OB Cornell Notes Ch 24 & 17
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
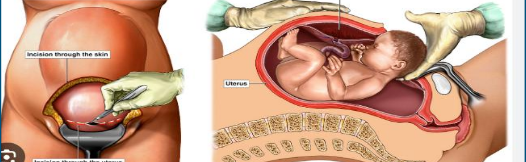
C-section
Birth w abdominal incision into uterus; slightly more hazardous than vag
Healthy People goal is to reduce rate of c-births among low-risk patients having first child
Prophylactic measure to alleviate problems of birth like cephalopelvic disproportion, breech or multiple fetus births, or failure to progress labor
Amniotomy
artificial rupturing membranes with a knife or som during labor if they don’t rupture spontaneously
Momentary risk for cord prolapse
Only perform if fetal head is well applied to cervix. Always measure FHR immediately after rupture

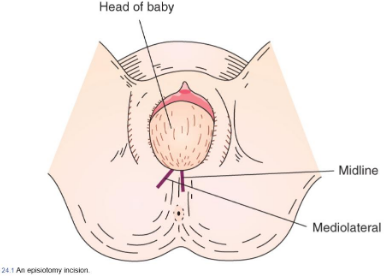
Episiotomy
Surgical incision of perineum to release pressure on the fetal head with birth and possibly shorten the last portion of the second stage of labor
Not done midline so it doesn’t split through anus. Mediolaterally
Pre-operative teaching
For c-section, acquaint pt with special equipment used (inform them whats abt to happen).
Teach pt exercises to maintain respiratory and circulatory function and prevent postoperative complications (e.g. early ambulation, turning, incentive spirometer). Prevents post-op complications.
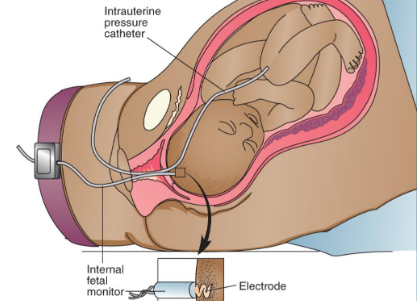
Internal Electric Monitoring
Most precise method to monitor FHR & contractions
Pass a pressure-sensing catheter through the vagina and into uterus after membranes ruptured, SCREW TO BABY HEAD
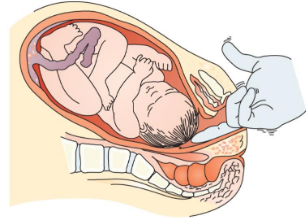
Scalp stimulation
If FHR variability is depressed during labor, this helps assess welfare of the fetus
Stim baby scalp w finger (through dilated cervix)
baby should have momentary inc FHR
if in distress, FHR acceleration will NOT occur
Uterus complication
Because uterus is handled during c-section birth, may not contract well afterward
Can lead to postpartum hemorrhage
Bladder complication
For provider to reach uterus, bladder must be displaced anteriorly
bladder mmay not sense filling as well post-procedure
Intestine complication
Paralytic ileus or halting of function with obstruction may occur
Lower extremity circulation complication
Thrombophlebitis from impaired blood flow is possible (e.g. DVT)
Post-op exercises
Deep breathing
Stasis of mucus can cause infection
prevent by doing 5-10 deep breaths/hr, hold for 1-2s.
Turning
Preventing respiratory and circulatory statis
Incentive spirometry
Used 3-4 times/day to encourage deep breathing
purpose to fully aerate lung spaces, so most models triggered by inhalation
Ambulation
Most effective way to stim lower extremity circulation after c-section
Discharge planning
Do not lift any object heavier than 10lbs
Do not walk up stairs more than once a day for first 2wks
Resume sex as soon as comfortable
Warning signs
Report redness/drainage at c-section incision line
lochia heavier than normal menstrual period
abd pain other than at suture line
Psychological changes postpartum and Nursing Care: (6 weeks-yr postpartum)
Psychological
Attachment to newborn
skin-to-skin for early attachment
En face position: direct eye contact w newborn, good sign of engrossment - how well a parent is attaching to kid
Feeling overlooked or forgotten
Disillusionment: disappointment after birth (tell mother this is normal❗)
postpartal blues: 50% patients experience ‘baby blues’, breastfeeding can help
Physiologic changes postpartum & Nursing care
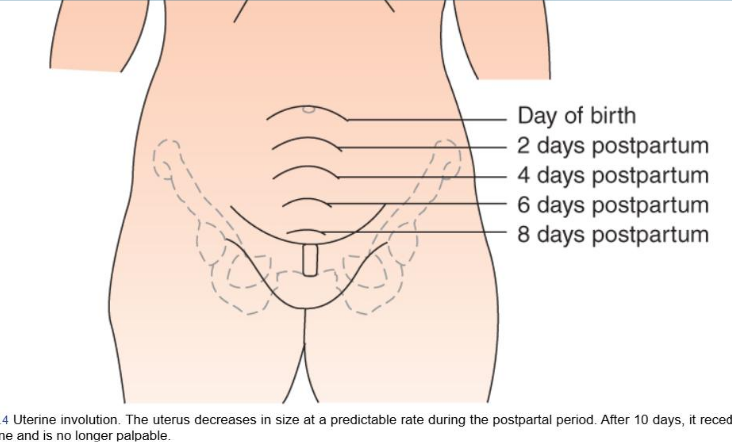
Uterus
Involution involves sealing of placenta area (prevent bleeding) and reducing size to pregestational size
Takes 6 weeks
Fundus
after birth, fundus palpable halfway btwn umbilicus and pubic bone for a few min
one hr later, rises to level of umbilicus (remains here for 24hrs)
decreases by 1cm/day
Lochia
residual blood, fragments of decidua, WBC, mucus, bacteria
Expected findings:
1-3d: red, moderate/heavy
3-7d: brownish
7-14d: serous
2-3wks: yellowish
3-4wks: grayish
Cervix
Internal os closes as before
external os used to be round, now it has slits on the side/stellate shaped
Vagina
soft, some rugae, diameter greater than normal
Perineum
Pressure during birth → perineum is endematous and tender immediately after
suggest comfort (gentle pillow, doughnut pad, warm packs, analgesics)
Nursing care for Urinary System changes
Extensive diaphoresis (sweating) and diuresis (excessive urine prod) almost immediately
Assess abdomen freq for overdistention
Second gauge of whether bladder is full: Uterine displacement and lack of contraction
Nursing care for Circulatory System changes
Diuresis 2-5d postpartum & blood loss at birth
happens so fast that BV returns to pre-preg in 1-2wks
bilateral ankle edema (shouldn’t go above knees)
Nursing care for Gastrointestinal System changes
bowel sounds active, BM slow bc of relaxin, difficult because of episiotomy/hemorrhoids
eat fiber, fruits, stool softener
Nursing care for Integumentary System changes
stretch marks
overstretching/separation of abs
modified ab exercises or surgery may be needed
Lactation
Lactogenesis II is often when the “milk has come in” , also known as engorgement and occurs from birth to 5-10 days postpartum; this is often termed “transitional milk.”
Postpartum Complication Warning Signs:
Respiratory: Pain in chest, difficulty breathing
Neurologic: Seizures, persistent headache, visual changes
Mental health: thoughts of hurting self or others
Infection: temp >100.4, edema/redness of lower extremities, incision not healing
Hemorrhage: Excessive bleeding, soaking through one pad/hr or larger than quarter size clots
CALL 911 + HEALTHCARE PROVIDER