clinical aspects of penumothorax
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
What parts does the parietal pleura cover?
The chest wall, diaphragm and mediastinum
What parts does the visceral pleura cover?
The lungs and interlobar fissures
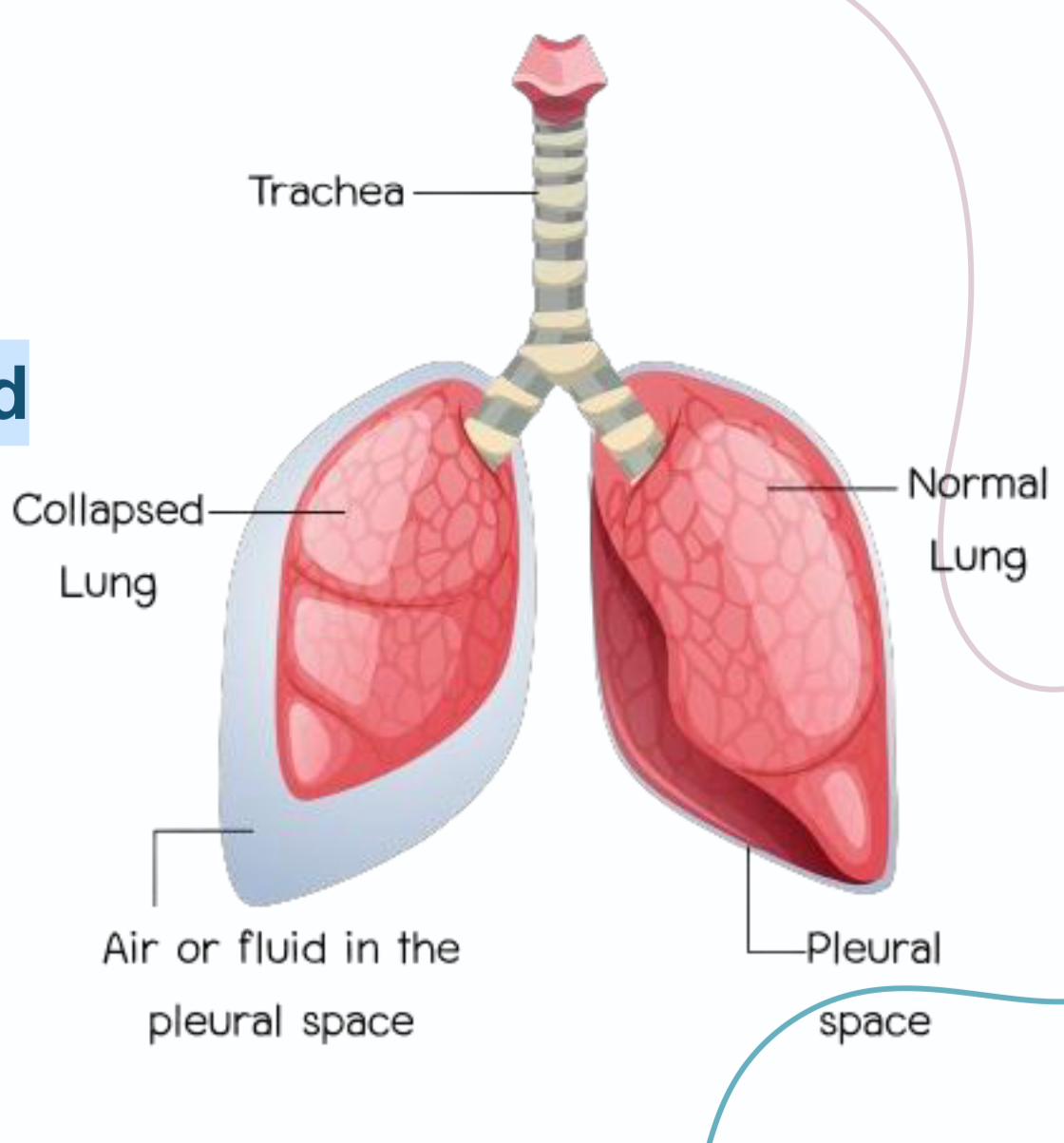
What is Pneumothorax?
Presence of air between visceral and
parietal pleura that leads to lung
collapse.
What are the classifications of pneumothorax?
1- Spontaneous (closed)
a. Primary
b.secondary
2- Traumatic (open)
a. Penetrating trauma
b. Blunt trauma
What are the causes of spontaneous PRIMARY pneumothorax?
1- young, slender, tall patients with healthy lung
What are the causes of spontaneous SECONDARY pneumothorax?
Patients with diseased lungs.
a. Emphysema (COPD)
b. Infections (pneumonia, TB)
c. Neoplasm (lung cancer)
What are the causes of traumatic pneumothorax?
1- Accidental
a. penetrating trauma
b. blunt trauma
2- latrogenic (caused by medical procedures)
a. lung or pleural biopsy
b. positive pressure ventilation
c. pleurocentesis
Explain tension pneumothorax
In tension pneumothorax, the injured tissue acts as a one way valve so air enters during inspiration but can’t exit during expiration so air is trapped inside the pleural space and inter pleural pressure accumulates
It can be developed by spontaneous or traumatic pneumothorax
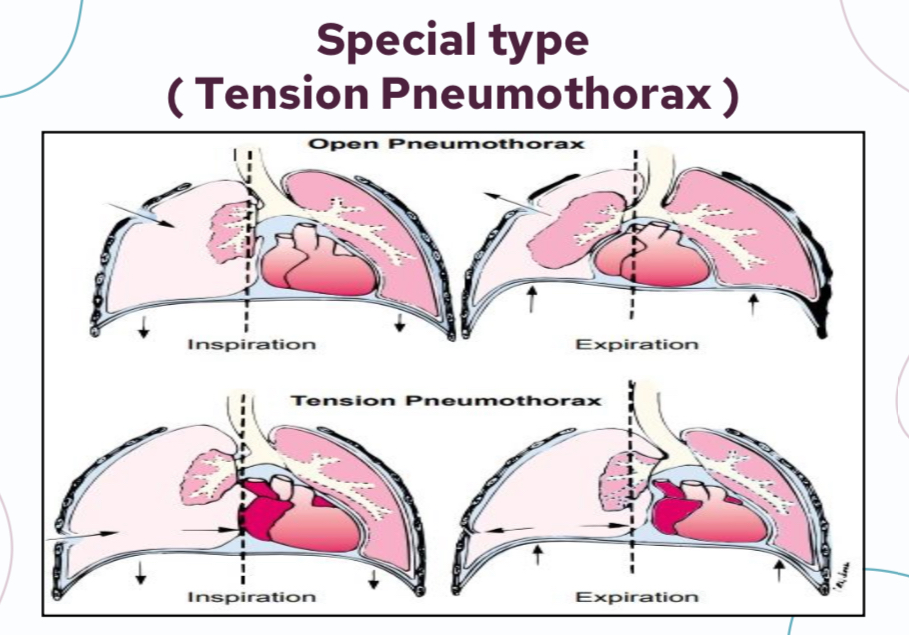
What are the events in tension pneumothorax
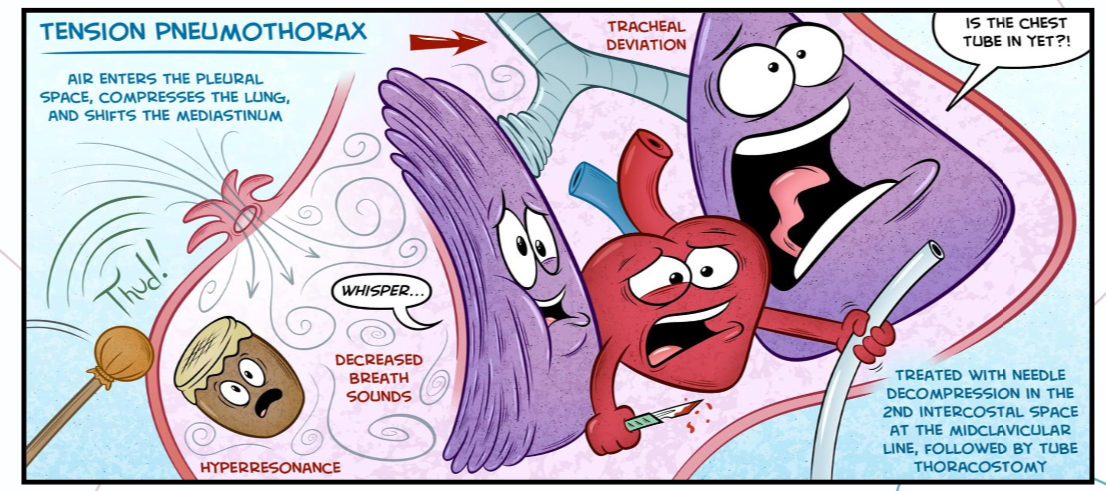
Air compresses the lungs, shifts the trachea and the mediastinum
The affected lung on the ipslateral pneumothorax is collapse and the lung, heart, blood vessels contralateral are pressurised
What is the result of the events of tension pneumothorax?
Severe dyspnea (ipslateral lung is collapsed, contralateral lung is pressurized), cyanosis (heart is compressed so less O2) and hypotension (due to reduced venous return) leading to death

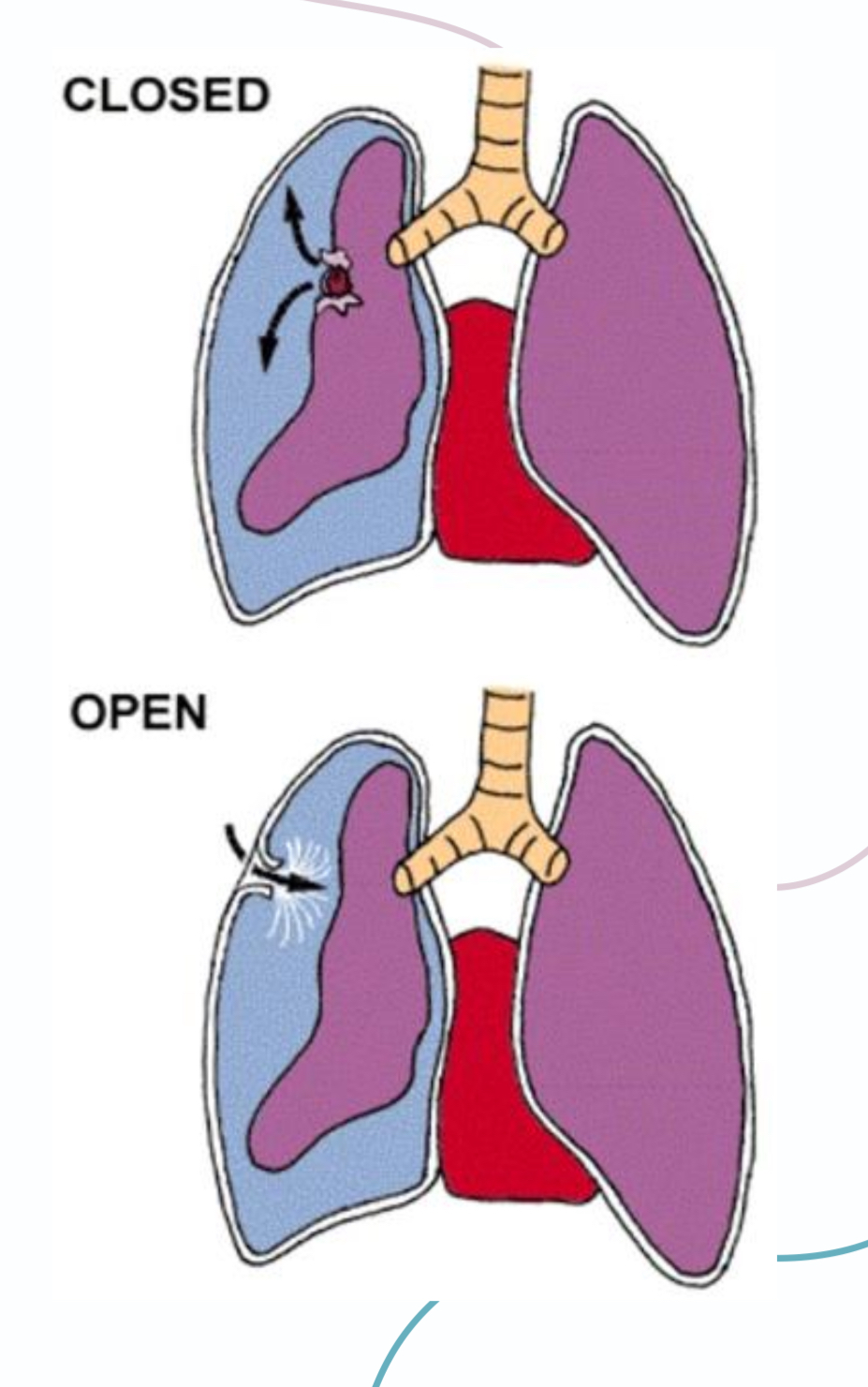
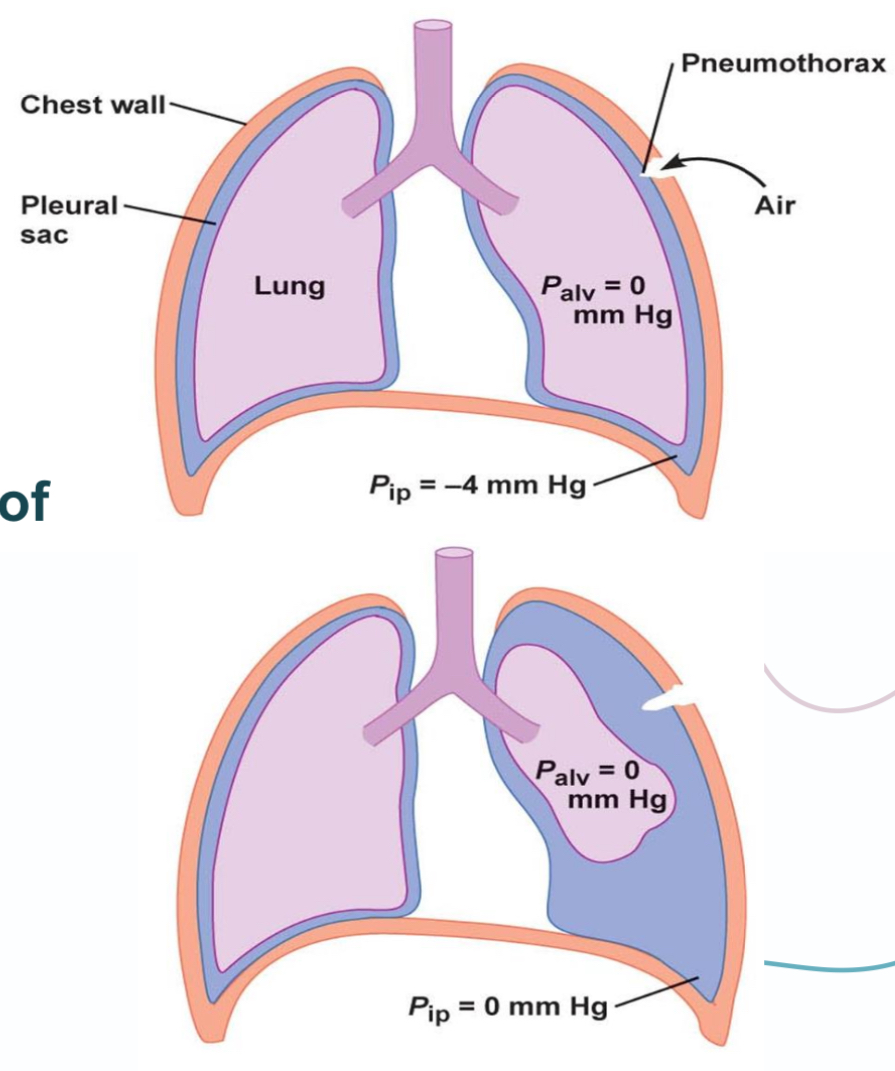
What is the pathophysiology of a closed pneumothorax?
The ruptured alveoli becomes connected with the pleural space so during inspiration air moves from the alveoli into the pleural space
What is the pathophysiology of open pneumothorax?
The pleural cavity becomes connected with the chest wall and air moves into the pleural cavity from the environment until the pressure difference reaches equilibrium or the opening is closed
What impairments does pneumothorax lead to?
1- loss of trans pulmonary negative pressure
2- lead to lung collapse
What does the clinical picture of pneumothorax depend on?
1- open or closed type
2- if it’s tension or not
What are the main SYMPTOMS of pneumothorax?
1- acute onset dyspnea (shortness of breath and difficulty breathing)
2- acute onset chest pain
3- tachypnea (increased respiratory rate)
4- asymmetric lung expansion: due to contralateral shift of mediastinum and trachea
What are the main SIGNS of pneumothorax?
Cyanosis: bluish discoloration of lips and nail beds due to decrease in O2 in blood
Inspection and palpation: chest not rising properly during inspiration
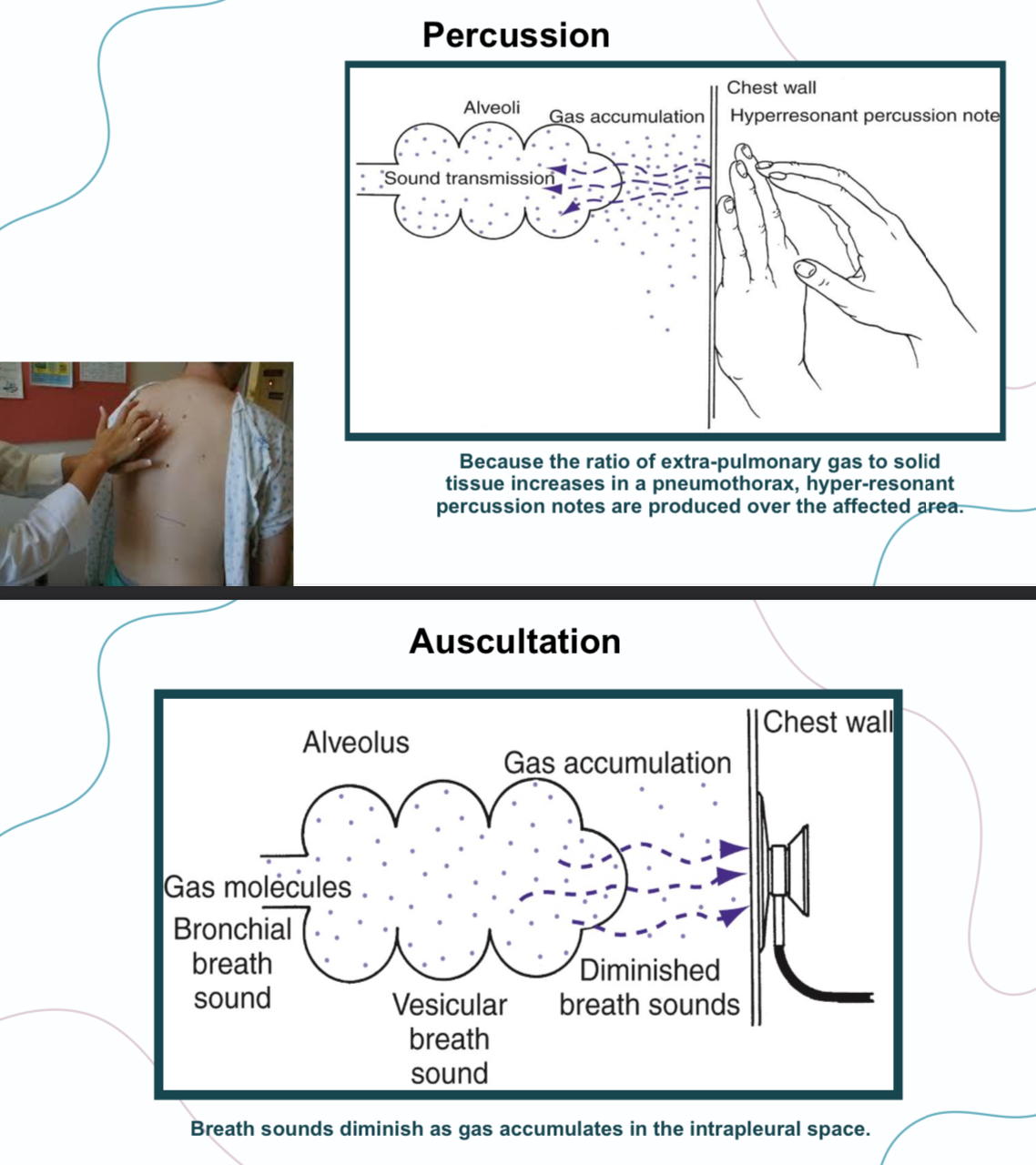
Percussion: hyper resonant note
Ascultation: diminished breathing sounds
What are the signs of special type pneumothorax?
Hypotension
Engorged neck veins
Distant heart sounds
Tracheal shift to the other side
These signs is the dangerous signs if
found in tension pneumothorax patients and
need urgent needle decompression
What are the investigations?
imaging
1- X-Ray ( best option )
2- CT scan
3- ultrasound scan
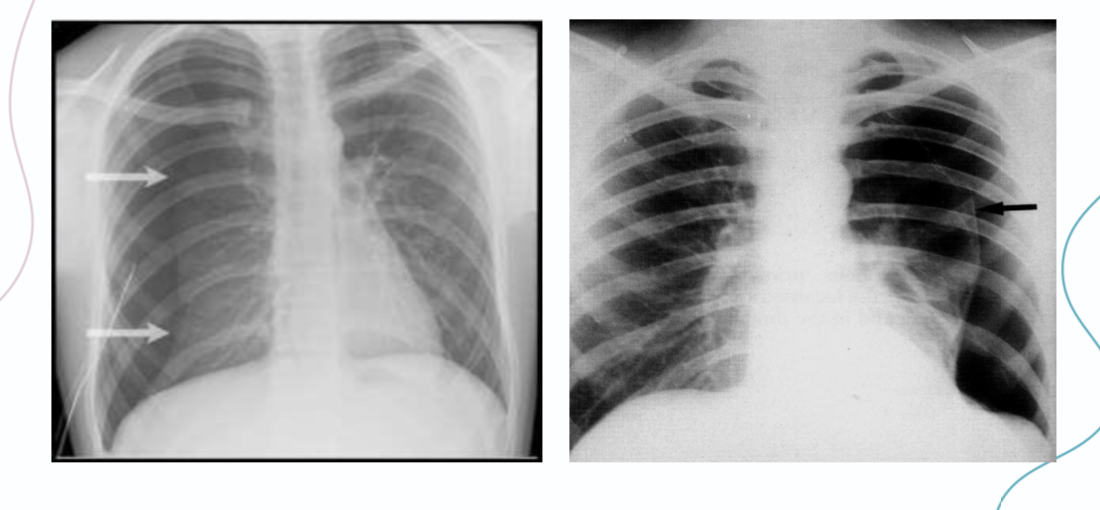
What are the signs of pneumothorax in chest x-ray?
1- absent lung markings
2- hyperlucent hemithorax (jet black)
3- presence of pleural line; The presence of a
pneumothorax is established by demonstrating a
white visceral pleural line on the chest radiograph.
What is the treatment steps of pneumothorax
1- first aid
2- definitive treatment
3- tension pneumothorax
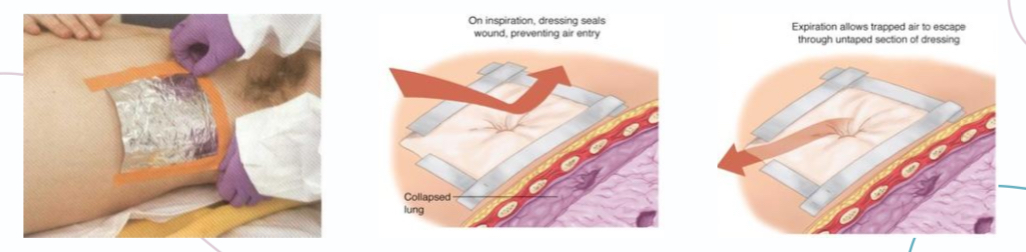
Explain first aid
1- three sided occlusive dressing
2- treat shock if present
3- supplemental O2
Describe definitive treatment steps
1- supplemental oxygen and observation if patient is clinically stable and pneumothorax is small ( < 2-3 cm air between chest wall and lung on chest radiograph)
2- fine needle aspiration if patient is clinically stable but pneumothorax is large (> 3cm rim between lung and chest wall)
3- chest intubation with underwater seal in patients with a large amount of air and clinically unstable
What should you do in the case of tension pneumothorax?
Chest tube insertion with underwater seal for clinically unstable patients
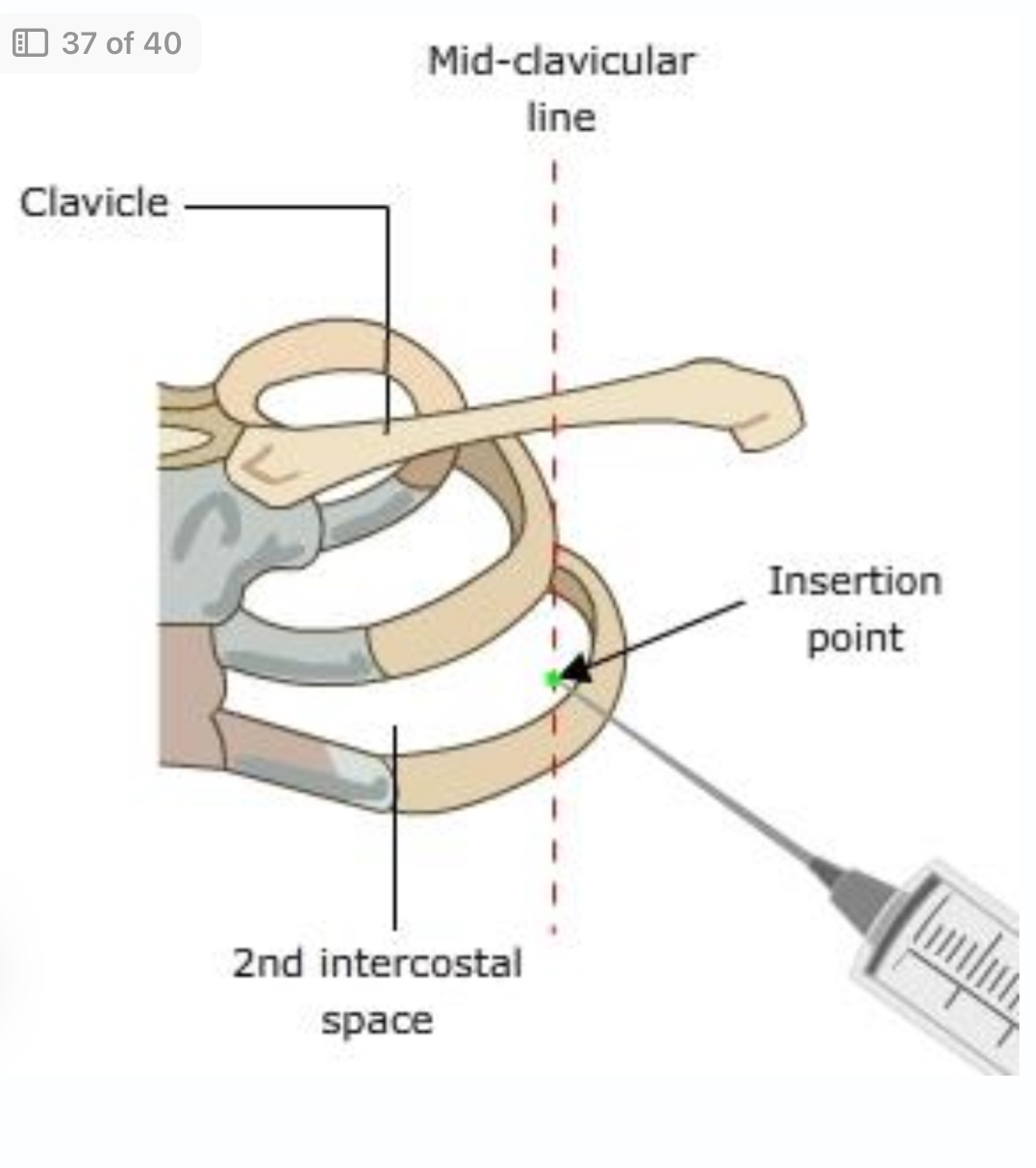
If chest tube insertion is delayed, decompression can be preformed by placing needle into the pleural space at the midclavicular line opposite the second intercostal space at the lower border of the intercostal space
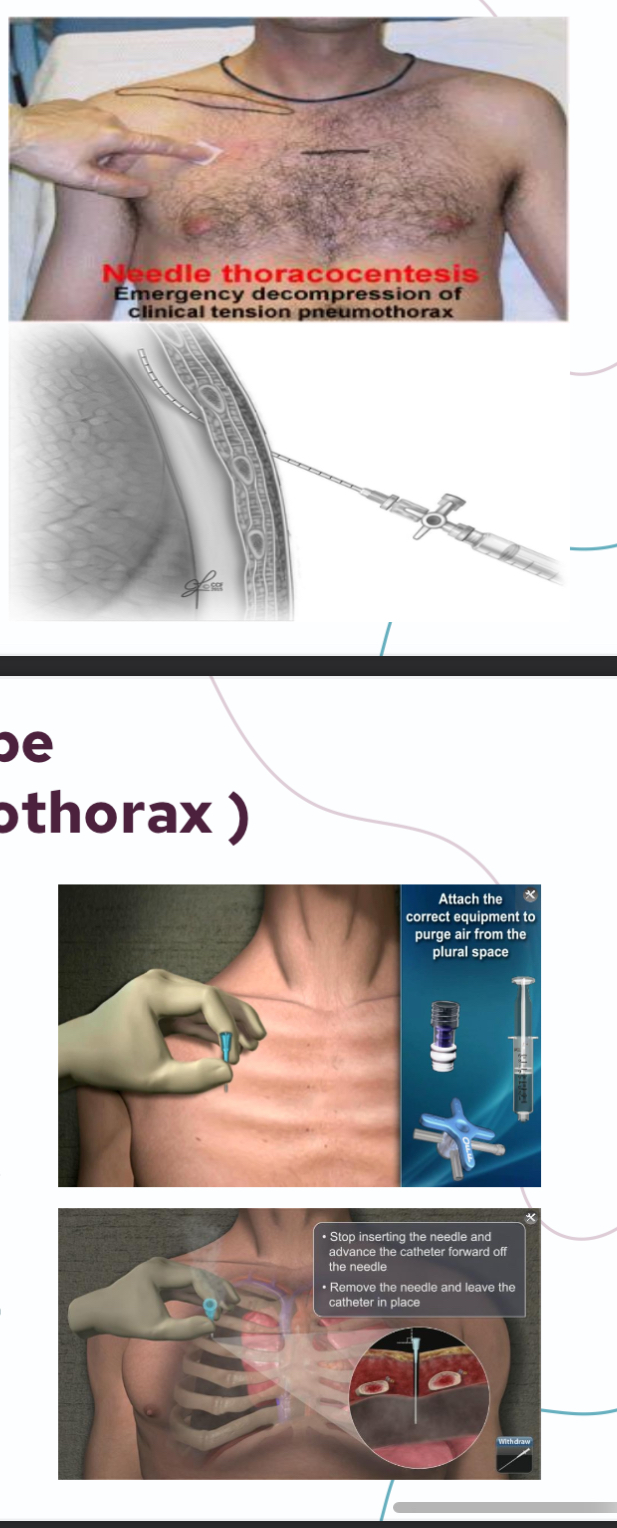
Explain needle aspiration site and indication
Site
§ 2nd intercostal space
§ Mid-clavicular line
§ Insert just above the upper border of the lower rib (to avoid intercostal vessels)
✅ Used in
Clinically Stable pneumothorax
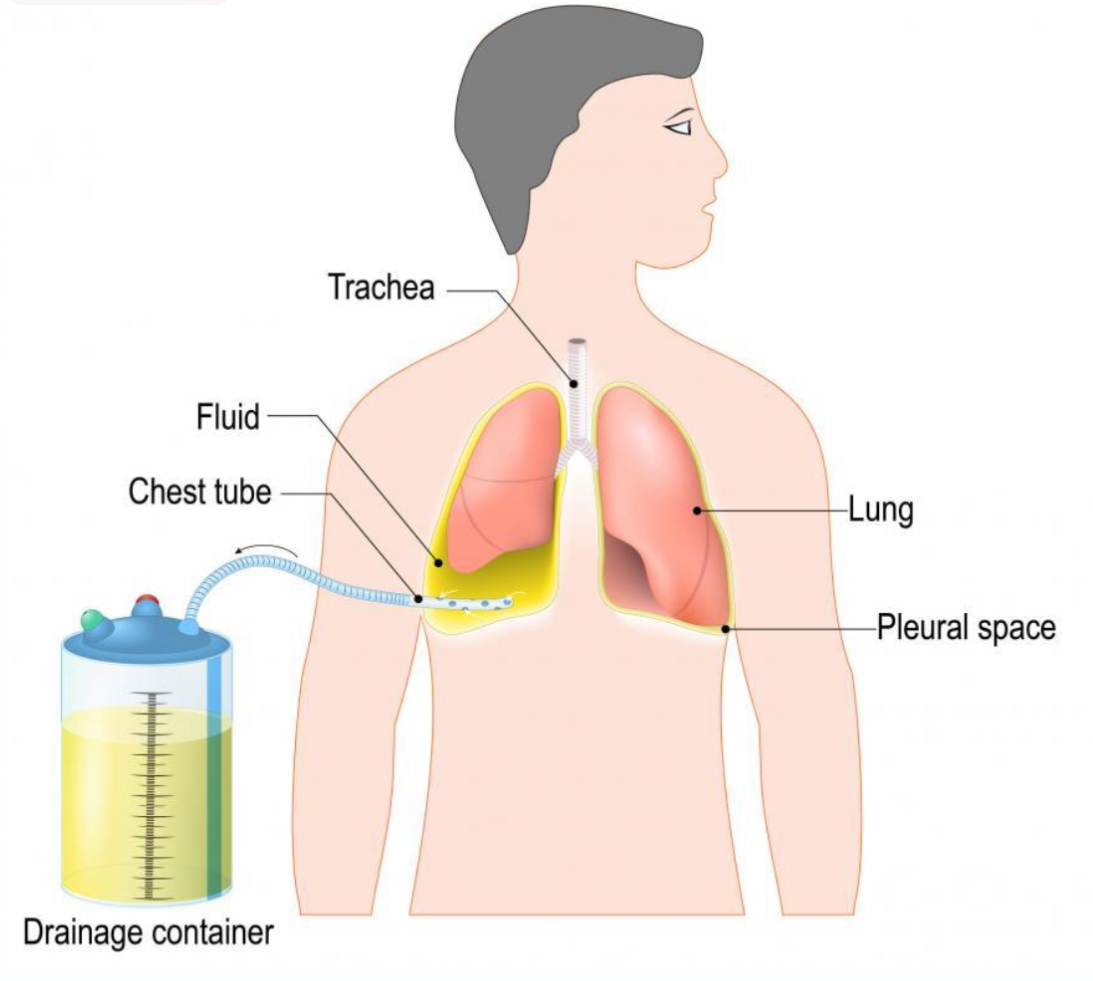
Explain chest tube insertion (underwater seal) site and indication
Site
§ 5th intercostal space
§ Mid-axillary line
§ Insert just above the upper border of the Lower rib (to avoid intercostal vessels)
✅ Used in
• Failed needle aspiration
• Clinically unstable patient
• Tension pneumothorax (after
emergency decompression
Pictures
