unit 2 Ventricular Septal Defects
1/93
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
What is a VSD?
A VSD is a communication between the left and right ventricles or between the left ventricle and right atrium.
List the 5 key facts about VSDs.
How common is a VSD in newborns
it can be _____ 20-30% or with ____
found with what other defects name 4
Defects are named according to _____
VSD is the most common congenital heart defect in newborns.
It can be isolated in 20–30% of cases.
It can occur with other congenital heart defects.
It is found with Tetralogy of Fallot, double outlet right ventricle, truncus arteriosus, and common AV canal defects.
Defects are named according to location.
Why is echo important in VSD evaluation?
Echo is the mainstay for ________ _______, direction of ________ _____, and determining the approach for ________.
Echo is the mainstay for clinical diagnosis, direction of clinical care, and determining the approach for intervention.
List the 3 things needed to evaluate a VSD properly on echo'
Full understanding of ______ anatomy
relationship of the ______to other _________
The impact on __________
Full understanding of septal anatomy
Relationship of the VSD to other anatomy
Hemodynamic impact
List the 2 main regions of the ventricular septum is divided into
Membranous
Muscular
List the 3 muscular septal regions.
Inlet
Outlet
Trabecular/muscular
Which septal region is the most anterior and superior portion of the septum?
The outlet septum.
List the 3 valves that determine the borders of the septal regions.
Tricuspid valve
Pulmonic valve
Aortic valve
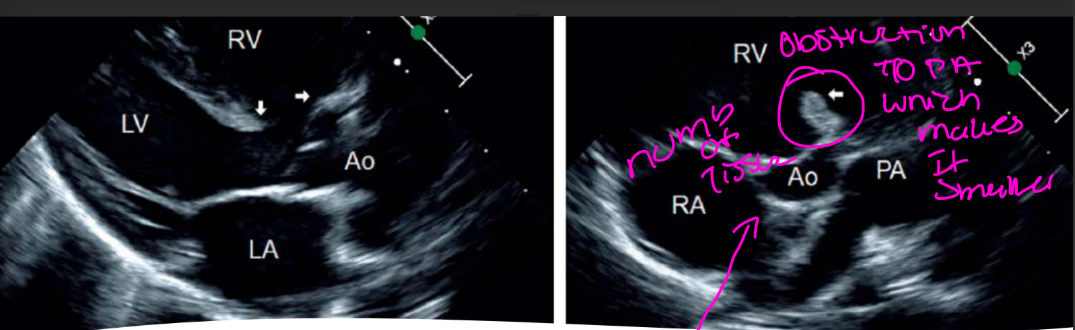
List the 2 fundamental types of VSDs.
Deficiency of tissue
Malaligned septal components
How can tissue-deficiency VSDs occur?
They can be congenital or acquired after myocardial infarction.
Where can VSDs occur within the septum?
They can occur within ____portion of the septum or _____across _____portions of the septum.
They can occur within one portion of the septum or extend across multiple portions of the septum.
List the 5 types of VSDs.
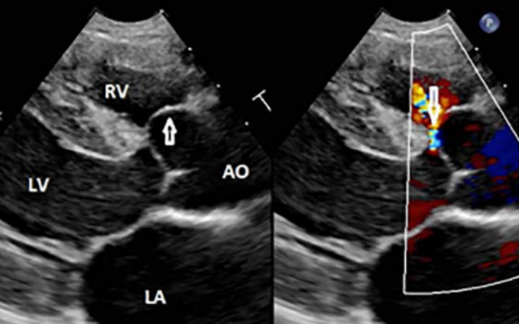
Perimembranous
Inlet
Muscular
Outlet / doubly committed VSD
Malalignment
List the 6 key features of perimembranous VSDs
They make up about what %
How common is this VSD, who is it the most common in ? (newborns or Adults)
How does this VSD occur? caused by failure of the…….
where is this VSD located ?
Adjacent to which valve?
may affect leaflets of which valves name 2
They make up about 80% of VSDs.
They are the most common type of VSD. in Adults
They are caused by failure of the membranous septum to develop.
They are located just beneath the right and non-coronary cusps of the aortic valve.
They are adjacent to the tricuspid valve.
They may affect the tricuspid valve leaflets and aortic valve leaflets.
Can perimembranous VSDs spontaneously close?
No, they cannot spontaneously close.
(The septum is formed by bulbar ridges, endocardial cushions of the ventricular septum, they cannot spontaneously close due to the type of tissue its made of)
List the 2 valve problems that perimembranous VSDs can cause.
Tricuspid septal leaflet distortion with tricuspid regurgitation
Aortic valve prolapse with aortic regurgitation
Tricuspid valve distortion means the tricuspid valve’s normal shape or position is being changed or pulled out of place.
With a perimembranous VSD, the defect is very close to the tricuspid valve. Tissue around the opening can pull on the valve or make part of the valve bulge toward the defect.
How can the tricuspid valve be affected by a perimembranous VSD?
The VSD may be restricted by tricuspid septal leaflet tissue, which can cause tricuspid septal leaflet distortion and tricuspid regurgitation.
That means the septal leaflet of the tricuspid valve partly covers the VSD, making the opening smaller.
So instead of blood flowing freely through a large hole, the tricuspid valve tissue acts like a flap over it and restricts the amount of shunting.
Simple way to remember:
Restricted by tricuspid septal leaflet tissue = tricuspid valve tissue partially blocks the VSD.
This is also why some perimembranous VSDs can appear smaller over time, even though the membranous tissue itself does not grow closed.
How can the aortic valve be affected by a perimembranous VSD?
Due to the close proximity of a perimembranous VSD to the Aortic valve,
the Aortic Valve may prolapse into the VSD leading to aortic regurgitation
Which aortic cusps are affected with aortic valve prolapse?
The right or non-coronary cusps
Which type is aortic valve prolapse more common with Perimembranous VSDs?
It is more common with subaortic defects.
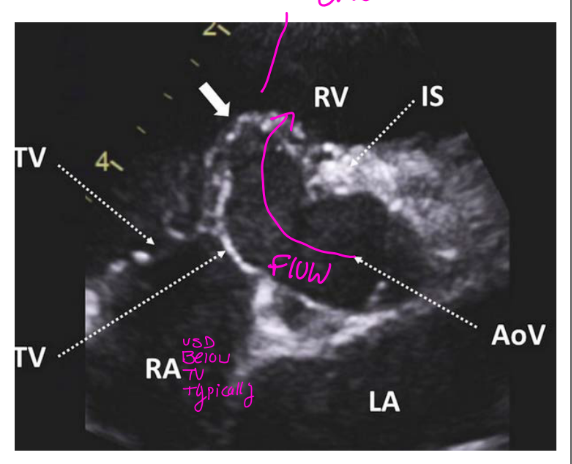
What is a Gerbode defect?
A Gerbode defect is an LV-to-RA communication, where blood travels from the LV through the VSD, across the tricuspid valve, and into the right atrium
List the 6 key facts about Gerbode defects.
what type of shunt / communication is this?
Gerbode defects may look like ____ (and what is the cardiac cycle is this in?)
They are mistaken for what?
what evaluation will help differentiate
Gerbode defects leads to what list 3
What part of the cardiac cycle is the VSD?
It is an LV-to-right atrial shunt / communication (LT to RT shunt)
It can look like tricuspid regurgitation. (TR is Holosystolic)
It may be mistaken for ruptured sinus of Valsalva.
Timing of blood shunting helps differentiate it.
It can cause RA enlargement and eventually RV dilation from increased preload
VSD are Holosystolic******
Simple reminder:
Gerbode = LV → RA shunt, not regular TR.
List the 3 key facts about muscular VSDs.
they make up what % of VSDs, this VSD is more common in who and why?
They are caused by what?
They are classified by _____location.
They make up 5–20% of VSDs. are more common in neonates b/c they spontaneously close
They are caused by extensive cavitation of myocardial tissue during IVS and ventricular wall formation.
They are classified by septal location.
It means that while the interventricular septum (IVS) and ventricular walls are developing, too much heart muscle tissue breaks down to form spaces.
Normally, small spaces form in the developing muscle and then join together correctly. If there is too much cavitation, some spaces remain open and create holes in the muscular septum.
Simple definition:
Too many spaces formed in the developing heart muscle, leaving one or more muscular VSDs.
This is often used to explain multiple muscular VSDs, sometimes called a “Swiss cheese” septum.
Cavitation = formation of spaces/holes in the developing myocardium.
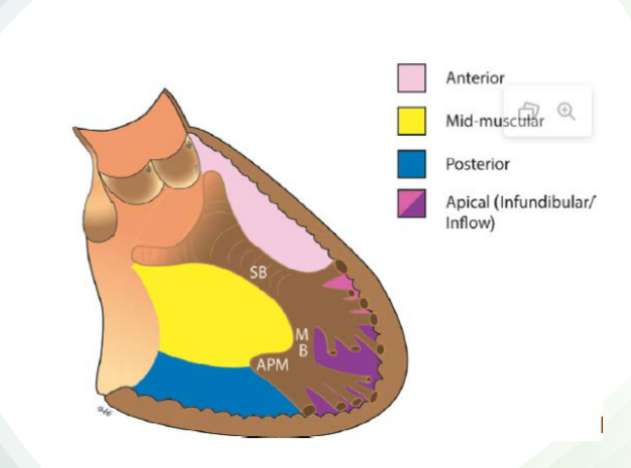
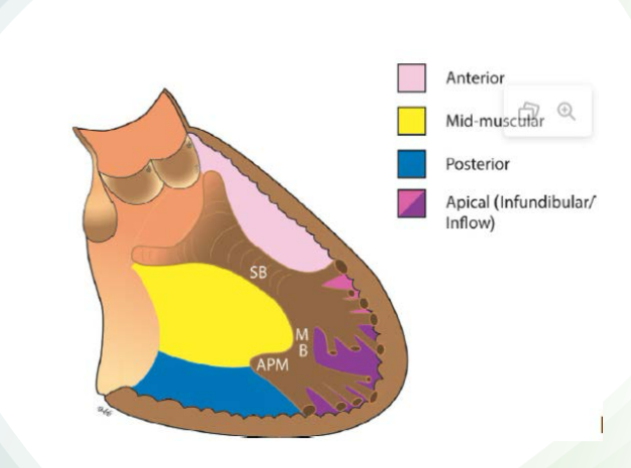
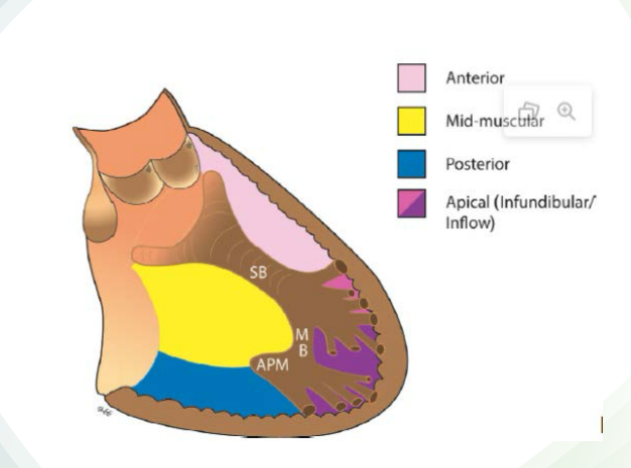
List the 4 muscular VSD locations.
Anterior
Mid-muscular
Posterior
Apical
Where should you sweep to assess an anterior muscular VSD?
Sweep up toward the aortic valve.
Muscular VSDs Classified on septal location:
for Mid-muscular what view helps?
PSAX helps
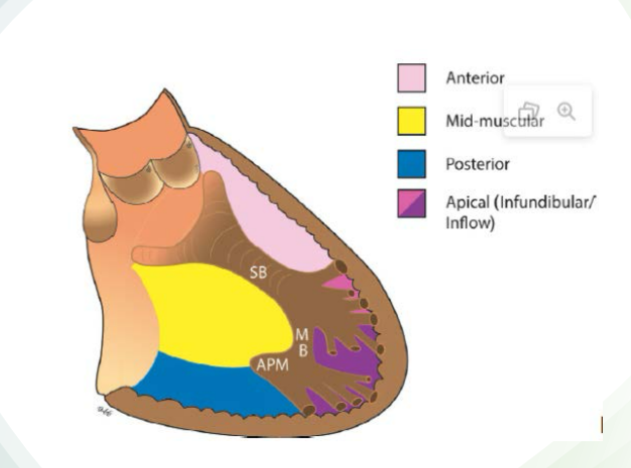
Where should you sweep to assess a posterior muscular VSD?
Sweep back toward the coronary sinus.
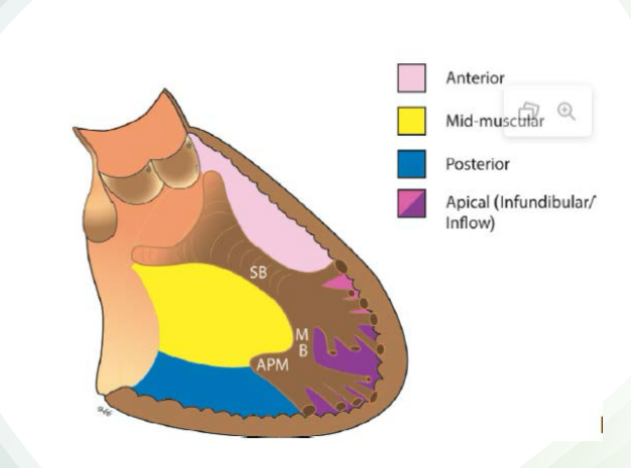
Muscular VSDs Classified on septal location:
where are Apical muscular defects located?***
Apical muscular defects are located below the moderator band***
List the 5 additional features of muscular VSDs.
can be a what defect (think how many list 2 results) for one list what the nickname its called?
May have a muscular VSD with a ^^^^
can be very ____ (what size)
Can they spontaneously close?
Imaging depends on _____of the VSD
They can be single or multiple.
Multiple muscular VSDs are called “Swiss cheese.”
A muscular VSD can occur with a VSD in another location.
They can be very small.
They may close spontaneously.
Imaging depends on the VSD location.
It means the patient can have more than one VSD:
one muscular VSD in the muscular part of the septum
another VSD in a different area, such as a perimembranous, inlet, or outlet VSD
Simple version:
A muscular VSD may occur by itself, or it may be present along with another type of VSD somewhere else in the septum.
List the 5 key facts about traumatic VSDs.
where do they occur? (what portion of the septum)
They are typically near the ____
how is it caused by name 2
Injury can be ____or occur when post injury
they have what outcome
They occur in the muscular portion of the septum.
They are typically near the apex.
They can be caused by a direct blow to the chest.
They can be caused by myocardial infarction.
Injury can be instant or occur 2–6 days after injury.
They have a poor outcome.
List the 6 key features of inlet VSDs
they make up what % of VSDs?
How/ why do they occur?
where is it located, which leaflet?
They are seen with what defects
^ what level - associated with what ?
where are they best imaged from list 2
They make up 5–8% of VSDs.
They are a deficiency of tissue in the inlet portion of the ventricular septum.
They are inferior and posterior to the septal leaflet of the tricuspid valve.
They are seen with AV canal defects. (so they are not isolated)
The AV valves are at the same level associated with trisomy 21, it can be part of a transitional defect or a complete defect, and how we know we are looking at a AV canal defect espically a big complete one our valves will be at the same level)
They are best imaged from subcostal 4-chamber or PSAX ventricle level inferior septal wall , and really close to the MV / slightly pass it bc inlet vsd belongs to the TV but remeber the TV sits apical inferior or apically displacemnet of the TV then the MV
(in order you will see what first is membranous first then muscluar, then inlet VSD in terms in order)
List the 4 associations/features of inlet VSDs.
Inlet VSDs may be formed by what list 2
what attachments is inlet VSD associated with list 2
mostly which valve is involved?
what is also assoicated with list 2
They may form from malalignment of the atrial and ventricular septa.
They are associated with straddling and/or overriding of tricuspid valve attachments.
The tricuspid valve is mostly involved.
They are associated with AV canal defect and cleft mitral valve.
Look at the tricuspid apparatus to determine whether the tricuspid valve is overriding the ventricular septum or whether the chordae tendineae and papillary muscles are straddling it.
To assess this, line up the ventricular septum with the tricuspid valve annulus. Overriding refers to the tricuspid valve annulus extending over the ventricular septum, while straddling refers to the chordae tendineae or papillary muscles attaching across the ventricular septum.
Remember, this is not typically a concern with the mitral valve because the mitral valve does not normally have attachments to the ventricular septum.
List the 6 key features of outlet VSDs.
They make up what % of VSDs.
they are also called
what O'clock are they located between?
where are the located at?
what does this VSD Communicates with?
Occurs more frequently in the ____population (30%)
They make up 5–7% of VSDs. (rare)
They are also called doubly committed subarterial VSDs. (bc of the loaction)
They are located between noon and 2 PM.
They are located anterior to the membranous septum. And they are below the pulmonic and aortic valves.
They communicate with the RV outflow tract.
They occur more frequently in the Asian population, about 30%.
List the 4 names/descriptions used for outlet VSDs.
Subpulmonic/subaortic
Doubly committed VSD
Malalignment VSD
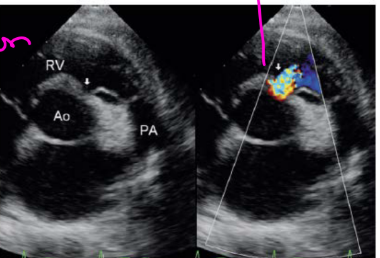
Where is an outlet VSD seen on echo? list 4 views, and decribe where you see the defect for two views
It is seen in PLAX under the aortic valve and in PSAX between the pulmonic and aortic valve. and A5C and A3C
List the 4 key facts about subarterial VSDs. (outlet VSD)
They are highly associated with what about what %
involves what?
they are asoicated with what?
May be seen in combination with what VSDs
They are highly associated with aortic valve prolapse, about 60–70%.
They are associated with aortic insufficiency.
They may be seen with malalignment VSDs.
(ventri effect)
Which aortic cusp is involved in subarterial VSD?
The right or non-coronary aortic cusp.
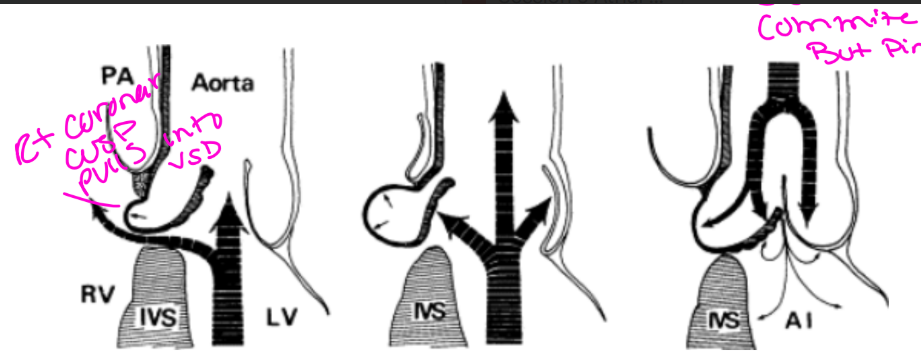
What is a malalignment VSD?
A malalignment VSD occurs when there is a lack of….
A malalignment VSD occurs when there is a lack of alignment between the outlet septum and trabecular septum.
Malalignment VSD:
What does anterior deviation of the septum create, as seen with what defects list 2
and explain how it affects the great arteries?
If the septum has an anterior deviation creates an overriding aorta, as seen with Tetralogy of Fallot and pulmonary stenosis.
Makes the Aorta BIGGER and the PA is SMALLER (thats why you’ll see PS)
Malalignment VSD:
What does posterior deviation of the septum create ____ assoicated with what list 2?
How does this affect the great arteries?
If the septum has a Posterior deviation creates a VSD associated with interrupted aortic arch and narrowing of the LVOT.
Makes the aorta SMALLER, and Rvot/ PA is BIGGER
(posterior = closer to LA)
List the 3 conditions associated with anterior deviation malalignment VSD.
Truncus arteriosus
Tetralogy of Fallot
Double outlet right ventricle
List the 3 conditions associated with posterior deviation malalignment VSD.
Interrupted aortic arch***********
Coarctation of the aorta
Double outlet left ventricle
Explain the basic pathophysiology of a VSD.
explain what it is - the type of communcation, how blood usually flows how? blood flow through VSD is ejected during what cardiac cycle and squeezed stright into where?
A VSD is a hole between the left and right ventricles.
Blood usually flows left-to-right, (from the LV to the RV.)
Blood flow through VSD is ejected in systole and squeezed straight into the pulmonary artery.
List the 3 major pathophysiologic effects of a VSD. what does it leads to - the affects on the heart?
Left ventricular volume overload
Excessive pulmonary blood flow
Pulmonary hypertension
Simple reminder:
VSD = extra blood goes to lungs → extra blood returns to left heart → LA/LV volume overload.
Extra blood exposes the pulmonary arteries to higher-than-normal _______
potentially driving up what?
If left untreated, _____pulmonary over _____can ______damage what?
Extra blood exposes the pulmonary arteries to higher-than-normal pressures,
potentially driving up pulmonary vascular resistance
If left untreated, chronic pulmonary over circulation can irreversibly damage lung
vessels (Eisebnebger’s syndrome a rare reversal of blood flow (right to left)
what does the Magnitude of the shunt depend on name 2?
Restrictive verses Nonrestrictive VSDs which size are each?
What causes a larger left-to-right shunt?
Magnitude of the shunt depends on size of the shunt and resistance of the pulmonary vascular bed
Restrictive = small VSDs
Nonrestrictive =Large VSDs
The greater the size of the lesion and the lower the PVR = the larger the left to right shunt.
List the 3 size/hemodynamic categories of VSDs.
Small
Moderate
Large
Why are small VSDs called restrictive VSDs?
They are called restrictive because blood flow across the defect is restricted.
List the 10 key features of small/restrictive VSDs.
How much blood will flow from the left side of the heart to the right side of the heart?
What is the pressure difference between the ventricles is maintained?
Do they feel symptomatic or asymptomatic
what is the murmur
what is the LV-to-RV peak instantaneous gradient.
what does the velocities fall between?
what is the peak pressure
how much is it for the aortic orifice
commonly occurs in ______
can they spontaneously close?
Little or no blood flows from the left side to the right side.
Normal pressure difference between the ventricles is maintained.
They are usually asymptomatic.
They have a high-pitched loud holosystolic murmur.
They have a high LV-to-RV peak instantaneous gradient.
Velocity is 2.5–4 m/s. (high velocities)
Peak pressure is >64 mmHg.
They are less than 1/3 of the aortic orifice.
They may occur in groups
Yes, may spontaneously close.
They may occur in groups” = So rather than one large hole in the ventricular septum, there can be a cluster of tiny holes, especially in the muscular septum.
List the 9 key features of moderate VSDs.
Flow across the defect is how much restricted?
There is a Significant what shunt?
list 2 things that are increased
The increased LV preload causes what list 2
what is the murmur?
what is the pressures gradient?
what does velocities fall between?
which categories does this fall into
how much of it of the aortic annulus
Flow across the defect is less restricted.
There is a significant left-to-right shunt.
Pulmonary flow increases. More blood returns to the left atrium.
Increased LV preload causes LA and LV dilation.
Murmur is a softer holosystolic murmur.
Pressure gradient is 25–60 mmHg.
Velocity is 2.5 m/s to below 4 m/s.
Moderately restrictive
1/3rd to 1⁄2 of aortic annulus
How large is a moderate VSD compared with the aortic annulus?
It is about 1/3 to 1/2 of the aortic annulus.
Why are large VSDs called nonrestrictive VSDs?
They are called nonrestrictive because there is minimal resistance to flow.
List the 7 key features of large/nonrestrictive VSDs.
Pressures in both ventricles _____
What murmus is this?
Very ____LV-to-RV gradient.
what is the velocity?
what happens to the PVR
The RVSP is __%? of the LVSP?
causing what flow list 2, possible what syndrome
Pressures in both ventricles equalize.
Low pansystolic murmur. (softer murmur = bigger hole)
Very low LV-to-RV gradient.
Velocity is below 2.5 m/s.
Pulmonary vascular resistance is increased.
RVSP is >80% of LVSP.
Can cause bidirectional flow.
Can cause right-to-left flow.
Possible Eisenmenger syndrome.
Symptoms appear at 4–6 weeks.
How large is a large VSD compared with the aortic annulus?
Greater than 1/2 to 2/3 of the aortic annulus.
How do symptoms differ between small, moderate, and large VSDs?
Small VSDs may be asymptomatic until adulthood.
Moderate VSDs may develop symptoms in late adolescence.
Large VSDs develop symptoms around 4–6 weeks.
List the 6 clinical symptoms of VSDs.
Exercise intolerance
Fatigue
Sweating while feeding
Dyspnea
Recurrent respiratory infections
Failure to thrive
What symptoms are associated with Eisenmenger syndrome? list 2
Cyanosis and clubbing.
What can large VSDs cause? list 2
Large VSDs can cause recurrent respiratory infections and heart failure.
List the 4 chest X-ray findings that may be seen with VSD.
Increased pulmonary vascular markings
Enlarged left atrium
Enlarged left ventricle
Enlarged pulmonary artery

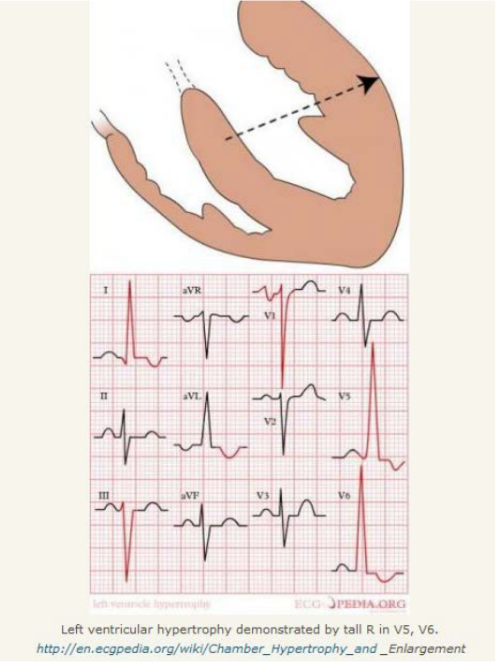
What ECG finding is associated with VSD?
ECG may show LVH.
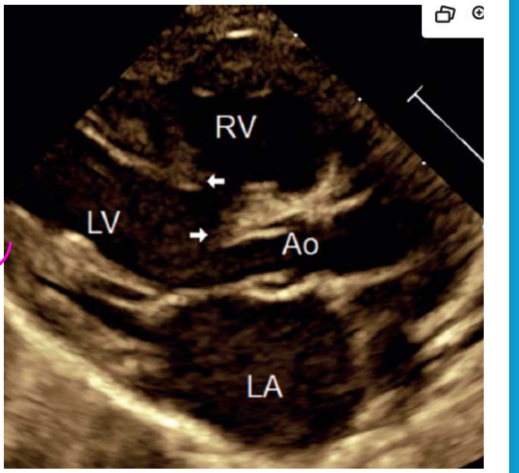
what are the Perimembranous VSD best echo views. List 6
Perimembranous: PLAX, PSAX at great vessel level, apical 3- and 5-chamber, subcostal LVOT view, and PSAX
what are the Muscular VSD best echo views. list 5
Muscular: PLAX with sweep and spectral Doppler, PSAX sweep from aortic valve to apex, A4C, subcostal 4C, and LVOT
what are the Inlet VSD best echo views. list 3
Inlet: A4C, PSAX mitral valve level, subcostal ventricle level
what are the Outlet VSD best echo views. list 3
Outlet: PSAX great vessel level, PLAX, subcostal PSAX
what are the Malalignment VSD best echo views. list 7
Malalignment: both outlet and perimembranous views
Outlet- PSAX great vessel level, PLAX, subcostal PSAX
Perimembranous - PLAX, PSAX at great vessel level,
Apical 3&5 Chamber, Subcostal LVOT view and PSAX
Associated CHDs include: Perimembranous list 3
Tricuspid pouch & TV function
double-chambered right ventricle (DCRV)
Associated CHDs include: mid muscular and perimembranous list 1
Coarctation of aorta
Associated CHDs include: Inlet list 2
Partial or complete AV canal defect & inflow regurgitation
Associated CHDs include: outlet list 5
AV Prolapse and AI,
RVOT obstruction from anterior deviation of the septum,
LVOT obstruction from posterior deviation of the septum,
TV straddling or overriding
Associated CHDs include: malignment List 4
Tetralogy of Fallot, DORV, Truncus Arteriosus, IAA (interrupted aortic arch.)
Associated CHDs include: for every VSD will have what list 2
PHTN (all)
Endocarditis (all)
List the 6 chromosomal/genetic syndromes associated with VSDs.
Trisomy 21
Trisomy 18 & Trisomy 13 (100% of getting CHD)
DiGeorge
Noonan
Holt-Oram (holes in the heart)
List the 3 maternal exposures associated with VSDs.
Fetal alcohol syndrome
Marijuana use
Cocaine use
List the 5 things to keep in mind when interrogating a VSD.
the VSD appearance name 4
Look for echo ____with 2D, including what -sign artifact
Use 2D and color for what
Examine the relationship of the VSD to which valves name 3
Look for ______defects
VSD type, location, size, and number
Look for echo dropout with 2D, including T-sign artifact
Use 2D and color for measurement
Examine the relationship of the VSD to the tricuspid, aortic, and pulmonic valves
Look for associated defects
What size VSD may spontaneously close?
A VSD <0.5 cm may spontaneously close.
List the 7 echocardiogram findings associated with VSDs.
Pulmonary artery and branch PA dilation
Pulmonary vein dilation
LA enlargement
LV enlargement
Assessment of left-sided diastolic and systolic function
Over time, RV hypertrophy and septal flattening
Gerbode defect causing RA enlargement
List the 6 Doppler/echo assessment goals for VSDs.
Assess hemodynamic significance with what list 2
list 3 measurements you make and with what dopplers used list 3
Doppler signal is primarily in what cardiac cycle
Estimation of what pressure
Evaluation of the degree of _____load
Evaluation of what performance
Assess hemodynamic significance with color and spectral Doppler
Measure peak velocity
Measure peak gradient
Determine direction of flow using color, CW, and PW
Recognize that the Doppler signal is primarily in systole
Estimate RV systolic pressure
Evaluate volume load and LV systolic/diastolic performance
What agent is listed for VSD assessment? to see better?
Definity.
List the 4 VSD quantification methods.
Mean PA pressure
RVSP
Qp:Qs
PISA
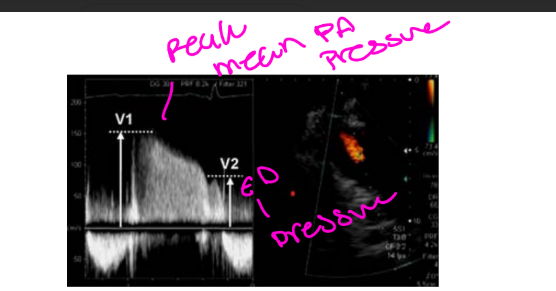
What signal can estimate mean PA pressure and PA end-diastolic pressure?
The pulmonary regurgitation signal.
What formulas are used for mean PA pressure and PAEDP?
mPAP = 4(PR max velocity)² + RAP
PAEDP = 4(PRED velocity)² + RAP
Why are these calculations helpful?
They alert physicians when PA pressures are elevated.
What formula estimates RVSP from a VSD?
RVSP = systolic BP − 4(VSD peak velocity)²
When does RVSP equal PASP?
In the absence of RVOT obstruction / PS, RVSP equals PASP.
What patient measurement is needed for this calculation?
The patient’s systolic blood pressure.
List the 3 Qp:Qs interpretation ranges.
______small to moderate restrictive shunt
______hemodynamically significant shunt
______patient should have surgical repair
1.0–1.4: small to moderate restrictive shunt
1.5–1.9: hemodynamically significant shunt
>2.0: patient should have surgical repair
What can be substituted for RVOT information?
The mitral valve annulus and mitral valve inflow TVI can be substituted.
List the 3 requirements/limitations for Qp:Qs measurement.
Absence of significant semilunar valve regurgitation
Absence of other shunt lesions
Optimal Doppler angle alignment for VTI measurement
What formula gives shunt volume?
Qp − Qs = shunt volume in L/min.
List the 3 VSD differentials.
Other types of VSDs
Aortic sinus aneurysm/rupture
Aortic regurgitation
List the 3 medication treatments for VSDs.
Prophylaxis for endocarditis prevention
Diuretics
ACE inhibitors
Which VSDs can an occluder device be used for?
An occluder device can be used for membranous and muscular VSDs.
Why is occluder device use limited for membranous VSDs?
It is limited because it can cause heart block and aortic insufficiency.
What surgical patch is listed for VSD treatment?
A Dacron patch.
List the 5 post-op interrogation findings after VSD repair.
Residual shunting
RVSP quantification
Valve issues from VSD patches, especially the tricuspid valve
LV and RV function
Aortic valve regurgitation and/or pulmonic valve regurgitation