Hallucinogens/ Psychedelics
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
Mescaline
found in tops of peyote cacti. Dried, powder, chewed, or cooked and eaten. Inspired Aldous Huxley’s “Doors of Perception” which influenced psychedelic use in 1960s
Psilocybin
come from a few mushroom species (conocybe, copelandia, pnaeolus, psilocybe, and stropharia)—dried, eaten raw, boiled to tea or cooked in food. 1-5g to have psychedelic effects.
Psilocin
the active agent in psylocybin, which it is converted into enzymatically after ingestion
DMT
most used tryptamine—smoked or snorted for an intense 30 min trip. When taken orally, completely metabolized by MAO in liver so no effect
“Foxy” or AMT
synthetic versions of DMT—can be taken orally in pill form or crushed and snorted
Other tryptamines
-5-MeO-DMT
-Bufotenine
Ayahausca
a strong herbal tea with DMT and B-carbolines from the Banisteriopsis vine—the B-carbolines inhibit MAO and prevent metabolism of DMT in the liver, allowing it to have it’s psychedelic effects. Used by Amazonian tribes in religious ceremonies and now only legal in US for specific syncretistic Catholic/traditional religious ceremonies
LSD
lysergic acid diethylamide—synthetic compound with similar chemical structure to fungal alkaloids. Banned for recreational use in 1967, but many still use illicitly and buy as droppers or tabs to swallow. Much research done on both therapeutic applications and by CIA and US Gov on utilizing as a psychochemical weapon (1940s-70s)
NBOMes
new hallucinogens—most notable one is 25I-NBOMe which is used on blotter paper or in powdered form, placed under tongue or chewed on gum. Subject to first-pass metabolism if taken orally. Very potent, easy to overdose and toxicity can be fatal
Salvanorin A
compound of the salvia mint plant native to Mexico—leaves chewed, dried and crushed. Administered sublingually or smoked. Effects only last 15 minutes but have a unique hallucinogenic profile including:
-out of body experiences of being a foreign object
-visiting the past/childhood
-motion or pulling/twisting sensations
-depersonalized or separate form self
-in several places at once
Legal status of Salvia
not on DEA controlled substances, but is illegal to own or sell in most states
Ibogaine
from a west African shrub “tabernanthe iboga”—typically dried bark or roots are chewed or ground into powder. Primarily a stimulant producing high energy, appetite reduction and euphoria, but at high doses is a hallucinogen. Was marketed in Europe as an antidepressant “Lamberene”, and also researched as a treatment for drug addiction.
Legal status of Ibogaine
Schedule I controlled by DEA, and not FDA approved. Toxicity can cause death
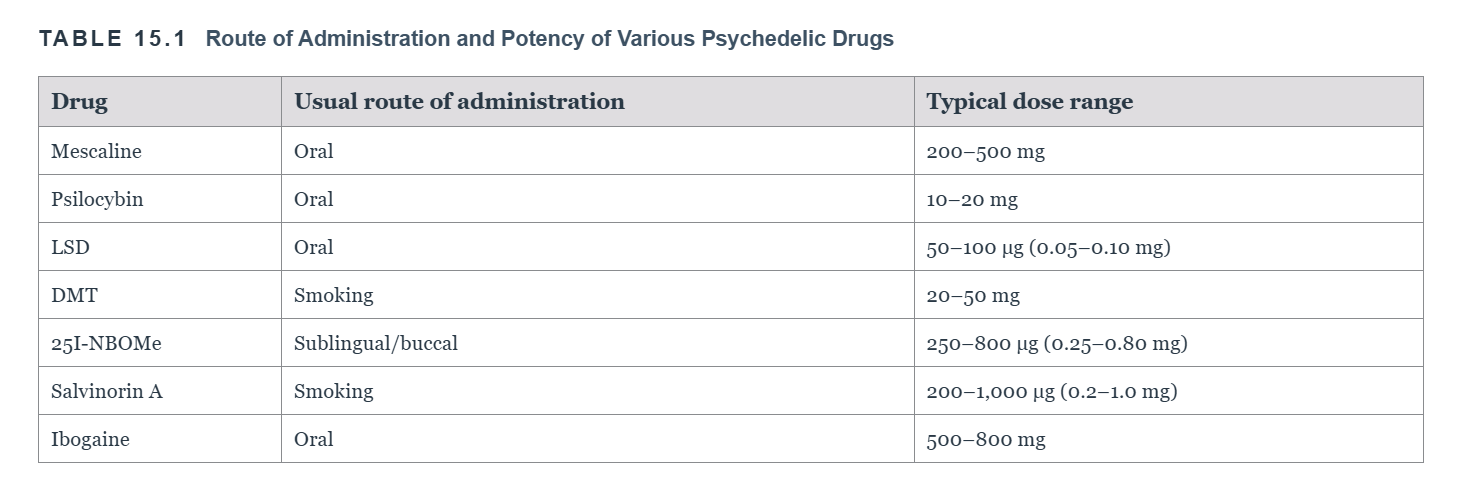
Route of administration and potency
Stages of LSD trip
1) Onset—30-60 mins after ingestion, colors brighten and strange patterns or objects appear
2) Plateau—next 2 hrs, slowed sense of time and more intense visuals
3) Peak—next 2-3 hrs, feeling of otherworldliness, stream of bizzare distorted images and synsethesia
4) Come-down—2 more hours, effects dissipate
Psychological aspect of “trips”
can swing from anxiety to euphoria to illogical thought to depersonalization— a “good” trip produces a mystical or enlightening experience, a “bad” trip a frightening or disturbing one
Psychometrics to evaluate trips
1) Altered States of Consciousness rating scale (ASC)
2) Strassman’s Hallucinogen Rating scale
Indeolamines
psychedelics that have a serotonin-like structure—includes:
-LSD
-Psilocybin/ psolicin
-DMT
-5-MEO- DMT
-Ibogaine
-synthetic Tryptamines
Phenethylamines
psychedelics that have a catecholamine-like structure (especially resembling NE, and amphetamine). Includes:
-NBOMes
-Mescaline
Salvanorin A structure
unique compared to other psychedelic compounds—not indoleamine or phenethylamine
Key serotonergic receptor subtype for hallucinogens
5-HT2a receptors—specifically, those that have complexed with glutamate receptor mGluR2, which changes it’s second messenger pathway signaling to produce psychedelic effects
Reason for LSD long trip
when LSD binds to a receptor, part of receptor protein forms a “lid” clamping it in place and allowing for extended duration of action
Salvanorin A’s chemical action
binds to k-opioid receptors in the thalamus, temporal and parietal cortices, and claustrum
Ibogaine’s chemical action
it and it’s active metabolite noribogaine both act as:
-partial agonists at k-opioid receptors and m-opioid receptors
-NMDA antagonists
-5-HT and DA reuptake inhibitors
Psychedelic neural circuit
Activation 5-HT2a and mGluR2 disrupts this circuit:
Cortices—> striatum—>thalamus—> cortices
which is necessary for thalamic gating of sensory/cognitive input running from subcortical to cortical areas
fMRI and EEG discoveries
REDUCED activity within the DMN
INCREASED connectivity among sensory cortical areas, between sensory cortical areas and thalamus, and between thalamus and ventral striatum and posterior cingulate cortex (PCC)
REDUCED connectivity between association areas and thalamus
Possible therapeutic use
psychedelics are being investigated for treatment of:
-treatment-resistant depression
-anxiety disorders
-OCD
-PTSD
-SUDs
-Cancer
Microdosing
administering small doses of hallucinogens frequently—unclear if there is any benefit
Psychoplastogen
a drug that results in increased neuroplasticity and dendritic and synaptic growth, e.g., hallucinogens
Adverse reactions
psychosis, agitation, kidney damage, seizures, hypertension, tachycardia, fever, muscle breakdown—at toxic doses, NBOMes are the worst and can even lead to death
Other hallucinogen use disorder
for those that continue using despite no addictive qualities and without regard for negative life effects—disincludes PCP
Hallucinogen Persisting Perception Disorder (HPPD)
in DSM V—effects of a trip last for an extended time afterwards and will not go away—producing great distress
PCP
phencyclidine—originally synthesized as anesthetic. Has analgesic properties, but instead of sedation it produces a trance-like state with complete dissociation, muscle rigidity or flexibility, and vacant face. Adverse reactions were disorientation, hallucinations, agitation and even violence. Gained some street popularity as “angel dust” or “hog” but not much
Ketamine
invented as safer alternative to PCP—still used as anesthetic and surpassed PCP as street drug. Taken by IV (for medical), intramuscular, oral, smoked, or snorted. Less potent and shorter acting with less adverse effects
Characteristics of “dissociative anesthesia”
as shown with PCP and Ketamine, produces symptoms very similar to those of schizophrenia
PCP & ketamine action
uncompetitive antagonists of NMDA— block ion flow and remain trapped in channel even when it closes. Results in increased GLU release which relates to positive psychotic symptoms
PCP & Ketamine effects on DA
increases firing in the dorsal striatum, NAcc, and PFC—constitutes the reinforcing component
Adverse effects of chronic Ketamine use
-persisting psychosis
-memory/ cognitive deficits
-delusions
-gray and white matter abnormalities
Therapeutic uses of Ketamine
treats MDD (alongside SSRI), analgesic, possibly addiction and PTSD