Disorders of the Esophagus
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
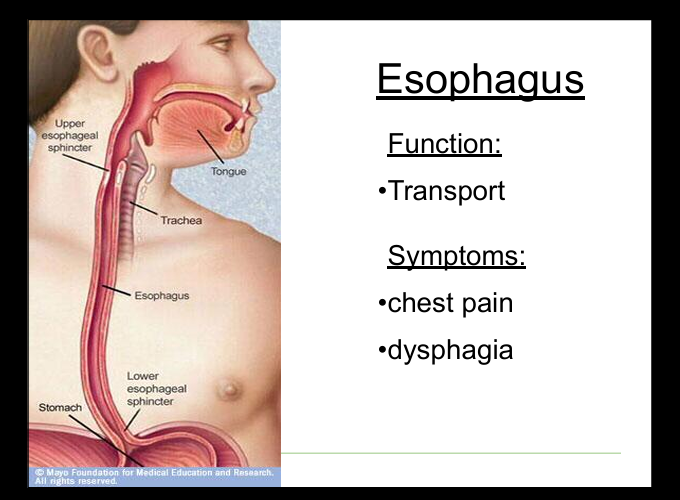
Symptoms of esophageal disease
Chest pain, dysphagia, odynophagia, regurgitation.
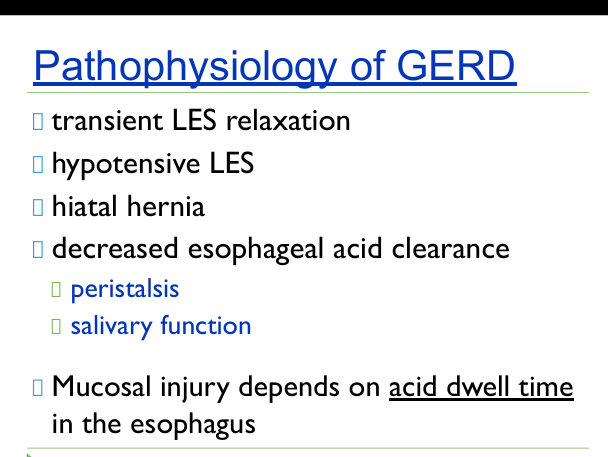
Pathophysiology of GERD
Reflux of gastric contents due to transient LES relaxations, hypotensive LES, hiatal hernia, impaired clearance due to peristalsis or salivary function
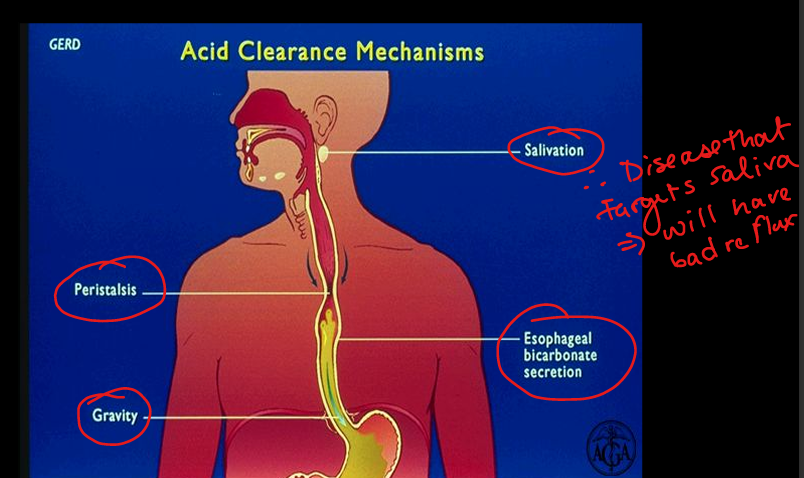
GERD acid clearance mechanisms
Peristalsis, saliva/bicarbonate, gravity.
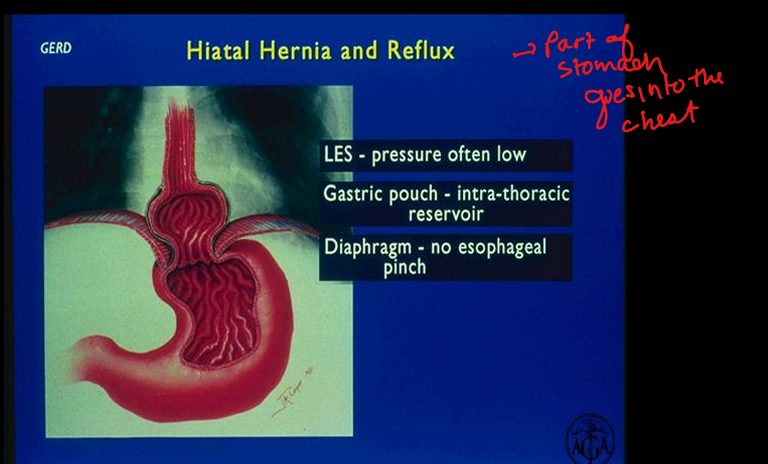
Hiatal hernia effect on GERD
Weakens LES, creates intrathoracic gastric pouch, reduces diaphragmatic pinch.
GERD complications
Erosions, ulcers, strictures, Barrett’s esophagus, adenocarcinoma.
GERD symptoms
Heartbuirn(pyrosis), Epigastric abdominal pain, regurgitation, nausea, bleching, dysphagia, chest pain, hiccups, respiratory symptoms
Clinical approach to heartburn
History, trial of PPI, lifestyle changes, EGD for alarm symptoms, pH monitoring if unclear.
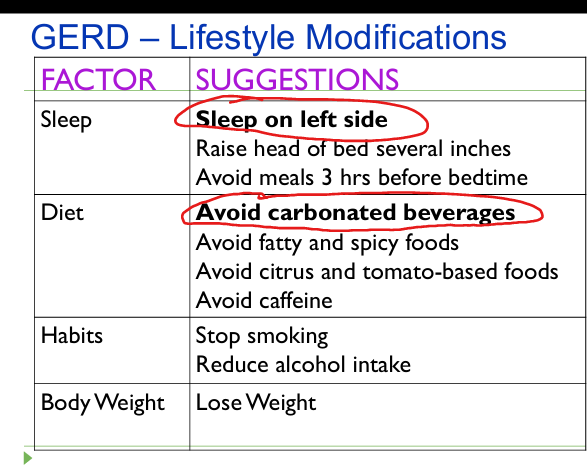
Lifestyle modifications for GERD
Sleep on left side, avoid carbonated beverages, elevate head of bed, avoid late meals, avoid trigger foods, stop smoking, weight loss.
Pharmacologic therapy for GERD
Antacids, H2 blockers, PPIs (most effective).
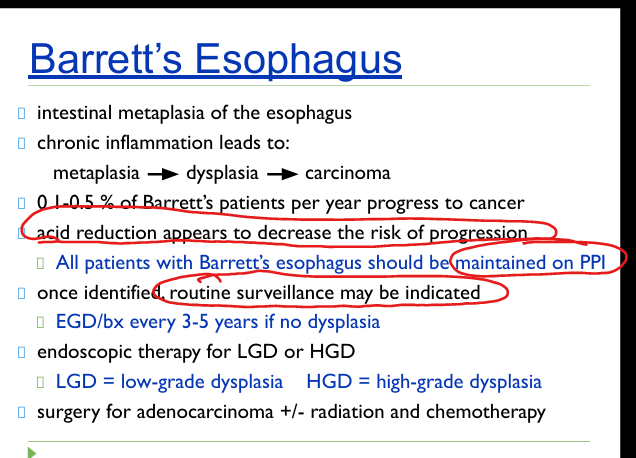
Definition of Barrett’s esophagus
Intestinal metaplasia replacing normal squamous epithelium in distal esophagus.
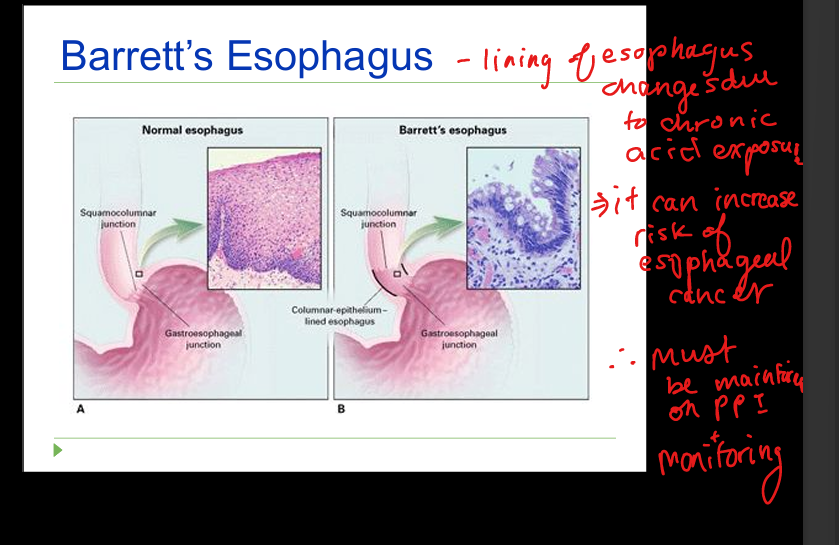
Management of Barrett’s
PPI therapy for all; surveillance EGD every 3–5 years if no dysplasia; endoscopic therapy for LGD/HGD.
Barrett’s cancer risk sequence
Chronic inflammation → metaplasia → dysplasia → adenocarcinoma.
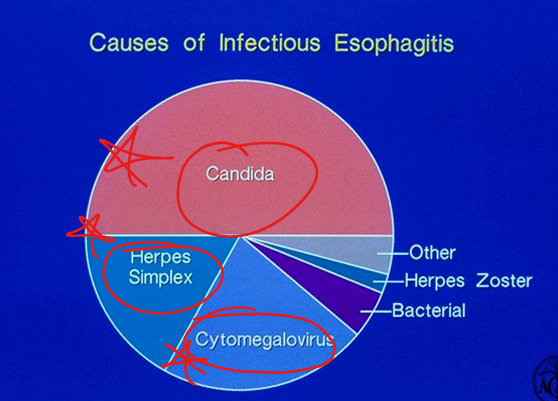
Common organisms in infectious esophagitis
Candida, HSV, CMV.
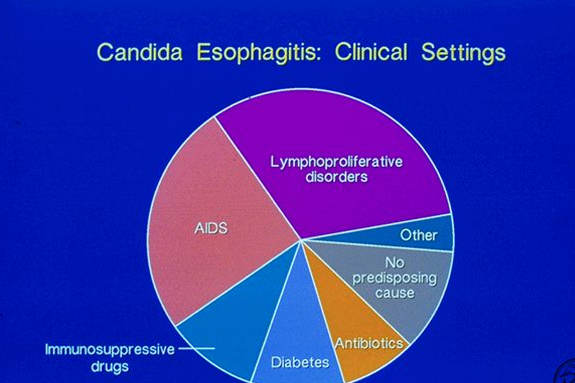
Candida esophagitis risk factors
Immunosuppression, diabetes, antibiotics, steroids.
Chest pain differential: esophageal
GERD, esophagitis, pill injury, radiation injury, Boerhaave’s, caustic ingestion, motility disorders.
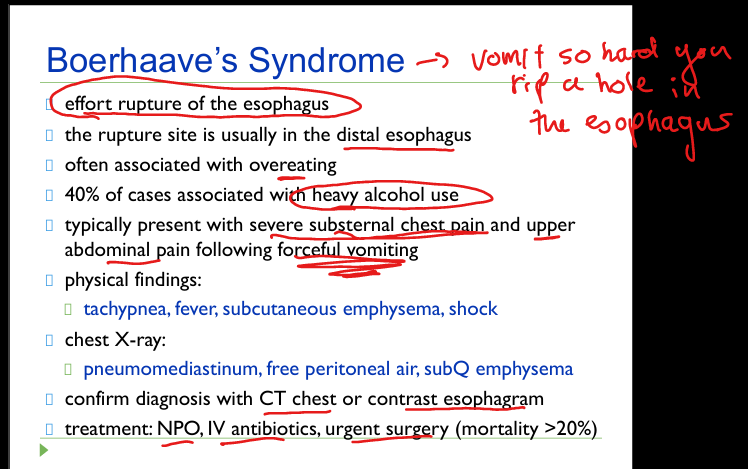
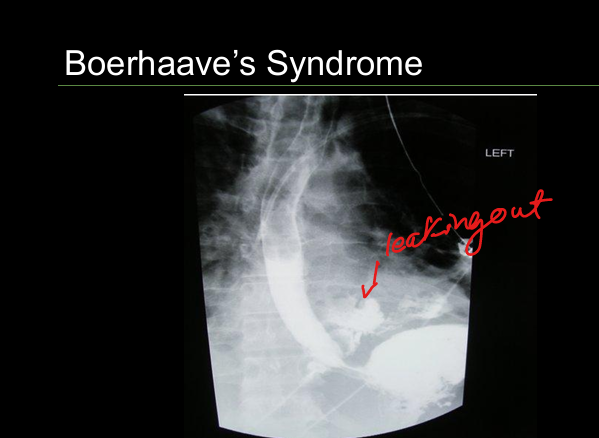
Boerhaave’s syndrome
Full‑thickness esophageal rupture after forceful vomiting; severe chest pain; subcutaneous emphysema.
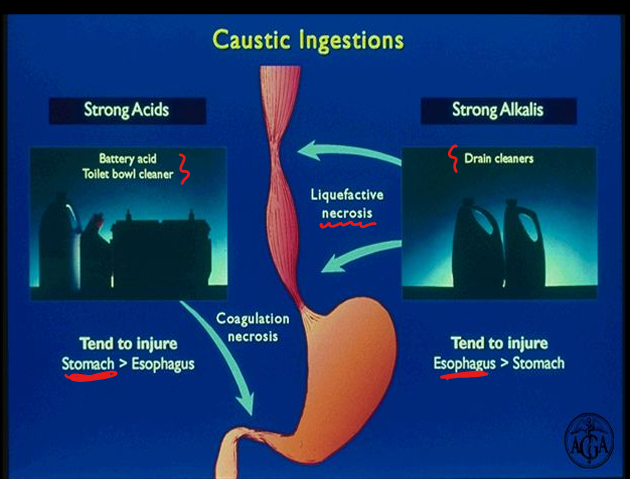
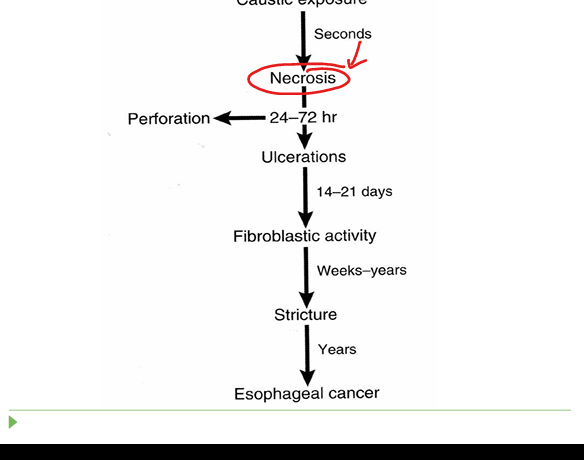
Caustic ingestion
Acids → stomach injury; alkali → esophageal injury; risk of perforation and strictures.
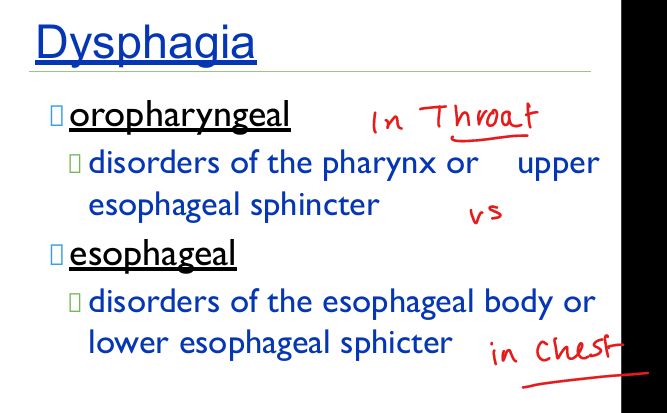
Oropharyngeal vs esophageal dysphagia
Oropharyngeal = difficulty initiating swallow; esophageal = food “stuck” in chest.
Symptoms of oropharyngeal dysphagia
Coughing, choking, nasal regurgitation, repeated swallows.
Causes of oropharyngeal dysphagia
Stroke, Parkinson’s, ALS, MG, polymyositis, Zenker’s diverticulum, decreased saliva.
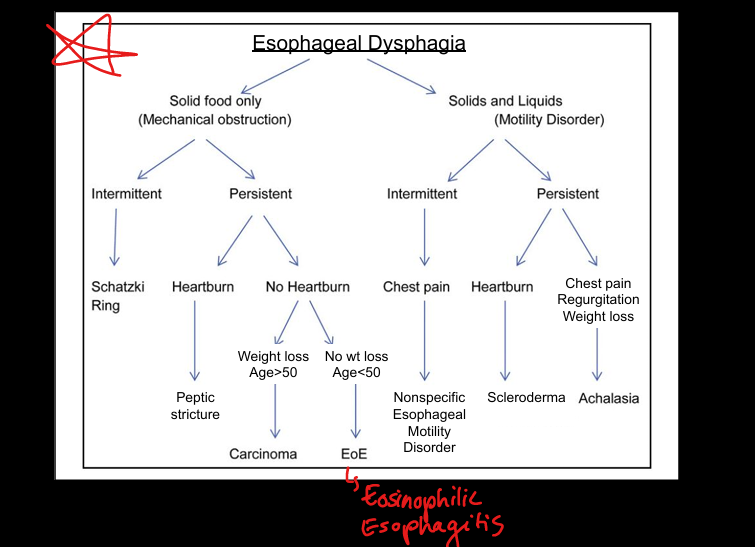
Symptoms of esophageal dysphagia
Food sticking in chest; bland regurgitation without acid taste.
Schatzki ring
Thin mucosal ring at GE junction; intermittent solid food dysphagia.

Peptic stricture
Chronic GERD → fibrosis → progressive solid food dysphagia.
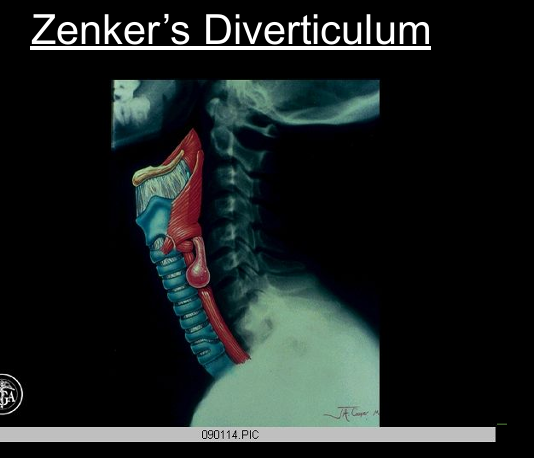
Zenker’s diverticulum
Outpouching above UES; regurgitation of undigested food; halitosis.
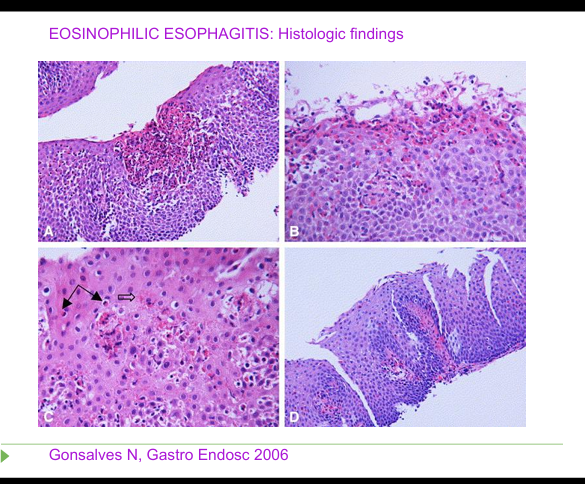
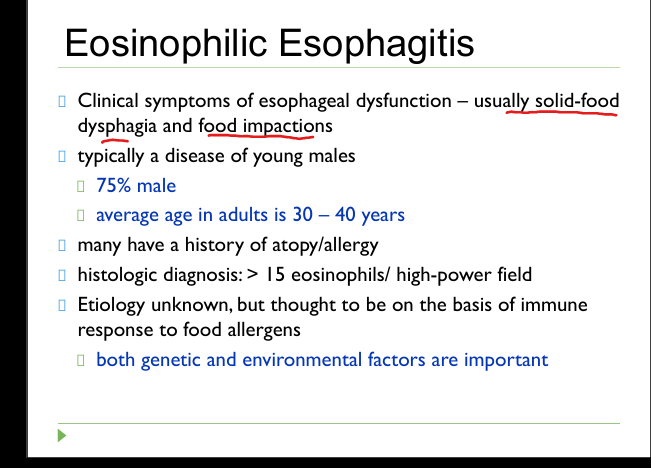
Definition of Eosinophilic Esophagitis
Solid‑food dysphagia + >15 eosinophils/HPF; young males; atopy.
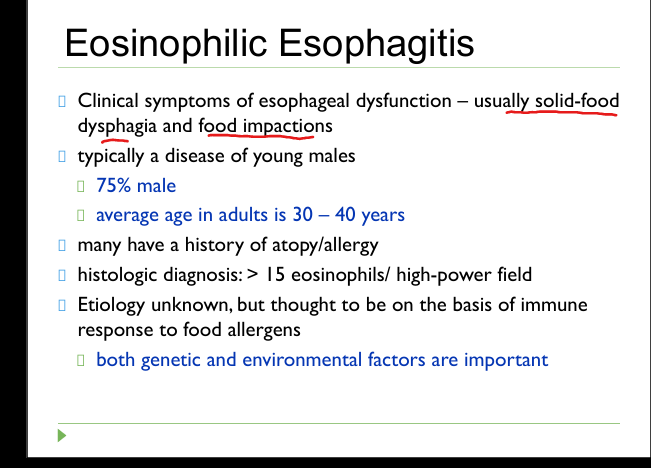
Esophilic Esophagitis symptoms
Dysphagia, food impaction, chest pain.
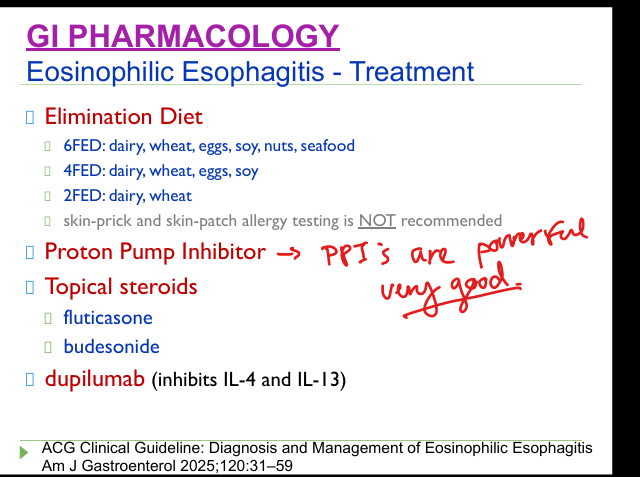
Eosinophilic Esophagitis treatment
Elimination diet (6‑FED/4‑FED/2‑FED), PPI, topical steroids (fluticasone, budesonide), dupilumab.
Achalasia pathophysiology
Loss of inhibitory NO‑producing inhibitory neurons → No peristalsis + incomplete LES relaxation.
Achalasia symptoms
Solids and liquids dysphagia, regurgitation, chest pain, weight loss.
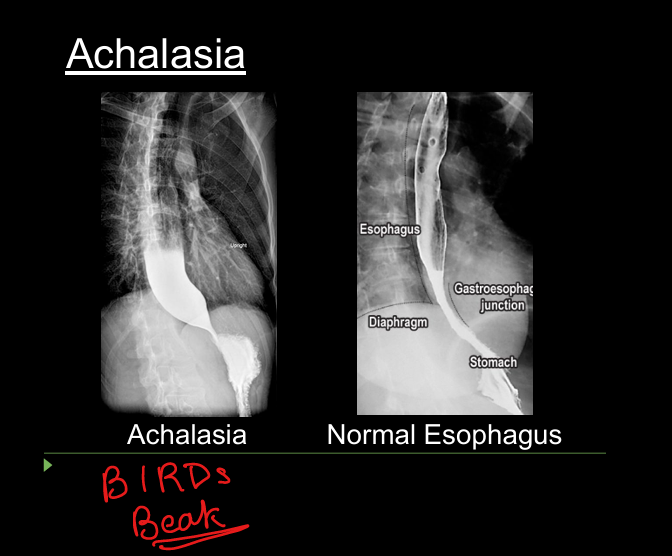
Achalasia manometry + imaging sign
Aperistalsis + incomplete LES relaxation. BIRDS BEAK
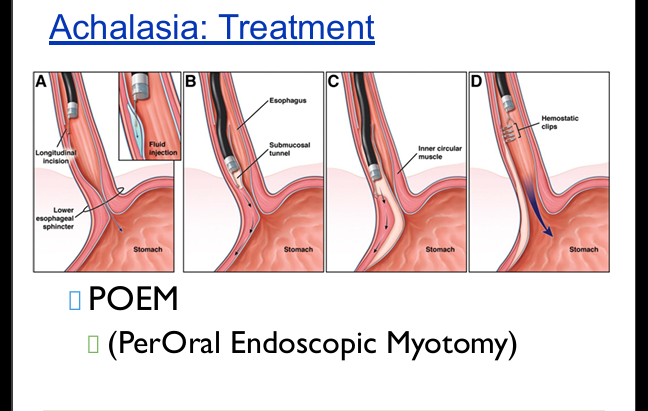
Achalasia treatment
Botox, pneumatic dilation, Heller myotomy, POEM.
Scleroderma esophagus pathophysiology
Smooth muscle atrophy + fibrosis → weak peristalsis + loose LES.
Scleroderma symptoms
Severe GERD, dysphagia, nocturnal aspiration.
Scleroderma treatment
Aggressive reflux control with PPIs; avoid smooth muscle relaxants; dilate strictures.
Nonspecific esophageal motility disorders
Chest pain, intermittent dysphagia; not progressive; associated with anxiety/depression.
Dysphagia algorithm
Solids only = mechanical obstruction; solids + liquids = motility disorder.