla oblongata is stimulated. Nausea occurs, salivation is increased (to protect against HCl), Glottis closes (to prevent vomit from going down trachea), Esophageal sphincters relax, Diaphragm and abdomen muscles contract and reverse peristalsis occurs
Vomiting benefits
Removal of harmful pathogens/toxins. Learning should occur to prevent ingestion of harmful substances in the future.
Vomiting disadvantages
Dehydration, loss of salts, loss of H+ (metabolic alkali - blood can become more basic), potential for tooth decay (enamel degradation)
Ulcers
A damaged/eroded area of the GIT mucosa, usually in the stomach and especially in the duodenum (where the lining is thinner). Caused by an imbalance between aggressive (pepsin, HCl) and protective factors (mucus and bicarbonate), H pylori, drugs which decrease prostaglandin (aspirin, ibuprofen), smoking, excessive alcohol etc.
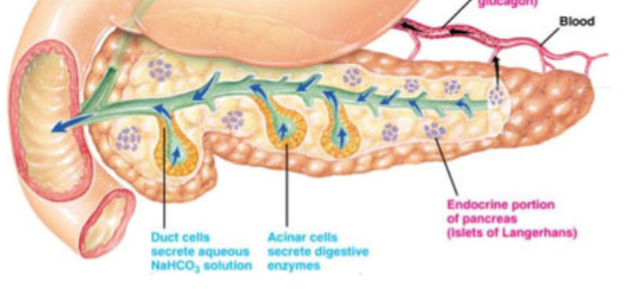
Pancreas functions
Exocrine duct (critical for digestion, produces secretions/enzymes which go to the duodenum and digest food, as well as neutralize HCl - lots of bicarbonate production. Produces enzymes in excess, loss of absorption/digestion only noted if function falls below 10%). Also an endocrine duct (produces hormones to regulate other body functions)
Oddi Sphincter
The common sphincter which connects the pancreatic duct with the bile duct before entry into the duodenum.
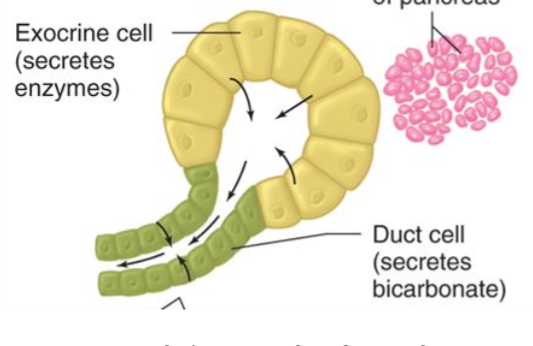
Pancreatic ducts
Very similar to salivary ducts. Acinar cells produce and secrete digestive enzymes. Duct cells secrete H2O and HCO3. Pancreatic juices secreted = Isotonic solution (Na/K same concentration as blood), High in bicarbonate, high in digestive enzymes, low Cl
Highest bicarbonate concentration
Produced by pancreatic cells
Medium bicarbonate concentration
Produced by salivary cells
Base and Acid tide
How the body maintains balance of pH - parietal cells produce a lot of HCl for the stomach, which causes an “alkaline tide” of HCO3 to rush into the blood. Later, the pancreatic cells produce a lot of HCO3 for the small intestine, which causes an “acid tide” of H to rush into the blood. Blood from both of these places then flows through the portal vein and combines in the liver for neutralization.
Prevention of autodigestion
The reason why all the proteases are stored and released as zymogens from the pancreas, so they do not degrade important transport proteins and other cellular machinery found in the pancreatic cells.
Cystic fibrosis pancreatic impacts
Mutation of the CFTR Cl channel which renders it much less effective. As a result, enzymes are not washed out of the ducts by HCO3 and H2O and therefore do not reach the intestine.
Enterokinase
Stored in the microvilli in the intestine. Cleaves trypsinogen to trypsin (activates).
Trypsin
Cleaves chymotrypsinogen to chymotrypsin; Pro-elastase to elastase and Pro-carboxypeptidase A and B to Carboxypeptidase A and B. Also cleaves Prephospholipase A2 to Phospholipase A2
Trypsin, Chymotrypsin and Elastase
Pancreatic digestive enzymes which are only able to chop up proteins from the middle, therefore unable to generate individual amino acids (cannot attack N or C term)
Carboxypeptidase A and B
The only pancreatic digestive enzyme which can generate individual amino acids, by cleaving at the C term.
Amylase
Pancreatic enzyme (same as the one found in saliva). Begins breaking down alpha 1-4 bonds in amylose (linear chain portions, not able to break up the branches). Cannot generate individual glucose molecules
Lipase
Pancreatic enzyme which breaks down triglycerides into free FA and 2-monoglycerides.
Cholesterol Esterase
Pancreatic enzyme which breaks down cholesterol-esters into cholesterol and free FA
S-cells
Endocrine regulation (local, shorter pathway) of pancreatic juices. Upon stimulation by acid in the duodenum, begins release of secretin which travels via the blood to pancreatic ducts to increase HCO3 production
I-cells
Endocrine regulation (local, shorter pathway) of pancreatic juices. Upon stimulation by partially digested fat/proteins in the duodenum, begins release of CCK which travels via the blood to pancreatic acinar cells to increase enzyme production
Nerve pancreatic regulation
Longer pathway, done through the parasympathetic NS, which upon sensation of food releases Ach to the pancreatic acinar and increases enzyme production
CCK example
When FA and amino acids are present in the small intestine, CCK is triggered to be released into the blood. CCK then travels to the pancreas and increases enzyme production, and also travels to the gall bladder, causing contraction and the flow of bile into the small intestine. It then causes the sphincter of Oddi to relax, allowing the enzymes and bile (fat emulsification) into the intestine. When the fats and amino acids are sufficiently absorbed, CCK release is stopped due to negative feedback.