INTRAORAL DIAGNOSIS
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
developmental lesions
cleft palate
hairy tongue
ankyloglossia
varix or varicosity
torus or exostosis
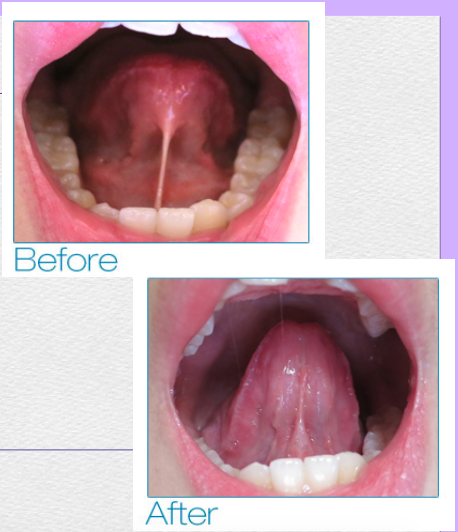
ankyloglossia
aka: tongue-tie
a condition in which the lingual frenum is attached too far anteriorly toward the tip of the tongue
prevents the tip of the tongue from reaching the hard palate when the mouth is open
effects:
aberration in speech
depending on the severity of the condition
management:
surgical correction when causes speech, swallowing, or other functional problems
hairy tongue
a condition in which the filiform papillae become markedly long, resulting in an appearance like a long-tufted carpet
causes of discoloration
the long filiform papillae may trap chromogenic bacteria, fungi, and food pigmentations
this can give the tongue various colors: white, brown, or black
management:
brushing the tongue with a toothbrush or using a tongue scraper will usually eliminate the discoloration

various colors of hairy tongue
white, brown, black
appearance of hairy tongue
long-tufted carpet
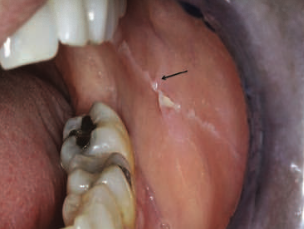
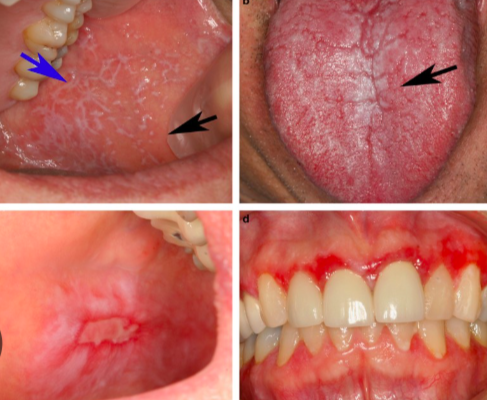
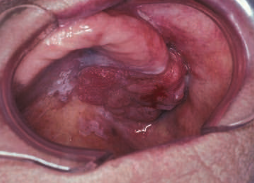
varix / varicosity
refers to dilation of a vein
treatment (TX)
no treatment is required
clinician must be able to differentiate this from other vascular or pigmented lesions found in the oral cavity

clinical appearance of varicosity
blanch with pressure
purple or blue papules
nodules or tortuous dilated veins
common locations of varicosity
lower lip in older adults
ventral surface of the tongue
torus or exostosis
an exostosis that occurs in one of two locations intra-orally
benign protuberances of bone that may arise on the cortical surface of the jaws
treatment:
surgical removal may be required if removable prostheses are planned
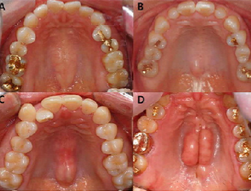
clinical appearance of exostosis
can be solitary or multiple
nodular masses on the buccal alveolar process
sometimes become confluent, forming a shelflike protuberance
torus mandibularis
may be unilateral or bilateral
appears on the lingual surface of the mandible near the canines and premolars
cleft palate
can occur with or without cleft lip

traumatic and reactive lesions
fibroma
linea alba
mucocele
hematoma
hyperkeratosis
amalgam tattoo
traumatic ulcers
nicotine stomatitis
pyogenic granuloma
chewing / biting of mucosa
chewing or biting of mucosa
lesions caused by chronic chewing of the mucosa
usually habit or stress induced, occur in children or adults
clinical considerations
problematic for CD patients
causes problems in vertical dimension

linea alba
similar to reticular papilla (Striae of Wickham)
a linear thickening of the buccal mucosa (hyperkeratosis) that occurs along the occlusal plane
clinical consideration
biopsy may be warranted in the presence of persistent trauma or unresolving ulceration
clinical appearance of linea alba
scalloping shape, representing occlusal indentations
traumatic ulcers
usually heal in 1 or 2 weeks
a lesion characterized by focal loss of epithelium
result from a cut, abrasion, or irritation of the mucosa

clinical appearance of traumatic ulcers
vary in size and shape
red borders caused by inflammation
hyperkeratosis
used clinically to refer to white areas on oral mucosa without annotation as to the cause of the condition
a term referring to a microscopic layer of thickened parakeratin and/or orthokeratin of the mucosal epithelium
treatment:
these lesions must be monitored
biopsy may be appropriate if changes in lesion color, shape, borders, or surface texture are observed

most common cause of hyperkeratosis
chronic irritation or frictional keratosis
clinical appearance of hyperkeratosis
whitish appearance in the moist environment of the oral cavity because of the thickened keratin layer
amalgam tattoo
usually an incidental finding
amalgam in the gingiva, alveolar process, palate, or buccal mucosa may produce a tattoo
clinical consideration:
dental team must be able to conclusively differentiate an amalgam tattoo from other types of intraoral pigmented lesions

appearance of amalgam tattoo
dark blue or black discoloration
ranging in size from a few millimeters to 1cm
radiograph:
radiopaque granules consistent with metal fragments
nicotine stomatitis
occurs on the posterior hard palate and anterior soft palate of smokers, especially pipe smokers
cause:
caused by heat on the mucosa
not actually by the nicotine itself!
treatment:
encourage the patient to STOP SMOKING

clinical appearance of nicotine stomatitis
sakura-like
the whiteness represents hyperkeratosis and the red spots
papules with an opaque white surface and a red dot in the center
pyogenic granuloma
an example of a tumescence
can occur anywhere in the oral mucosa or on the skin
an overgrowth of young, highly vascular granulation tissue
cause:
reaction to chronic irritation or dental plaque
pregnancy or puberty, hormonal changes may cause exaggerated tissue reactions
management:
dentist must identify and resolve the underlying cause (ex: iatrogenic restoration, foreign body, or dental infection)
[ note: misnomer – does not produce pus and is not a true granuloma ]
![<p>an example of a<span style="color: red;"> tumescence</span></p><p>can occur<span style="color: red;"> </span>anywhere in the oral mucosa or on the skin</p><p>an <span style="color: red;">overgrowth of young, highly vascular granulation tissue</span></p><ul><li><p><strong>cause:</strong></p><ul><li><p>reaction to <span style="color: red;">chronic irritation or dental plaque</span></p></li><li><p>pregnancy or puberty, <span style="color: red;">hormonal changes</span> may cause exaggerated tissue reactions</p></li></ul></li></ul><ul><li><p><strong>management:</strong></p><ul><li><p>dentist must identify and <span style="color: red;">resolve the underlying cause</span> (ex: iatrogenic restoration, foreign body, or dental infection)</p></li></ul></li></ul><p></p><p><em>[ note: misnomer – does not produce pus and is not a true granuloma ]</em></p>](https://knowt-user-attachments.s3.amazonaws.com/fed6eb79-6bce-4ec8-8545-36c714906264.png)
clinical appearance of pyogenic granuloma
lesion bleeds easily
bright red enlargement due to vascularity of granulation tissue and frequent loss of epithelium over the lesion
fibroma
refers to a reactive overgrowth of fibrous tissue and is not a true neoplasm
cause / history:
patients usually report a history of trauma in the area
in such cases, the term "traumatic fibroma" is widely used
management:
excisional biopsy should be considered if the lesion is unsightly, repeatedly traumatized, or habitually manipulated by the patient
excisional biopsy is more recommended than incisional biopsy

clinical appearance of fibroma
usually less than 1cm in dimension
well-circumscribed firm swelling on the lip or buccal mucosa
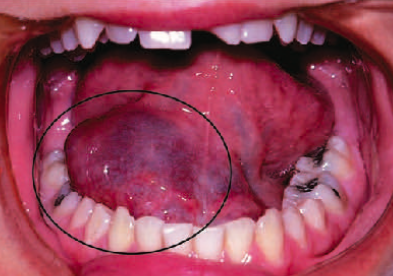
hematoma
consists of extravasated blood pooling under the epithelium or deep in the connective tissue or muscle, usually because of blunt trauma
cause:
usually due to blunt trauma
occurs more often in individuals with bleeding disorders
occasionally administration of an inferior alveolar nerve block
treatment:
can be expected to resolve spontaneously
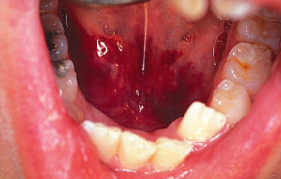
clinical appearance of hematoma
a dark red papule or nodule that ruptures easily
infections or inflammations
parulis
candidiasis
herpes infection
angular cheilitis
verruca vulgaris
patent sinus tract
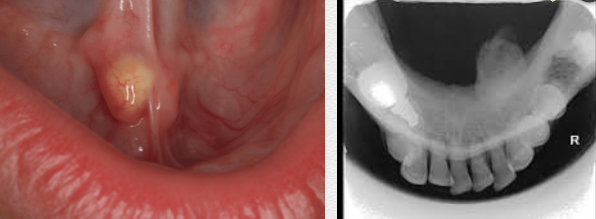
parulis
aka: gumboil
a small abscess on the gingiva, originating from an apical or periodontal abscess
treatment:
will resolve if the source of infection is eliminated

clinical appearance of parulis
localized and often acute swelling on the gingiva with fluctuation
a yellow point appears at the center of the swelling before spontaneous drainage
patent sinus tract
results in continuous drainage of pus through the formed sinus tract
can develop following drainage of a parulis if the source of infection (commonly a necrotic pulp) is not removed
treatment:
the papule may persist as a fibroma
the sinus tract will close when the source of infection is eliminated

appearance of patent sinus tract
this papule represents the opening of a fistula or sinus tract
asymptomatic papule of granulation tissue forms on the gingiva in response to chronic irritation from the drainage
herpes infection
generalized gingivitis may occur
primary infection is often subclinical
lesions usually resolve in 10-14 days without a trace
oral lesions are widespread with small vesicles forming anywhere on the lips and mucosa
triggers:
stress, strong sunlight exposure, or immune suppression
recurrent infection
recurring painful intraoral episodes may require antiviral medication
vesicles are short-lived; ulcers are discrete and typically smaller than 2mm
usually less severe; lesions occur only on keratinized tissue (perioral skin, gingiva, hard palate)

clinical appearance of herpes infection
vesicles coalesce and rupture
will then form widespread ulcers known as primary herpetic gingivostomatitis
pathophysiology of herpes infection
these viruses target epithelial cells, causing skin and mucosal lesions
after infecting epithelial cells → viruses replicate, enter neurons, and travel to nerve ganglia, where they remain latent until reactivated
upon reactivation, viruses travel back to skin or mucosa, causing lesions
[ both HSV-1 & HSV-2 → infect perioral skin and oral mucosa ]
subtle systemic symptoms of herpes infection
mild fever
pharyngitis
general malaise
treatment for herpes infection
acyclovir
types of herpes viruses that infect humans
varicella zoster virus (VZV)
herpes simplex virus type 1 (HSV-1)
herpes simplex virus type 2 (HSV-2)
candidiasis
an opportunistic infection of candida albicans
treatment:
antifungal agents with persistent candidiasis

clinical forms of candidiasis
erythematous
pseudomembranous
chronic hyperplastic candidiasis
candida-associated angular cheilitis
central papillary atrophy (median rhomboid glossitis)
denture stomatitis – often included, though may be a reactive lesion rather than true infection
predisposing factors of candidiasis
HIV/AIDS
birth control pills
cancer, aging, pregnancy
diabetes mellitus, smoking
hyposalivation, chemotherapy
extended course of antibiotics
systemic or inhaled corticosteroids
pathophysiology of candidiasis
most healthy individuals have candida-specific innate immunity
infection occurs when innate defense mechanisms are defective, candida alters its virulence, or environmental factors favor growth
candida organisms are commensal in:
human gastrointestinal (GI) tract
lower female reproductive tract
angular cheilitis
presents as an inflammation at the corner of the mouth
occurs mostly in aged individuals with deep labial folds after loss of occlusal height (decreased VDO)
habitual licking of the corner of the mouth may also lead to development even without deep labial folds
treatment:
topical antifungal agents

predisposing factors of angular cheilitis
deficiencies of vitamin B, iron or folic acid
causes of angular cheilitis
Candida albicans
Staphylococcus aureus
Beta-hemolytic streptococcus
habitual licking of the corner of the mouth may also lead to development even without deep labial folds
clinical appearance of angular cheilitis
deep labial folds become red, sore, and fissured due to constant saliva exposure
verruca vulgaris
latin for "common wart"
a benign epithelial lesion of the skin and mucous membrane
cause:
human papillomavirus (HPV) types 1, 2, 4
management:
similar to that for a fibroma
excisional biopsy

appearance of verruca vulgaris
a pedunculated or sessile papule with a whitish-pink cauliflower-like surface
can occur anywhere on the oral mucosa
autoimmune diseases
lichen planus
aphthous ulcers
atrophic glossitis
lichenoid reaction
aphthous ulcers
common oral mucosal disease
ulcerations with no known cause and a wide spectrum of severity and frequency of recurrence
triggers:
represent an autoimmune reaction
precipitated by stress or hormonal changes
associated with systemic conditions such as vitamin deficiencies, iron deficiency, and inflammatory bowel diseases.
treatment:
topical steroids for recurrent cases

appearance of aphthous ulcers
solitary or multiple nonspecific ulcers
usually on nonkeratinized oral mucosa
other names of aphthous ulcers
canker sores
aphthous stomatitis
recurrent aphthous ulcers
recurrent aphthous stomatitis
lichen planus
a chronic inflammatory skin disorder, can persist for months or years
believed to be a cell-mediated immune response, but exact cause is unknown
the oral component (OLP) may occur before, concurrent with, or after skin lesions
management
topical or short-term systemic steroids for erosive form

clinical appearance of lichen planus
plaque, erosion, or ulceration of the oral mucosa
pruritic, purple eruptions with white streaks (Wickham striae) on the surface
bandlike, subepithelial lymphocytic infiltration and basement membrane degeneration, cause is unknown
lichenoid reaction
an oral mucosal condition that is clinically and histologically indistinguishable from OLP except for identifiable causes
when the cause (such as amalgam or an offending medication) is removed the lesion will resolve with time
atrophic glossitis
refers to papillary atrophy of the tongue
characterized by an absence of filiform and fungiform papillae
treatment:
treatment varies depending on the underlying cause of the condition

associated conditions of atrophic glossitis
anemia
avitaminosis
sjögren syndrome
vitamin B deficiency
graft versus host disease
appearance of atrophic glossitis
fiery red, edematous, painful
hence the term "burning tongue”
cysts, tumors and neoplasms
leukoplakia
erythroplakia
squamous cell carcinoma
developmental odontogenic cysts
erythroleukoplakia (speckled erythroplakia)
developmental odontogenic cysts
a pathologic cavity lined with epithelium
contains fluid or semi-solid material in the lumen
arise from the epithelium of the tooth-forming apparatus
not inflammatory in nature, and thus are to be distinguished from periapical (radicular) cysts
types of developmental odontogenic cysts
dentigerous cysts
odontogenic keratocysts
lateral periodontal cysts
leukoplakia
derived from Greek, meaning "white patch"
a clinical diagnosis with no specific histologic implication
refers to a clinically evident white plaque or patch with malignant potential
considered a diagnosis of exclusion after ruling out other white lesions such as:
frictional keratosis
smoker's keratosis
hyperplastic candidiasis
treatment:
biopsy should be performed regardless of lesion location to rule out:
dysplasia (precancerous)
invasive cancer (malignancy)
carcinoma in situ (early malignancy)

erythroplakia
term used as a clinical diagnosis, not a histologic one, similar to oral leukoplakia
bright red, velvety plaques which cannot be characterized clinically or pathologically as being due to any other condition as per WHO (1978)
clinical significance
studies show that 90% of lesions clinically diagnosed as erythroplakia are either premalignant or malignant
treatment:
biopsies to confirm or rule out the presence of premalignancy or malignancy
erythroleukoplakia (speckled erythroplakia)
risk of premalignancy or malignancy is higher than for homogenous leukoplakia
a clinical diagnosis describing:
oral leukoplakia → a red component, or
oral erythroplakia → intermingled with white plaque
clinical studies show:
14% of lesions are invasive carcinoma
51% are epithelial dysplasia
treatment:
biopsy is essential
sample should include the red area for accurate diagnosis

squamous cell carcinoma
the most common oral malignancy
differentiating this from benign lesions with similar features can be challenging
clinical considerations:
early detection and treatment is the key for survival
oral healthcare providers are best qualified to examine oral tissues and identify suspicious lesion
any suspicious lesion, especially in patients with common risk factors, must be biopsied due to the morbidity and mortality associated with SCC

most common contributing factors of squamous cell carcinoma
tobacco and alcohol consumption
clinical appearance of squamous cell carcinoma
white or red plaque
ulceration, papule or nodule
lesion with mixed white and red components
common sites of squamous cell carcinoma
oropharynx
floor of the mouth
lateral border of the tongue
non-neoplastic salivary gland abnormalities
xerostomia
sialolithiasis
hyposalivation
sjogren syndrome
ranula & mucocele
mucocele
found on the lower lip
the common clinical term for mucous extravasation phenomenon
occurs when saliva is retained inside the duct, gland, or surrounding tissue spaces

extravasation phenomenon
the term used if saliva has escaped the duct
ranula
located in the floor of the mouth
essentially a type of mucocele in this specific location
a mucous extravasation phenomenon associated with the submandibular or sublingual glands
sialolithiasis
presence of salivary stones in the salivary glands
rarely in:
sublingual glands
less frequently in:
parotid gland
most commonly found in:
submandibular gland
hyposalivation
aka: hypoptyalism
defined as a diminished secretion of saliva
xerostomia
aka: dry mouth
dryness of the oral cavity due to reduced or absent saliva
causes:
primary → degenerative or autoimmune diseases affecting the salivary glands
secondary → conditions that inhibit salivary secretion, frequently as a side effect of:
medications
dehydration
hormonal imbalances
sialometry → used to measure salivary flow
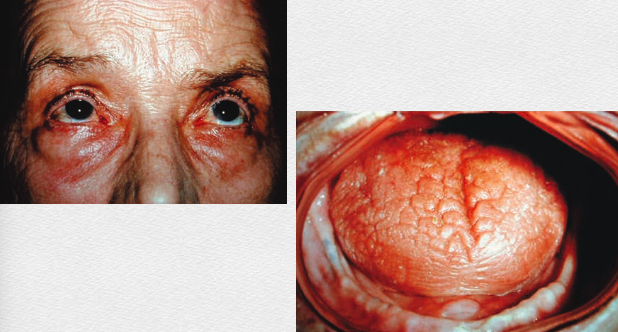
sjogren syndrome
an autoimmune disorder affecting exocrine glands
specifically the lacrimal and salivary glands, causing dry eyes and dry mouth
primary sjögren syndrome
may also involve vaginal or nasal dryness
can be associated with chronic bronchitis
secondary sjögren syndrome
associated with other autoimmune diseases, such as:
lupus
sarcoidosis
scleroderma
rheumatoid arthritis
neoplastic salivary gland abnormalities
pleomorphic adenoma
pleomorphic adenoma
referred as benign mixed tumor
presents initially as a dome shaped mass without ulceration or symptoms
