APK4125 C - Exam 3
1/257
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
258 Terms
What is the typical time period for a Mesocycle? Why?
4-6 weeks
The body responds best to 4-5 weeks of incremental stress
What is the typical time period for a microcycle?
One week
Within a meso cycle, what is changing? For what reason?
Only one variable will change (depending on the goal: duration, frequency, or intensity) per microcycle until the last 1 or 2 microcycles.
Designed this way to focus predominantly on one goal.
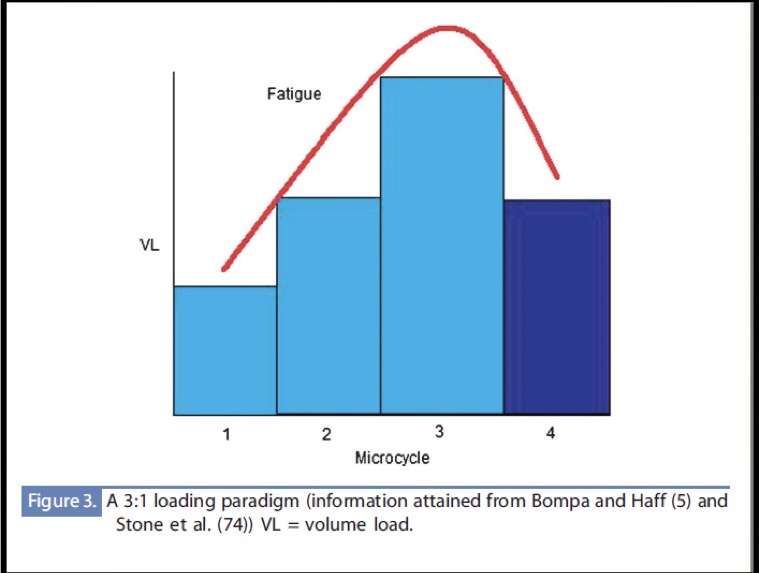
What is it called when we increase stress within a mesocycle, until the last 1 or 2 microcycles?
Loading:deloading
True or False: At the end of a mesocycle, we will change most variables (intensity, frequency, and duration).
True
Depending on the long-term goal of the client
What combination of intensity and frequency had the highest client adherence?
Moderate Intensity - High Frequency
What combination of intensity and frequency had the most changes (most beneficial)?
Hard Intensity and High Frequency
What does the frequency, intensity, and duration of the exercises we program depend on?
Goals (adaptations wanted) of the client
Initial health/fitness levels
Preferences
Time constraints
What adaptations normally increase with CV training?
Heart Volume
Hemoglobin
Stroke Volume
Cardiac Output
VO2 max
a-v O2 diff
Lung volume
Mitochondrial enzymes
Mitochondria
Fat oxidation
Strength of connective tissue
Heat acclimatization
HDL cholesterol
Mood/Mental State
Myoglobin stores
What adaptations normally decrease with CV training?
Resting HR
Resting BP
Body Fat
Total Cholesterol
LDL Cholesterol
Specific Chronic Disease Symptoms
Are central adaptations short term or long term?
Short term
Peripheral adaptations are long term
What CV training adaptations are central?
Anything pertaining to CO:
increase plasma volume
Increase stroke volume
Increase muscle pump
Increase respiratory pump
Increase venoconstriction
Increase contractility
How long after exercising do we see Central adaptations?
10-14 days
What CV training adaptations are peripheral?
Anything pertaining to the a-v O2 diff in the Fick’s equation (VO2 max = CO * a-v O2 diff):
Increase capillary number
Increase capillary recruitment
Increase mitochondria
Increase oxidative enzymes
Increase myoglobin
How long after exercising do we see Peripheral adaptations?
Over 12 weeks
Items to include in a program:
Specific Frequency, including the days (MWF, explains rest days)
Mode of Exercise
Relative Intensity (physiologic)
Either Absolute Intensity or another form of Relative Intensity (non-physiologic)
Duration
Microcycle Volume
Give examples of Relative Intensity (physiologic)
HR Reserve, percentage HR max, VO2 percentage
True or False: Relative Intensity can still be programmed for clients on medications that affect HR.
False:
Clients on medications that significantly influence HR, like Beta-blockers. Instead use modified Borg.
Give examples of absolute intensity
MPH, Watts, Kgm/min
Should be mode specific
Why do we normally prescribe absolute intensity to go with relative intensity (physiologic)?
Most clients aren’t familiar with their HRR at different intensities.
Absolute should only be used if acquired from testing though.
Examples of Relative Intensity (non-physiologic)
RPE, Modified RPE, OMNI scale, Talk test, Counting Talk test
Only prescribed if relative intensity can’t be prescribed, or absolute can’t be prescribed.
True or False: Relative Intensity (non-physiologic) is just as accurate as Absolute Intensity or Relative Intensity (physiologic)
False
Are the adaptations that occur for one patient at a given relative intensity the same for another patient at that same relative intensity?
No
Absolute intensities - are general measurements of intensity that apply to anyone.
Relative - specific to person and will illicit different absolute intensities.
The ACSM guidelines prescribes ranges of intensity and duration. Should we prescribe our patients ranges for relative or absolute intensities?
No
Acceptable range is plus or minus 5 of the specific number we want them to be at.
We give this plus or minus, so that patients aren’t too strict on the number since they normally fluctuate slightly.
Exercise mode, or type, is primarily prescribed based off …?
The goal of the client
Preference
Health and physical ability
For patients with a goal of “losing weight”, what type of exercises will we prescribe?
Those that burn the most amount of kcals, so more muscle mass that is involved.
True or False: Intermittent exercises, like HIIT or stop-and-go sports, may be used to accumulate the recommended frequency, intensity, and time needed for cardiorespiratory fitness.
True
Rank these exercises from least to most complex:
Running
Basketball
Indoor Cycling
Jumping Rope
3<1<4<2
Type A: Indoor cycling, walking, aqua-aerobics, and slow dancing
Type B: Jogging/running, rowing, stair climbing, hiking, nordic skiing, elliptical training, and spinning
Type C: Aerobic dancing, step aerobics, in-line skating, nordic skiing, jumping rope, simulated climbing, and fast dancing
Type D: Basketball, downhill skiing, handball, racket sports, swimming
True or False: All modes are equal feeling of intensity for everyone, which is why we use RPE to determine effort/difficulty.
False
We prefer HR over RPE, bc each individual will have varying RPE’s per mode.
Describe Borg’s RPE and modified RPE and how they are tied to cardiovascular training?
Borg’s RPE scale goes from 6-20, which correlates perceived exertion with HR by multiplying HR by 10. For a 20 y/o.
Ex. Someone perceives they are at an intensity of 12 and their HR is 120. (Makes sense)
Borg’s modified RPE scale goes from 1-10, and correlates perceived exertion with % of HRR.
Ex. Someone who perceives they are at an intensity of 6 and their HRR is 60%.
What influenced RPE?
Medications
Age
What is it called when someone perceives their intensity is at 16 on Borg’s RPE, but their heart rate is 120? What are some thing that could cause this sense of heightened intensity?
They are not perceiving intensity correctly. They are overestimating their exertion/activity.
Other reasons they may have a lower HR is use of medication like Beta-blockers. Or it feels more intense because they feel pain or exertion from other systems not CV. (Soreness from resistance training etc).
What is it called when someone perceives their intensity is at 12 on Borg’s RPE, but their heart rate is 160? What are some things that could cause this sense of heightened HR?
They are misperceiving their intensity. They are underestimating their intensity.
Reasons: stimulants like caffeine, illicit drugs, or ADHD med like adreall.
Which type of muscle fibers has a higher lactate threshold?
Type 1 - less fatiguing
Describe lactate threshold
The point at which we can no longer remove lactate fast enough so it does not accumulate.
It is a sign that we are using glycolysis as our energy system, since pyruvate is a byproduct of glycolysis that is converted to lactic acid.
A combination of these things leads to an increase in lactate?
Low muscle oxygen
Accelerated glycolysis
Reduced rate of lactate removal
Recruitment of Type II muscle fibers
True or False: We can easily measure lactate threshold during exercise sessions.
False
There is no easily assessable way to monitor lactate threshold during exercise sessions, but lactate levels largely dictate how a client feels during exercise.
How do we measure lactate threshold then?
As a % of VO2 max
What are the five training sessions and what do they represent?
Overdistance - regenerative/low-intensity endurance training
Endurance - aerobic threshold (metabolic event #1) - Onset of Blood Lactate Accumulation (OBLA)
Tempo - moderate/sweet spot endurance training
Lactate Threshold - Maximal Lactate Steady State (MLSS) or anaerobic threshold (metabolic event #2)
VO2 max - interval training sessions
Is the OBLA or MLSS associated with the heart rate deflection point (HRDP)? What does that mean?
MLSS
HRDP - HR plateaus. Client won’t be able to maintain that pace for much longer.
MLSS is also associated with ventilatory threshold/
True or False: We can estimate MLSS directly from HR during GXT.
True
MLSS = HRDP
How does exercise affect these phases of training?
Graph will be shifted due to the adaptations leading to - high intensity needed before reaching OBLA and MLSS.
For the general public, lactate threshold is around 60-70% of VO2 max. For de conditioned individuals, lactate threshold is around 40-45% VO2 max.
How long do changes in lactate threshold normally take?
At least 8 weeks, but normally months. They are metabolic changes.
First couple of weeks we see small changes from SV improves as plasma volume increases, and mechanical efficiency.
Why do we prefer to use HRR instead of HR max when prescribing CV training?
HR will respond to factors like dehydration, fatigue, and stimulants.
HRR incorporates client’s resting HR and the autoregulatory nature of HR.
Percentage of heart rate reserve (% HRR) is considered to have a ____ to ____ relationship with VO2 max reserve.
1 to 1
How is HRR calculated?
HR matching HRR = (max HR - resting HR) * Desired Intensity + resting HR
% of HRR does not add back the resting HR.
What do we need to calculate kcal expenditure using HRR reserve?
VO2 reserve
1 MET =
3.5 mL/kg/min
Describe the talk-test
Very general intensity monitor based on how easily you can speak while exercising.
Client recites a standard phase, often the Pledge of Allegiance.
Light intensity: Can speak the full sentence comfortably without getting out of breath.
two sentences w/o getting out of breath
Moderate intensity: Need to pause occasionally to breathe while speaking
Between 2 words and 2 sentences
Lactate threshold is considered to be in between moderate and vigorous.
Vigorous intensity: Can only say a few words before needing to stop for breath
Only 2 words
Describe the counting talk test
Slightly more structured version of the talk test used to estimate exercise intensity:
The person takes a maximal breath in, then counts out loud at a normal speaking pace (“1-one thousand, 2-one thousand…”) until they need another breath
They should not hold their breath at any point
How it’s used:
First, determine the maximum number they can count to at rest or baseline
Then prescribe exercise intensity based on a percentage of that number during activity.
The lower the percentage (# of sec when exercising/# of sec at rest) = the more intense the workout.
Key points:
It has high validity, showing a strong correlation with % heart rate reserve (r = -0.92)
However, it’s more accurate but less practical, since it can be fatiguing and harder for clients to use continuously during exercise.
Normally used in a group setting.
With which population would we use Borg’s RPE for relative intensity (non-physiologic)?
Younger population (since max HR is 200 - matches RPE max of 20), if used in testing as well.
How do we use modified Borg’s RPE with patients during CV training, as a relative intensity (non-physiologic) measure?
Compare % of HRR in multiples of 10 with modified Borg’s RPE.
If we want them to go at a 60% HRR, we say 6 on the modified Borg scale.
Do we typically use OMNI RPE Scale to prescribe intensity?
No, unless person cannot asses their intensity level.
Do we typically use METs to prescribe intensity?
Not as useful
Technically classified as an absolute measure of intensity
METs are more used in retrospective to try to calculate kcals burnt without HR.
Which medications don’t affect BP nor HR?
Lipid medications
NSAIDs
Antidepressants (if small dosages)
Antihistamines
Hypothyroid agents
Weight-loss agents
Which medications reduce HR?
Beta-blockers
Calcium-channel blockers
Antiarrhythmic agents
Which medications increase HR?
Vasodilators
Antidepressants (depends on dosage)
Stimulants like ADHD medications or caffeine
What medication requires us to use other method than HRR because HR reductions are significant up to 30 bpm for submaximal efforts?
Beta-blockers
Technically also Antiarrhytmic agents, but not as common.
In that case, we would use modified RPE. Max percentage HRR - 50%
What is/are the factors that affect HR max?
Only Age
True or False: We should always ask clients/patients if they have taken their medication correctly before exercising or GXT?
True
What are the ACSM guidelines recommendations for frequency?
5 days of moderate intensity
Or
3 days of vigorous intensity
What do the ACSM guidelines consider Vigorous intensity?
60-85% HRR
Anything over 85% is considered max training.
What do the ACSM guidelines consider Moderate intensity?
40-59% HRR
What do the ACSM guidelines consider light intensity?
30-39% HRR
What are the ACSM guidelines recommendations for time/duration?
Moderate intensities: 30-60 minutes (totaling 150 minutes or more per week)
Vigorous intensities: 20-60 minutes (totaling 75 minutes or more per week)
Less than 20 minutes may still be beneficial for sedentary individuals.
What are the ACSM guidelines recommendations for mode?
Rhythmic aerobic exercises involving large muscle groups
True or False: We don’t want the client to go past lactate threshold during vigorous intensity workouts, but they can get close.
True
Fatigue too quick if they do
How are MET-min/week calculated?
MET x total mins that week
What are the ACSM guidelines recommendations for exercise volume?
500-1000 MET-min/week
Achieve at least 7,000 steps
What is the ACSM suggestion for rate of progression?
Increase duration across microcycles, not intensity which could lead to failure to adhere.
“Initiate exercise at a light-to-moderate intensity in currently inactive individuals and then increasing duration as tolerated is recommended. As increase in exercise duration per session of 5-10% weekly every 1-2 weeks over the first mesocycle of a training program is reasonable for the average adult. “
ACSM says 5-10 minutes weekly, but Dr. Gordon said general rule of thumb is 5-10%.
Avoid increasing multiple variables (FITT) at the same time per microcycle.
How can we find the percentages of HRR that match each phase of CV training?
Endurance: add or subtract 2.5% from the OBLA
Lactate threshold: add or subtract 2.5% from the MLSS
Tempo: between the Endurance and the Lactate threshold %s
Endurance: 40 until the OBLA
VO2 max: anything above the MLSS
How do we decide what phase of training our client should be in?
Match it to their specific performance goal.
Takes at least 16 weeks (4 months) to train it, and we build a macrocycle around the comp.
True or False: Macrocycles for endurance athletes or clients with aerobic goals are normally focused on one major event.
True
A race or a racing event.
To use this style of training the participant must have
a performance goal, and they must have at least 4 months to train before the goal date.
What trends do we see for intensity and volume over time with CV training? (Progression)
Intensity increases
Volume decreases
How does amount of time spent in Over-distance training change across the Preparatory - Pre-competition - Taper - Competition - Transition phases?
Prep - 60%
Precomp - 55%
Taper - 55%
Comp - 55%
Transition - 85%
How does amount of time spent in Endurance training change across the Preparatory - Pre-competition - Taper - Competition - Transition phases?
Prep - 30%
Precomp - 25%
Taper - 25%
Comp - 20%
Transition - 5-10%
How does amount of time spent in Tempo training change across the Preparatory - Pre-competition - Taper - Competition - Transition phases?
Prep - 5%
Precomp - 5-10%
Taper - 5-10%
Comp - 5-10%
Transition - 0-5%
How does amount of time spent in Lactate-Threshold training change across the Preparatory - Pre-competition - Taper - Competition - Transition phases?
Prep - 5%
Precomp - 10-15%
Taper - 10-15%
Comp - 5-10%
Transition - 0%
How does amount of time spent in VO2 Max training change across the Preparatory - Pre-competition - Taper - Competition - Transition phases?
Prep - 0%
Precomp - 0-10%
Taper - 2-5%
Comp - 0-5%
Transition - 0%
Describe the goals for training in OverDistance
Creation of an aerobic base (improving submax VO2 primarily a-v O2 diff):
creating mitochondria
Mitochondrial enzymes
Capillaries
Myoglobin
Increases stroke volume
Improving fat utilization with corresponding glycogen sparing
Describe the goals for training in Endurance phase
Creation of an aerobic base (improving submax VO2 primarily a-v O2 diff):
creating mitochondria, mitochondrial enzymes, capillaries, myoglobin, increasing stroke volume, and improving fat utilization with corresponding glycogen sparing.
Doing all of this with the presence of lactate accumulation
Describe the goals for training in Tempo phase
Improvement of mechanics at this pace
A shifting of the lactate threshold
An improved buffering capacity of lactate.
Describe the goals for training in Lactate Threshold phase
Improvement of mechanics at this pace
A shifting of the lactate threshold
Improvement in Anaerobic capacity
An Improved tolerance of intensity
Describe the goals for training in VO2 max phase
All-out performance
Improvement of mechanics at this pace
Improve tolerance of intensity
Increase in ability to perform at all out intensity
What do each of the variables of training (FITT) depend on?
F - depends on the cycle of training (or mesocycle)
I - dependent on MLSS and OBLA
T- time: depends on the overall goal
T - type: depends on the overall goal
Which phase(s) normally has the longest duration exercises?
OverDistance and Endurance
True or False: Clients in the OverDistance or Endurance phases may incorporate sessions longer than their goal. For example, if their goal is to run a 5k, they might train for 60 minutes, even if their 5k time is shorter than 60 mins.
True
True or False: Clients in the Tempo and Lactate Threshold phase will typically have sessions a little shorter than the goal race.
False:
Tempo - always be shorter than the goal race
Lactate threshold - will never go over half of the length of any goal race.
The duration of the VO2 max sessions must always be less than _____ minutes.
15
Roughly ____% of total time before event is spent in the preparatory phase.
75
What is the main goal of the preparatory phase?
Increase volume of daily exercise to levels higher than goal distance
Roughly ____% of total time before event is spent in the pre-competition phase.
20
What is the main goal of the pre-competition phase?
Increase intensity to levels higher than enough for competition
Roughly ____% of total time before event is spent in the taper phase.
5
What is the main goal of the taper phase?
Allow the body to fully recover before competition
Why do we not include a competition or transition phase for most clients using these phases of training?
When would we use them?
Client’s performance goal is one event.
We would use them if training a professional athlete who has a season and wants to continue to improve for next event. Transition phase would be used for one mesocycle after the goal competition, in this case.
Calculations: Provide the conversion factors for the following:
METs to MET-min
Relative VO2 to METs
Units for Relative mL/kg/min
Absolute VO2 to Relative VO2
Units for Absolute = L/min
Absolute VO2 to Kcal/min
Kcal/min to total Kcal spent
Relative VO2 to % of VO2R(eserve)
Resting VO2 given or assumed to be 3.5 mL/kg/min
% of VO2 R to % of HRR
% HRR to modified RPE
% of HRR to HR
HR max given or assumed to be 220-age
HR to % HR max
HR to RPE
METs * total mins = MET-min
Relative / 3.5 mL/kg/min = METs
Absolute * 1000/BW (in kg) = Relative
Absolute * 5kcal/L = kcal/min
Kcal/min * min = total kcal
(Relative - resting) *100 / (VO2 max - resting) = % of VO2R
% of VO2 R = % of HRR (1-to1 relationship)
modified RPE * 10 = % of HRR
(% of HRR * HR max-resting HR)/100 + resting HR = HR
HR/HR max = % of HR max
RPE*10 = HR
One training variable should be increased continuously during a mesocycle until the deload week. What variable do we increase using preparatory vs precompetition?
Preparatory we increase volume.
Pre-competition we increase intensity.
What factors of muscular fitness are health-related goals?
Muscular strength and Muscular Endurance