CM II Week 6 (Sleep Disorders)
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
Myths vs Facts of Sleep
lots of them just to read
All Facts
•Less than 35% of US adults get the recommended 7-9 hours of sleep
•The brain CANNOT recover lost sleep
•You CANNOT “catch-up” on weekends
•Surgeons were 170% more likely to make an error w/o at least 6 hr of sleep
•Mental health and sleep are related-particularly in adolescents
•Association between amount of sleep and lifespan
•Heart disease, cancer, dementia, obesity, diabetes all worsen with decreased sleep
•One study concluded than <6 hours of sleep = 4-5x more likely to have an MI
•Sleeping less than 6 hours (instead of 7-8) doubled the risk of MI/CVA
•Sleeping improves BP (take BP meds before sleep for better outcomes)
•Sleep stabilizes mood and reactions
•Even 20 minutes of sleep loss causes trouble
•Less emotional regulation when the end of sleep is interrupted- because the end is when you are literally processing feelings.
•More traffic accidents and disasters occur in early morning hours (3 Mile Island in Pennsylvania, Chernobyl)
•Inadequate sleep costs American business $411 billion/year and countless lost creative opportunities
Sleep deprivation is how many hours of sleep
less than 6 hours
Explain the role of the optic nerve in sleep
The optic nerve is located beneath the suprachiasmatic nucleus, which signals the pineal gland to produce melatonin which tells your brain, "it's dark".
Where does sleep begin in the brain
frontal lobe
•Sleep is active, starts in frontal lobes.
What portion of the brain blocks external stimuli from reaching the cortex of the brain during sleep?
Thalamus
The thalamus blocks external stimuli form reaching the cortex.
Thalamus function in sleep
blocks external stimuli
What factors impede sleep?
Temperature
Loud sounds
Light
Pain
Stress
Shift work
brain stem role in sleep
when asleep, the brain stem starts a cycle of awake with many other structures including prefrontal cortex and hippocampus
Role of melatonin in sleep
hormone that serves as a time cue, that it is dark and time to sleep
How to do the stages of sleep progress?
As slow waves from the front to the back of the brain
Stages 1-4 progress as slow waves synchronously move from the front of the brain to back, broken by sleep spindles
What portions of the brain begin the "wake cycle"
brainstem, prefrontal cortex, hippocampus
function of hippocampus
memory
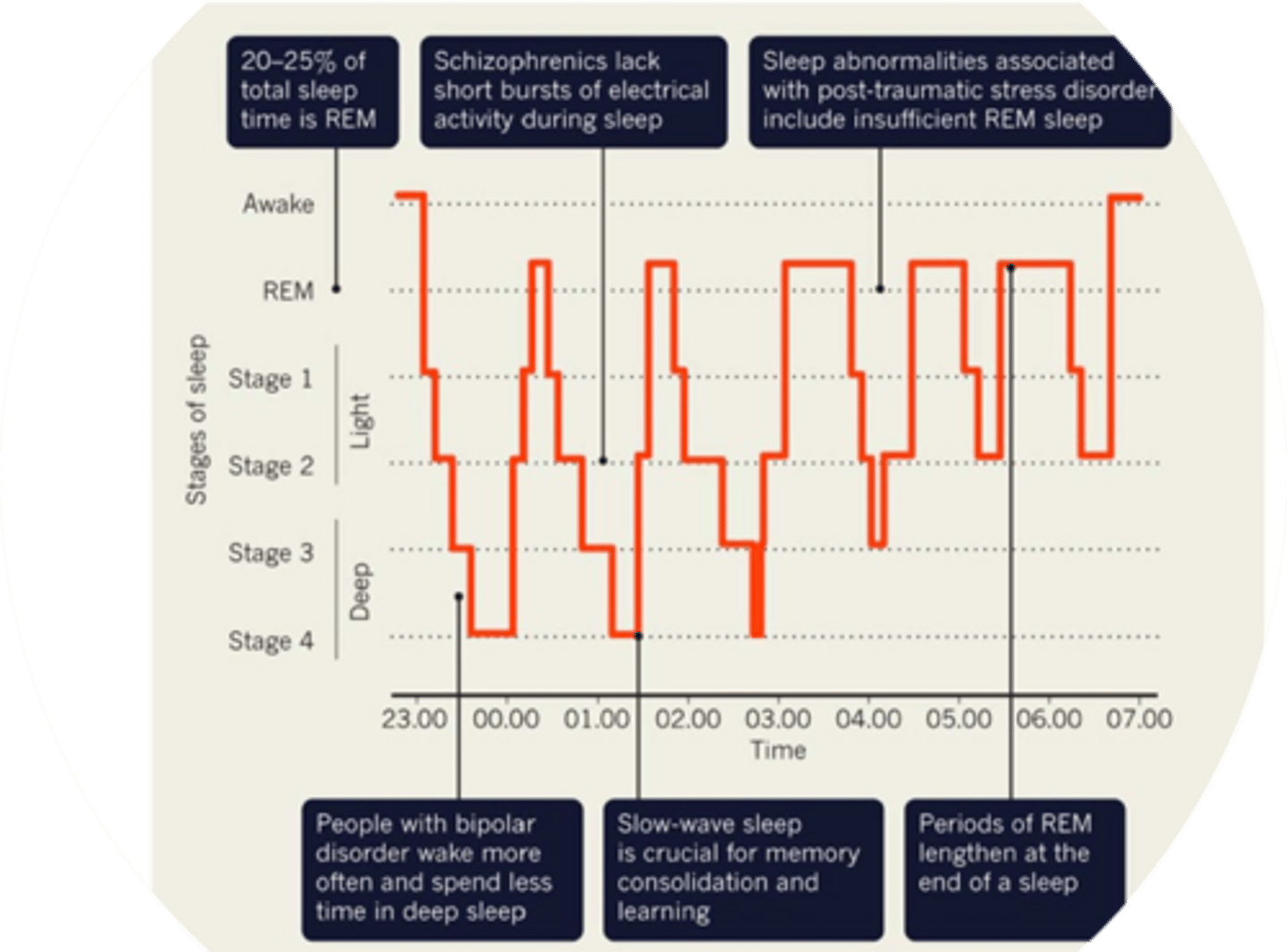
How much of sleep is REM?
20-25%
What mental health disorder is associated with insufficient REM sleep
PTSD
What mental health disorder is associated disruptive and less deep sleep
Bipolar disorder
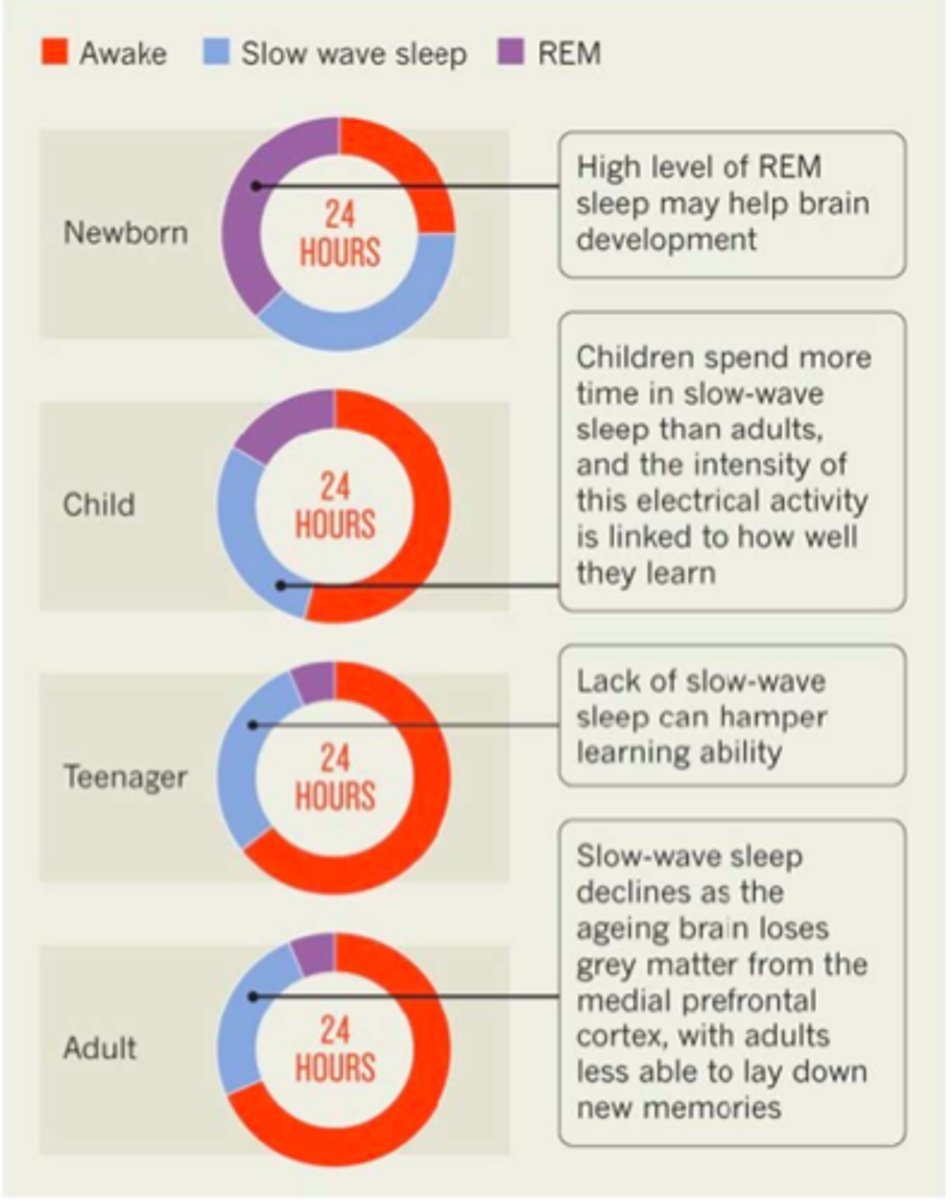
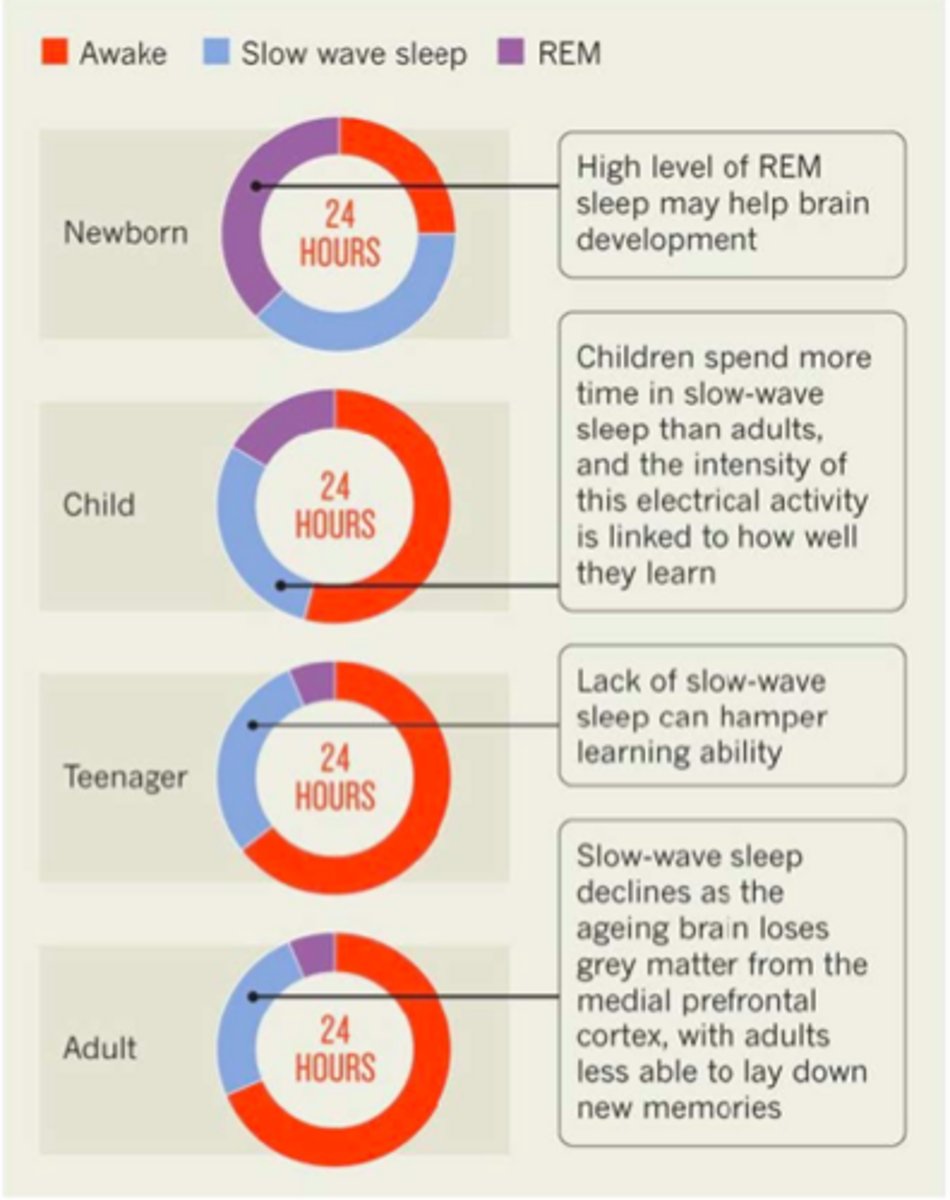
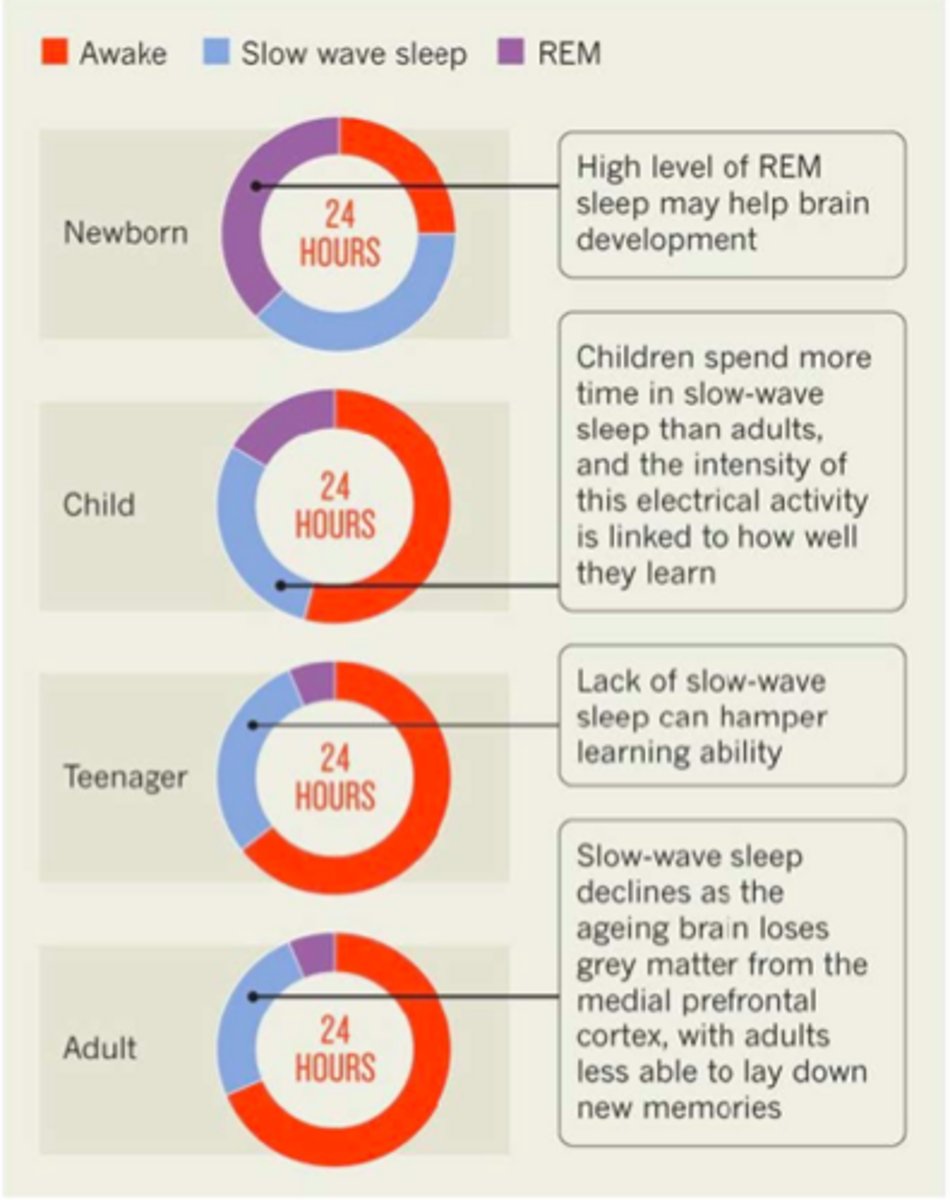
levels of REM sleep comparison: NB, child, teenager, adult
"Slow-wave" sleep is necessary for...
memory consolidation and learning
lack of slow wave sleep can hamper learning ability
When do the periods of REM sleep lengthen
at the end of sleep
High levels of REM sleep helps...
brain development & activity (e.g. in newborns)
What portions of the brain process sensation
sensory cortex & amygdala
sensations come in and are processed in the sensory cortex with amygdala (emotional) influence, then move to the prefrontal cortex for working memory and hippocampus for short term storage
From the hippocampus, memories are encoded and sent back to?
From the hippocampus, memories are encoded and sent back to the cortex for long term storage in declarative memory
Where are memories about movement, actions or step-by-step processes stored
basal ganglia & cerebellum
Memories about movement, actions or step-by-step processes, called procedural memories, are stored in the basal ganglia and cerebellum
Slow wave (non-REM) sleep promotes
Slow waves (non REM) sleep promotes cerebral recovery and improves cognitive functioning
Sleep consolidates
memories!
How do we get from sleep to success?
Think of sleep as a car wash for your brain and body, like a computer defragmenting
Immune system is hard at work
Memories are consolidated (made) and cells are repaired- especially during REM. REM is also when we prune connections and regulate emotions.
7 major categories of sleep disorders
1. insomnia
2. sleep-related breathing disorders
3. central disorders of hypersomnolence
4. circadian rhythm sleep-wake disorders
5.parasomnias
6. sleep-related movement disorders
7. other sleep disorders
Insomnia
recurrent difficulty falling and staying asleep despite adequate opportunity
Sleep-related breathing disorders
respiratory abnormalities that occur during rest
Central Disorders of Hypersomnolence
daytime sleepiness not caused by disturbed sleep or misaligned circadian rhythm
Circadian rhythm sleep-wake disorders
misalignment between the endogenous circadian clock and external environment leading to sleep-wake disruptions and symptoms of insomnia or sleepiness, shift work disorder
Parasomnias
involuntary physical events and experiences occurring when falling asleeping, during sleep, or waking up
Parasomnia may lead to
injuries, adverse health effects, psychosocial effects, hypersomnia
Sleep-related movement disorders
simple movements that disturb sleep or sleep onset
HPI for sleep (long just general concept)
Listen for vague terms/complaints: sleepiness, fatigue, lack of energy, tired, lethargy, moodiness, and difficulty concentrating, sleepiness in ADLS, trouble staying awake, performance, problems driving, including near-miss accidents, sxs of obstructive sleep apnea (OSA): loud snoring alternating with quiet episodes of pauses in breathing, dry mouth, nasal congestion, nocturnal enuresis, morning headaches- may need to ask sleep partner, sleeping patterns and sleepiness: time of sleep onset and offset, sleep latency, variability on the weekends, total sleep time (including naps), chronic pain, use of hypnotics to fall asleep or stimulants to stay awake, and daytime energy
meds to consider in H&P with sleep disorders
benzodiazepines, opioids, barbiturates, anticonvulsants, antihistamines, neuroleptics, dopamine agonists, and antidepressants.
What family hx should be considered for sleep disorders
narcolepsy
obstructive sleep apnea
restless leg syndrome
periodic leg movement disorder
major depressive disorder
bipolar disorder
PE sleep
Likely unremarkable unless another cause of sleep concerns
What are the diagnostic tests for suspected sleep disorders?
Sleep logs
Actigraphy: monitor rest & activity
Polysomnography: study brain wave, breathing, HR, O2 and leg movement during sleep
multiple sleep latency test
performance eval for sleep
psychomotor vigilance test (PVT)
Oxford sleep resistance (OSLER) test
Psychomotor Vigilance Test (PVT)
Measures reaction time and alertness
-assess behavioral consequences of excessive daytime sleepiness
Oxford Sleep Resistance (OSLER)
assess vigilance and the ability to stay awake
additional factors to consider in H&P
hypothyroidism, anemia, narcolepsy type 1, or restless legs syndrome, urine toxicology, electroencephalogram (seizure), neuroimaging rarely needed
Questionnaires to detect Sleep Disorders
Epworth Sleepiness Scale (ESS)
Stanford Sleepiness Scale (SSS)
Karolinska Sleepiness Scale (KSS)
Pittsburgh Sleep Quality Index
Ullanlinna Narcolepsy Scale or Swiss Narcolepsy Scale
Epworth Sleepiness Scale (ESS)
•8 scenarios are considered for likelihood of falling asleep (sitting and reading)
•score ranges from 0 (awake) to 24 (sleepy)
What score on the ESS warrants further evaluation of sleep disorder?
10 or more
The stanford sleepiness scale (SSS) assesses
current state of sleepiness
Karolinska Sleepiness Scale (KSS) assesses
the current state of sleepiness
What two questionnaires assess the current state of sleepiness
Stanford Sleepiness Scale (SSS) and Karolinska Sleepiness Scale (KSS)
Pittsburgh Sleep Quality Index is a...
19 item self-report measure of sleep quality from the previous month, score range 0-21
Sleep Hygiene Index (to read, questions asked with ranking: Always (5), Frequently (4), Sometimes (3), Rarely (2), Never (1))
1. I take daytime naps lasting two or more hours.
2. I go to bed at different times from day to day.
3. I get out of bed at different times from day to day.
4. I exercise to the point of sweating within 1 h of going to bed.
5 .I stay in bed longer than I should two or three times a week.
6. I use alcohol, tobacco, or caffeine within 4 h of going to bed or after going to bed.
7. I do something that may wake me up before bedtime (for example: play video games, use the internet, or clean).
8. I go to bed feeling stressed, angry, upset, or nervous.
9. I use my bed for things other than sleeping or sex (for example: watch television, read, eat, or study).
10. I sleep on an uncomfortable bed (for example: poor mattress or pillow, too much or not enough blankets).
11. I sleep in an uncomfortable bedroom (for example: too bright, too stuffy, too hot, too cold, or too noisy).
12. I do important work before bedtime (for example: pay bills, schedule, or study).
13. I think, plan, or worry when I am in bed.
Sleep well: How to get better sleep quality and duration
•Cold, dark and quiet room
•Protect enough time
•No phones! (remember the suprachiasmatic nucleus)
•Little caffeine
•No meds or ETOH
•A nap before 3 if you must
•Still can't sleep? Find a sleep (CBT) therapist
True of False: People who take sleeping pills (Ambien and Temazepam) are more likely to die
true

What defines insomnia
difficulty falling or staying asleep:
1. >30 min to fall asleep
2. Awake for 30 minutes after falling asleep (cant go back to sleep)
3. Sleep efficiency <85%
4. Less than 6.5 hours of sleep
*most common sleep disorder*
First line tx for insomnia
sleep hygiene
What is the most effective treatment for insomnia
Cognitive Behavioral Therapy
Are meds recommended for insomnia
NO, last line. Only used if all else does not work
•Sleep hygiene is first line
•Sleep CBT is most effective (CBT-I)
•Can supplement with meds (benzo, hyponotics, anticholinergics) but not best options
•Non-prescription and herbal supplements not recommended
All tx regimens for insomnia
1. Sleep Hygiene
2. Treat underlying condition
3. CBT for sleep
4. Relaxation therapy, acupuncture, music relaxation
If all of the above have been tried seriously some meds with serious side effects can be tried...
If all of the above have been tried seriously some meds with serious side effects can be tried...
•short-intermediate acting benzodiazepines like temazepam, estazolam, or lorazepam
•nonbenzodiazepine hypnotic sedatives: zolpidem, eszopiclone, zaleplon
•melatonin receptor agonist: ramelteon
•sedating antidepressants (better choice if the patient also has depression and/or anxiety; trazodone, amitriptyline, doxepin, or mirtazapine)
•combination of hypnotic sedative plus sedating antidepressant
•Does the patient have epilepsy or a psychotic disorder? anticonvulsants (gabapentin, tiagabine), antipsychotics (quetiapine, olanzapine)
•Don't use antihistamines or OTC sleep aids (pain reliever+ sleep aid)
•Valerian and melatonin not recommended
Sleep Disturbances with Psychiatric Dx
•Schizophrenia, sleep architecture and clozapine (risk of agranulocytosis vs benefit)
•ADHD-stimulant meds often used, co-occurring anxiety must be treated
•Mania, Anxiety, PTSD (bipolar)- treat underlying condition first
•Anxiety can cause sleep disorders and sleep deprivation can cause anxiety disorders
•Sleep disorders can cause and exacerbate mood disorders
•Mood disorders can exacerbate sleep problems.
•Sleep problems can lead to sleep anxiety
•Anxiety= can't fall asleep vs depression= can't stay asleep (early AM)? Evidence?
What is shift work disorder
Insomnia or excessive sleepiness associated with a "nontraditional" work schedule.
Increased rates of cancer in one study!
Diagnostic workup for shift work disorder
Sleep log for +2 weeks
Actinography (measures sleep activity)
Tx for Shift Work Disorder
- Encourage sleep hygiene
- 3 mg of melatonin
- Stimulant and sedative combinations timed correctly
- Overlap workday and day off sleep
- Bright light before activities and avoid light before bed
Obstructive Sleep Apnea (OSA)
repetitive pharyngeal collapse during sleep, which leads to absence of breathing, hypoxemia, & recurrent arousal
Apnea
cessation of breathing >10 seconds
Hypopnea
partial airflow obstruction causing shallow breathing & frequent arousal
Apnea-hypopnea index
Apnea-hypopnea index is the number of apneas and/or hypopneas/ hour of sleep as measured by polysomnography study or a home sleep apnea study.
issues with OSA
Alterations in intrathoracic pressure cause sympathetic nervous activation and systemic and pulmonary arterial hypertension
chronic and sustained systemic and pulmonary HTN, arrhythmias, and associated complications.
Signs and symptoms of OSA
Snoring
Breathing pauses
Restless/ nonrefreshing sleep
Awakening caused by gasping
Insomnia
Daytime sleepiness
Risk factors for OSA
Large neck circumference
Family History
Older age
Race
Craniofacial abnormalities
Obesity
Smoking
Alcohol
What is the "gold standard" assessment for OSA
Polysomnography (PSG)
How to confirm diagnosis of OSA
Diagnosis confirmed if number of obstructive events (apnea, hypopnea, or respiratory event-related arousal) on PSG is ≥ 5 events/hour.
Modified Mallampati Score
assesses anatomy of the oral cavity for likelihood of apnea
What is examined in Modified Mallampati
Looking for low visibility of the posterior pharynx when patient opens mouth
List some examples of findings on Modified Mallampati that would increase risk of apnea
retrognathia or increased overjet (top incisor teeth ahead of bottom incisors)
lateral peritonsillar narrowing
macroglossia
tonsillar hypertrophy
elongated or enlarged uvula
high-arched or narrow hard palate
nasal abnormalities (polyps, deviation of septum, turbinate hypertrophy)
Mild OSA for RDI
mild for respiratory disturbance index (RDI) ≥ 5 events/hour and < 15 events/hour
Moderate OSA for RDI
moderate for RDI ≥ 15 events/hour and < 30 events/hour
Severe OSA for RDI
severe for RDI ≥ 30 events/hour
How to manage OSA
Weight reduction in overweight patients
CPAP
Oral Appliances (for mild to moderate that dont like CPAP or arent candidates for it)
Medications: only given to improve daytime sleepiness
What is the treatment of choice for OSA
CPAP!
for moderate-to-severe improve quality of life, reduce excessive daytime sleepiness, and decrease MVAs
What should be repeated in pts w/ OSA
polysomnography
Why give patients with OSA oral appliances than CPAP
Not all patients are candidates for CPAP
Patient preference
Unresponsive to CPAP
mandibular advancement devices (MAD) and tongue retaining devices
what meds may improve OSA sx
Medications (modafinil/Provigil) may improve daytime sleepiness
may be used in conjunction with CPAP or MAD therapy in selected cases, not as sole therapy for OSA
surgical procedures for OSA
possible, but efficacy is controversial
Restless Leg Syndrome (RLS)
definitions and causes
Uncontrollable urge to move legs, specifically at night
Can be idiopathic of secondary to neuropathy, iron deficiency, chronic renal insufficiency, pregnancy
Can interrupt sleep
Suggested treatments of RLS
Exercise
Avoid caffeine, nic, alc
Avoid every med ever (antihistamines, theophyllines, lithium, beta blockers, anti-psychs & convulsants)
labs for RLS
Check ferritin, B12, folate, thyroid
How to treat moderate to severe RLS
Alpha-2-delta ligands: gabapentin, enacarbil, and pregabalin first-line treatment.
Dopamine agonists can also be considered as first-line. **some ADRs: paradoxical increase in RLS symptom severity following initial symptom reduction, loss of impulse control, and drowsiness.
Difference between RLS and Periodic Limb Movement Disorder (PLMD)
•PLMD= Movement of feet or legs (sometimes arms) during sleep, unknown to the patient, but can wake them, disrupting sleep
•Not the same as RLS, but can co-occur
•RLS happens while the person is awake and is a crawling or tingling sensation that forces the person to move to relieve it
•Can happen minimally or up to 15 times an hour
•Can be secondary to a variety of causes like iron deficiency
What pharm tx ay help PLMD
•Add iron, improve sleep hygiene, avoid alcohol and caffeine
•Melatonin, gabapentin, bezos, dopamine agonists, GABA agonists, clonazapam
Narcolepsy
Excessive sleepiness, disturbed sleep, sleep paralysis, sleep hallucinations (not the same as dreaming) upon falling asleep and waking up.
type 1 narcolepsy
(+) cataplexy and low CSF of hypocretin
What is hypocretin
hormone made by the hypothalamus that helps regulate sleep
what is cataplexy
sudden onset of muscle weakness usually caused by intense emotional episodes
pathognomonic for narcopelspy
Type 2 Narcolepsy
(-) cataplexy, normal CSF levels of hypocretin
How to treat narcolepsy
modafinil (provigil)
Sleep hygiene, huge variety of other meds, symptoms management, specialist referral.
What are the types of parasomnia
nightmares
sleep terrors - autonomic arousal
sleep walking - arousal problem like sleep terrors
enuresis (incontinence during sleep, mostly children)
Summary
•Pay more respect to sleep as a medical risk and treatment.
•Sleep is as important as diet and probably more important than exercise in personal choices
•CBT for SLEEP is #1!
•It influences all aspects of health including our #1 cause of death (cardio, obesity, glucose regulation, behavioral med, and dementia
•Ask patients about sleep and treat thoroughly
•Sleep meds are garbage. Melatonin is too.
•Order sleep studies liberally- can be done at home
•Prioritize your own high-quality sleep.
•Respect the sleep of hospitalized patients.