Accommodation and Vergence Therapy - Diagnosis and Management of Common Ocular Conditions Spring 2026
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
What does accommodative amplitude assess?
maximum accommodation potential
What is the most common clinical method of accommodative amplitude testing?
push up technique
How is the push up test done in clinic to assess accommodative amplitude?
-Viewing 20/30 vertical line of letters
-Slowly bring the letters toward eye (increases accommodative amplitude of the target)
-Target blurs when the accommodative demand exceeds the maximum ability to accommodate
During the accommodative amplitude push up test done in clinic, when would the vertical line of betters become blurry to the patient?
Target blurs when the accommodative demand exceeds the maximum ability to accommodate
What unit is the accommodative amplitude recorded in?
Diopters (1/distance)
What does the accommodative amplitude push up test assume about the patients refractive error?
assumes that RE is fully corrected
What is the standard method of "push ups" done?
-3x each eye
-1x binocular
Why is the push up test done so many times per eye?
to assess accommodative fatigue
EXAMPLE:
You patch your emmetropic patient's left eye and slowly bring 20/30 letters toward the patients right eye. The target blurs at 10cm from the spec plane. What is the patients accommodative amplitude?
AA = 1 / 0.1m
AA = 10D
EXAMPLE:
You patch your uncorrected 1D hyperopic patient's left eye and slowly bring 20/30 letters toward the patients right eye. The target blurs at 10cm from the spec plane. What is the patients accommodative amplitude?
AA = 1/0.1m + 1
AA = 10+1
AA = 11D
EXAMPLE:
You patch your uncorrected 1D mypoes patient's left eye and slowly bring 20/30 letters toward the patients right eye. The target blurs at 10cm from the spec plane. What is the patients accommodative amplitude?
AA = 1/0.1m - 1
AA = 10-1
AA = 9D
When an uncorrected myope if fully corrected behind the phoropter, what may they expereince?
It may be harder to accommodate. They are used to being able to underaccommodate for a clear target d/t the built in add.
How to calculate the normal age-expected AA of a patient?
18 - 0.3(age)
How to calculate the minimum age-expected AA of a patient?
15 - 0.25(age)
If the patients accommodative amplitude is BELOW the minimum age-expected accommodative amplitude, we can say that the patient has what condition?
accommodative insufficiency
Do you want you patient to MEET or EXCEED the average age-expected AA?
yes
What will a patient with accommodative insufficiency experience with extended near work?
symptoms of blur, HA, and eye strain
Why will a patient with accommodative insufficiency experience blur, HA, and eyestrain with extended near work?
Due to the strain on blur accommodation -- there is an insufficient amount of accommodation left in "reserve"
What are possible treatments for convergence insufficiency?
-vision therapy
-near add
What is the goal of vision therapy for a patient with convergence insufficiency?
to improve their amplitude of accommodation (to meet or exceed age-expected norms)
Why does a NEAR ADD improve the symptoms of accommodative insufficiency?
to decrease accommodation demand at near
What are the possible ways in which we can introduce a near add to a patient with accommodative insufficiency?
Bifocal, reading glasses, anti-fatigue lenses
What does accommodative facility testing evaluate?
the patients ability to quickly and accurately change accommodation (switch focus of the eyes to different distances)
What is the best clinical method to evaluate accommodative facility?
lens flipper technique
Why is the lens flipper method the best clinical method to evaluate accommodative facility?
lenses change the accommodative demand of the target at a fixed distance
How to evaluate accommodative facility?
-20/30 row of vertical letters as target
-flip to opposite lens when patient reports that the target is clear
-Record the number of cycles per min (flips/2)
When doing accommodative facility, should you do monocular or binocular testing 1st?
binocular 1st
To ensure the patient is using both eyes during accommodative facility testing, what should you use?
suppression check (polarized bar reader and glasses)
The target must be _______ before flipping the lenses during accommodative facility testing?
clear, single, and with no suppression
If binocular facility is normal, is the accommodative facility of the patient normal?
Yes -- no further testing needed
If binocular facility is reduced, what does this suggest?
accommodative problem and/or fusional vergence problem
If binocular facility is reduced, what do you need to do next?
monocular facility testing
What does monocular facility testing determine?
If the problem is d/t accommodation or vergence related
If monocular accommodative facility is normal, what does this suggest?
Accommodative facility is NORMAL, this is a fusional vergence deficiency
If monocular accommodative facility is reduced, what does this suggest?
Accommodative facility is poor, unsure about a vergence deficiency
If both binocular and monocular accommodative facility is reduced, the patient is said to have what condition?
accommodative infacility
What will patients with accommodative infacility complain of?
intermittent blur when looking at different distances, HA, strain (when a lot of change in viewing distance is required)
What are the recommended treatments for accommodative infacility?
Vision therapy
Near add
Why would vision therapy be beneficial for a patient with accommodative infacility?
to improve the accommodative infacility
Why would a near add be beneficial for a patient with accommodative infacility?
to decrease the need to change accommodation
What are the clinical assessments of accommodation?
-Monocular Estimation Method (MEM)
-NOTT (objective test)
-BCC (subjective test)
What are the expected values for the clinical assessment of accommodation?
+0.25 - +0.75
What do patients with accommodative excess/spasm complain of?
Blur worsening after reading/computer work
Headaches
Eyestrain
What time of the day will accommodative excess/spasm?
often worse at the end of the day
What is the treatment for accommodative spasm?
Vision therapy
Near add
Temporary cycloplegia
Why does a near add help an individual with accommodative spasm?
Decreases demand of the target at near
When treating an accommodative disorder, what is the management order?
1) Correct uncorrected refractive error
2) Added lens or vision therapy
What are the objectives during Phase 1 Therapy Treatment for Convergence Insufficiency?
Develop awareness of therapy feedback: feeling of looking closely and accommodation
Normalize accommodative amplitude and ability to stimulate accommodation
Develop voluntary convergence
What should be focused on/examples of activities in Phase 1 of Therapy Treatment for Convergence Insufficiency?
Focus on minus lenses (and a little convergence)
Lens sorting with minus to stimulate accommodation
Monocular lens rock with minus & then add plus
VTS4 accommodative rock
Minus lens trombone
Monocular push up
Brock string
What changes during Phase 2 Therapy for Convergence Insufficiency?
start to emphasize speed more, adding more with plus
What are the objectives of Phase 2 Therapy for Convergence Insufficiency?
Normalize accommodative ability to stimulate and relax accommodation
Normalize quickness of response
Build divergence and convergence abilities
What should be focused on/examples of activities in Phase 2 of Therapy Treatment for Convergence Insufficiency?
Lens rock with emphasis on speed
VTS4 accommodative rock
Hart chart
Binocular lens rock for quality
Divergence and convergence activities
What changes during Phase 3 Therapy for Convergence Insufficiency?
Emphasis on integration of accommodation and vergence
What are the objectives of Phase 3 Therapy for Convergence Insufficiency?
Integrate accommodative facility with binocular techniques
Develop quick change in vergence/accommodative demands
Integrate accommodative/vergence abilities with saccades and pursuits
What should be focused on/examples of activities in Phase 3 of Therapy Treatment for Convergence Insufficiency?
-binocular lens rock for speed
-binocular lens rock w/ vergence activities
-binocular lens rock free fusion activities
What is vergence therapy?
orthoptic therapy commonly prescribed to develop adequate fusional vergence ranges
(Positive/negative) fusional range treatment is generally greater effect and faster progress
postitive
What is the success rate for positive fusional vergence training in convergence insufficiency patients?
73-90%
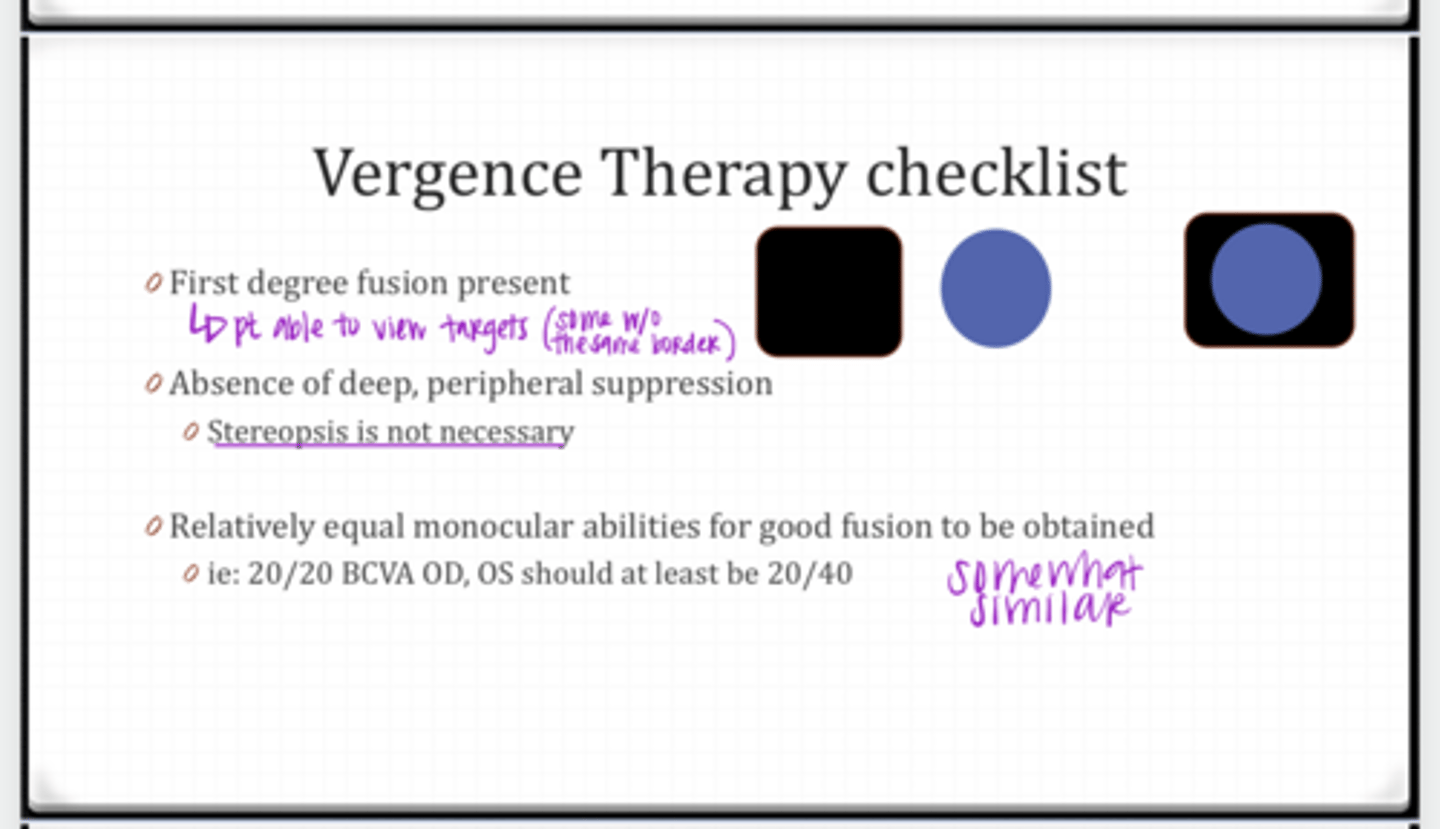
In order to complete vergence training, what is the checklist that the patient MUST HAVE in order for success?
-first degree fusion present
-absence of deep, peripheral suppression
-relatively equal monocular acuities for good fusion to be obtained
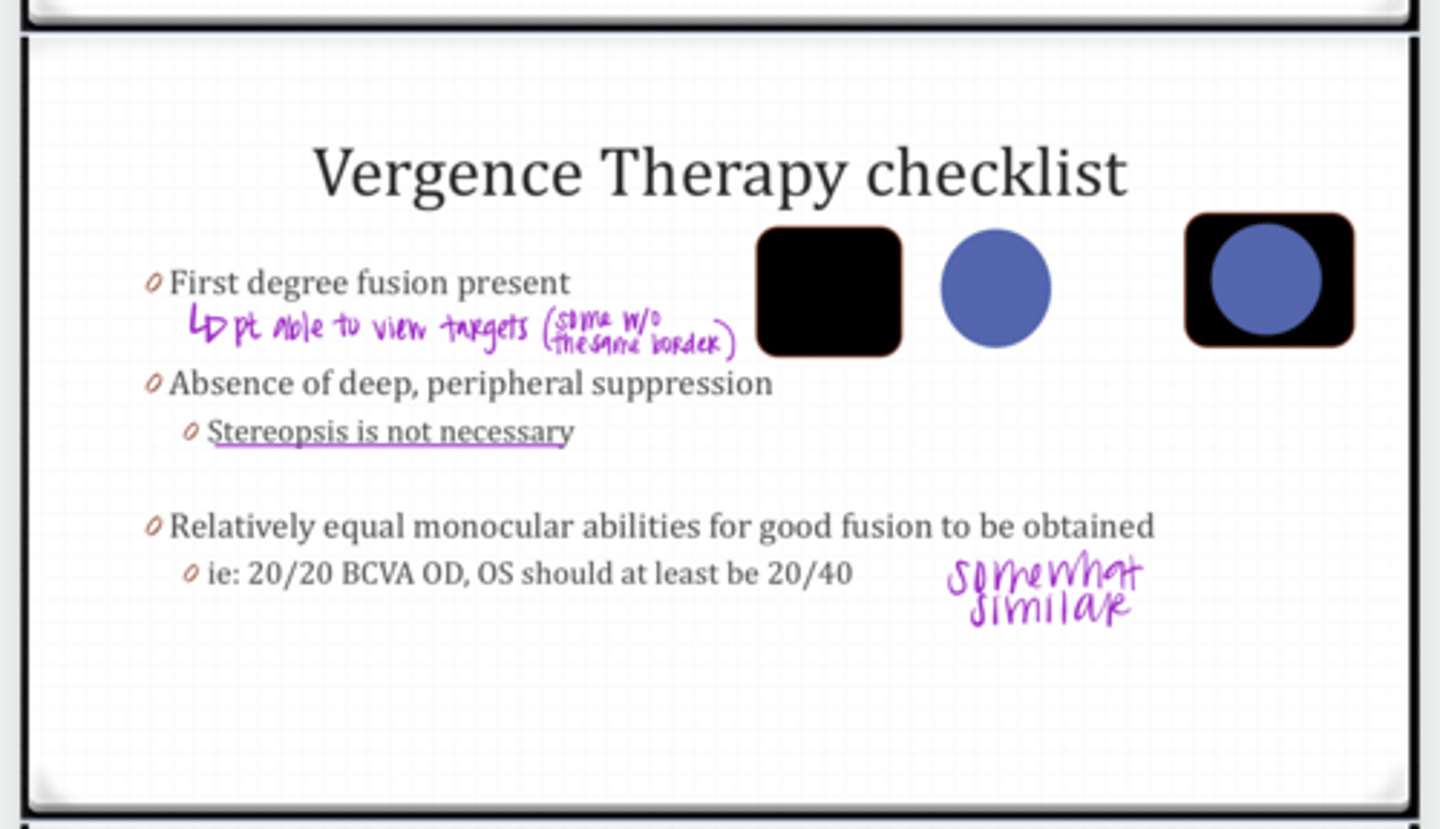
Is stereopsis necessary for vergence therapy?
No
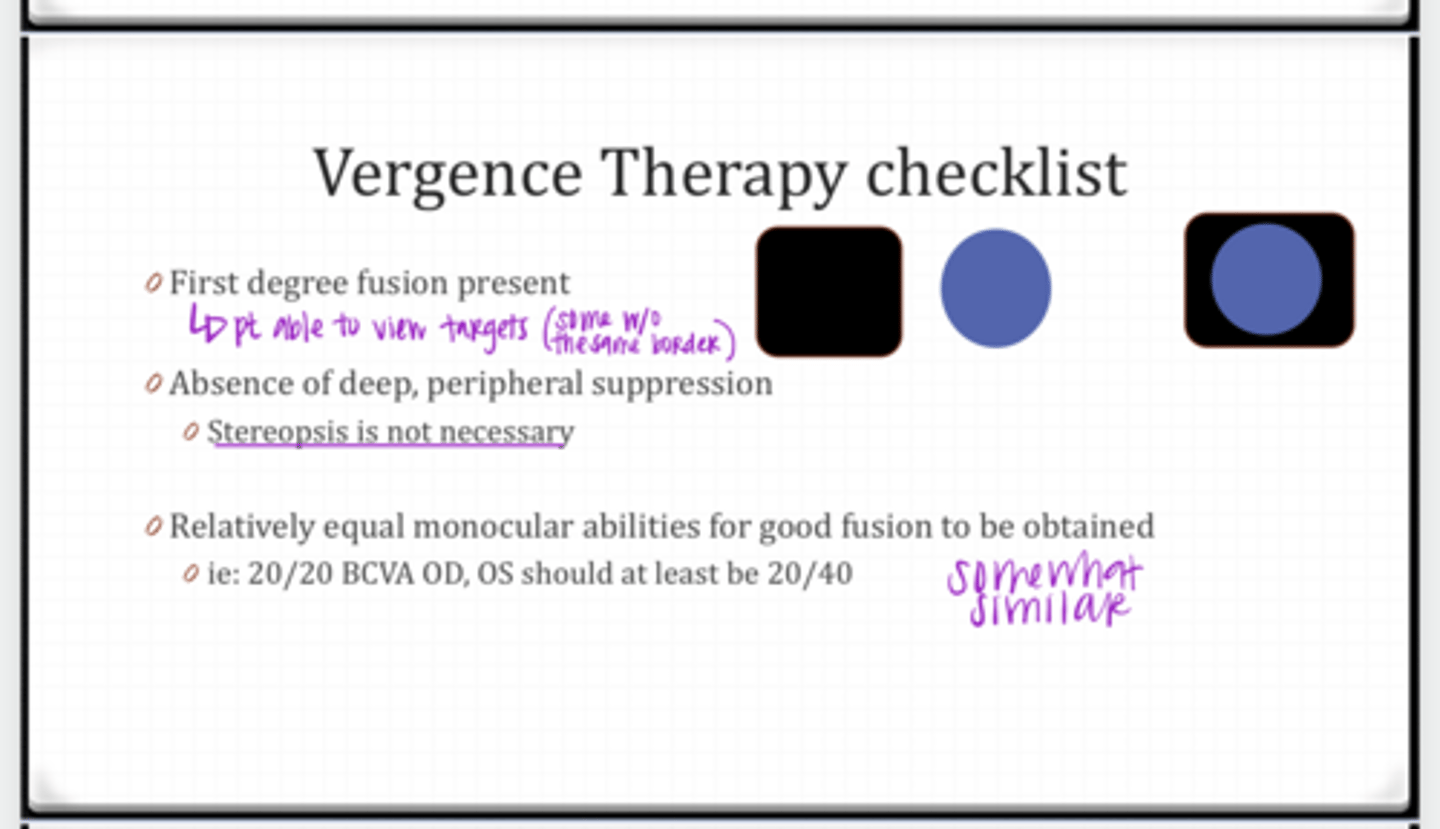
If VA OD is 20/20, what should the VA in OS be in order for success during vergence therapy?
20/40 or better
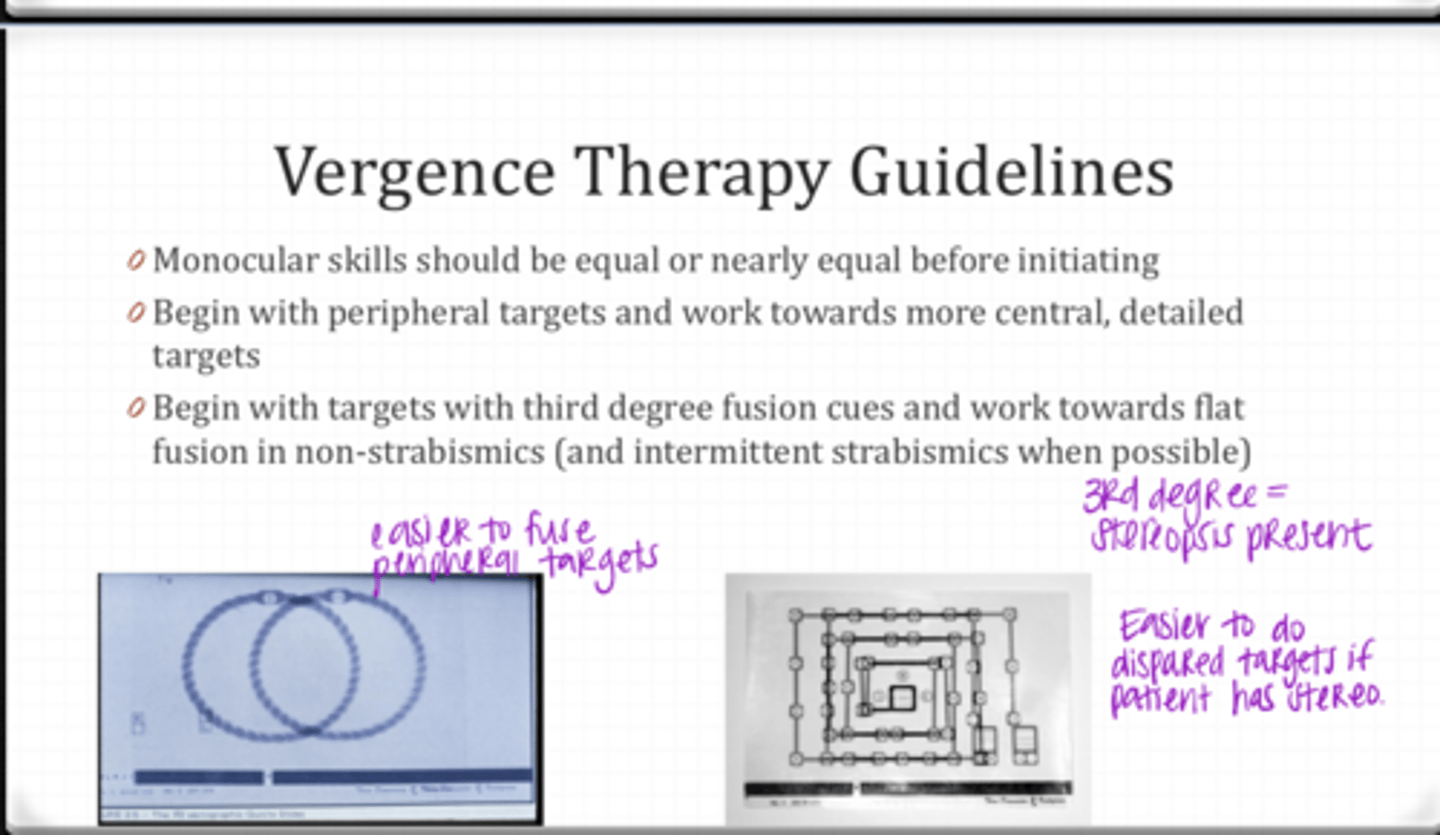
What are the vergence therapy guidelines given in this module?
-monocular skills should be equal or nearly equal before initiating
-begin with peripheral targets and work towards more central, detailed targets
-begin with targets with third degree fusion cues and work toward flat fusion in non-strabismics
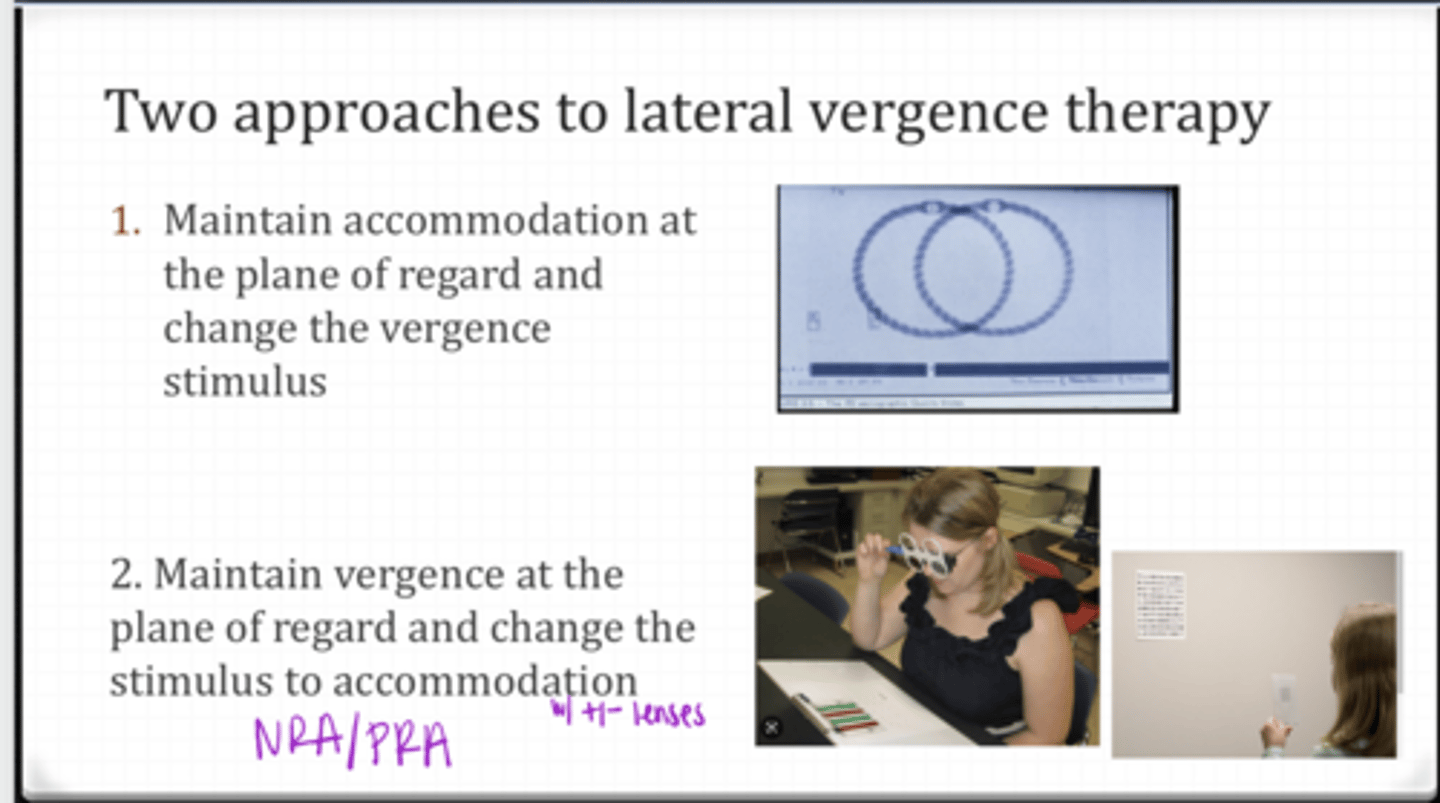
What are the 2 approaches to lateral vergence therapy?
1) Maintain accommodation at the plane of regard and change the vergence stimulus
2) Maintain vergence at the plane of regard and change the stimulus to accommodation with +/- lenses
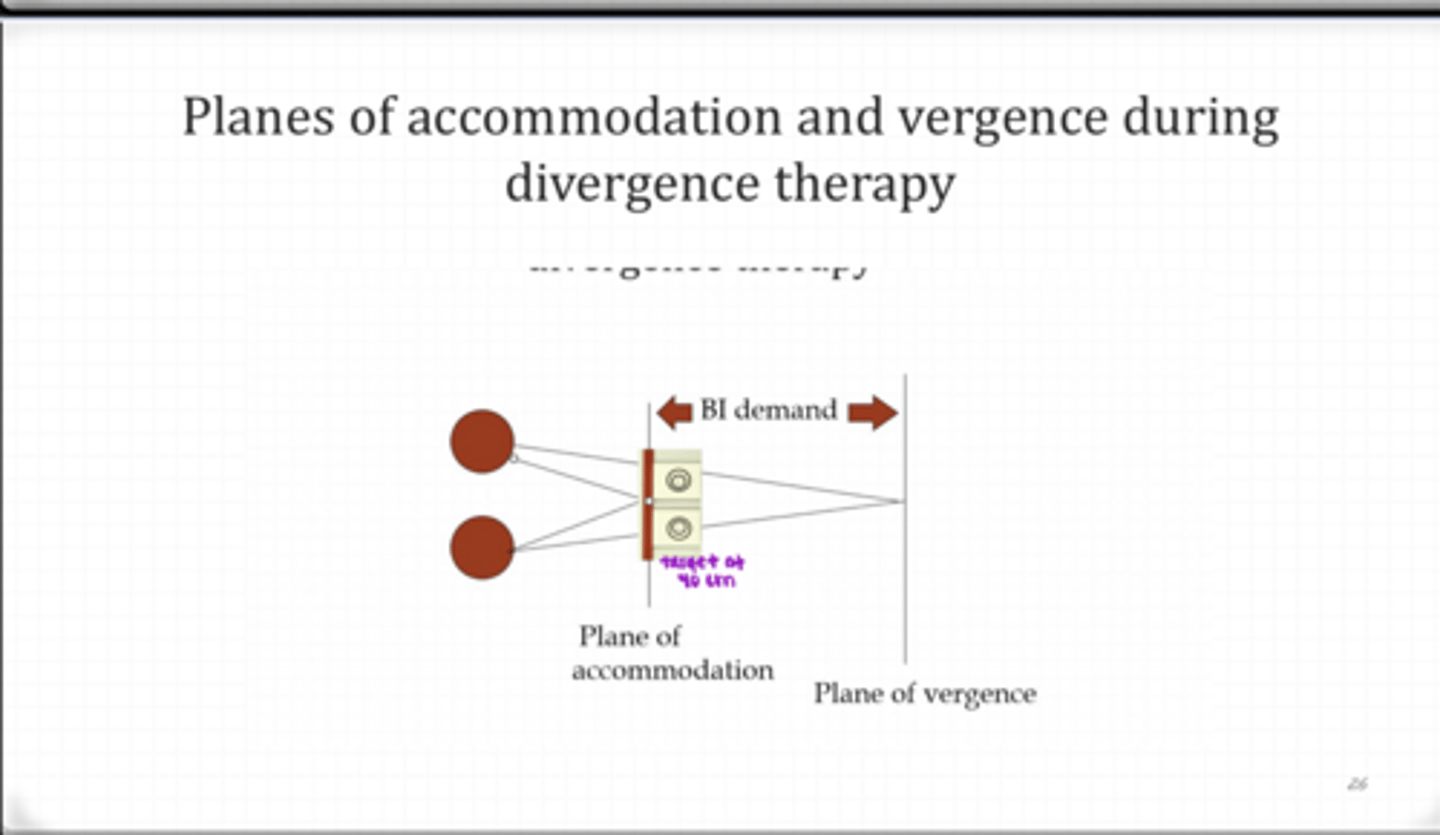
Planes of Accommodation and Vergence During Divergence Therapy (Pic)
Planes of Accommodation and Vergence During Divergence Therapy (Pic)
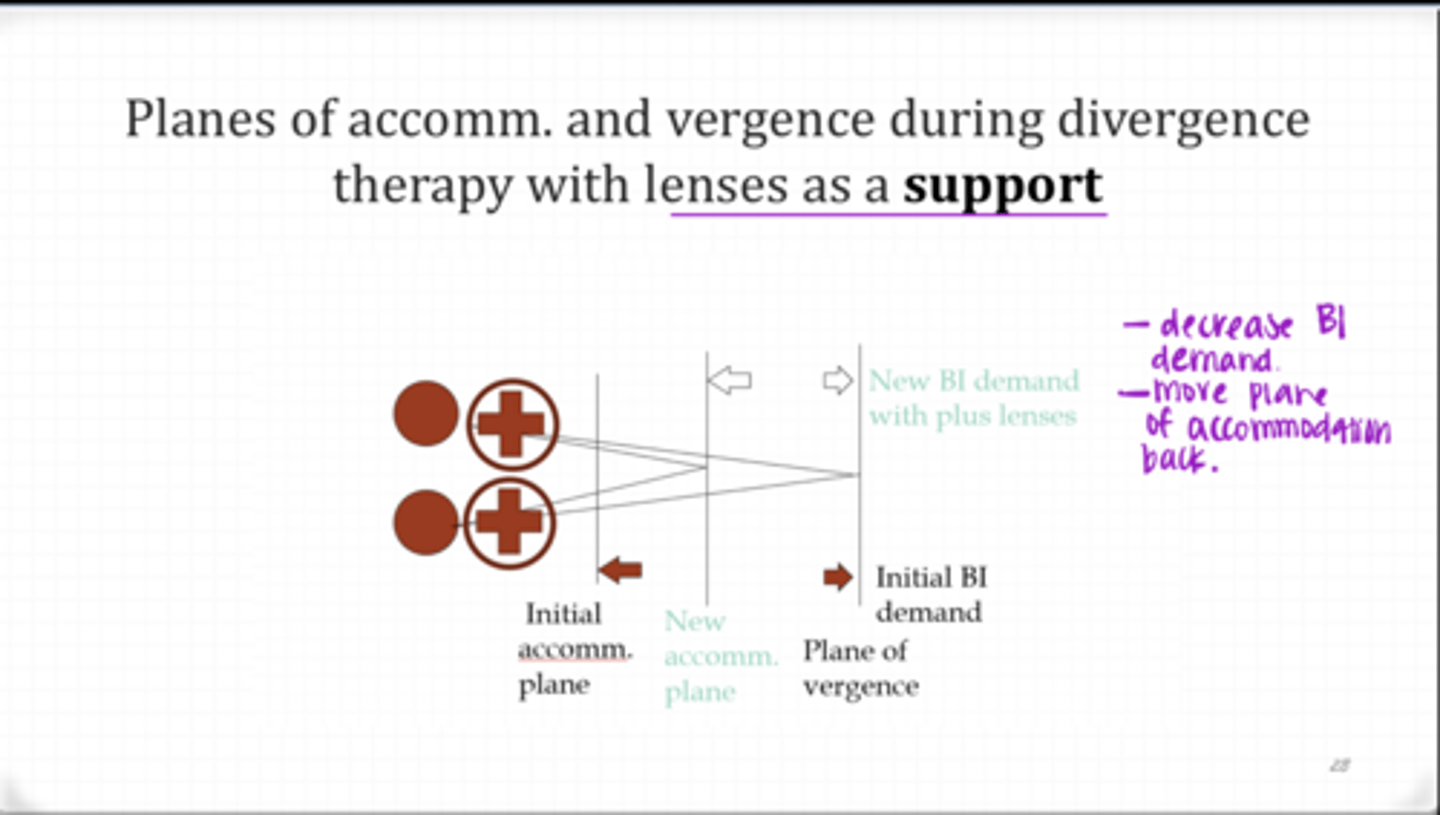
What happens when plus lenses are added during Divergence Therapy?
-decreased BI demand
-moves the plane of accommodation further from the eye
-plus lenses are a supporting lens
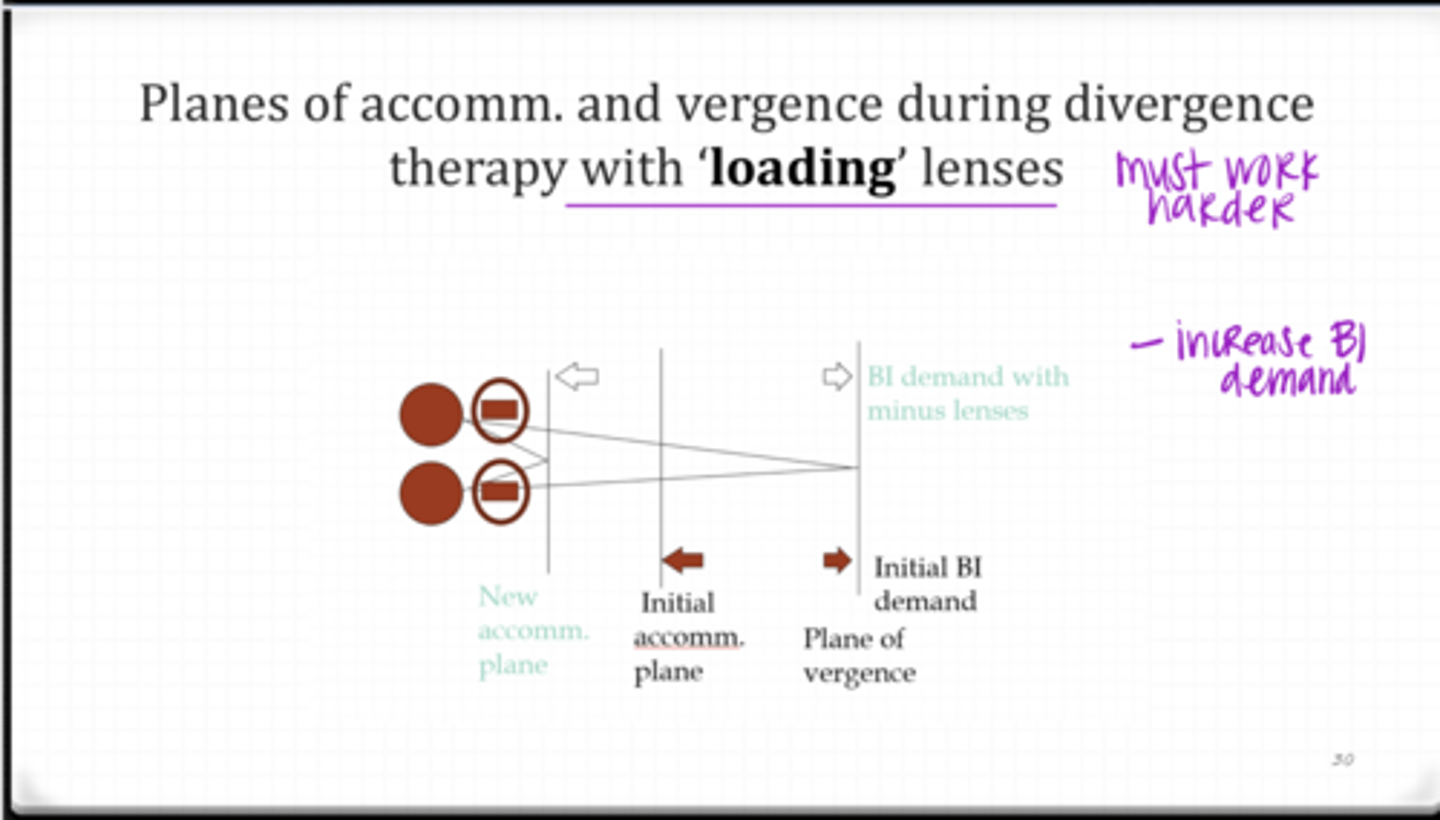
What happens when minus lenses are added during Divergence Therapy?
-increased BI demand
-moves the plane of accommodation closer to the eye
-minus lenses are a loading lens
In vergence therapy, you should stress _______ before ______
amplitude before facility (jumps)
In vergence therapy, you should work on _____ as well as blur/break
recovery
Should suppression checks be used in vergence therapy?
yes -- always
______ may help initially clear the target during vergence therapy.
Blinking
What vision therapy activities include gross/voluntary vergence & kinesthetic awareness?
Brock string
Barrel card
Binocular push ups
What vision therapy activities include ramp/smooth/tonic vergence?
Vectogram
Computer
Tranaglyph
What vision therapy activities include steps & jumps?
-vectogram
-computer
-tranaglyph
-aperture rule
-prism
converging in front or diverge behind the plane of accommodation
Chiastopic/orthopic free space fusion
What vision therapy activities include Chiastopic/orthopic free space fusion?
-LifeSaver Card
-Eccentric circles
BOP/BIM with lenses is used how in vision therapy?
to LOAD activities
What is the meaning of BOP & BIM?
BOP = base out plus; BIM = base in minus
What are the feedback mechanisms that may be present during vision therapy?
-diplopia
-blur
-suppression
-kinesthetic awareness
-SILO
-localization
-luster
-parallax
How can you decrease a patient's suppression in vision therapy?
-blink rapidly
-wiggle finger in front of suppressing eye
-increase or decrease distance (depending on the dx)
-try to make necessary vergence movements
What are the goals of vergence therapy?
-elimination/relief of symptoms
-kinesthetic awareness
-ability to realize JNDs
-ability to voluntarily converge and diverge
-appropriate amplitudes & facilities (vergence, NPC, and vergence facility)
What are the vergence therapy goals that need to be developed?
-normalize positive and negative fusional facility
-ability to jump between convergence and divergence demands
-integrate vergence, accommodation, and oculomotor skills
-ability to perform therapy in the presence of distractions
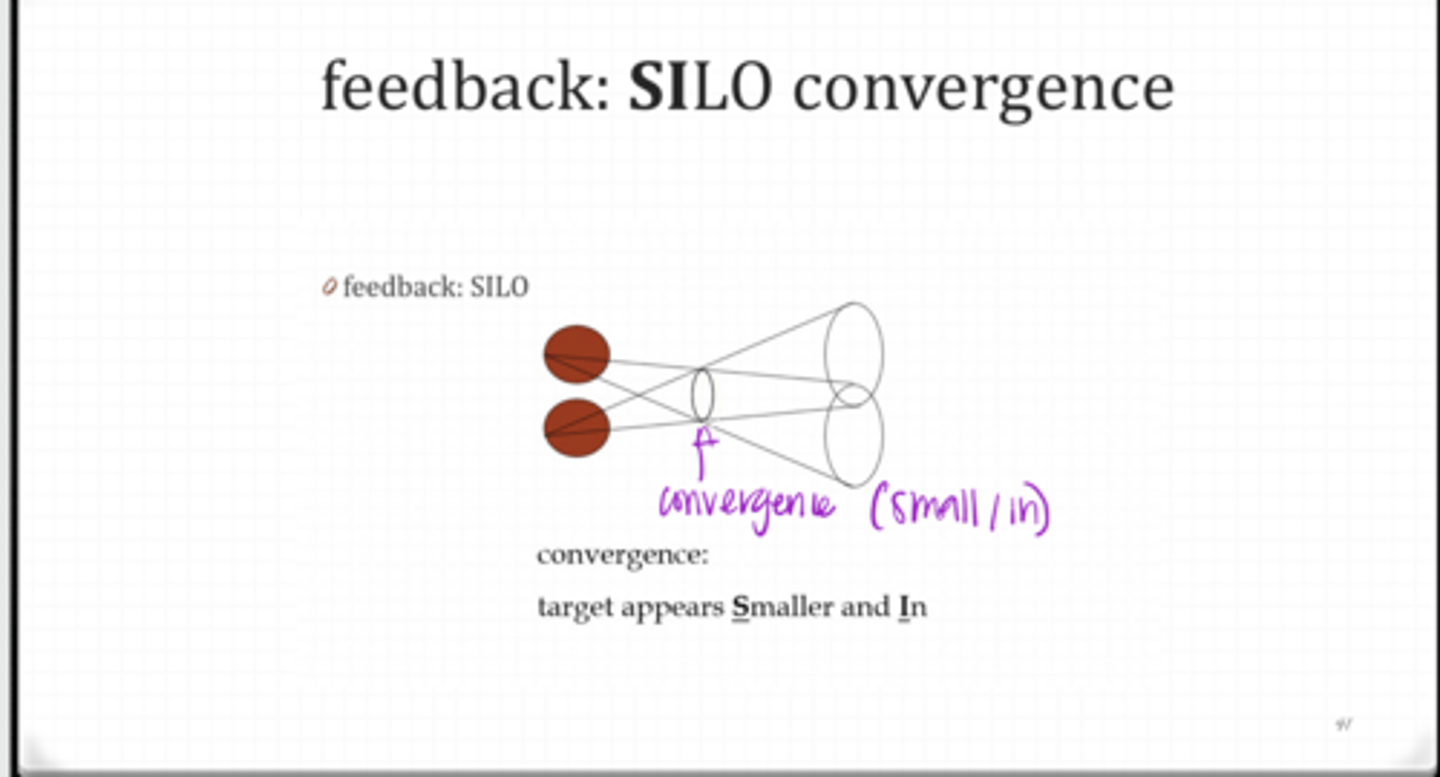
What is SILO (Vision Therapy Guideline)?
-small in
-large out
-SILO = vergence as a cue for distance perception
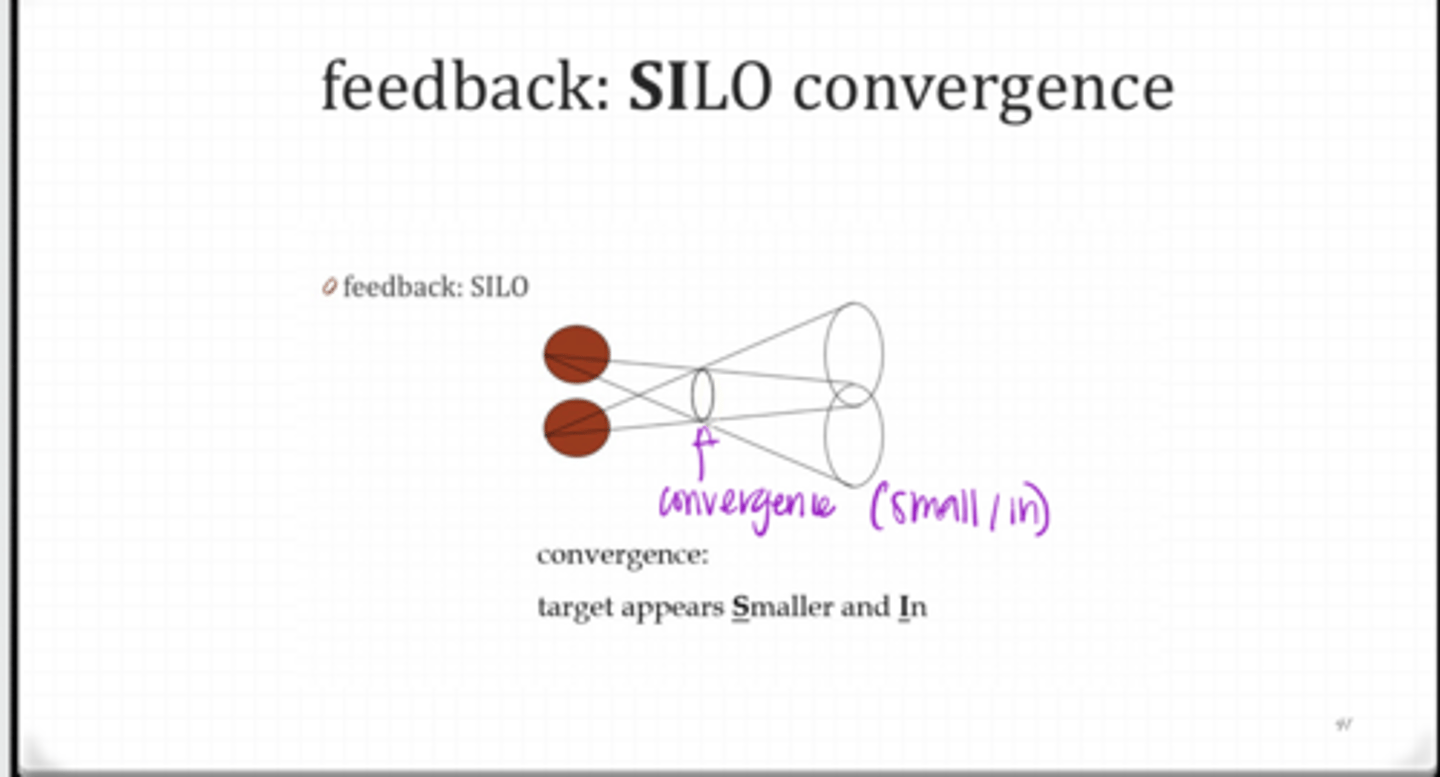
When converging, the target appears ______ and ______
smaller; in
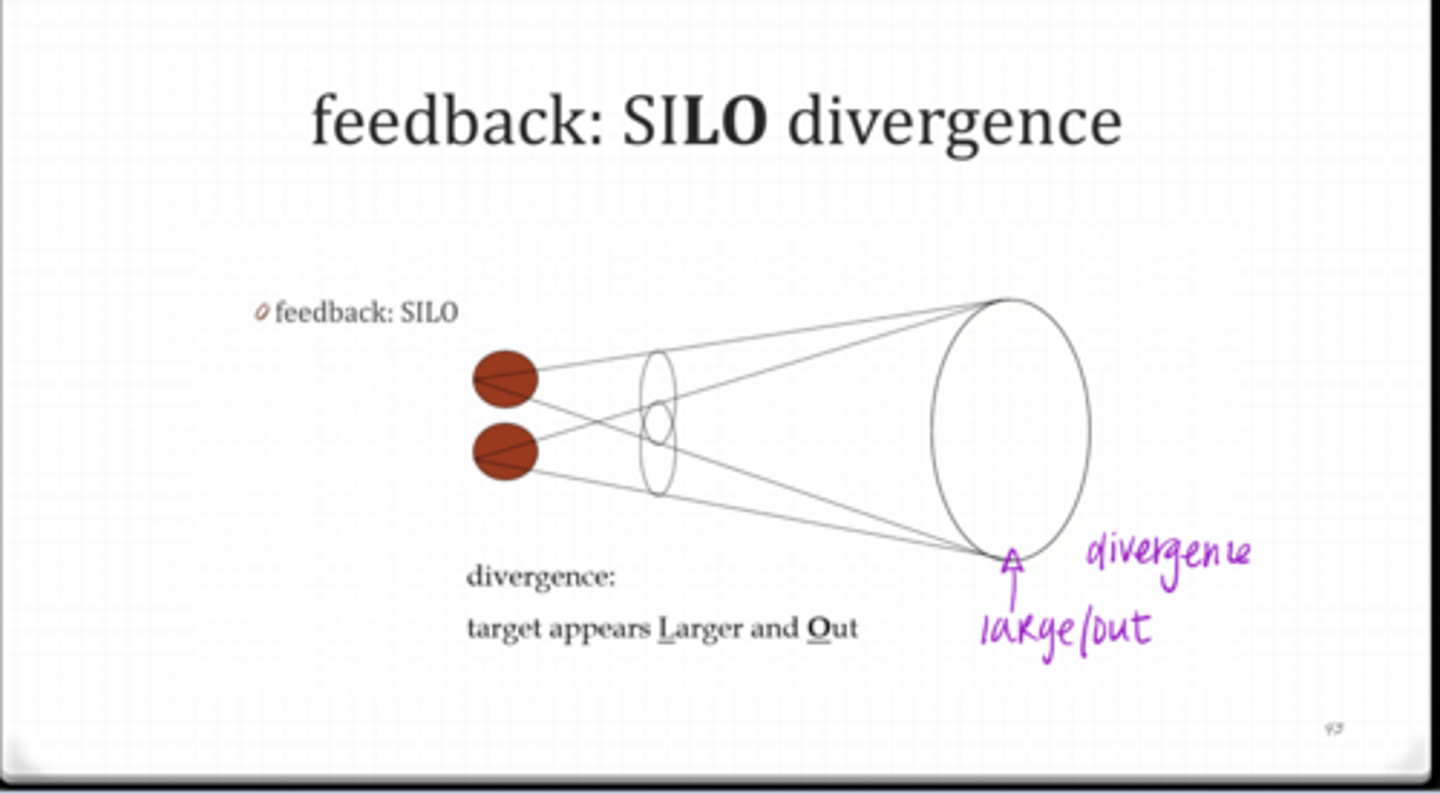
When diverging, the target appears ______ and ______
larger; out
What is SOLI (Vision Therapy Guideline)?
SOLI = size as a cue for distance perception
SILO Convergence Feedback (Pic)
SILO Convergence Feedback (Pic)
With PARALLAX, convergence will move the target in the (same/opposite) direction as the person
same
With PARALLAX, divergence will move the target in the (same/opposite) direction as the person
opposite
What are some vergence therapy supports for patients?
-keep patient at effective level
-motor/localization by using a pointer or finger
-clear v opaque target
-auditory/cognitive
-use lenses (+ and -)
-prism
What is the effect of BO prism in vergence therapy?
decreases difficulty of divergence therapy
What is the effect of BI prism in vergence therapy?
decreases difficulty of convergence therapy
What are some vergence therapy distractions for patients?
-motor (stand on one foot, balance board)
-clear vs opaque
-cognitive problems
-auditory distractions
-Lenses
-Prisms