Lecture 33: Chest Trauma and Pneumothorax I
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
Negative
Pressure in pleural space is _____________ with respect to alveolar pressure
Pneumothorax
accumulation of air in the pleural space
Open Pneumothorax
open thoracic wall injury causing accumulation of air in the pleural space
Closed Pneumothorax
Alveolar Injury/tearing resulting in accumulation of aire in the pleural space
Inspiration
During _________________, Air enters the pleural space and accumulates, leading to collapse of ipsilateral lung
Decreases
In a pneumothorax, the tidal volume of the healthy lung ________________
Pneumothorax
-decreased vital capacity
-decreased arterial PO2 (Hypoxia)
-areas of low V/Q ratios
-Right to Left shunt
-Alveolar Hypoventilation
Pneumothorax
-sudden onset of ipsilateral chest or shoulder pain
-dyspnea
-cough
-mild resting tachycardia
-tachypnea
-unilateral decreased breath sounds
Pneumothorax
-respiratory distress
-hyperresonance to percussion
-unilateral enlargement of hemithorax
-decreased chest excursion with respiration
Chest X-Ray
most important initial test if there is a suspected Pneumothorax
Upright (except Tension pneumothorax)
what position is recommended for CXR for suspected Pneumothorax
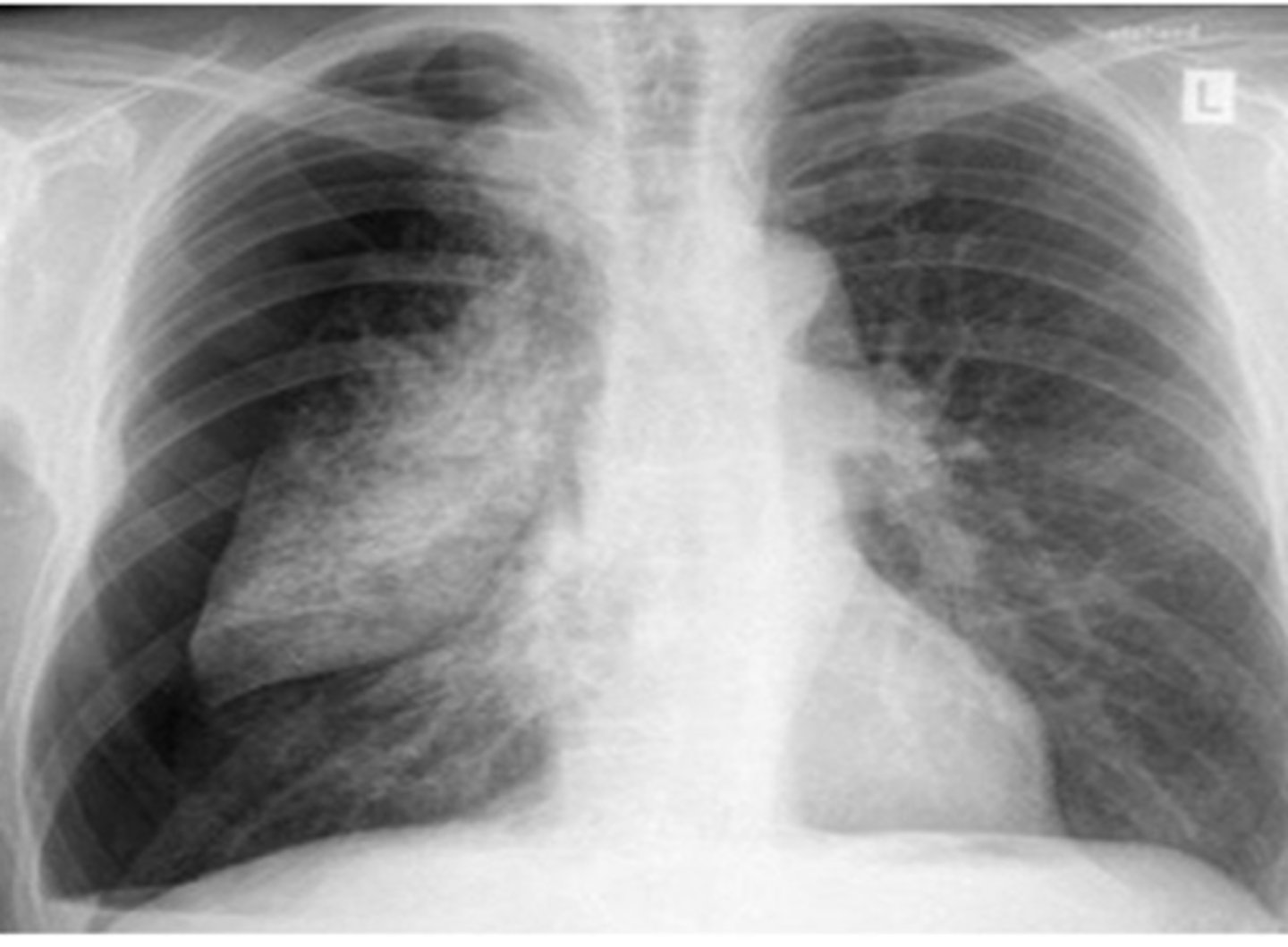
Pneumothorax
Thin visceral pleural line lying parallel to the chest wall separated by a radiolucent band containing no lung markings

Pneumothorax
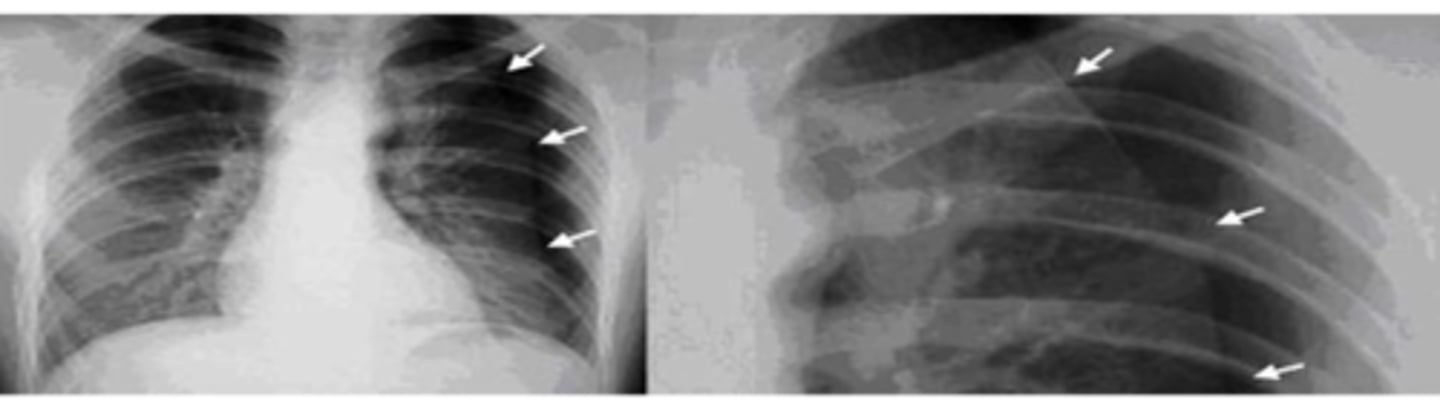
Pneumothorax
Expiratory
Historically ______________ CXR thought to help optimize visualization of small ptx, but they are not more sensitive so not generally recommended
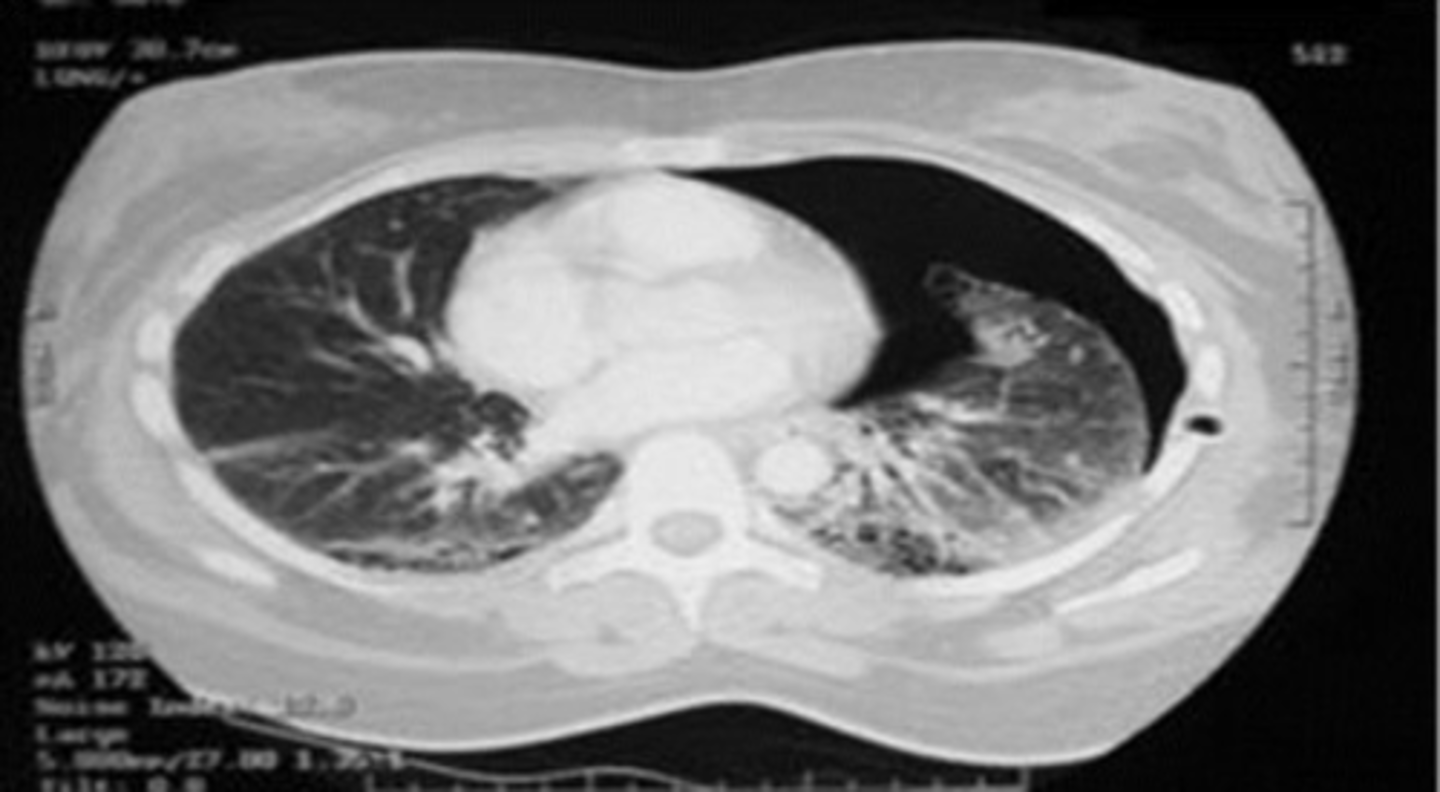
CT
-much more sensitive than plain CXR
-more accurate in sizing ptx than plain CXR
-not routinely ordered in evaluation of suspected pneumothorax
-can identify blebs or bulla as source of primary pneumothoracies
Pneumothorax
Primary Pneumothorax
-Spontaneous PTX in pts without known pulmonary dx
-<40 yo
-occurs at rest, not related to physical exertion
-related to cigarette smoking and Marfan's syndrome
Primary Pneumothorax
-chest pain and dyspnea
-acute onset, ipsilateral
-often pleuritic
-vital signs normal
-tachycardia
-Ipsilateral: decreased movement with breathing, hyperresonant to percussion, decreased breathing sounds, and decreased fremitus
• Tall patients
• Those who continue to smoke
who is at greatest risk for recurrence or primary pneumothorax
Secondary Pneumothorax
• PTX in setting of underlying lung disease
• Peak age 60-65 years; male to female 3:1
• More likely to present with dyspnea & more severe symptoms . Why?
• Much higher mortality
Secondary Pneumothorax
-primary symptom is dyspnea; often severe and out of proportion to size of pneumothorax
-chest pain
-hypoxia and hypotension
-vitals signs abnormal
Iatrogenic Pneumothorax
assoc with:
-Transthoracic needle aspiration or biopsy
-Thoracentesis
-Transbronchial biopsy
-Subclavian or IJ central line catheterization
-Mechanical ventilation
-CPR
-Nasogastric tube (NG) placement
• Eliminate air from the pleural space
• Decrease likelihood of occurrence
the two major goals of treatment of a pneumothorax
• Observation*
• Supplemental Oxygen*
• Simple aspiration*
• Tube thoracostomy*
treatment of a pneumothorax
• Tube thoracostomy with pleurodesis
• Thoracoscopy with oversewing of blebs & pleurodesis
• Open thoracotomy
prevents recurrence of a pneumothorax
• Small PSP (< 2-3 cm)
• Patient stable
• Observation for SSP NOT generally recommended
eligibility of observation of pneumothorax
• Observe for 3-6 hours
• Repeat CXR
• If no progression & patient stable, can discharge home
• Pts should return in 24-48 hours for f/u CXR
guidelines for observation of a pneumothorax
Increases
Supplemental O2 ________________ rate of pleural air absorption
High %O2
Pts given ____________ reabsorb their pneumothorax approx 4x faster
Simple Aspiration
• Initial tx of choice for most pts with primary spontaneous pneumothraces
• NOT generally recommended for secondary spontaneous pneumothorax
• Lower success rates; generally require chest tube
• Less pain - smaller needle
• Hospitalization often not required or \/ stay; less expensive
Tube thoracostomy
If aspiration unsuccessful, __________________________ required
Tube Thoracostomy ("Chest Tube")
-Historically most common initial treatment for ptx
-Rapid re-expansion of underlying lung
-Indications: large pneymothoraces, or pneumothorax where pt is unstable
32-40
tube size if associated with hemothorax/trauma
4th-5th ICS (about nipple level)
Mid to anterior axillary line
what is the location of chest tube placement
Pleurodesis
Creation of fibrous adhesion between visceral & parietal layers of the pleura, obliterates pleural space
Video-Assisted Thoracoscopic Surgery (VATS)
-used to prevent recurrentce of Ptx
-facilitates elimination of blebs and pleurodesis
-preferred to thoracotomy
Open Thoracotomy
• Generally done if VATS unavailable, unsuccessful
• Surgical removal of blebs
• Oversewing of blebs
• Pleurodesis
• Most invasive
• Very effective in preventing recurrences
• Look at added morbidity compared to VATS
Small Wounds
-act as a one way valve
-air enters during inspiration and cant leave during expiration
-may rapidly lead to tension pneumothorax
Large Open Wounds
->2/3rd the area of the trachea
-air enters pleural cavity through chest wall, not the tracheobronchial tree
-sucking chest wound
-causes significant ventilation impairment
Cover wound immediately with an occlusive dressing taped on 3 sides and then place chest tube
What do you need to do if you have an open pneumothorax due to a large open wound
Tension Pneumothorax
-air trapping that increases intraspleural pressure and compression of contralateral lung
Tension Pneumothorax
-Respiratory distress
-Diminished breath sounds
-Hyperresonance to percussion
-Hypotension
-Tachycardia
-Hypoxia
-JVD
-Tracheal deviation
Tension Pneumothorax
-Complete lung collapse on affected side
-Gross distention of thoracic cavity on the affected side
-shift of heart/mediastinum to opposite side
-Collapse of contralateral lung
Tension Pneumothorax

Immediate Needle Decompression followed by chest tube
What is the first thing you are gonna do for a tension pneumothorax?
Needle Decompression
-Temporizing measure
-Insert 14-16 gauge IV catheter over rib at 2nd ICS, midclavicular
line
-Advance catheter & remove needle
-Rush of air is confirmatory
Tube Thoracostomy
-28-36F in Trauma
-16-20F for Spontaneous
-4th-5th ICS (about nipple level)
-Mid to anterior axillary line
Deep Sulcus Sign
• A deep lateral costophrenic angle in a supine patient is suggestive of a pneumothorax on that side
• May be the only indication of a ptx in a supine patient**
Deep Sulcus Sign
