Quiz 1 Study Guide
1/59
Earn XP
Description and Tags
UT 609A - OB 1
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Spontaneous abortion
Physiological termination prior to 20 weeks gestation
Hemorrhage of decidua basalis → inflammation and necrosis around region of implantation → detachment of conceptus → UT contractions and expulsion of intrauterine contents via dilated CVX
US role in spontaneous abortions: access presence and amount of retained product of conception in UT cavity
Common etiology: endocrine factors, failure of corpus luteum, chromosomal causes, diabetes, PCOS, smoking, etc.
Complete abortion
Evacuation of all products of conception
Clinical signs:
Rapid decline of HCG levels
Vaginal bleeding w/ tissue/clots
Cramping
Disappearance of pregnancy symptoms
Cessation of pain and bleeding after conceptus is passed
US findings:
Empty uterus with “clean” endometrial stripe
Uterine enlargement
Incomplete abortion
Partial evacuation of products of conception (POC)
Clinical signs:
Slow fall or plateauing of HCG levels
Moderate cramping
Persistent, heavy bleeding
US findings:
Presence of complex collection of echoes in endometrium of retained products of conception (RPOC)
Air bubbles
Retained bony fragments
Hematoma
Persistence of trophoblastic waveforms near EC 5 days post abortion
Anembryonic pregnancy (AKA blighted ovum)
Intrauterine gestational sac is empty
Embryonic demise or failure of embryo to develop
Clinical signs:
Uterus small for dates
Variable HCG levels
Vaginal spotting
Closed CVX
US findings:
No identifiable embryo in GS of >25 mm
Absence of “double sac sign” or “double decidual sign”
Threatened abortion
Bleeding, spotting, or cramping with a closed cervical OS
50/50 odds for normal outcome or spontaneous abortion
Clinical signs:
No reliable signs
More clinical than sonographic
Vaginal bleeding < 20 weeks
Lower abdominal ache
Imminent/inevitable abortion
Occurs when 2+ clinical signs are present
Clinical signs:
Effacement of CVX
Cervical dilation >3 cm
Rupture of membranes
Bleeding for >7 days
Persistent cramping
US findings:
Gestational sac seen in CVX or LUS
Cervical dilatation
Sonolucent crescent around gestational sac
Missed abortion (AKA silent miscarriage)
Fetus is no longer alive but body does not recognize pregnancy loss or expels tissue
US findings:
Embryo in gestational sac w/o fetal heart tones
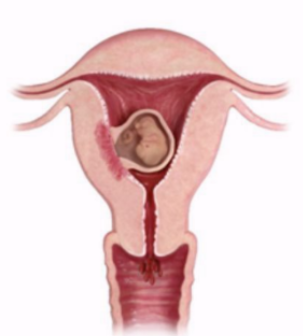
Ectopic pregnancy
Implantation of conceptus outside endometrial cavity
Locations:
Fallopian tubes (95%)
Ampulla (70%) - most common location in FT
Uterine, cervical (high morbidity and mortality), abdominal, ovary
Cause - anything interfering with passage of ovum to UT cavity
Leading cause of maternal mortality and morbidity
If HCG > 2000 + no IUP → investigate for ectopic pregnancy
Treatment - methotrexate (MTX) for ectopic w/o heartbeats
Surgery to remove mass
Risk factors for ectopic pregnancy
Increase in frequency is most likely due to PID and ART use
Prior ectopic
PID
Assisted reproductive technology (ART)
IUDs
Smoking
Increased maternal age
Clinical findings of an ectopic pregnancy
Clinical triad: vaginal bleeding, pain, and palpable mass
Variable HCG levels
Adnexal mass
Pelvic pain and bleeding
Leukocytosis
Fever
Pain referred to shoulder → intraperitoneal hemorrhage
Clinical triad of ectopic pregnancy
Vaginal bleeding
Pain
Palpable mass
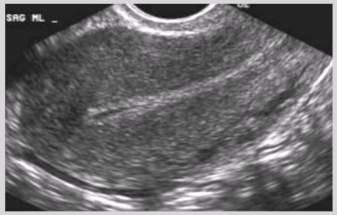
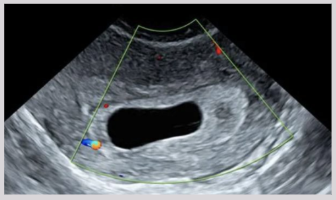
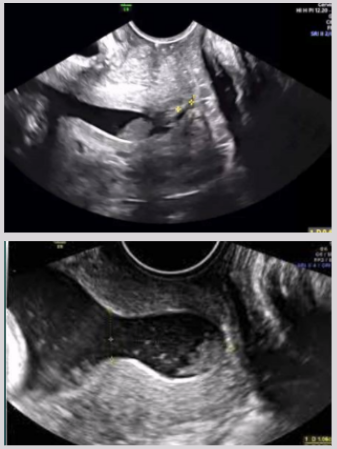
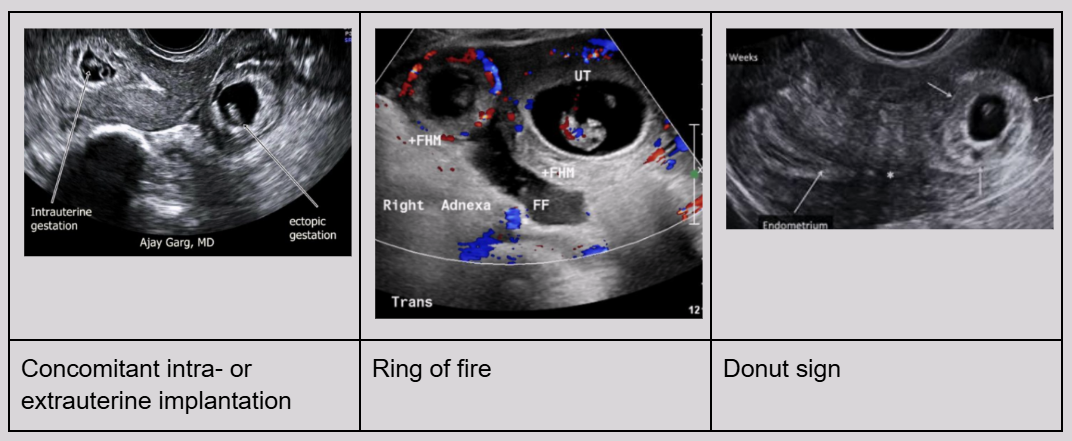
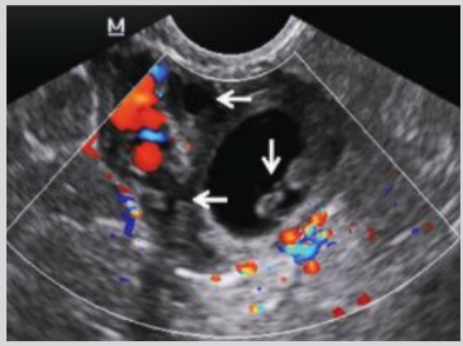
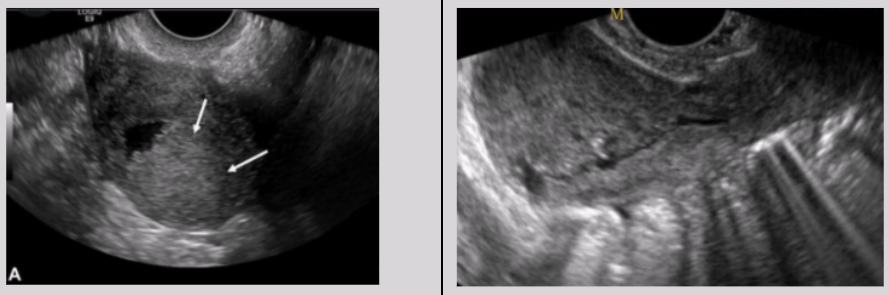
US findings of ectopic pregnancies
Extrauterine GS w/ yolk sac
Empty uterus on EV, if hCG levels are > 800-1000 mIU/mL
Adnexal mass, separate from ovaries
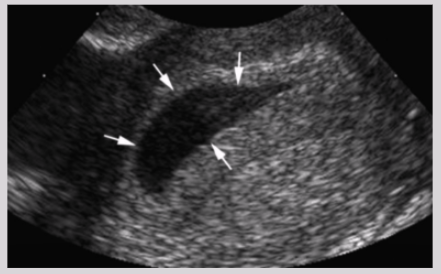
Free fluid in cul-de-sac, adnexa, or pericolic gutters
Concomitant intra- or extrauterine implantation
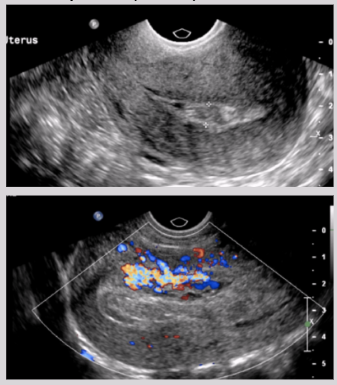
Ring of fire - trophoblastic tissue surrounding conceptus
Donut sign
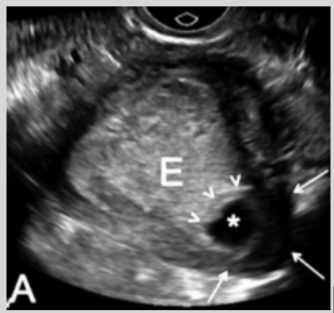
Pitfalls when scanning for ectopic pregnancies
Pseudogestational sacs
Corpus luteum cyst vs. adnexal ectopic both have ring of fire appearance
Corpus luteum cyst - more hypoechoic
Adnexal ectopic - echogenic decidual donut
Heterotopic pregnancy
Presence of multiple gestations, one in UT cavity and other outside of UT
Cornual ectopic pregnancy
Occurs in uterine horn
High susceptibility of rupturing
Associated w/ uterine anomalies
Most deadly along w/ interstitial
High vascularity from UT arteries
Intramural ectopic pregnancy
Gestational sac implanted into the myometrium
Causes: past surgical procedures
Ex: myomectomy or C-section
On the rise due to rise of C-section usage

Cervical ectopic pregnancy
Implantation in endocervical canal
Risk factors:
Previous D&C
Amniotic anomalies
Endometriosis
IUD
IVF
C-section scar ectopic pregnancy
Gestational sac implants into myometrium of previous c-section scar
Ovarian ectopic pregnancy
Gestational sac implants in the ovary
Increasing incidence due to PID and IUD usage
IUD prevents implantation into UT
Symptoms: low abdominal pain and bleeding
Abdominal ectopic pregnancy
Gestational sac implants into abdominal cavity
Symptoms: general malaise, nausea, vomiting, vaginal bleeding
Risk factors: PID, endometriosis, tubal damage
Possible sites: spleen, UT surface, liver, diaphragm, bowel, etc.
Acute rupture of tubal ectopic pregnancy
Ectopic pregnancy not seen due to amount of blood and clot

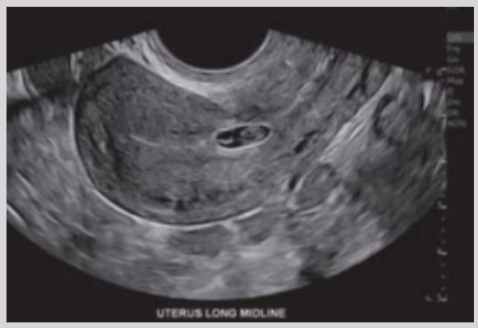
Gestational sac
Well-defined circle of echoes in central fundus of UT
The gestational sac grows ___ mm/day prior to 6 weeks
1
How to measure mean sac diameter (MSD)
length + width + height / 3
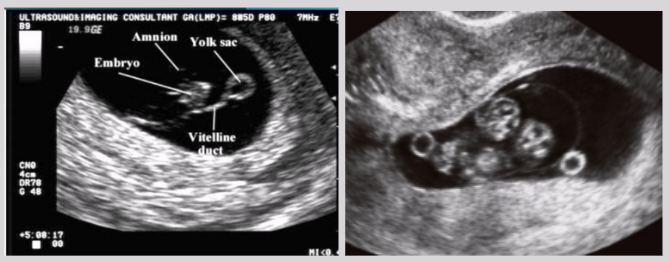
Double bleb sign
Sonographic feature of gestational sac containing yolk sac + adjacent amniotic sac
Appearance of 2 small bubbles

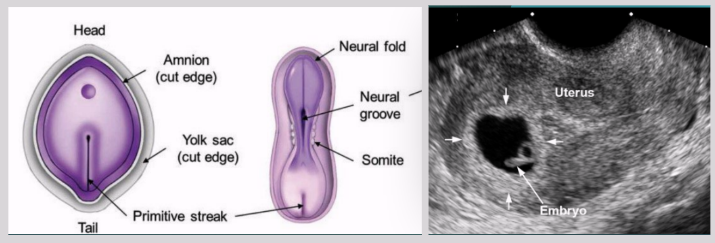
Trilaminar disk
Early stage in development of triploblastic organisms
Gastrulation
Formation of primitive streak along epiblast disc
Primitive streak
Formed from proliferation and movement of epiblast cells to the median plane of embryonic disc
Once it appears, can identify embryo’s craniocaudal axis
Sacrococcygeal teratoma (SCT)
Most common neoplasm in newborn
Formed from remnants of primitive streak
Benign tumor that has elements of incomplete differentiated germ layers
Mostly found in females

Three germinal layers of the trilaminar disc
Ectoderm - remaining epiblast cells
Epidermis, nails, hair, sebaceous glands
Mesoderm - infiltrated epiblast cells
Muscles, skeleton, cartilage
Endoderm - remaining hypoblast cells
Lines GI tract, aka stomach, colon, liver, bladder
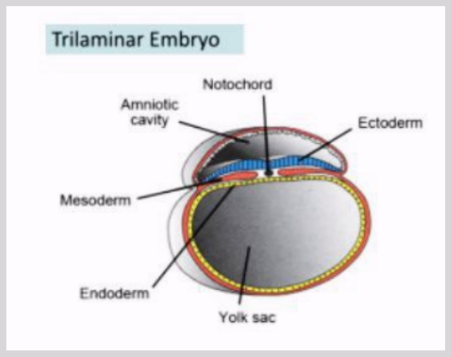
Yolk sac
Provides some of the first cells + circulation necessary for life
Produces RBCs needed for primitive circulatory system
Source of nutrients
Connected to embryo via vitelline duct
Located within chorionic cavity
Emergence: first few days of gestation
~ 7 weeks, role diminishes and is supplanted by placenta
Disappears around week 10
Useful in assessing amnion number in multiple gestations
US appearance: spherical w/ sonolucent center and clearly defined echogenic walls
The yolk sac should always be visualized when the MSD > ___ mm (~ 5.5 weeks)
8
Trophoblast
Thin layer of cells that protect developing embryo, attaches it to the wall of UT, and forms part of placenta
Gestational trophoblastic disease (GTD)
Group of interrelated tumors originating from placenta
Usually occurs shortly after UT implantation of fertilized ovum
Histological confirmation is mandatory for Dx
Gold standard = histological confirmation post-curettage
Clinical findings of GTD
Enlarged UT
Grossly elevated hCG levels
Hyperemesis gravidarum - severe nausea and vomiting
UT bleeding in first trimester
Absence of FHT
Theca-lutein cysts (50% of time due to elevated hCG)
Onset of preeclampsia - HTN, proteinuria, edema, headaches
Hyperthyroidism
Molar pregnancy association w/ very early onset preeclampsia
Molar placentas produce more anti-angiogenic proteins → produce systemic endothelial dysfunction → HTN, proteinuria, etc.
Endothelium - thin membrane lining heart and blood vessels
Endothelial cells - controls vascular relaxation and contraction
Forms of GTD
Complete hydatidiform mole
Partial mole
Mole w/ coexisting fetus
Hydroponic degeneration of placenta
Persistent trophoblastic neoplasia
Invasive mole (chorioadenoma destruens)
Uterine choriocarcinoma (gestational choriocarcinoma)
Placental site trophoblastic tumor
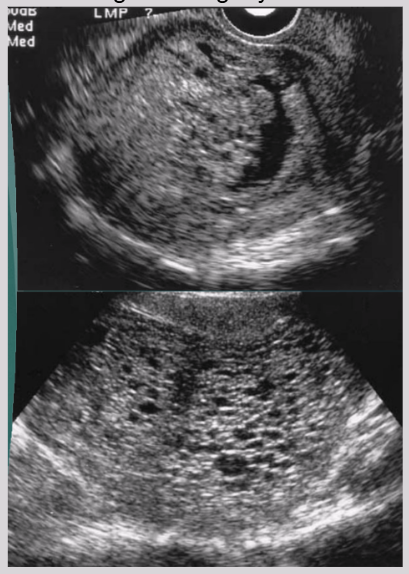
Complete hydatidiform mole
Most common form of GTD
Chorionic villi are diffusely hydropic + surrounded by trophoblasts
No fetal tissue identified
Maternal risk factors: young age or over 40 y/o
GTD → high hCG → theca-lutein cysts (50% of cases)
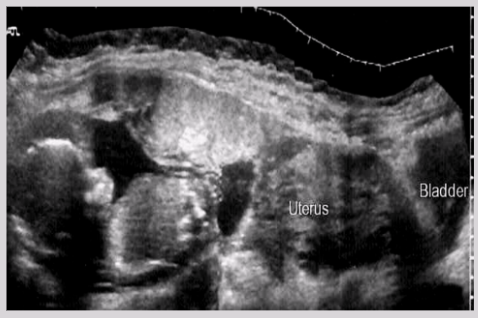
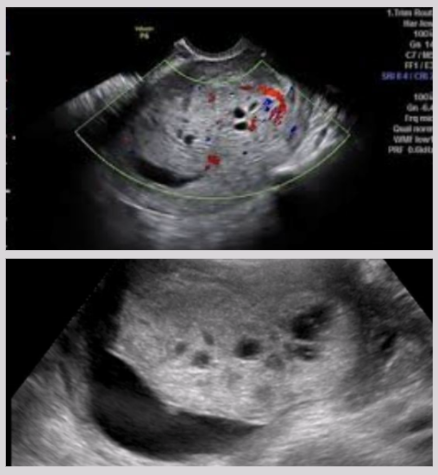
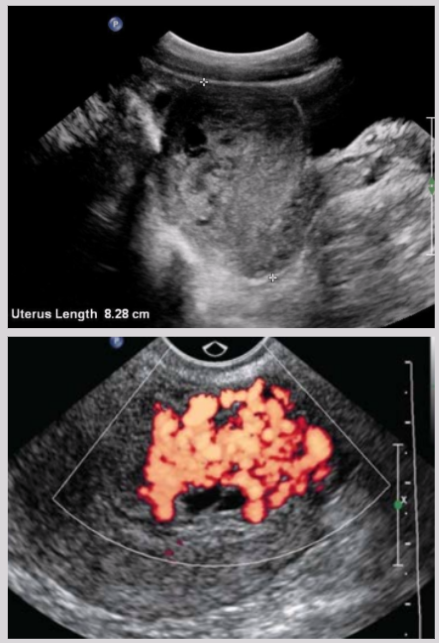
US findings of complete hydatidiform mole
Endometrial cavity filled with heterogeneous echogenic material
Vesicular appearance - multiple cysts
Increased UT size
Fluid collection around molar mass
Mimics appearance of degenerating myoma
Partial mole
Triploidy - fetus w/ extra set of chromosomes
Normal 23 pairs of chromosomes, 46 total
Fetus is usually non-viable and triploid due to structural abnormality
Will always be evacuated after diagnosis
US findings of partial mole
Molar placenta - grossly enlarged placenta + cystic areas
focal/diffuse areas of increased echogenicity in or around placenta
Presence of fetal tissue

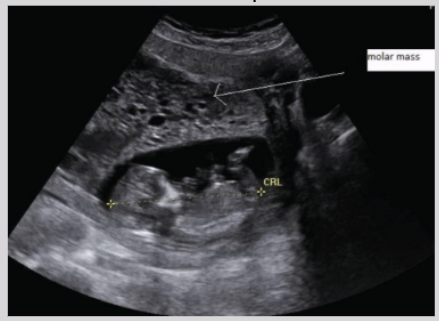
Mole w/ coexisting fetus
Outside of realm of true GTD
Technically 2 conceptions
1. Normal pregnancy
2. Molar pregnancy
US findings of mole w/ coexisting fetus
Similar to partial mole but with viable and complete fetal tissue
Hydroponic degeneration of placenta
Characterized by presence of numerous cystic areas within enlarged placenta
Not considered part of GTD spectrum
Associated w/ partial mole and paternal triploidy
Simple hydropic degeneration in first trimester → increased risk of fetal demise
Persistent trophoblastic neoplasia
Pregnancy complication following GTD
Treatment of molar pregnancy → molar tissue still remaining → grows into tumor
Just under 100% cure rate
Treatment - chemotherapy
Highest risk - severe histological types of initial trophoblastic proliferation
Lowest risk - partial molar pregnancy
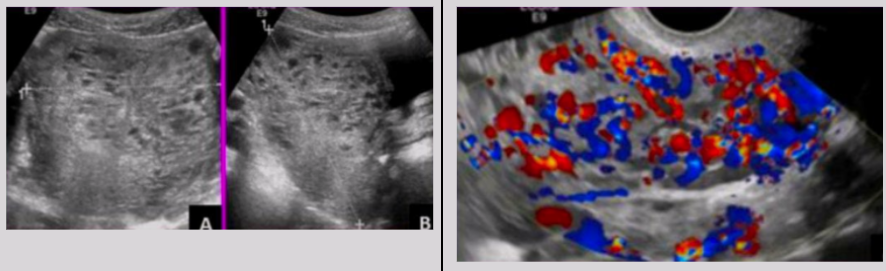
US findings of persistent trophoblastic neoplasia
Heterogeneous uterine mass
Multiple lacunae surrounding mass w/ high-amp low-resistance blood flow
Invasive mole (AKA chorioadenoma destruens)
Rare molar tissue that invades myometrium and adjacent anatomic structures
Malignant non-metastatic form of GTD
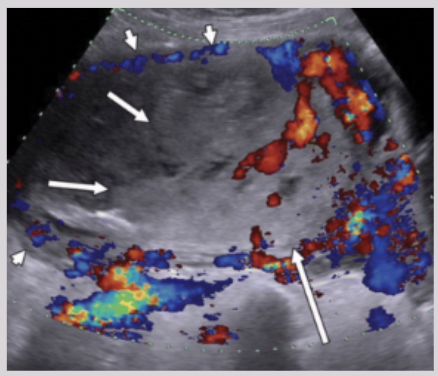
US findings of invasive mole
Focal/diffuse echogenic material in endometrium
Possible extension to myometrium
Irregular sonolucent areas surrounding trophoblastic tissue
Swiss-cheese appearance
Hypervascular
Theca-lutein cysts
Uterine choriocarcinoma (AKA gestational choriocarcinoma)
Pure epithelial tumor
Implantation of trophoblast → two layers
Synctiotrophoblast (ST)
Cytotrophoblast
Absence of hydropic villi
Appearance of sheets/foci of trophoblasts identified w/ background of hemorrhage and necrosis
Malignant metastatic form of GTD
US findings of uterine choriocarcinoma
Enlarged UT
Eccentrically situated irregular complex mass in UT
Low-resistance blood flow around mass
Placental site trophoblastic tumor
Arises from placental implantation site
Tumor can infiltrate myometrium and grown between smooth-muscle cells
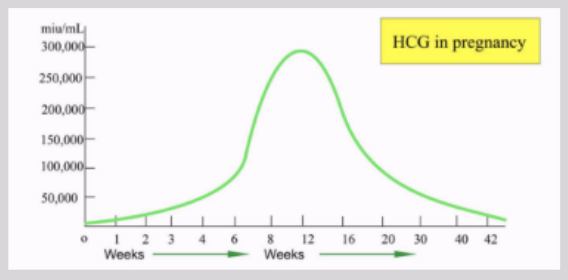
Human chorionic gonadotropin (HCG)
Glycoprotein secreted by physiologically active trophoblastic tissue
Presence of HCG in maternal blood = strongest indicator of presence of gestation
Shows ~6-8 days post conception
Doubles every 2 days (~ 48 hours)
Peaks at 10 weeks' gestation before declining and stabilizing
Undetectable HCG → excludes gestation from anywhere in body
If HCG plateaus or falls prematurely → pregnancy may not be viable
Most sensitive test: quantitative serum (blood) test
HCG doubles every __ days
2
HCG peals at __ weeks' gestation before declining and stabilizing
10
Discriminatory levels of HCG
Levels in which intrauterine pregnancy (IUP) is always going to be seen
Endovaginal: > 800-1000 mIU/mL
Transabdominal: > 1800 mIU/mL
Pregnancy not seen in endometrial cavity at these levels → failed pregnancy highly suspected
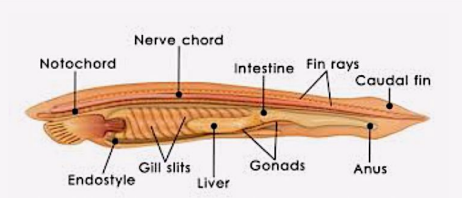
Notochord
First mesodermal tissue to form
Formation of the primitive node and streak and the rod-shaped group of cells that define the body’s primary supporting axis
Forms within embryonic plate between ectoderm and endoderm
Source of midline signals that pattern the surrounding tissues + acts as skeletal element for developing embryo
Early embryo, induces development of structures
Late embryo, develops into nucleus pulposus of the discs of the spinal column
Bradycardia
Abnormally slow heart action
Tachycardia
Abnormally rapid heart action
FHR at 5-6 weeks
100-115 bpm
FHR after 9 weeks