MB2080: Topic 6 - Atherosclerosis, Stroke & Mitochondrial Disease
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
Arterial wall anatomy
tunica externa — elastic/collagen fibres
tunica media — contains smooth muscle cells
tunica intima — consists of endothelial cells
Functional role of arterial wall layers
adventitia — structure
media — contractile function to regulate vascular tone
intima — smooth surface for blood flow
Atherosclerosis
the build-up of fibrous and fatty material inside arterial walls and is the underlying condition that causes coronary heart disease and other cardiovascular diseases
Significance of atherosclerosis
CVD is the no.1 cause of death globally
~17.9M people died from CVDs in 2019, 32% of global deaths
~85% of CVD deaths are due to either coronary heart disease or stroke
Atherosclerosis symptoms
absent for many years?
angina (chest pain)
heart attack
claudication
stroke
Claudication
cramping pain in leg during exercise (non-cerebral, non-coronary = ‘peripheral arterial disease’)
Atherosclerosis as a cause of stroke
caused by a build up in the carotid arteries
Peripheral arterial disease
non-cerebral, non-coronary atherosclerosis which affects blood flow to the limbs
Atheroma
a fatty deposit made up of cholesterol, waste, endothelial and smooth muscle cells as well as inflammatory leukocytes, restricting blood flow
Diapedesis
passage of immune cells into the arterial wall
Macrophage Function in Atherogenesis
penetration
activation
Macrophage penetration in atherogenesis
leukocytes respond to chemotactic stimuli and penetrate the endothelial surface and enter into the arterial lamina
Macrophage activation in atherogenesis
once inside the intima, the mononuclear phagocyte undergoes activation
expresses scavenger receptors that can internalise modified LDL
promotes foam cell formation
Molecular mediators of atherogenesis
Adhesion molecules (e.g. VCAM-1) — cause binding of inflammatory leukocytes to the endothelium
Chemoattractants (e.g. MCP-1) — cause direct migration of leukocytes into the intima
Activators (e.g. M-CSF) — cause expression of scavenger receptors, releasing cytokines and stimulating macrophage proliferation
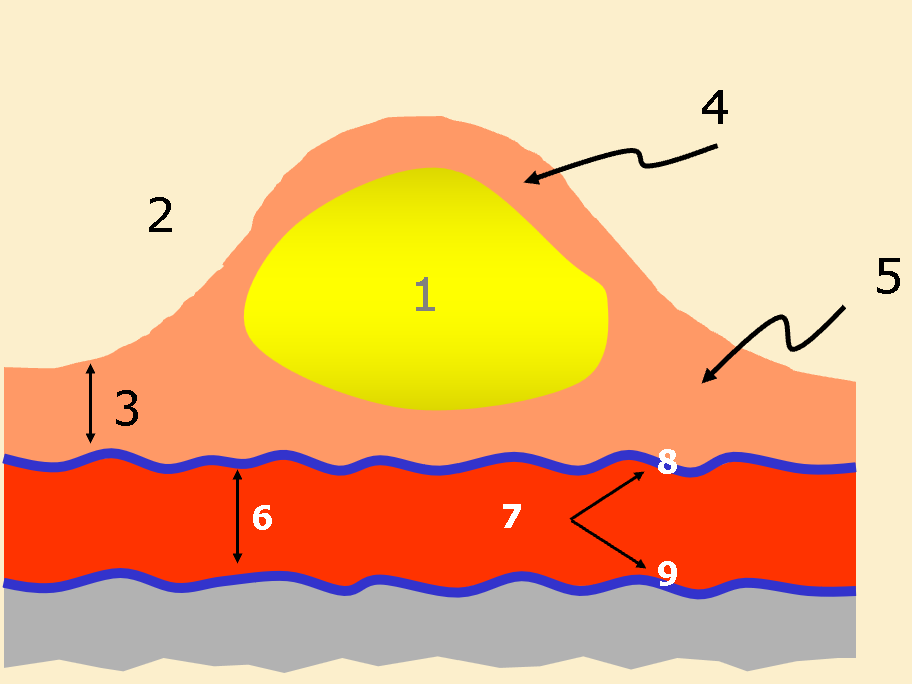
Label the atherosclerotic plaque
Lipid core
Lumen
Intima
Fibrous cap
Shoulder
Media
Elastic laminae
Internal elastic laminae
external elastic laminae
Lipid core formation
Overloaded foam cells die from necrosis or apoptosis, releasing their lipid content into the intima, forming the lipid core
Most common cause of acute coronary syndromes
thrombosis of disrupted atheroma
Thrombosis of atheroma
formation of a blood clot caused by the weakening of the fibrous cap
Inflammatory cells effect on collagen of the fibrous cap
inhibit the ability for smooth muscle cells to synthesize new collagen
release proteolytic enzyme that degrade collagen and other connective tissue
weakening the fibrous cap over time
Tissue factor
a potent procoagulant produced by inflammatory cells, partly responsible for thrombosis of ruptured plaque
Ischaemia
restriction of blood flow to tissues, causing a shortage of oxygen and nutrients required for cell metabolism
Consequence of ischaemia
cell damage
cell death
release of proteins: enzymes, troponin
Risk factors of atherosclerosis
drugs
sugar
alcohol
smoking
Primary prevention
preventing onset of disease by addressing risk factors and reducing them by altering behaviour, exposure or enhancing resistance
Secondary prevention
detection and treatment of pre-clinical changes to prevent progression
Examples of secondary preventors of CVD
statins
aspirin
angiotensin II inhibitors
ACEi
ARB
diureitcs
beta blockers
Cardiac interventions
valve repair
bypass graft
stents
heart transplant
Bypass graft
healthy blood vessel is taken from another part of the body and attached above and below the blockage to create a new route for blood flow
Stent
small mesh tube inserted into vessels to hold it open for improved blood flow
Stent procedure
stent with balloon is inserted into partially blocked artery
balloon inflated to expand state and open up the vessel
balloon is removed, expanded stent is left in the artery, keeping it open
Neurodegeneration
progressive damage or death of neurons leading to gradual deterioration of the bodily functions controlled by the affected part of the nervous system
Stroke
occurs when blood flow to the brain is cut off leading to acute neurodegeneration
Types of strokes (and prevalence)
Ischaemic stroke (80%)
Haemorrhagic (20%)
Ischaemic stroke
blockage in the blood supply feeding the brain with oxygenated blood (area of brain becomes blood deprived)
Haemorrhagic stroke
break in blood vessel (aneurysm) in brain — area of bleeding in the brain
UK stroke prevalence
250-400 strokes per 100,000 people
3rd cause of death
1st cause of disability
Clinical symptoms of stroke
sudden or gradual onset one-sided limb weakness/paralysis
confusion, loss of speech/vision
headache
loss of consciousness
cognitive impairment
Types of cognitive impairment caused by stroke
amnesia
inattention
confusion
depression
mood & behaviour changes
Transient Ischaemic Attack
transient episode of neurological dysfunction without acute tissue death
Primary cause of stroke-induced cell death
excessive amounts of glutamate
Core pathology of stroke
rapid necrotic cell death mainly due to excess NMDA
Penumbra pathology of stroke
slower apoptotic cell death due to more moderate NMDA receptor hyperactivity
How does post-stroke depression differ from primary depression
more cognitive impairment
increased irritability
more psychomotor slowing
more mood liability
Excitotoxic hypothesis
excess amino acids results in prolonged depolarisation of receptive neurons which in some way leads to their eventual damage or death (excitotoxic lesions)
Events following stroke
excitotoxicity
inflammation
increased sodium ions retention
microglia
blood-brain barrier breakdown
oedema formation
Stroke treatment methods
pharmacological
thrombolysis
aspirin
modifiable risk factors
physiotherapy
stem cells
Limitations of NMDA receptor antagonists
glutamate plays a crucial role in normal cell physiology and survival — this is disrupted by NMDA receptor antagonists
difficult to administer the antagonists to the core of the stroke
Thrombolysis
break down of blood clots to restore blood flow to blocked organs or limbs
Major limitation of t-PA
needs to be administered within 3 hours of a stroke
Surgical intervention for thrombolysis
carotid endarterectomy
intra-arterial clot removal
Aspirin for stroke treatment
prevents recurring strokes
reducing severity of stroke
Modifiable stroke risk factors
high blood pressure
smoking
physical inactivity
obesity
Physiotherapy for stroke treatment
Improve motility/avoid injury
Everyday activities
Independent living
Exercise, manipulation, massage, skills training, electrical treatment
Mitochondrial disease
a group chronic, genetic disorders caused by dysfunctional mitochondria
Features of mtDNA
16,569 bp
polyploidy
codes 13 polypeptides, 22 tRNAS, 2 rRNAs
maternal inheritance
polycistronic
Mitochondrial disease prevelance
children: prevalence >6.2/100,000 births
much higher in consanguineous communities
adults: 1 in 4300 affected or at risk
mtDNA mutations in 75% clin affected adults
152 births per annum at risk of tranmission in UK (778 US)
no cure
progressive nature
Features of mtDNA mutations
either homoplasic or heteroplasmic
cellular threshold for biochemical effect to be seen
maternal inheritance
Homoplasmy
all mtDNA copies within a cell are identical
Heteroplasmy
mixed populations of mtDNA within a cell
MELAS
Mitochondria Encephalomyopathy Lactic Acidosis and Stroke-like episodes
Clinical symptoms of MELAS
migraine
limb weakness
neuro deficit
stroke like radiol
hearing loss
diabetes cardiomyopathy
MERRF
Myoclonic Epilepsy and Ragged Red Fibres — caused by mtDNA 80-90s lysine tRNA mutation
MERRF symptoms
encephalomyopathy
ataxia
muscle weakness
hearing loss
lactic acidosis
cardiomyopathy
MNGIE
Myoneurogastrointenstinal Encephalomyopathy (caused by mutation in thymidine phosphorylase) — nDNA
Mitochondrial donation
the transfer of the nuclear chromosomal DNA from an oocyte or zygote from a woman with pathogenic mtDNA mutation into an enucleated, recipient donor oocyte or zygote
Potential therapeutic interventions for mitochondrial disease
increasing mitochondria biogenesis to restore OXPHOS function
promoting respiratory efficiency or mitochondria protein synthesis
restoring mtDNA homeostasis
shifting mtDNA heteroplasmy by genome editing