Discuss the clinical features, possible causes, and management of perioperative upper airway obstruction including laryngospasm
1/11
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
12 Terms
Perioperative upper airway obstruction may be due to:
Pre-op
OSA (e.g. due to hypertrophic tonsils)
epiglottitis
pharyngeal abscess
trauma
anaphylaxis
croup (tracheobronchitis)
laryngomalacia
tracheomalacia
Intra-op
due to poor mask ventilation technique
laryngospasm
Post-op
stridor
post-intubation croup
laryngeal oedema
laryngospasm
Clinical features of upper airway obstruction include
Stridor – inspiratory stridor and prolonged inspiration
Voice changes (muffled voice = supraglottic obstruction, hoarse voice or aphonia = glottis obstruction)
Inability to swallow secretions
Respiratory distress – evidenced by rocking chest and abdomen during breathing and use of accessory muscles (tracheal tug, flaring nostrils, intercostal chest retraction, tachypnea and tachycardia)
Hypoxemia & desaturation
Laryngospasm
powerful and prolonged contraction of the glottis and supraglottic laryngeal adductor muscles ->
leading to closure of vocal cords and false cords and infolding of the arytenoids which seals off the larynx at 3 levels ->
results in hypoxemia and can result in post-obstruction pulmonary oedema or even cardiac arrest
Common causes of laryngospasm periop
Secretions or blood in airway during induction or emergence
Painful stimulus in the setting of inadequate depth of anaesthesia
Mx of laryngospasm
100% Oxygen
Remove stimulus
PEEP
Jaw thrust
Prop 1-2 mg/kg (alleviate spasm in 75% of cases)
Sux (IV 1.5 mg/kg or 4 mg/kg via deltoid)
Risk factors for Laryngospasm
Patient factors
Current or recent URTI within last 2 weeks (up to 10x increased risk)
Young age
Passive smoking
Asthma
Nocturnal dry cough
Wheezing during exercise
History of hayfever or eczema
FHx of asthma, eczema or hayfever
Surgical factors
Blood or secretions in upper airway
Shared airway
Sudden surgical stimulation
Emergence (compared to induction)
Anaesthetic factors
Inhalational rather than IV induction
Thiopentone > sevo > propofol
Light anaesthesia particularly during instrumentation of the airway
Invasive airway management (lowest risk with face mask and LMA)
Probably no difference between deep or awake extubation
Causes of critical airway obstruction in children
LUMINAL
FB aspiration
Stenosis
Papillomatosis
Haemangiomas
Cysts
Wall
Tracheobronchitis
Laryngospasm
Tracheomalacia
Laryngeal cleft
Tracheobronchomalacia
Extraluminal
Tumous
Epiglottitis
Abscess
Vocal cord palsy
Laryngomalacia
inspiratory stridor within first 2/52 of life exacerbated by feeding, agitation, supine, airway obstruction caused by collapse of supraglottic structures on inspiration -> Mx = aryepiglottoplasty

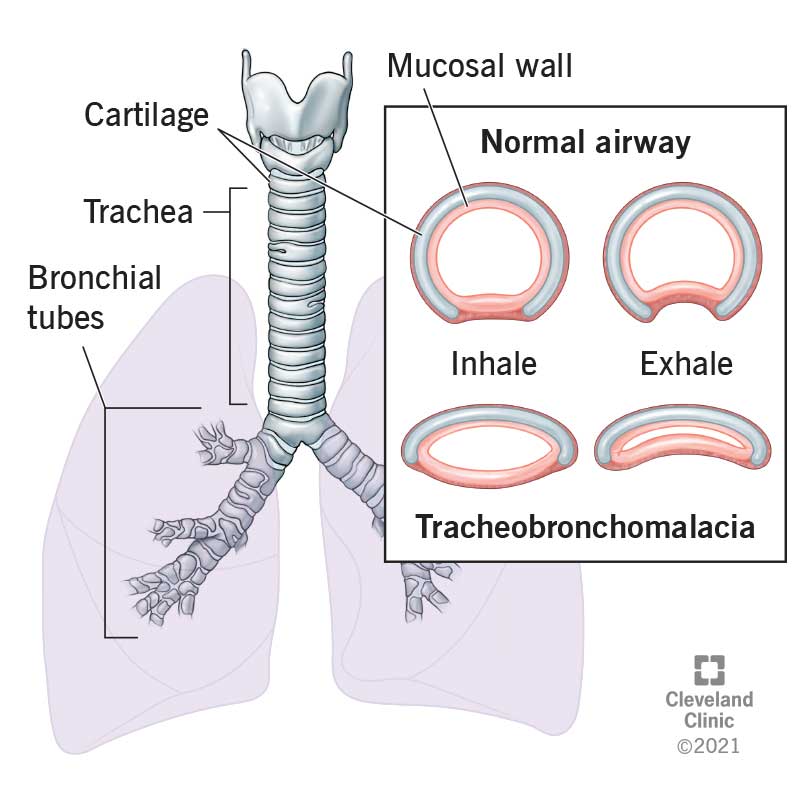
Tracheomalacia and tracheobronchomalacia
airway collapse during expiration due to insufficient rigidity of the cartilaginous framework of the trachea-bronchial tree – usually presents within 12/12 of life, biphasic stridor, expiratory wheeze, recurrent LRTI, cough, cyanotic episodes and apneas
Management of critical airway obstruction will depend upon the pathology but may often require surgical management with ENT using rigid bronchoscopy under GA with inhalational induction and spontaneous breathing (which may be difficult given risk of worsening dynamic airway obstruction with anaesthesia) – or alternatively paediatric tracheostomy (which is difficult and associated with significant morbidity and mortality)
FB ASPIRATION
What
Presentation
Exam
Ix
First aid
Gold standard
What
Life-threatening emergency
Kids 1-3
Due to distractions when swallowing, immature swallowing, no molars
Present
Cough
Wheeze
SOB
Fever
If near glottic inlet
Airway distress
Hoarse voice
Stridor (high mortality 45%)
Exam
Reduced A/e
Wheeze focal or gen
Signs of superimposed pneumonia
Ix
May be normal
May show radiolucency of FB eg. tooth (note organic substances won’t show up)
First aid
5 x back blows then 5 x chest thrusts
No abdo thrusts → liver injury
Gold standard
RIGID Bronch using optical forceps
FB Anaesthetic Plan
Preop
Hx, exam and Ix as above
IV equipment
Remi - 2 mg in 33 ml → 60 mcg/ml
Take 2 ml of this and make up to 20 ml with N saline
120 mcg in 20 ml
6 mcg/ml
When infused at 1 ml/kg/hr ——> 0.1 mcg/kg/min
NEXT
Propofol 20 ml in SD
Glyc 10 mcg/kg
Dexa 0.2 - 0.5 mcg/kg
Airway equipment
Lig 4 mg/kg in 5 ml LL syringe with MAD tip (for surgeons)
Co phenylcaine with standard nozzle
Appropriate range of cuffed and non cuffed ETT
If using circuit for maintaining oxygenation in case put HMA on machine side
8 or 10 Fr O2 tubing connected to aux O2 outlet on machine
INTRAOP
Gas down
IV access L hand or foot
Spray cophenylcaine both nostrils (Lig 5 mg/spray)
Prop at 10 mg/kg/hr (older so 2-3yrs may need more)
Remi and 0.1 mcg/kg/min
Reduce volatile
Second IV if possible and hook up minimum extension line
Dexa and glyc
Turn sevo off. You want SS TIVA prior to surgery start
Measure nostril to angle of mandible - place ETT in L nostril and secure to left cheek THIS IS YOUR NP airway
Surg is happy do laryngoscopy spray cords with half the lig, then MAD tip beyond cords and spray
Check NP JUST visible at top of oropharynx
If pt responding to laryngoscopy and RR > 15-20
Increase remi
If RR OK then deepen with more prop boluses
If RR slow and irreg
Reduce remi
If RR irreg and responding
Add sevo into circuit
Connect disposable T piece to NP ETT run 100% O2 to max of 0.5 L/kg/min
HAND over to surgeons
Sit on L side of pt and hand on abdo
Usually first look is with telescope and layrngoscope
oxygenate using NP ETT
Suspension laryngoscope
O2 catheter to aux O2 outlet → placed inside the cone of the SL
If ventilating bronch is used
T piece on side port of bronch once it is in trachea. Remember to occlude end of T piece
When down affected bronchus do not occlude t piece as this may push FB down further
IF NEED TO APPLY CPAP QUICKLY
If instruments in the mouth
Connect t piece to NP ETT - occlude other nostril and mouth
If NO instruments in the mouth
FM back on and use T piece for O2 flow
CPAP ok
BIPAP bad
ONCE FB OUT
Intubate with cuffed ETT
Recruits
Wake up
PEEP on as re expanded lung prone to collapse