T5 - IE4 - Pulmonology - Ostrom - Pharmacology + Pathophysiology of Cystic Fibrosis
1/125
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
126 Terms
CFTR is only expressed in the ____________ membrane
- apical (membrane)
The side with the cilia that is facing the hydrophilic areas
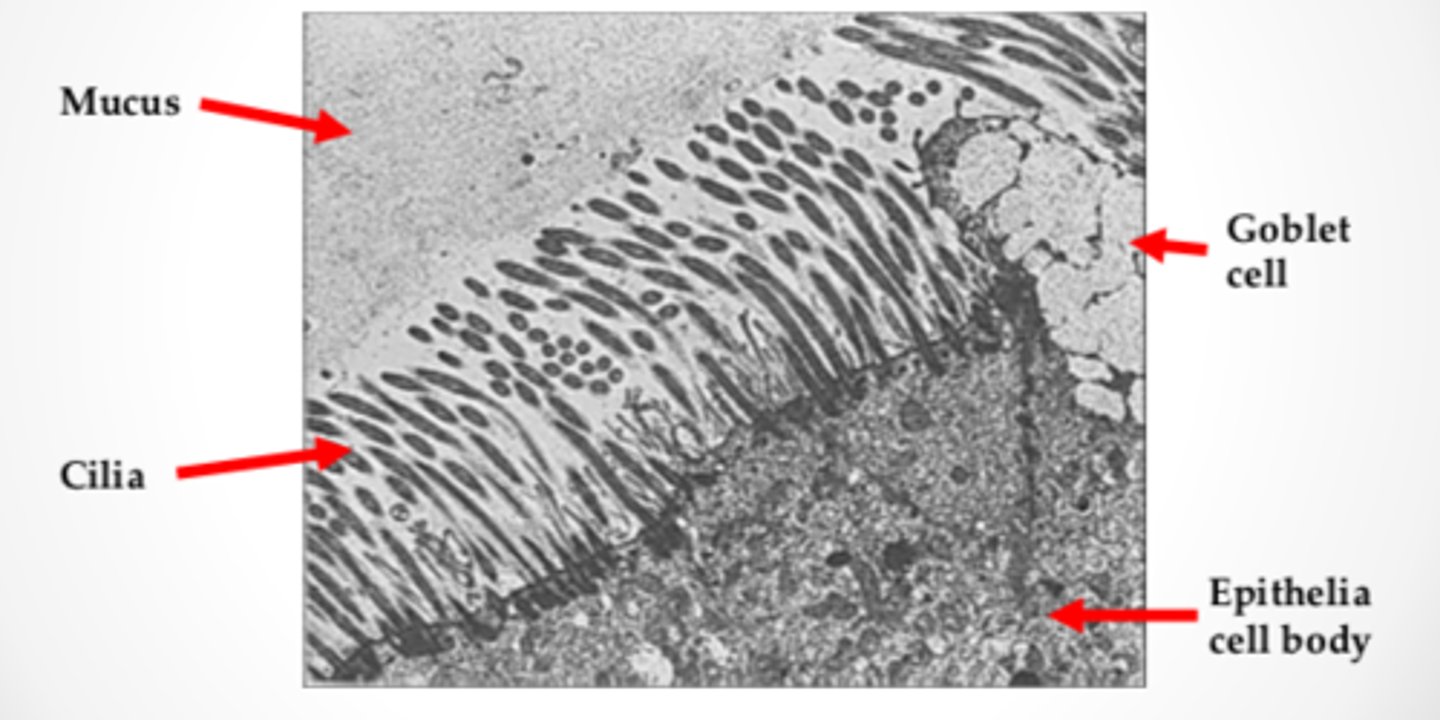
Mucociliary escalator: specialized cells produce the __________ ___________
- (produce the) mucus secretions
Mucociliary escalator: the mucus layer is like a __________ ____, moving the mucus and trapped particle up and out of the ___________
- conveyor belt
- (out of the) lung
Mucociliary escalator: the mucus layer is like a conveyor belt, moving the _______ and ________ _______ up and out of the lung
- mucus
- trapped particle (up and out of the lung)
Impairment of normal lung mucociliary function
mucus impairment
ciliary impairment
Impairment of normal lung mucociliary function - ciliary impairment: ____________ by toxic gases
- paralysis (by toxic gases)
Impairment of normal lung mucociliary function - ciliary impairment: bronchial epithelium ____________
- (epithelium) destroyed
Impairment of normal lung mucociliary function - ciliary impairment: ____________ defect of ciliary motion
- congenital (defect of ciliary motion)
Behavior of aerosols in the lung
deposition
clearance
absorption
Mechanisms of deposition of aerosol - where the aerosol lands depends on _______________ _______
- (depends on) particle size
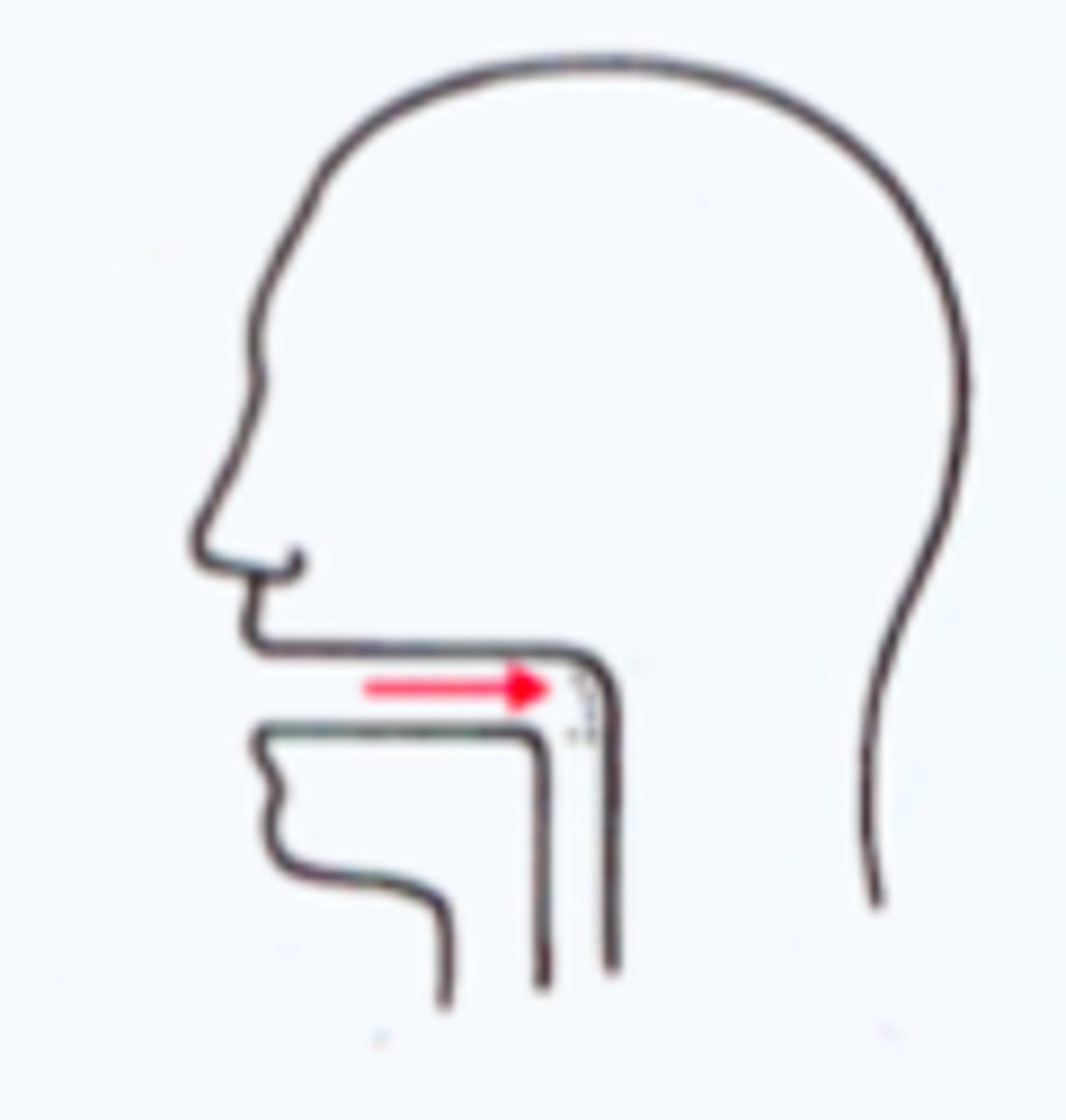
large particle sizes = nasopharynx
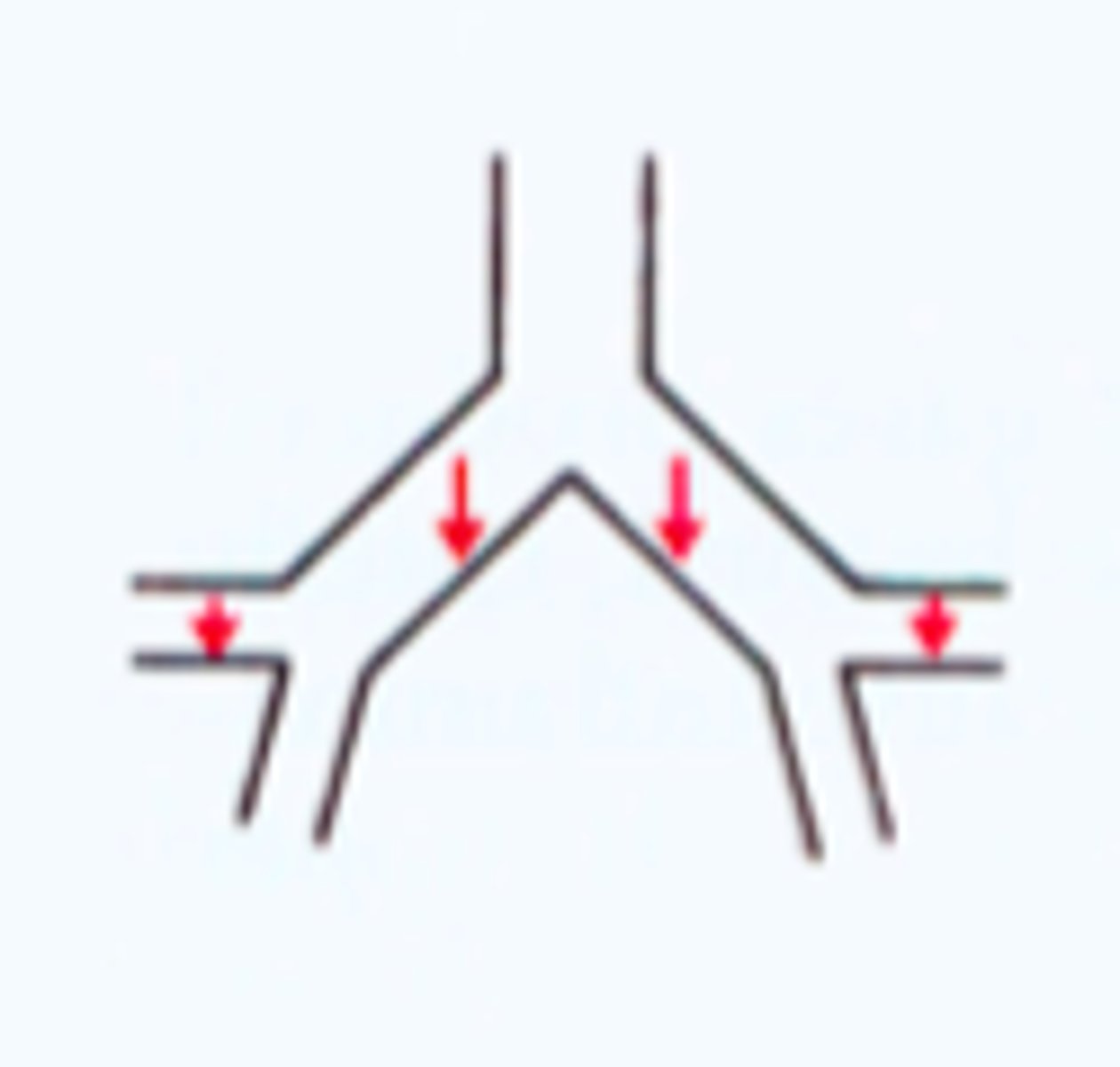
medium particle size = small airways
small particle size = alveoli
Mechanisms of deposition of aerosol figure
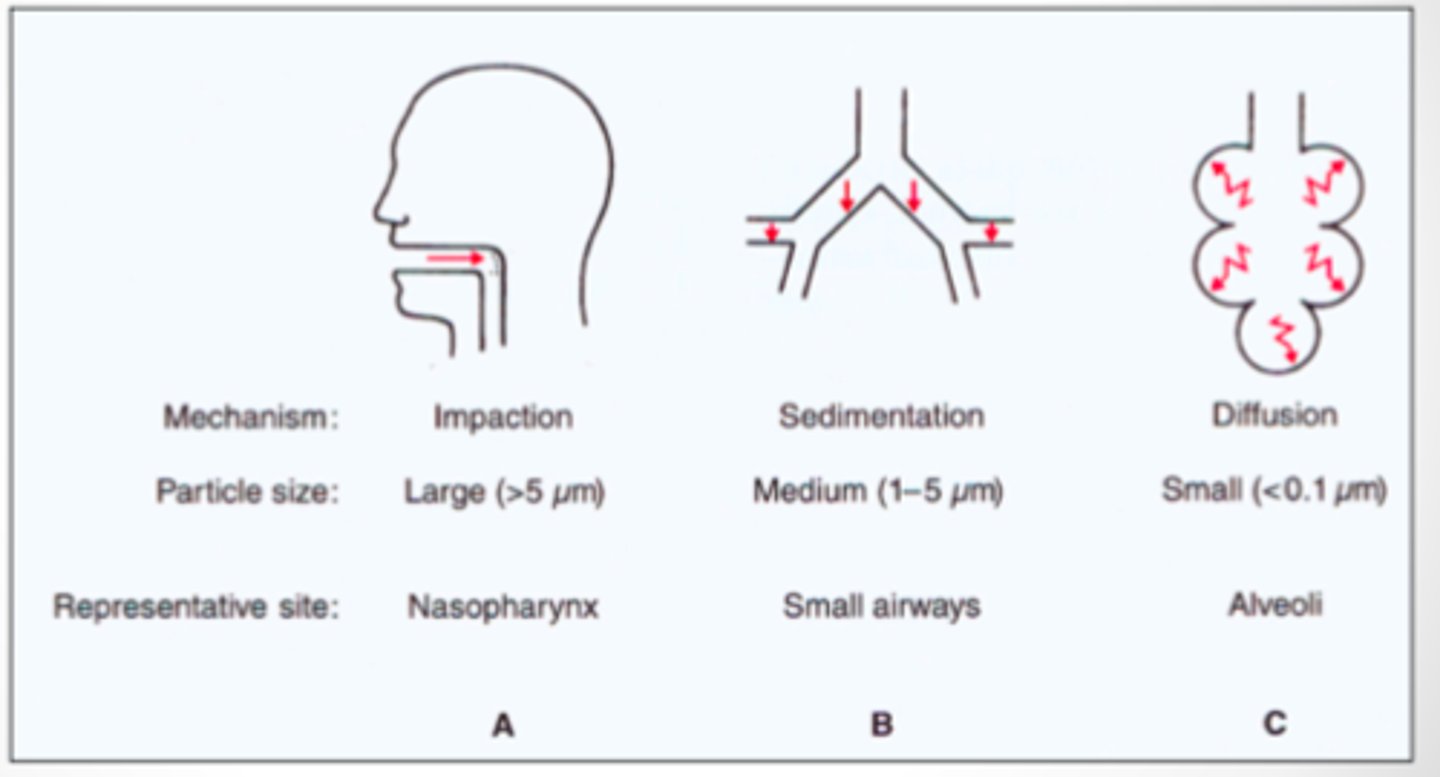
Mechanisms of deposition of aerosol: nasopharynx
impaction
Mechanisms of deposition of aerosol: small airways
sedimentation
Mechanisms of deposition of aerosol: alveoli
diffusion

Clearance of deposited particles: particles can be ________ up or _________ in the nasal passages, people can also _______ them
- coughed (up)
- trapped (in the nasal passages)
- swallow (them)
Most smaller particles get trapped in the mucus layer of the bronchi and cilia beat to clear the particles. If particles get into the alveoli there is no cilia so the particle must be phagocytksed by alveolar macrophages.
Clearance of deposited particles: most smaller particles get trapped in the __________ layer of the bronchi and cilia _______ to clear the particles. If particles get into the _________ there is no cilia so the particle must be ________________ by alveolar macrophages.
- mucus (layer of the bronchi)
- beat (to clear)
- (get into the) alveoli
- phagocytosed (by alveolar macrophages)
Clearance of deposited particles: most smaller particles get trapped in the mucus layer of the _________ and cilia beat to _______ the particles. If particles get into the alveoli there is no cilia so the particle must be phagocytosed by alveolar ________________
- (mucus layer of the) bronchi
- (beat to) clear
- (phagocytosed by alveolar) macrophages
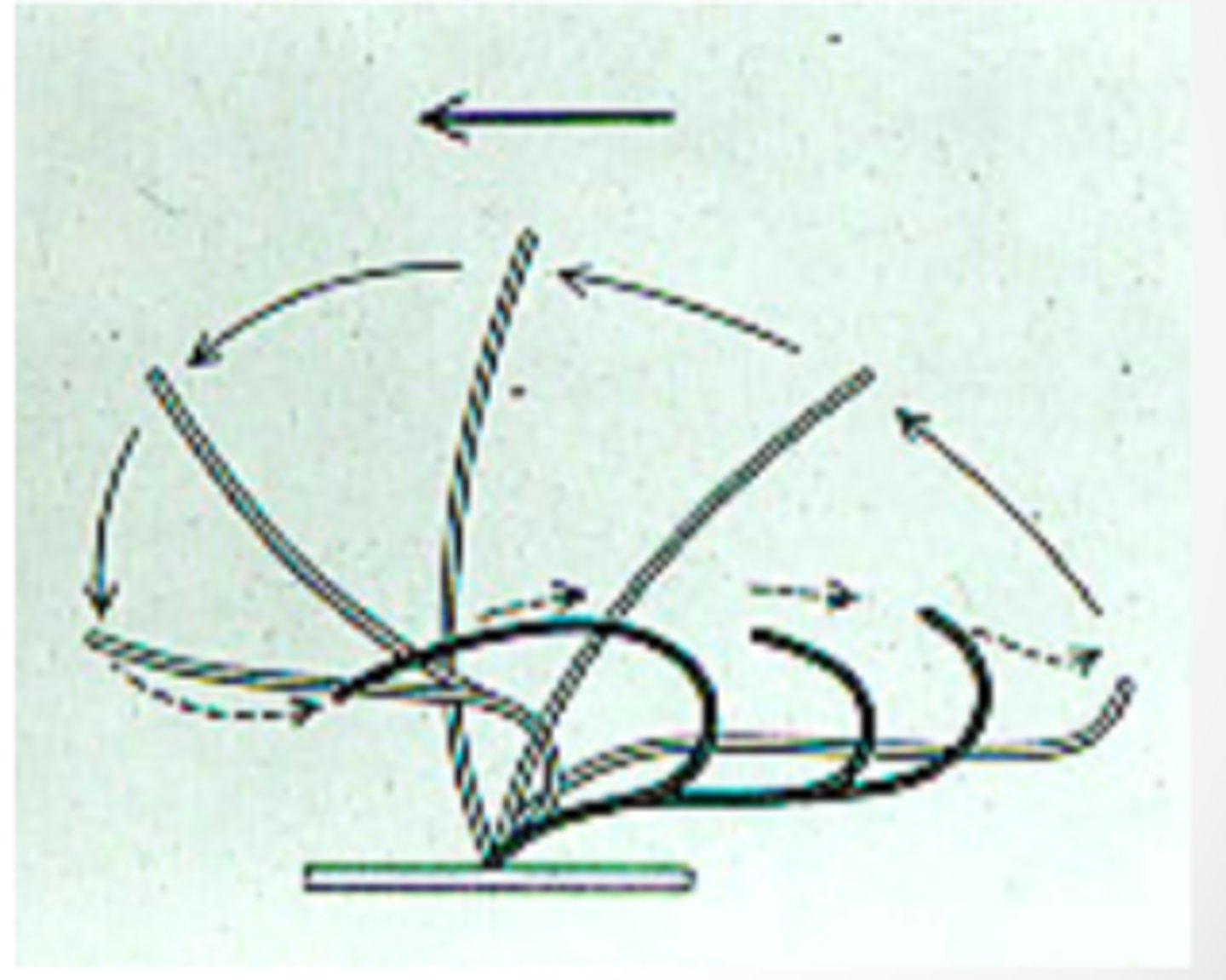
Mucociliary escalator: the mucus layer has a _____ layer (just mucus) and a ____ layer (mostly the cilia)
- gel (layer)
- sol (layer)
Gel layer is comprised of ____________
- (comprised of) mucus
Sol layer is mostly cilia
Sol layer is comprised of mostly ___________
- (mostly) cilia
Gel layer is comprised of mucus
Gel layer of the mucus above the sol layer figure
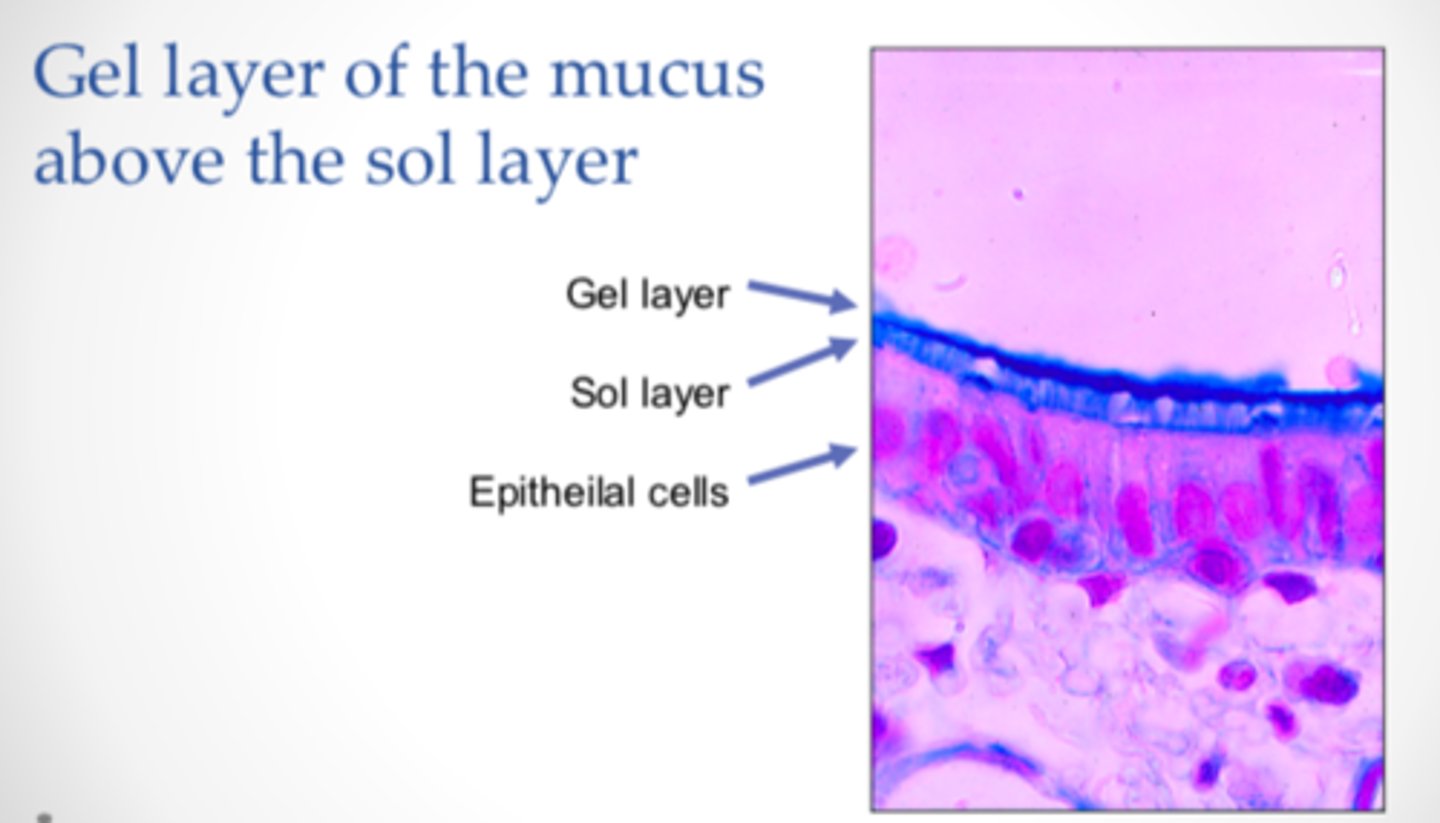
Cilia just touching the gel layer
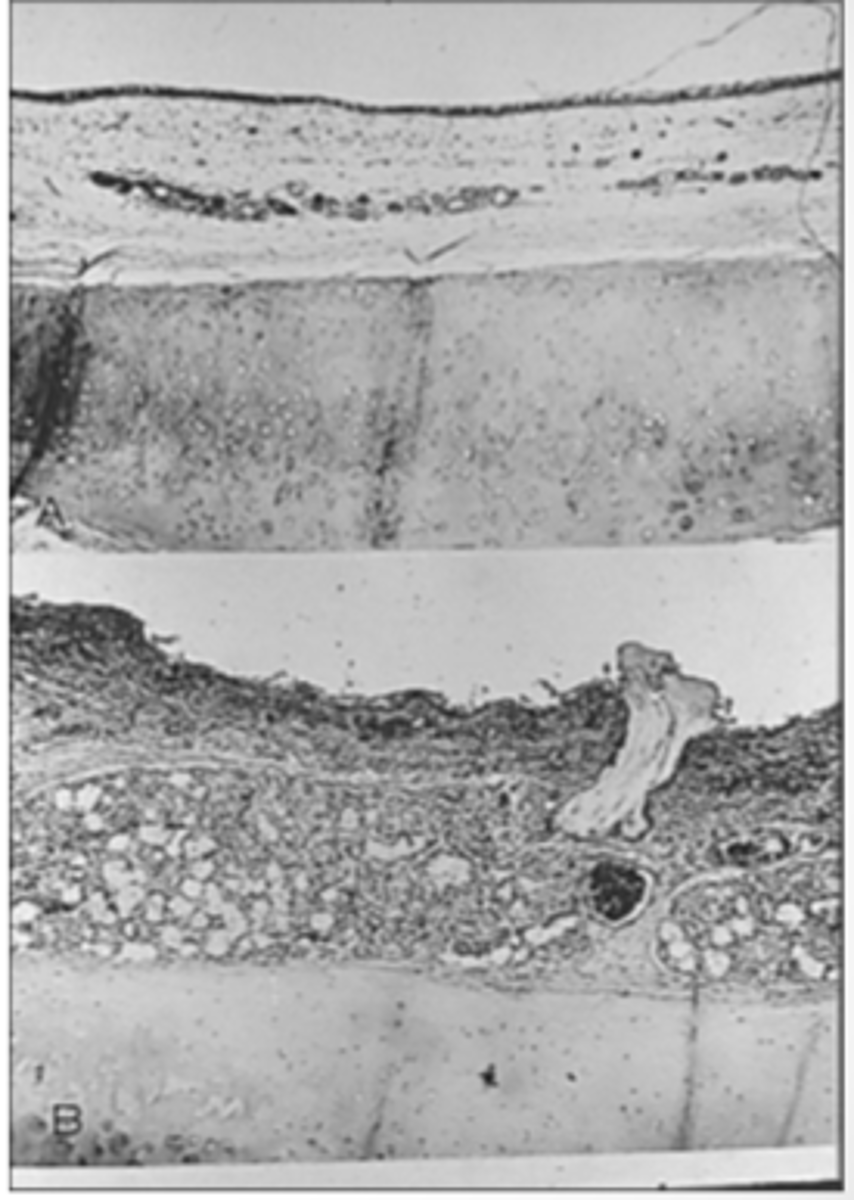
Normal airway vs. enlarged mucous glands: in various lung diseases caused by inhaling lots of particles or having chronic infections, the lung will show _____________ _____ and _________ of mucus glands
- increased size
- numbers (of mucus glands)
Normal airway vs enlarged mucous glands figure
Normal (top)
Enlarged (bottom)
Ciliary action: cilia are __-____ µm long and __ __ µm wide
- 1-10 (µm long)
- < 1 (µm wide)
Cilia beat via changes in intracellular calcium levels
Ciliary action: cilia beat via changes in ____________ __________ levels
- intracellular calcium (levels)
Mechanostimulation and high viscosity increases beat frequency
Ciliary action: ______________ and _____ ___________ increases beat frequency
- Mechanostimulation
- high viscosity
Impairment of normal lung mucociliary function - mucus impairment
too much, or change in composition e.g., chronic bronchitis, cystic fibrosis, asthma
Impairment of normal lung mucociliary function - ciliary impairment
paralysis by toxic gases
bronchial epithelium destroyed
congenital defect of ciliary motion
Alveolar macrophage function
phagocytosis of harmful particles
Impairment of normal lung macrophage function
inhaled gases
- ozone
- cigarette smoke
toxic particles
- silica
alveolar hypoxia, radiation, corticosteroids, and alcohol ingestion
Impairment of normal lung macrophage function: inhaled gases
ozone
cigarette smoke
Impairment of normal lung macrophage function: toxic particles
silica
Impairment of normal lung macrophage function: others
alveolar hypoxia
radiation
corticosteroids
alcohol ingestion
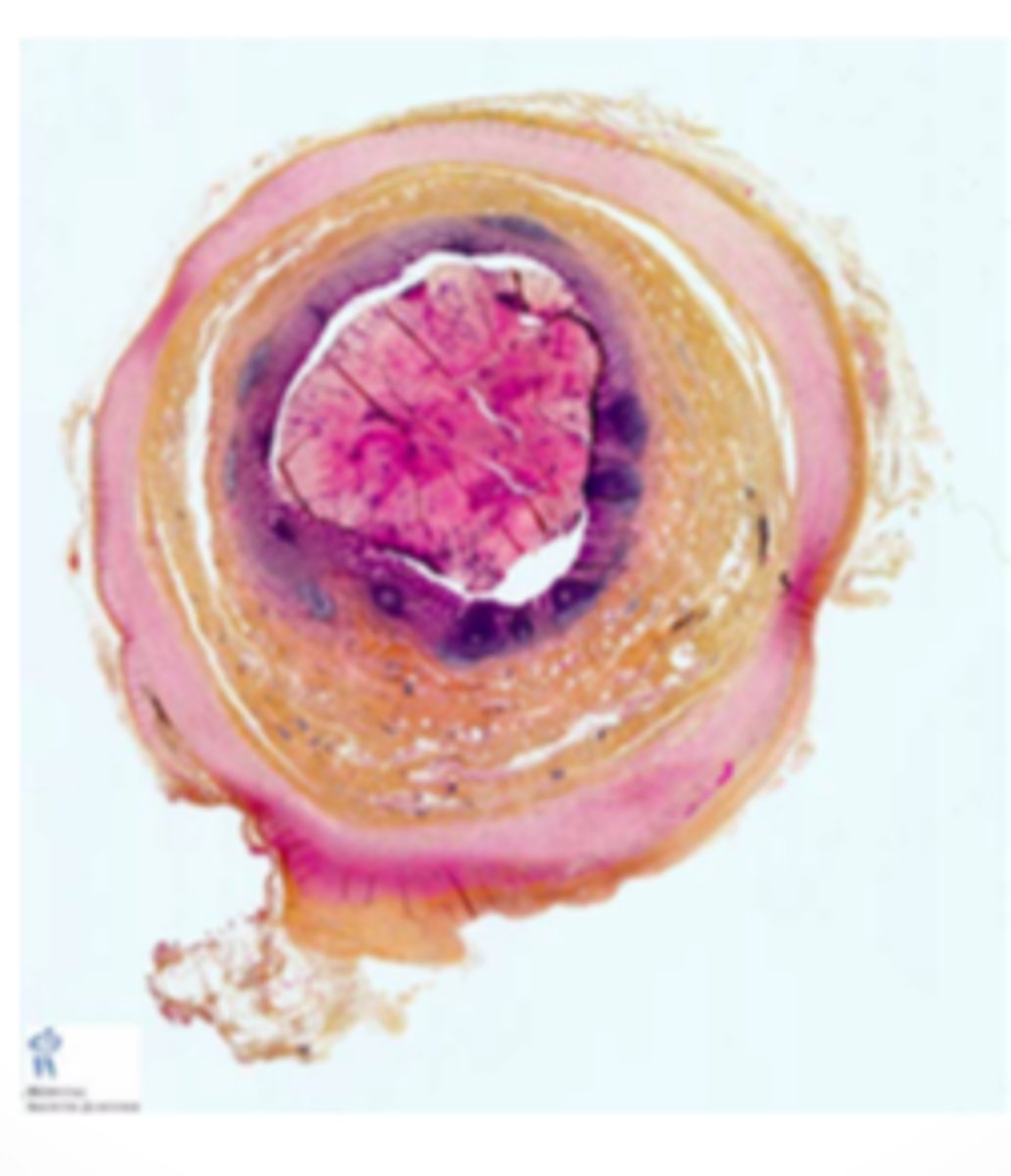
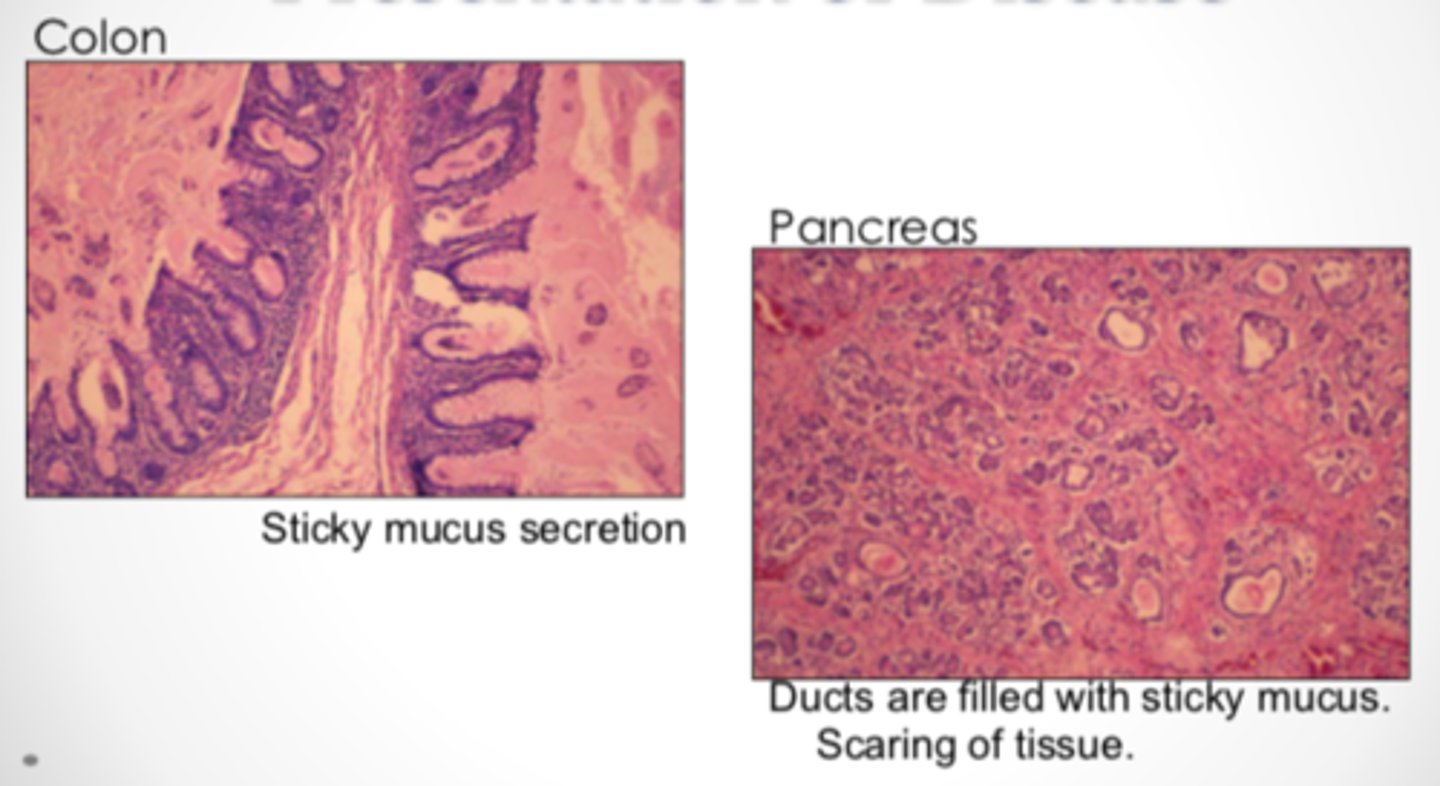
Cystic fibrosis histology
Clinical features of CF: ____________ _____________ _________ disorder
- heterogeneous recessive genetic (disorder)
Mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene
Clinical features of CF: ___________ in the cystic fibrosis transmembrane conductance regulator (CFTR) gene
- mutation (in the cystic fibrosis transmembrane conductance regulator [CFTR])
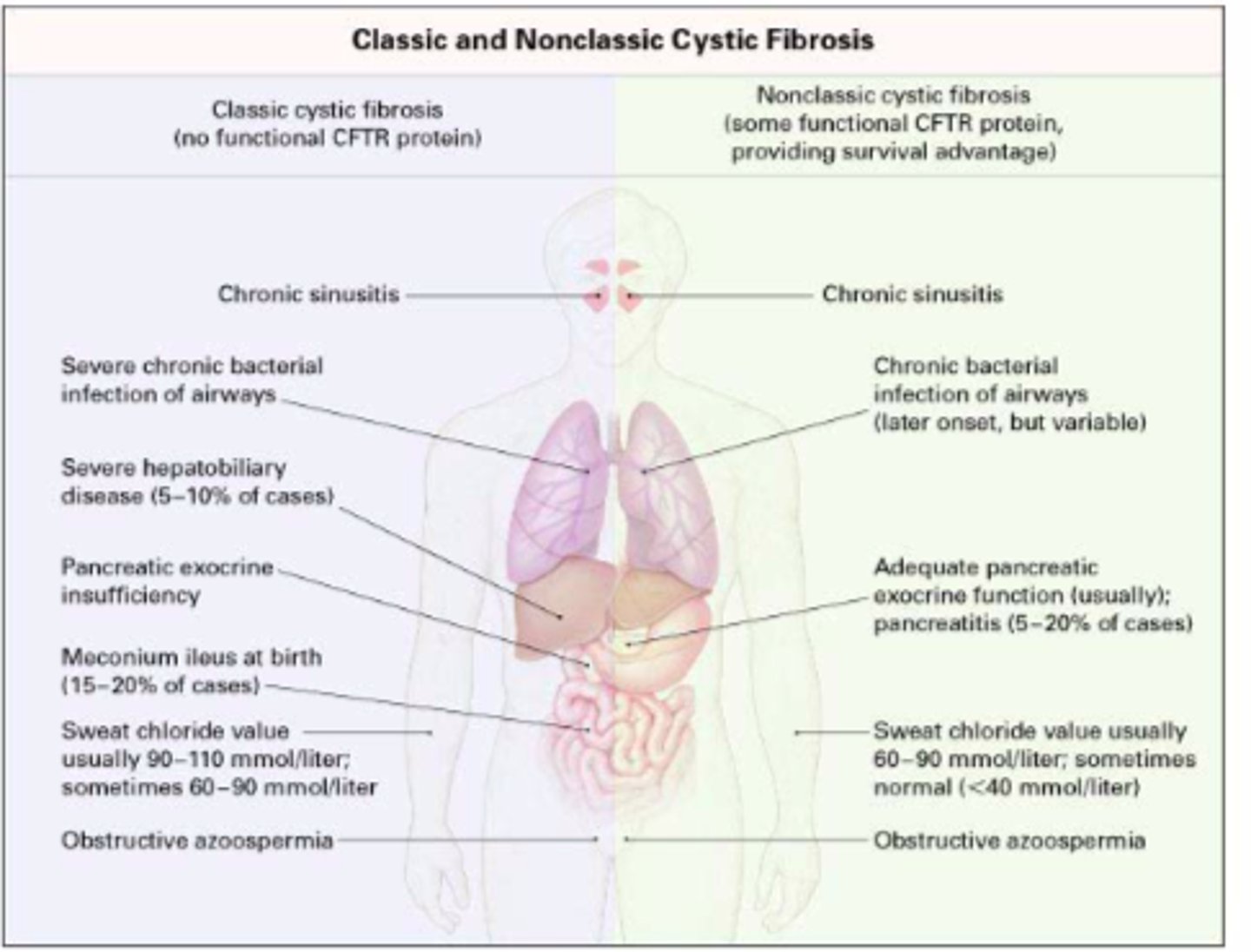
Classic cystic fibrosis: chronic bacterial infection of the ________ and _________
- (of the) airways
- sinuses
Classic cystic fibrosis: _____ ____________ due to pancreatic exocrine insufficiency
- fat maldigestion (due to pancreatic)
Classic cystic fibrosis: fat maldigestion due to __________ ___________ _____________
- (fat maldigestion due to) pancreatic exocrine insufficiency
Classic cystic fibrosis: ________ in males due to obstructive azoospermia
- infertility (in males due to obstructive azoospermia)
Classic cystic fibrosis: infertility in males due to ____________ ___________
- (due to) obstructive azoospermia
Classic cystic fibrosis: ___________ concentrations of chloride in sweat
- elevated (concentrations of chloride)
Sweat may taste salty as a sign of first diagnosis
Nonclassic cystic fibrosis
have at least one copy of a mutant gene that confers partial function of the CFTR gene
usually have no overt signs of maldigestion because some pancreatic exocrine function is preserved
Nonclassic cystic fibrosis: have at least one copy of a mutant gene that confers ________ _________ of the CFTR gene
- (confers) partial function
usually have no overt signs of maldigestion because some pancreatic exocrine function is preserved
Nonclassic cystic fibrosis: these patients usually have ___ _______ signs of maldigestion because some pancreatic exocrine function is _________
- no overt (signs of maldigestion)
- (pancreatic exocrine function is) preserved
Classic vs. non-classic cystic fibrosis figure
Genotype and phenotype: CF is caused by mutations in the _______ gene.
Genotypic variation only roughly _____________ to phenotype
- CFTR (gene)
- (only roughly) correlates (to phenotype)
Genotype and phenotype: poor correlation between ______ _________ and ________ of lung disease strongly suggests an influence of environmental and secondary genetic modifiers
- CFTR genotype
- severity (of lung disease)
Genotype and Phenotype: _______ correlation between CFTR genotype and severity of lung disease strongly suggests an influence of ____________ and ____________ genetic modifiers.
- poor (correlation)
- environmental
- secondary (genetic modifiers)
Genotype and Phenotype: Genes related to ________ and _________ immune response may be key ____________ _____ modifiers.
- innate
- adaptive (immune response)
- pulmonary CF (modifiers)
Genotype and Phenotype: phenotypic spectrum is much more than just...
classical and non-classical CF
Wide range of cystic fibrosis
Classic Cystic Fibrosis Mutation
∆F508
classic is more predominant than non-classic
CFTR function and biochemistry: CFTR controls ___________ ______ movement in and out of the cell
- chloride ion (movement)
CFTR function and biochemistry: _______ controls chloride ion movement in and out of the cell
- CFTR (controls chloride ion movement)
CFTR Function and biochemistry figure
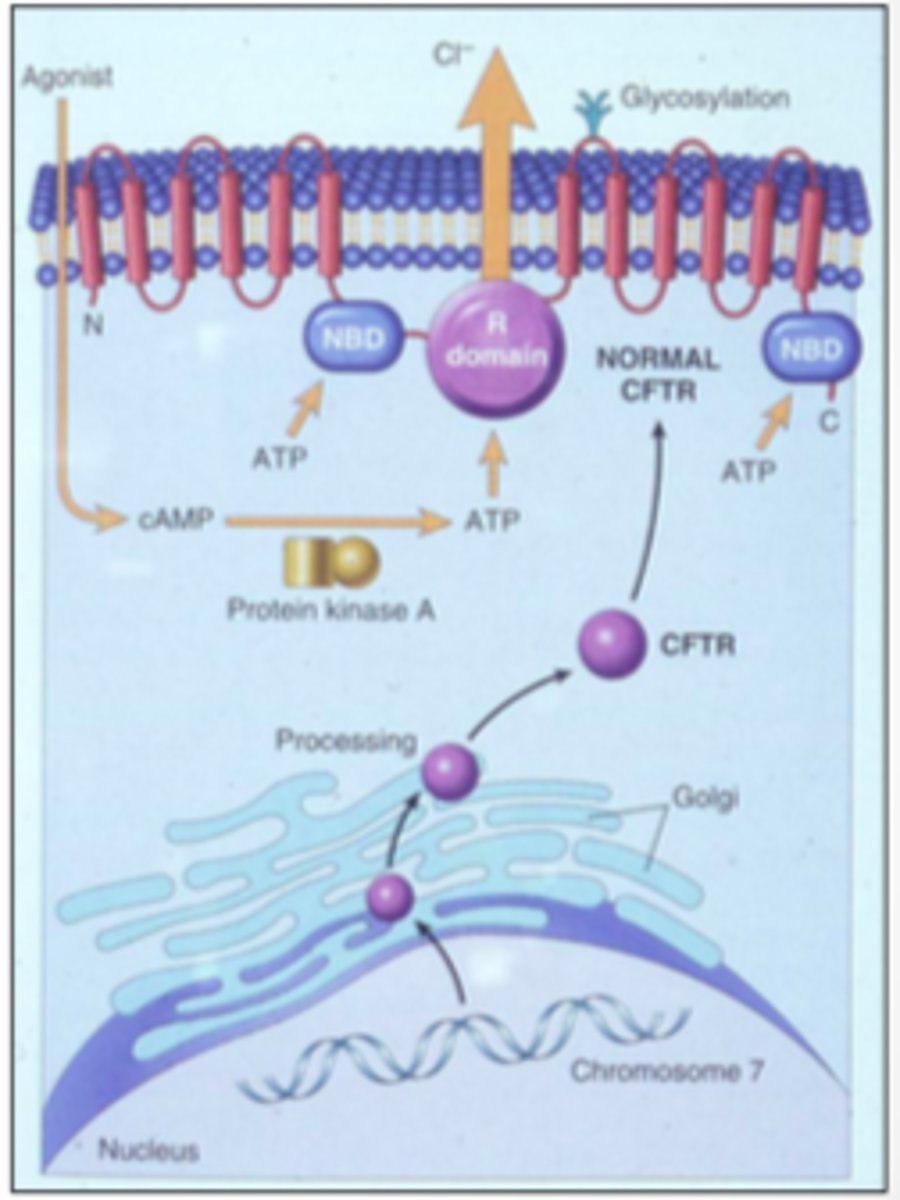
CFTR exists on the ___________ membrane of the cell
- apical (membrane of the cell)
When it moves chloride, Na+ and water follow it, thus there is increased secretion wherever chloride ions are moved
CFTR moves chloride, _____ and _______ follow it, thus there is __________ secretion wherever chloride ions are moved
- Na+
- water (follow it)
- increased (secretion)
CFTR function figure: normal vs cystic fibrosis
In CF, the mucus is dehydrated due to the lack of chloride movement, Na+ and water do not follow it out
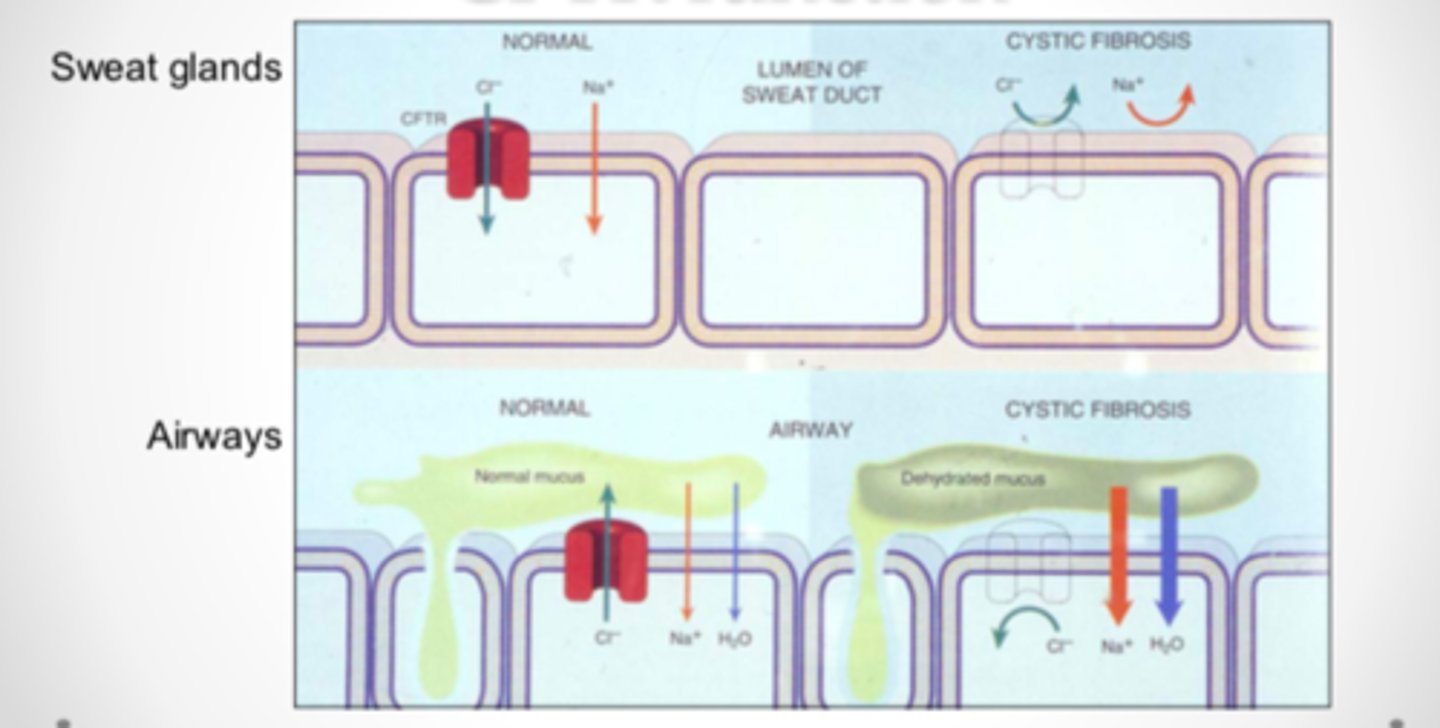
CFTR function, in cystic fibrosis, the mucus is ___________ due to the lack of ___________ ________, Na+ and water stay inside the cell membrane
- dehydrated
- (lack of) chloride movement
Protein structure and function: CFTR __________ chloride ions across the membranes of the lungs, liver, pancreas, digestive tract, reproductive tract, and skin
- transports (chloride ions across the membranes)
Protein structure and function: CFTR is made up of _______ domains
- five (domains)
Two membrane spanning domains (MSD1 and MSD2) that form the chloride ion channel
Two nucleotide binding domains (NBD1 and NBD2) that bind and hydrolyze ATP (adenosine triphosphate)
and a regulatory R domain
Changes in protein structure: CFTR functions principally as a ________-_________ __________ ___________ and appears capable of regulating other ion channels
- cAMP-induced chloride channel
Changes in protein structure: CFTR functions principally as a cAMP-induced chloride channel and appears capable of ___________ other ion channels
- regulating (other ion channels)
Besides the most common mutation, ∆F508, accounting for about 70% of CF chromosomes worldwide, more than 850 mutant alleles have been reported tot he CF genetic analysis consortium
Changes in protein structure: Besides the most common mutation, ∆F508, accounting for about 70% of CF chromosomes worldwide, more than _____ _________ _________ have been reported to the CF genetic analysis consortium
- (more than) 850 mutant alleles
These mutations affect CFTR through a variety of molecular mechanisms which can produce little or no functional CFTR at the apical membrane.
Changes in protein structure: these mutations affect CFTR through a _________ of molecular mechanisms which can produce _____ or ___ __________ CFTR at the apical membrane.
- variety (of molecular mechanisms)
- little
- no functional (CFTR)
Molecular biology of ∆F508: when a CFTR protein with the ∆F508 mutation reaches the ___________ _______, the quality-control mechanism of this cellular component recognizes that the protein is folded __________ and marks the defective protein for _________.
As a result, ∆F508 NEVER reaches the cell membrane
- (reaches the) endoplasmic reticulum
- (folded) incorrectly
- (defective protein for) degradation
Molecular biology of ∆F508: when a CFTR protein with the ∆F508 mutation reaches the endoplasmic reticulum, the ________-_________ mechanism of this cellular component recognizes that the protein is folded incorrectly and marks the _________ protein for degradation
As a result, ∆F508 _______ ________ the cell membrane
- quality-control (mechanism)
- defective (protein for degradation)
- NEVER reaches (the cell membrane)
Molecular biology of ∆F508:
People who are homozygous for ∆F508 mutation tend to have the _________ __________ symptoms of cystic fibrosis due to critical loss of _______________ ______ __________
- most severe (symptoms of cystic fibrosis)
- (critical lss of) chloride transport
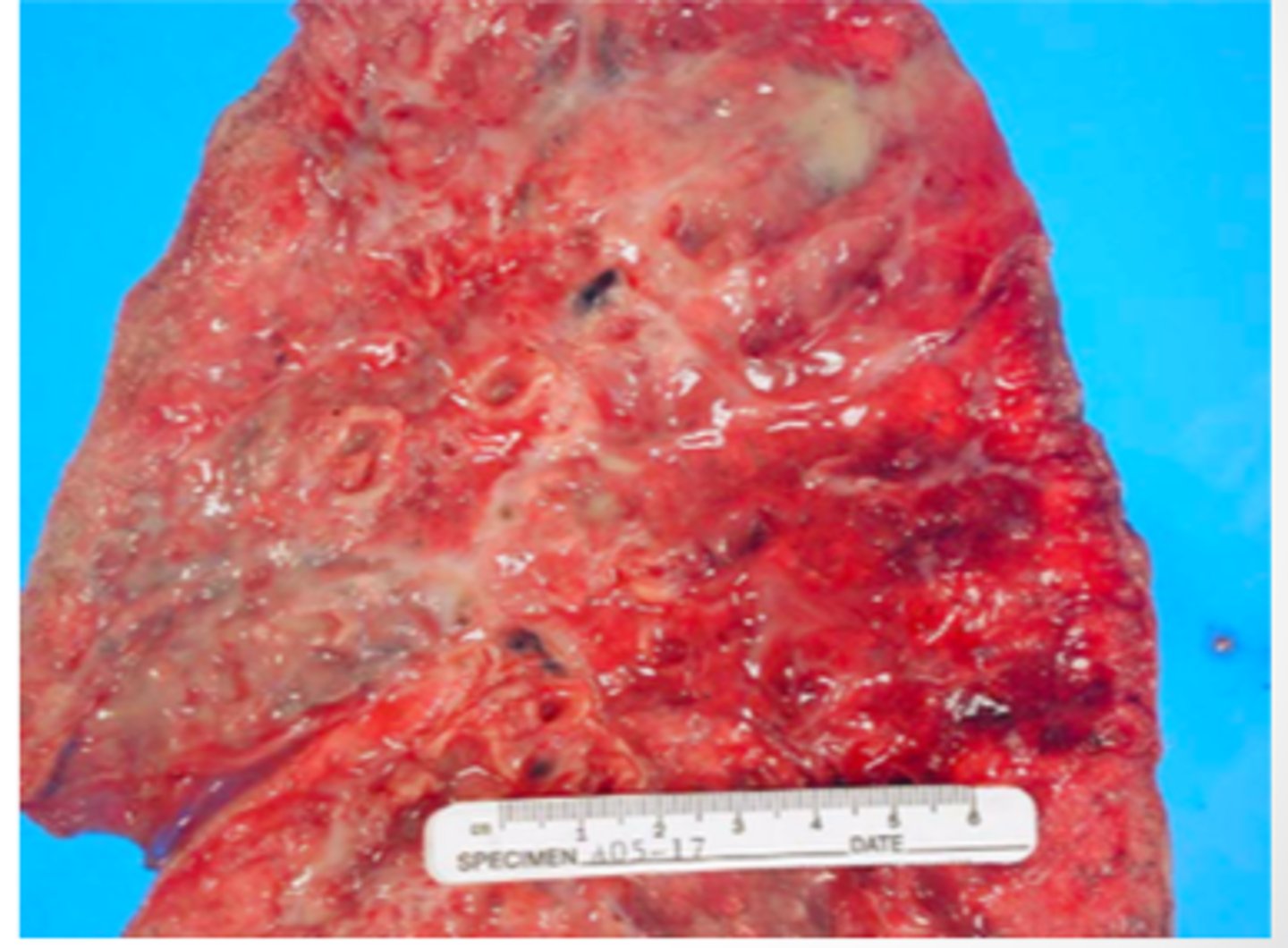
Presentation of disease: mucus in the airways cannot be _________ __________ from the lungs, leading to ________ infections that can become fatal
- easily cleared (from the lungs)
- chronic (infections)
Presentation of CF - disease in the lungs figure
Presentation of CF - disease in colon and pancreas
Treatment of CF: the only way to cure CF would be to use ______ ________ to replace the defective gene to express the _______ form of the protein
- gene therapy (to replace the defective gene)
- normal (form of the protein)
Treatment of CF: major goals in treating CF
1. clear the abnormal and excess secretions
2. control infections in the lungs
3. prevent obstruction in the lungs
Treatment of CF - major goals in treating CF: clear the _________ and ________ secretions
- abnormal
- excess (secretions)
Treatment of CF - major goals in treating CF: control the __________ in the lungs
- infections (in the lungs)
Treatment of CF - major goals in treating CF: prevent ___________ in the intestines
- (prevent) obstruction (in the intestines)
Treatment of CF: symptoms treated with _________ and ____-________ for bronchodilation.
Although treating the symptoms does _______ _______ the disease
- (symptoms treated with) antibiotics
- β-agonists (for bronchodilation)
- NOT cure (the disease)
It can greatly improve the quality of life for most patients and has over the years, increased the average life span of CF patients to ~30 years
Treatment of CF: for patients with __________ stages of the disease, a ______ ___________ may be necessary
- advanced (stages of the disease)
- lung transplant (may be necessary)
Gastrointestinal treatment of CF: _________________ of diet is essential
- MODIFICATION (of diet is essential)
Gastrointestinal treatment of CF - due to pancreatic disorders, children with CF require a modified diet: vitamin supplements
K, A, D, E
K, A, D, E are the fat soluble vitamins. Pancreatic lipases have issues with being excreted
Gastrointestinal treatment of CF - due to pancreatic disorders, children with CF require a modified diet: __________ enzymes and _________ caloric content (________ the normal)
- pancreatic (enzymes)
- increased (caloric content)
- double (the normal)
Gastrointestinal treatment of CF - due to pancreatic disorders, children with CF require a modified diet: _____ fat and ____ protein
- high (fat)
- high (protein)
Ivacaftor (KALYDECO): for patients with the _______ or ________ mutations (as well as ____ other rare mutations)
- G551D
- R117H (mutations)
- 8 (other rare mutations)
Ivacaftor (KALYDECO): these patients have ________ at the membrane but it does ______ _________ chloride ion
- CFTR (at the membrane)
- NOT conduct (chloride ion)
i.e., patients with G551D or R117H mutations
Ivacaftor (KALYDECO): will enhance the _____ ___________ by increasing the channel opening probability
- Cl conductance (by increasing the channel opening)
Ivacaftor (KALYDECO): will enhance the Cl conductance by increasing the ________ ___________ ______________
- (increasing the) channel opening probability
Ivacaftor (KALYDECO): approved for use in patients as young as ___ _______
- (as young as) 1 y/o
DOES NOT WORK in patients with F508 deletions
Ivacaftor (KALYDECO): DOES NOT WORK in patients with ______ ___________
- ∆F508 deletions
Ivacaftor (KALYDECO) side effects
abdominal pain (can be serious)
diarrhea
dizziness
upper respiratory tract reactions
headache
Ivacaftor (KALYDECO): primarily metabolized by _________
- CYP3A
Ivacaftor
KALYDECO
Lumacaftor / Ivacaftor (ORKAMBI): for patients homozygous for _______ ___________ as young as age __ y/o
- ∆F08 deletion
- (young as age) 2 (y/o)
Lumacaftor / Ivacaftor (ORKAMBI): Lumacaftor acts as a _________ to get more CFTR channel to the _________
- (acts as a) chaperone
- (to the) membrane
Ivacaftor helps it work better once CFTR is at the membrane
Lumacaftor / Ivacaftor (ORKAMBI): Lumacaftor acts as a chaperone to get more CFTR Channel to the membrane
Ivacaftor helps it work ________ once _________ is at the membrane
- (work) better
- (once) CFTR (is at the membrane)
Lumacaftor / Ivacaftor (ORKAMBI): __________ ______ testing needed
- annual liver (testing needed)
Lumacaftor / Ivacaftor (ORKAMBI) side effects
Dyspnea upon drug initiation
Hypertension
Cataracts
abdominal pain
jaundice
loss of appetite
N/V
confusion
Tezacaftor / Ivacaftor
SYMDEKO
Tezacaftor / Ivacaftor (SYMDEKO): for patients ___________ for ∆F508 deletion, ages ___ and up
- homozygous (for ∆F508 deletion)
- 12 (and up)
Lumacaftor/Ivacaftor (ORKAMBI) is also used for ∆F508 homozygous patients
Tezacaftor / Ivacaftor (SYMDEKO): Tezacaftor acts as a ___________ to get more CFTR channel to the membrane
Ivacaftor helps it work _______ once it is there
- (Tezacaftor acts as a) chaperone
- (Ivacaftor helps it work) better