Unit 2 Lesson 2 HCM Types and Hemodynamics
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
List the 2 ways HCM can be classified.
Anatomic description
Hemodynamic description
List the 4 anatomic descriptions of HCM.
Neutral
Sigmoid
Reverse curvature
Apical
List the 2 hemodynamic descriptions of HCM
Non-obstructive
Obstructive
Simple reminder:
HCM can be described by where/how the septum looks or by whether it obstructs flow.
List the 4 ventricular septal morphologies in HCM.
Neutral
Sigmoid
Reverse curvature
Apical
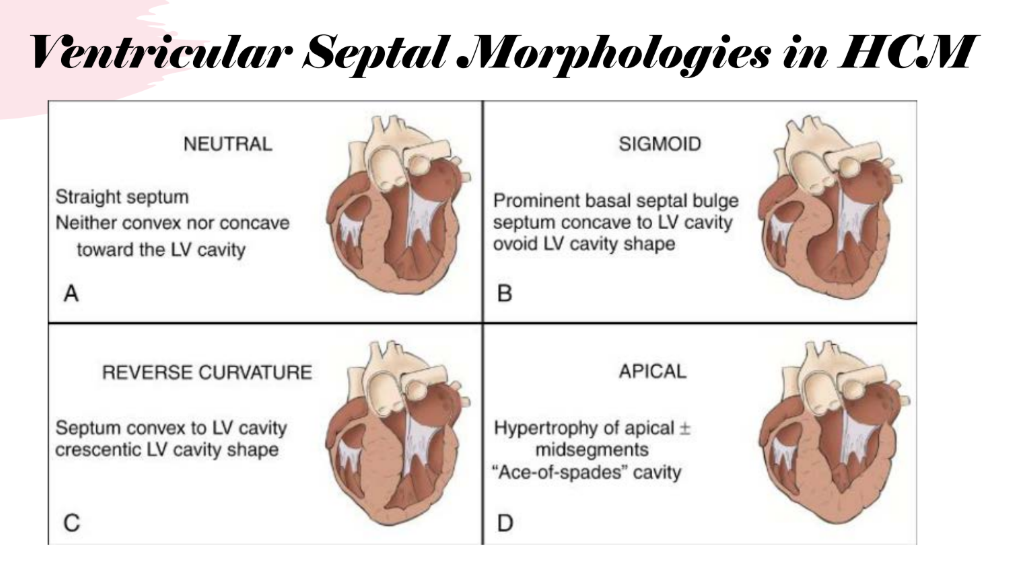
Describe neutral HCM morphology.
Neutral morphology has a straight septum that is neither convex nor concave toward the LV cavity.
Describe sigmoid HCM morphology.
Sigmoid morphology has a prominent basal septal bulge with the septum concave to the LV cavity, creating an ovoid LV cavity shape.
Describe reverse curvature HCM morphology.
Reverse curvature morphology has the septum convex to the LV cavity, creating a crescentic LV cavity shape.
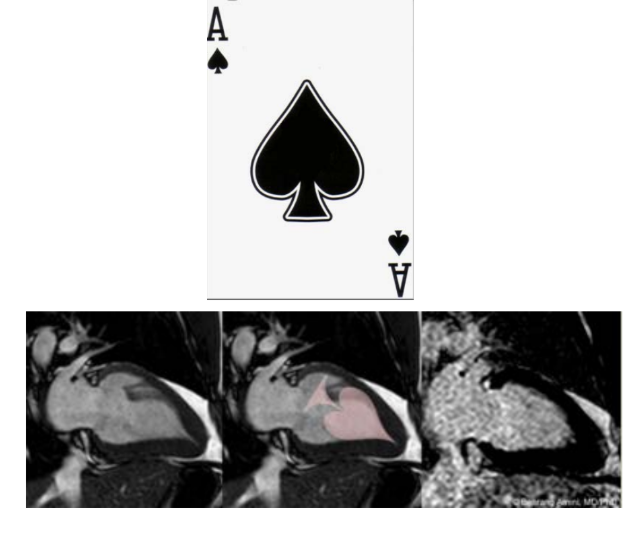
Describe apical HCM morphology.
Apical HCM has hypertrophy of the apical segments, creating an “ace-of-spades” cavity.
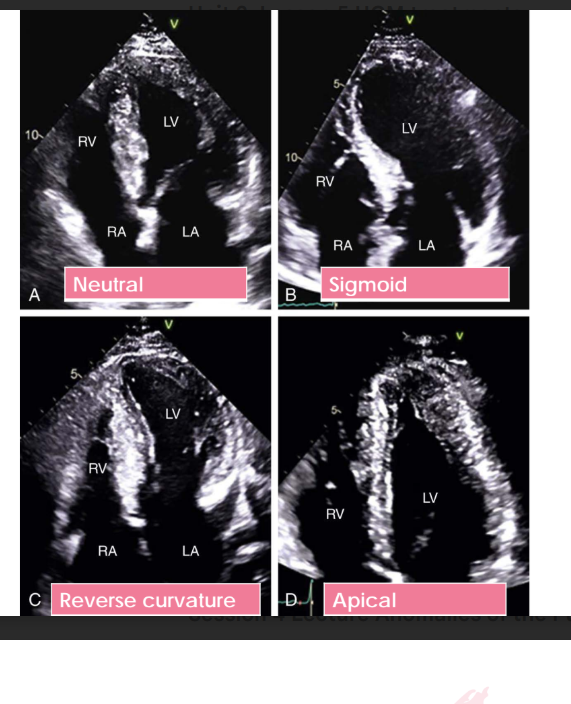
List the 4 HCM morphologies identified on echo images.
Neutral
Sigmoid
Reverse curvature
Apical
Simple reminder:
These are the same 4 anatomic forms from the prior slide, now demonstrated by echo examples.
What major classification is introduced after the anatomic descriptions?
The hemodynamic description of HCM.
Simple reminder:
Hemodynamic description focuses on whether HCM causes obstruction to flow.
Compare non-obstructive HCM and obstructive HCM by percentage and LVOT gradient.
Non-obstructive HCM makes up about 1/3 of HCM cases and has an LVOT gradient of <30 mmHg at rest or with provocation.
Obstructive HCM makes up about 2/3 of HCM cases and is defined as a peak LVOT gradient of >30 mmHg at rest or with provocation.
In obstructive HCM, how often is obstruction present at rest versus with provocation?
Of the obstructive cases, about 50% are present at rest and 50% arise with provocation.
What type of obstruction is rare in HCM?
Mid-ventricular obstruction is rare
High-yield numbers:
Non-obstructive: 1/3, LVOT gradient <30 mmHg
Obstructive: 2/3, LVOT gradient >30 mmHg
Obstructive cases: 50% at rest, 50% with provocation
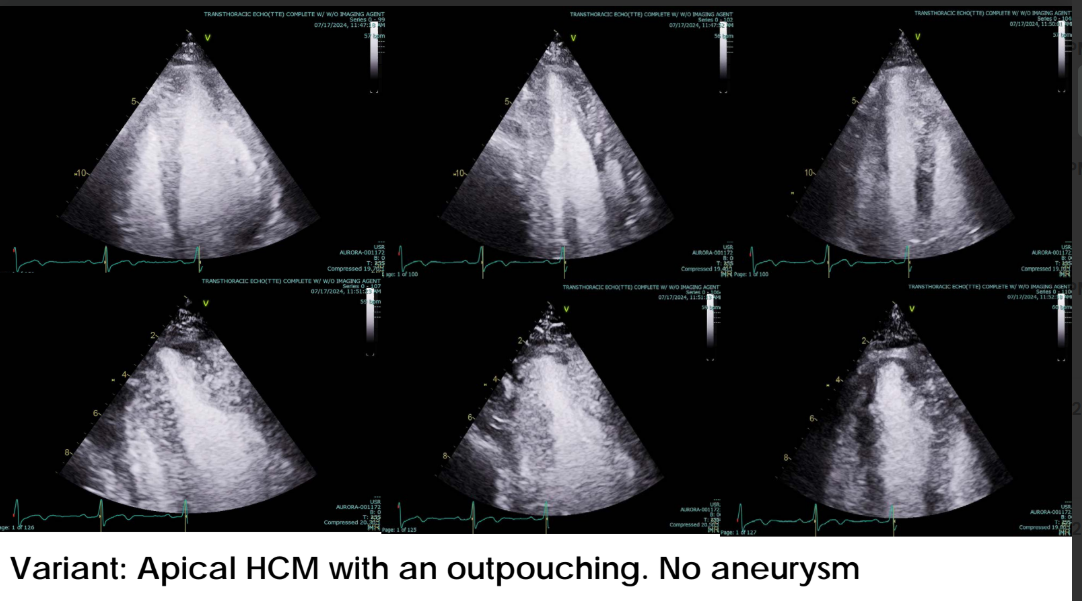
List the 3 apical HCM variants.
Asymmetric apical HCM
Apical HCM with an outpouching, no aneurysm
Apical HCM with apical aneurysm
What HCM category is introduced here?
Non-obstructive HCM.
List the 4 key features of hypertrophic non-obstructive cardiomyopathy.
No obstruction
Asymptomatic
Normal physical examination
Better mortality prognosis than other forms of HCM
Simple reminder:
Non-obstructive HCM means the heart muscle is thick, but there is no significant obstruction

What HCM variant is introduced here?
Asymmetric apical HCM.
List the 4 key features of asymmetric apical HCM.
Less common
Predominantly involves the LV apex
May demonstrate an apical “pouch”
Ultrasound enhancement agents, or contrast, may be useful in delineating the anatomy
Simple reminder:
Apical HCM mainly affects the LV apex, and contrast can help define the anatomy better.
List the 4 key features of apical HCM.
Asymmetric apical hypertrophy
Ace-of-spades appearance
Apical HCM
Usually no obstruction at rest
Simple reminder:
Apical HCM = thick apex + ace-of-spades LV cavity shape, usually without resting obstruction.
What area of the LV should you focus on with apical HCM?
The LV apex.
Define apical outpouching in apical HCM.
Apical outpouching is a persistent apical cavity dimension at end-systole that is greater than the midventricular cavity dimension at end-systole.
Simple reminder:
At end-systole, the apical cavity remains larger than the midventricular cavity
Define an apical aneurysm in apical HCM.
An apical aneurysm is a discrete, thin-walled dyskinetic or akinetic segment of the most distal portion of the chamber, with a relatively wide communication to the LV cavity.
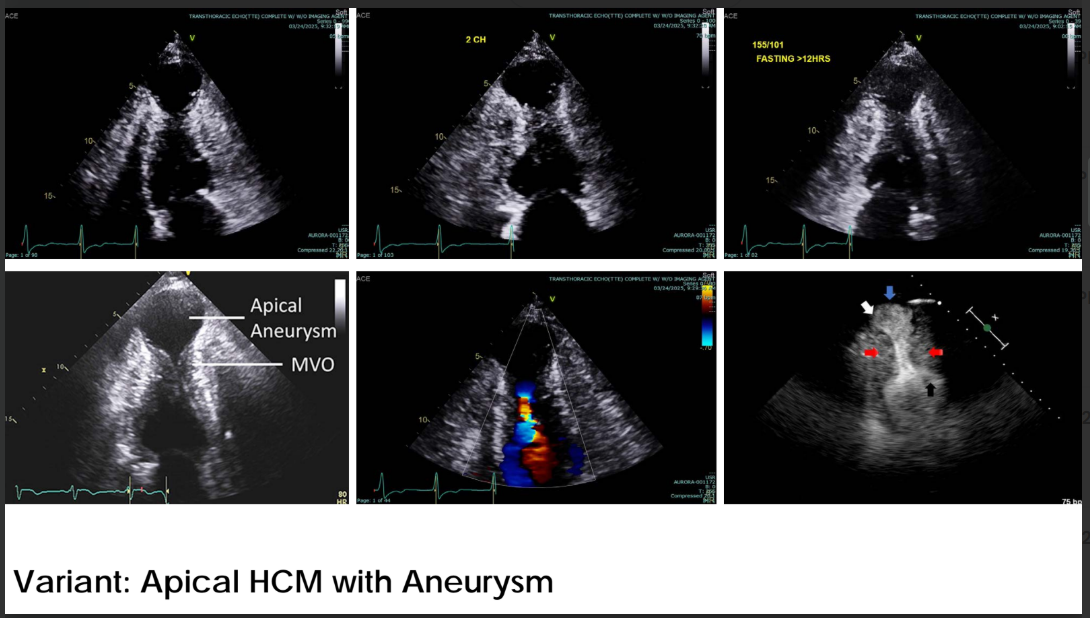
List the 4 defining features of an apical aneurysm.
Discrete segment
Thin-walled segment
Dyskinetic or akinetic segment
Wide communication to the LV cavity
Simple reminder:
Aneurysm = thin wall + abnormal motion + communication with the LV cavity.
List the 5 obstruction-related concepts in obstructive HCM.
Ventricular obstruction
Midventricular obstruction
LVOT obstruction
Eject-obstruct-leak
SAM
Explain ventricular obstruction in HCM and list the structures/patterns involved.
Ventricular obstruction is a general term meaning there is an obstruction somewhere in the left ventricle. It may be subaortic and can involve the mitral valve apparatus or the ventricular septum.
List the 4 septal patterns associated with ventricular obstruction
ASH
Reverse curvature
Sigmoid septum
Neutral
Simple reminder:
Ventricular obstruction means obstruction somewhere in the LV, often related to the septum and/or mitral valve apparatus.
Explain midventricular obstruction in HCM.
Midventricular obstruction occurs when hypertrophy in the midventricular segment causes narrowing, often due to septal hypertrophy meeting a hypercontractile LV free wall.
List the 4 key features of midventricular obstruction.
Hypertrophy in the midventricular segment
Septal hypertrophy meeting a hypercontractile LV free wall
Hypertrophied papillary muscle
Rare, occurring in approximately 1–10% of patients
High-yield reminder:
Midventricular obstruction is rare and occurs in about 1–10% of patients.
What causes LVOT obstruction in HCM?
LVOT obstruction is caused by an increased gradient through the LVOT due to anatomic abnormalities.
List the 5 anatomic abnormalities that can contribute to LVOT obstruction.
Basal septal hypertrophy
AMVL elongation
Mitral valve apparatus dysfunction
Anterior displacement of papillary muscles
Papillary hypertrophy
How do these abnormalities create LVOT obstruction?
Together with LV hypercontractility, these abnormalities narrow the LVOT and cause an elevated pressure gradient.
Simple reminder:
LVOT obstruction = narrowed outflow tract + increased gradient.
What is SAM, and why is it important in HOCM?
SAM stands for systolic anterior motion. It is the physiologic phenomenon involving the mitral valve apparatus and basal septal hypertrophy that causes LVOT obstruction.
List the 3 major concepts linked to SAM.
Venturi effect
E-O-L
Eject, obstruct, leak
Simple reminder:
SAM is when the mitral valve apparatus moves anteriorly during systole and contributes to LVOT obstruction.
Explain the Venturi effect in HOCM.
The Venturi effect is based on fluid dynamics. When blood passes through a narrowed orifice, velocity increases according to the Bernoulli principle, and static pressure decreases to conserve kinetic energy.
List the 3 key parts of the Venturi effect.
Fluid passes through a narrowed orifice
Fluid velocity increases
Static pressure decreases
Simple reminder:
Narrow opening → faster flow → lower pressure
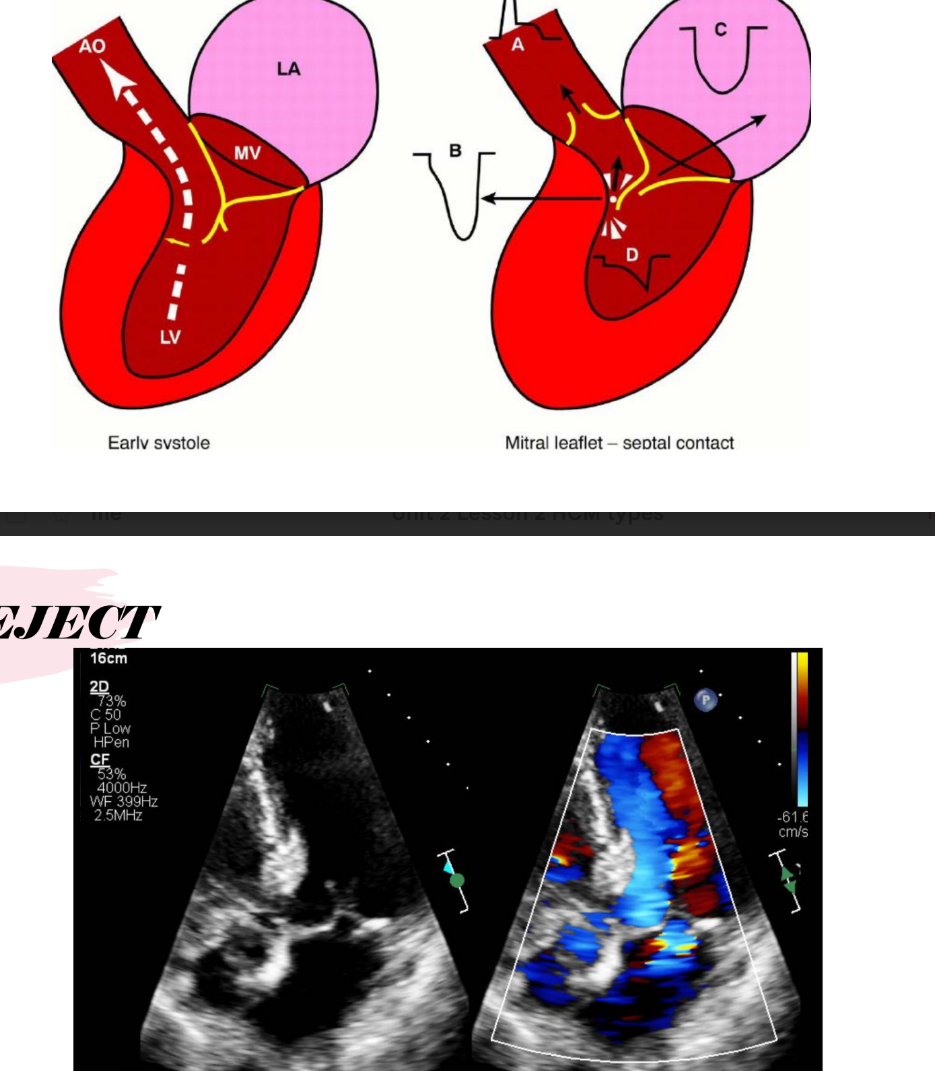
Explain the “eject” step of eject-obstruct-leak.
During early systole, blood ejects through a narrow LVOT, causing velocity to increase and pressure to decrease in the LVOT. This Venturi effect pulls the mitral valve apparatus into the LVOT.
List the 4 steps of the eject phase.
Early systolic ejection occurs
Velocities increase through the narrow LVOT
Pressure decreases in the LVOT
The mitral valve apparatus is pulled into the LVOT
Explain the “obstruct” step of eject-obstruct-leak.
The mitral valve leaflets or chordal apparatus move anteriorly toward the area of decreased pressure, causing LVOT obstruction.
List the 3 parts of the obstruct phase.
SAM of the mitral valve leaflets or chordal apparatus
Movement toward the area of decreased pressure
Obstruction in the LVOT
Explain the “leak” step of eject-obstruct-leak.
As the mitral valve apparatus or leaflet is pulled toward the LVOT, a gap forms between the anterior and posterior mitral leaflets during systole, causing mitral regurgitation.
List the 3 parts of the leak phase.
Mitral valve apparatus or leaflet is pulled toward the LVOT
A systolic gap forms between the anterior and posterior leaflets
Mitral regurgitation occurs
Simple reminder:
Eject → flow speeds up.
Obstruct → mitral valve moves into LVOT.
Leak → mitral leaflets do not close fully, causing MR.
What happens from early systole to mitral leaflet-septal contact?
During early systole, blood ejects through the narrowed LVOT. Then the mitral leaflet moves toward the septum, causing mitral leaflet-septal contact and obstruction.
What is happening during the eject phase?
Blood is being ejected through the LVOT, and flow velocity begins increasing through the narrowed outflow tract.
What phase of eject-obstruct-leak is demonstrated?
The obstruct phase.
What is happening during the obstruct phase?
The mitral valve apparatus moves into the LVOT, causing obstruction.
What is happening during the leak phase?
Mitral regurgitation occurs because the mitral leaflets do not close normally during systole.
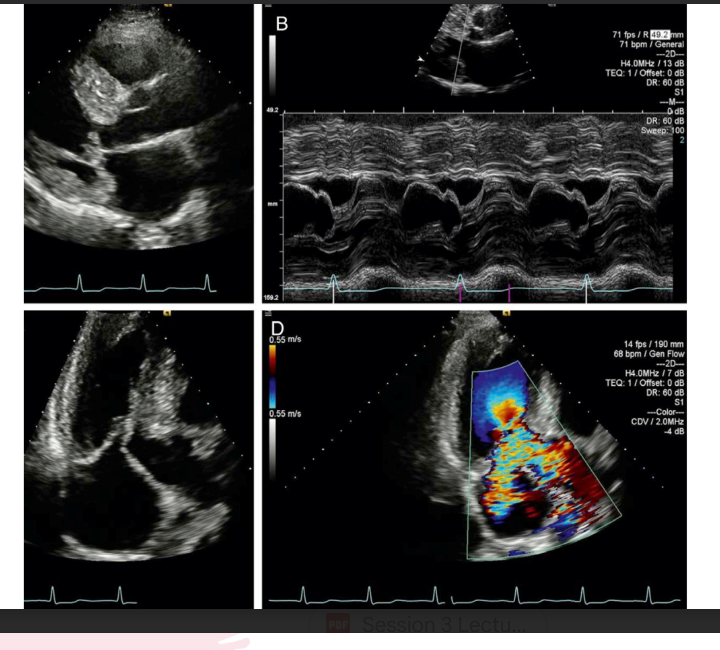
SAM pulls the mitral valve apparatus toward the LVOT, which creates obstruction and can also cause MR.