HEDC RESTORATIVE DENTISTRY PERSPECTIVE
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
what should you do when meeting a patient
introduce yourself by name and role
confirm patient identity: name, DOB, first line of address
ensure patient notes match the patient
confirm reason for attendance
outline the medical history
should be taken at least every 12 months to ensure patient’s medical status allows safe dental treatment
determine whether proposed treatment needs any special precautions
determine impacts of current medication on dental treatment
patient allergies to medication or materials used during treatment
potential drug interactions to medication used during treatment
indicator of capacity to give consent
what medication has interactions with warfarin
metronidazole
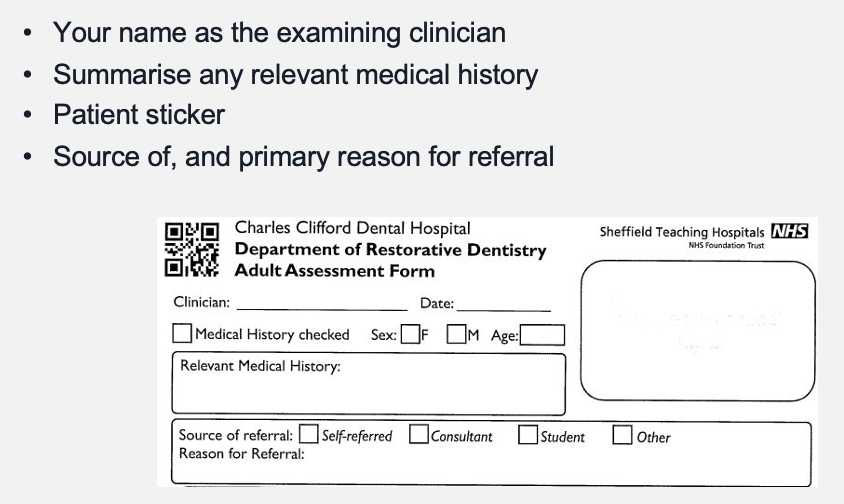
CCDH restorative dentistry assessment sheet
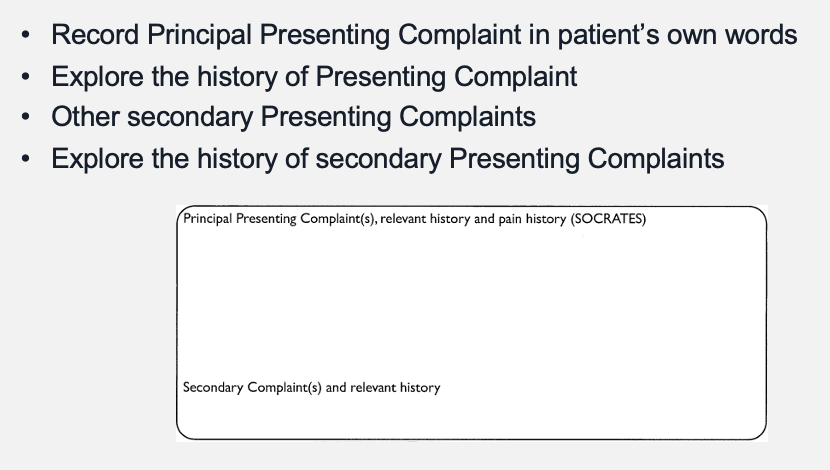
outline dental history
patient’s attitudes
perceived dental treatment needed
patient’s expectations of treatment
determine whether realistic and achievable
manage expectations to ensure adequate consent achieved
past dental experience e.g. type of work carried out, MDAS scale
problems encountered e.g. retching issues
MDAS scale
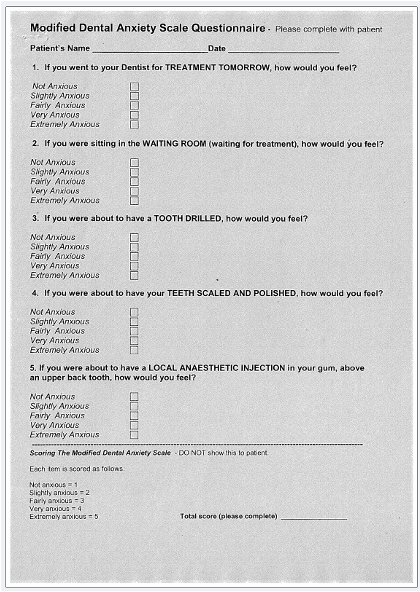
when would the MDAS scale be important
when referring patients for sedation, they must hit a certain threshold on this scale
outline social history
understanding of patient’s life e.g. how do they travel to surgery, arranging appointments around work/ school/ bus pass timings
occupation incl. caring for family
personal circumstances i.e. living arrangements - important for elderly and children
smoking, alcohol, recreational drugs
opinions on use of animal products (bovine/ porcine)
why is social history important
able to plan extent of treatment
able to plan timing of treatment
may improve likelihood of successful treatment outcomes
outline smoking in social history
major risk factor for periodontitis and oral cancer
synergistic effect if alcohol user
weakens immune system
reduces blood flow to gingivae - this masks disease
often whilst they’re smoking, there is little to no bleeding, when they stop they bleed profusely
increases progression of gingivitis to periodontitis
delayed healing after extractions and surgery
stained teeth/ halitosis
altered smell/ taste
what risk is increased in smokers post-extraction
increased risk of dry socket post-extraction
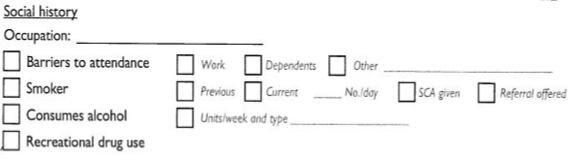
how should smoking be recorded in the social history
record whether current or previous smoker
record number smoked per day to calculate ‘pack years’
20 cigarettes per day = 1 pack year
10 cigarettes per day = ½ pack year
record in notes with orange sticker if smoking cessation offered
action referral if patient shows interest
outline VBA
very brief advice
3 step process:
ASK about a patient’s smoking status
ADVISE them on the best way to quit
ACT to offer support, such as referring to specialist service or prescribing medication
what is the aim of VBA
to trigger a quit attempt by identifying smokers and connecting them with evidence-based support
outline alcohol in social history
erosion of teeth
acidity of alcoholic drinks directly affects teeth
vomiting if excess alcohol also contributes
increased caries risk
diuretic effect reduces saliva
alcohol metabolises to sugar and some drinks are high in sugar
increased risk of oral, laryngeal and oesophageal cancer
synergistic effect if also a smoker
increased risk of trauma and assault
outline the Audit C tool
Alcohol Use Disorders Identification Test for Consumption
screening tool was originally developed by the WHO as a simple method of screening for excessive drinking
consists of 3 questions which the patient scores 0-4 with their answer
total score identifies harmful or hazardous drinkers
clinicians need to be aware of units of alcohol
image of Audit-C tool

outline recreational drugs in social history
effects from chemical properties
xerostomia increases caries risk
tooth erosion as many are highly acidic
gingival damage if rubbed into gums
effects from behavioural change
clenching/ grinding » tooth wear/ breakage/ TMJ
neglect with poor OH increases caries and periodontitis risk
desire to eat sweet foods increases caries rate e.g. Methadone users (heroine addiction)

what does this clinical image show
meth mouth
what can be an alternative to sugars in drinks
sweeteners
how should current oral hygiene measures and diet be recorded
consider brief OHE if obvious OH concerns
consider diet diary if obvious dietary concerns
what are the aims of clinical examination
determine the patient’s dental health now
to assess disease progression over time
medico-legal requirement
to fully record the patient for identification purposes post-mortem
outline extra-oral clinical examination
examine TMJ for clicks, deviation on opening/ closing, pain
palpate lymph nodes
examine muscles of mastication
examine gland/ tonsillar tissues
examine all soft tissues systematically
note any lesions and measure them if appropriate
normally, how many fingers can you fit between incisors when patients open their mouth
2 fingers
outline criteria for intra-oral examination
clean, dry teeth - also examine wet
good lighting
good vision - magnification
examining the dentition
teeth present/ absent, supernumerary, retained roots
presence of caries: site, extent (early/ cavitated), activity (active/ arrested), status (primary/ secondary )
presence of tooth tissue loss not caused by caries
record tooth wear using Smith & Knight scale: Grade 0-3 (3 = pulpal involvement)
record any tooth mobility: grade 0-3 (mm thresholds)
what are signs and symptoms of an unstable occlusion
tooth wear
fractured cusps
fractured restorations
localised periodontitis
pulpitis
failure of crowns and bridges
cracked tooth syndrome
TMJ symptoms

how should occlusion be examined
use articulating paper to see contacts in ICP and in CR
assess whether ICP is stable or unstable
assess whether occlusal vertical dimension is normal or reduced
determine whether ICP = RCP
if not, determine whether the slide between them is vertical/ horizontal
assess in protrusive and lateral excursions
can take impressions for study models to view occlusion on an articulator
what kind of tool is the BPE
BPE is for screening, it is not a diagnostic tool
outline examining the periodontium
do BPE (excludes 8s)
required for all new patients
required every examination for code 0/1/2 patients
code 3 or 4 patients require a more detailed periodontal charting
use indices to score patients at baseline and monitor progress
6PPC, PI, BI, M, R (recession), F (furcation)
when would 8s be included in a BPE
if the 6s or 7s are absent
pathways for different BPE scores
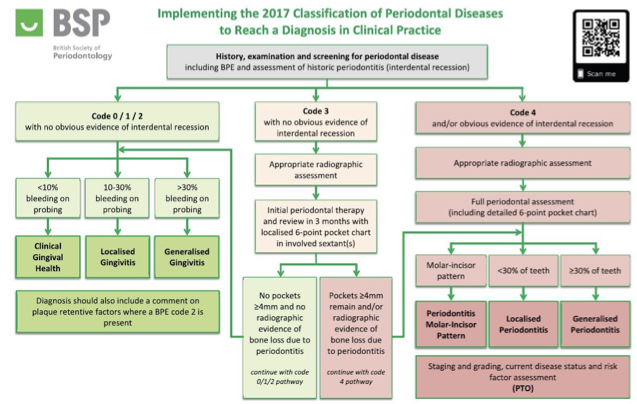
when should the indices be taken for a code 3 pathway patient
for code 3 pathway, indices are taken 3 months following the initial therapy
when should the indices be taken for a code 4 pathway patient
for code 4 pathway, indices are taken initially and post-therapy
outline denture examination
examine dentures in situ and out of patient’s mouth and assess:
appearance
extension of denture bases and flanges
occlusion
speech
vertical dimension
design

what else should be recorded about dentures
type: partial/ complete
record material: acrylic, cobalt chrome, nylon
assess retention and stability
assess amount of wear, hygiene status and age
outline special investigations
pulpal diagnosis: sensibility tests e.g. EndoFrost, EPT, ethyl chloride
periapical diagnosis: percussion testing, palpation of sulci
cracked tooth syndrome (CTS): tooth slooth
transillumination
radiographs
outline the types radiographs and when they would be taken
bitewings: posterior proximal caries, bone levels
periapicals: caries extent, periapical pathology, bone levels
OPT: overall view, trauma, pathology, 3rd molars
CBCT: implants, endodontics, pathology
—
ALL RADIOGRAPHS SHOULD BE GRADE FOR QUALITY (A/ NA), DATED AND REPORTED ON
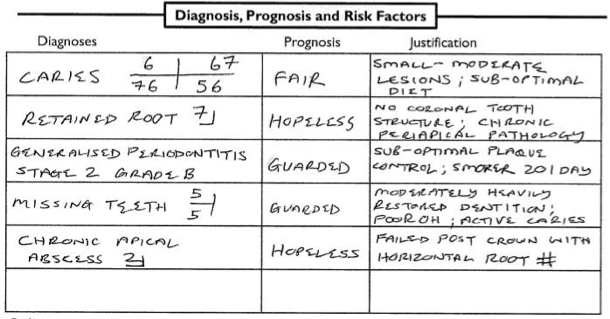
outline diagnosis, prognosis, risk factors
make diagnoses for any conditions
assign prognoses to all diagnoses with justification
consider general prognosis for multiple conditions
example of diagnosis, prognosis and risk factor table
if in doubt of prognosis, go lower
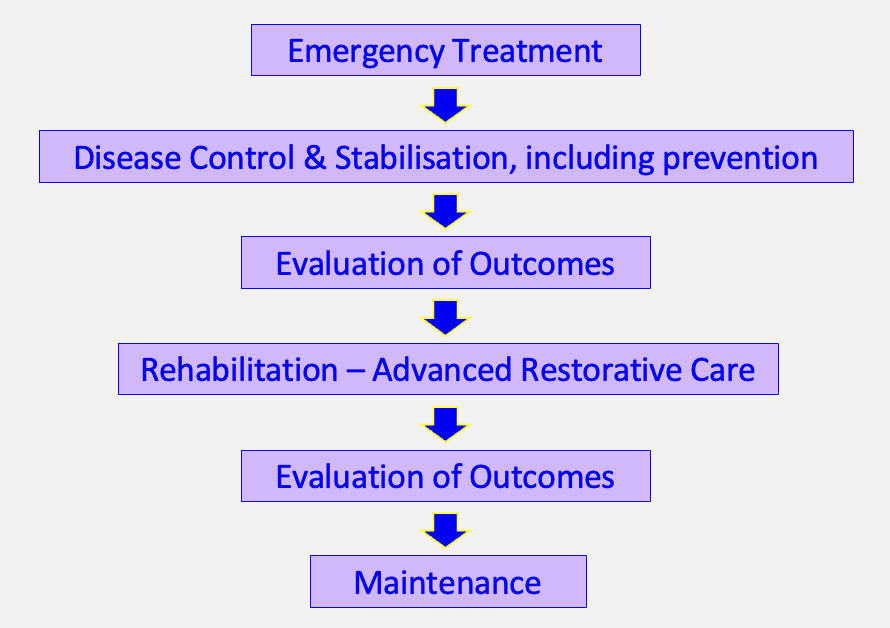
staging treatment plans 1 - ALWAYS PREVENTION FIRST
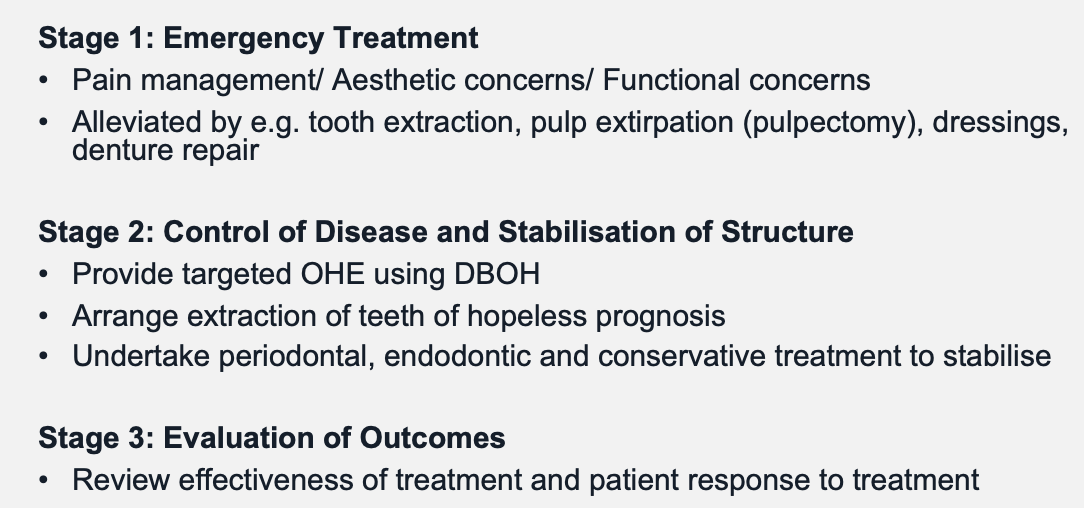
staging treatment plans 2 - ALWAYS PREVENTION FIRST
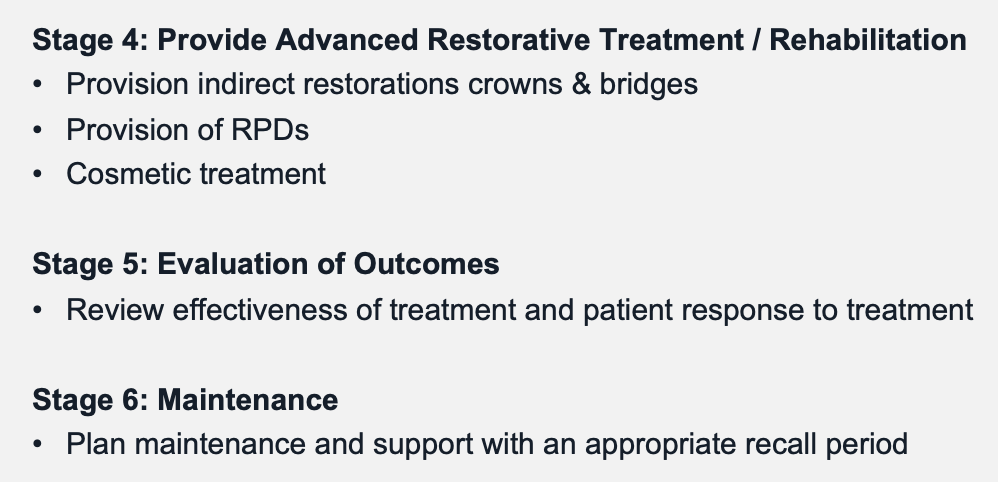
stages of treatment plans flow chart
treatment planning involving patient
plan the order of treatment required
discuss with patient respecting their views
gain patient consent for treatment


finalising the treatment plan
gain informed patient consent for treatment
provide written treatment plan
discuss any costs involved
plan maintenance following treatment