Patho Test 4
1/115
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
116 Terms
Cleft Lip
Failure of maxillary processes to fuse with nasal elevations or failure of upper lip fusion (4-8 weeks into fetal development)
Cleft Palate
Failure of hard and soft palates to fuse 7-12 weeks into gestation
Etiology of hyperkeratosis leading to oral cancers (SCC)
Hyperkeratosis: Excess keratin production
Leukoplakia
Whitish plaque
Chronic irritation
Possibly pre- cancerous
Cancer
Squamous cell carcinoma
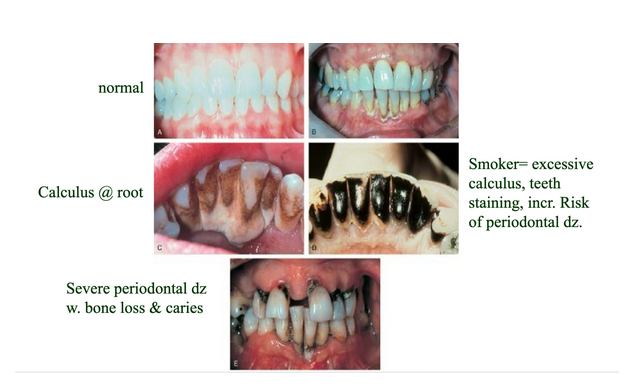
Periodontal disease (gingivitis, periodontitis)
Plaque-bacterial sheet
Caries (cavities)
Gingivitis
Surface
early
Periodontal disease
Roots
advanced
Tartar/calculus
Hardened plaque
Sialadenitis and infectious parotitis (mumps)
Salivary gland disorders
Sialadentitis
Infectious or non-infectious
Infectious parotitis
(Mumps)
Describe dysphagia and achalasia
Difficulty swallowing
Achalasia
Loss of innervation of lower esophageal sphincter
Congenital atresia
Stenosis
Esophageal diverticula
Tumors
Congenital esophageal atresia
A developmental defect where the esophagus isn’t connected.
Esophageal cancer
(squamous cell carcinoma), very malignant and quick to metastasize, S/S: dysphagia due to narrowed lumen, weight loss, obstruction
Hiatal hernias
A portion of the stomach and the gastroesophageal junction move above the diaphragm.
Describe GERD
Periodic flow of gastric contents into the esophagus. Often seen in conjunction with a hiatal hernia.
Discuss the pathophysiology of acute and chronic gastritis (pp. 452-454)
Acute:
Gastric mucosa is inflamed and edematous due to irritants such as allergies, spicy foods, and radiation therapy. S/S: nausea, vomiting, epigastric pain/cramps, sometimes fever, headache, diarrhea
Chronic
Atrophy and irritation of the stomach mucosa, leading to reduced secretions and presenting as dyspepsia (indigestion). A loss of parietal cells leads to achlorhydria (absence of stomach acid). Can be caused by genetic, autoimmune, and bacterial factors; H. pylori is present. Loss of intrinsic factor is due to an autoimmune cause.
Describe the etiology of gastroenteritis
Inflammatory process in the stomach and intestines, usually caused by an infection, but it is also possibly caused by an allergy. Handwashing helps prevent this, and it’s often caused by food- or waterborne illnesses. Gastric mucosal inflammation stimulates vomiting and diarrhea.
Peptic ulcer disease (PUD), gastrointestinal ulcers, and their complications
A form of inflammation with erosion of the gastric mucosa, with H. pylori usually causing it. Crater with an area of surrounding necrosis, affected by gastric acid. Issues come from bleeding (melena, hematemesis, penetration), cicatrization (pyloric stenosis), and duodenal ulcer perforation (food empties into the abdominal cavity, peritonitis). Pain is relieved by reducing stomach acid.
Dumping syndrome
Lack of pyloric sphincter, food moves directly into the small intestine, and abnormal chyme (Hyperosmolar-draws water and results in diarrhea, cramps, and hypoglycemia)
Pyloric Stenosis
The opposite problem from dumping, where the pylorus is narrow. Persistent feeling of fullness, bloating, and vomitus has undigested food.
Describe the pathophysiology of gastric cancer
On the decline in the U.S., but it is associated with countries with high seafood diets and smoked and salted foods. H. pylori infection increases risk and metastasizes to lymph nodes, liver, abdominal organs, and lungs. Adenocarcinoma that affects secretory epithelium. S/S: dyspepsia, pain, weight loss, mass in the stomach.
Describe the congenital disorder biliary atresia
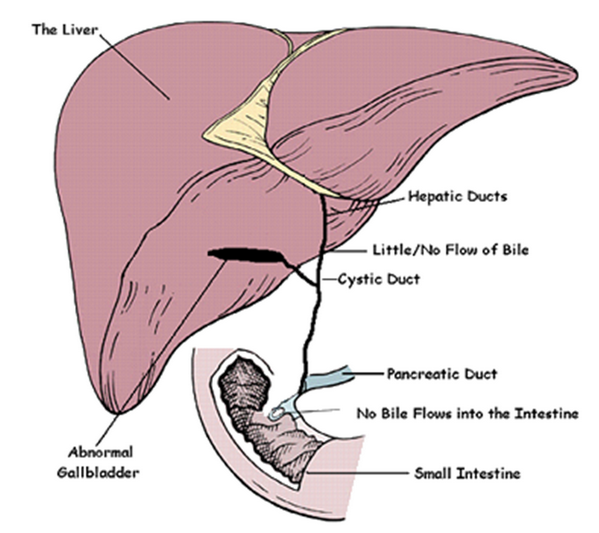
Describe the pathophysiology of biliary obstruction and cholecystitis
Biliary obstruction – Choledocholithiasis pertains to obstruction caused by gallstones of the biliary tract
Cholecystitis refers to inflammation of the gallbladder and cystic duct.
Know difference between cholelithiasis, choledocholithiasis, cholestasis, cholecystitis, cholangitis
Choledocholithiasis refers to inflammation of the gallbladder and cystic duct.
Cholelithiasis refers to the formation of gallstones, which are masses of solid material or calculi that form in the bile
Cholestasis increases from cholelithiasis, bile accumulation in the liver, and the bloodstream
Cholecystitis refers to inflammation of the gallbladder and cystic duct, without the presence of stones. Chronic symptoms include belching, bloating after fatty foods, and mild epigastric or RUQ pain.
Cholangitis is inflammation usually related to infection of the bile ducts.
<break into multiple cards?>
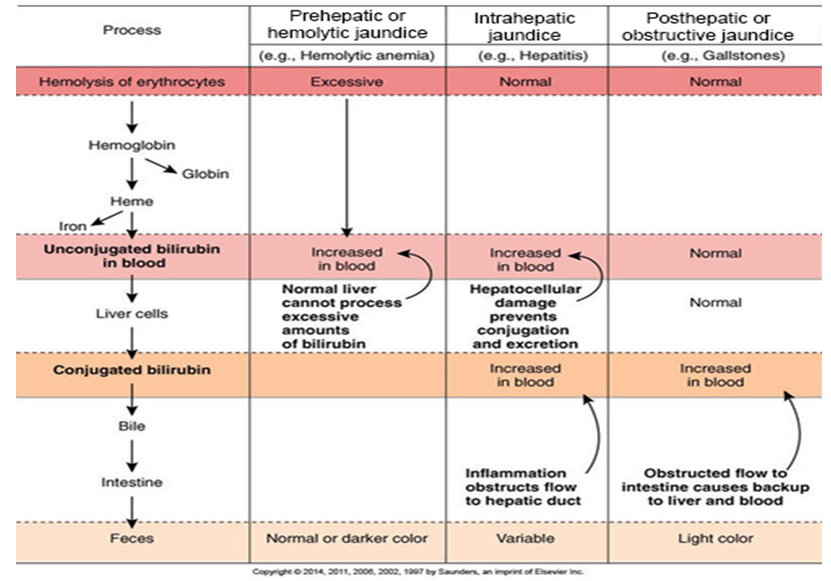
Jaundice
Yellow staining of skin and eyes due to excessive bilirubin in circulation.
Pre-hepatic
excessive RBC breakdown
Hepatic
hepatocyte damage
Post-hepatic
obstructive, bile cannot flow
Know the ins-and-outs of jaundice (icterus)—what causes it (slides 54,55—move pictures out of the way)
Jaundice - Yellow staining of skin and eyes due to excessive bilirubin in circulation.
Pre-hepatic - excessive RBC breakdown
Hepatic - hepatocyte damage
Post-hepatic - obstructive, bile cannot flow
Hepatitis - Differentiate between A, B, C, D & E (particularly transmission route, see table)
<split into multiple?>
Hepatitis A:
Spreads from feces that contaminates food and water
Hepatitis B:
Spreads from blood/blood derived body fluids
Childbirth
Contact with infected bodily fluids
Sexual contact
Hepatitis C:
Spreads from blood/blood derived body fluids
Contact with infected bodily fluids
Sexual contact
Hepatitis D:
Spreads from blood/blood derived body fluids
Contact with infected body fluid (only occurs in people who infected with hepatitis B)
Sexual contact
Hepatitis E:
Spreads from feces that contaminates food and water
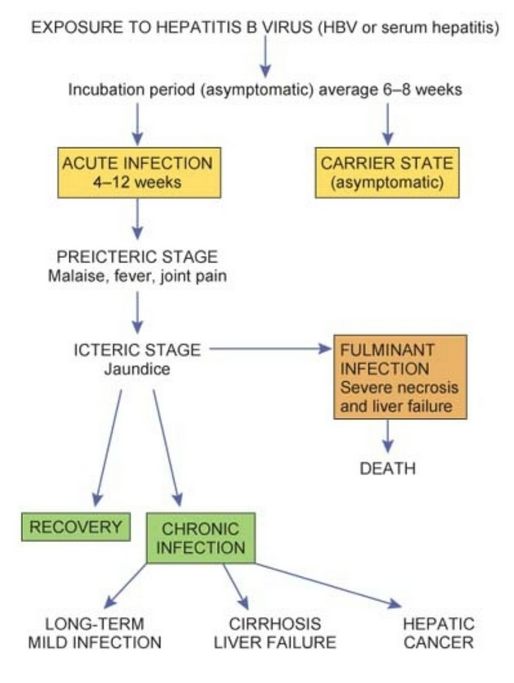
Understand the course of hepatitis B
MASLD - Define metabolic dysfunction-associated steatototic liver disease (slide 62)
Defined by underlying obesity/dyslipidemia or another metabolic condition, often asymptomatic at first
AKA “fatty” liver disease
Inflammation to hepatocytes leading to fibrosis and eventually cirrhosis, related to MASH and as non-alcoholic steatohepatitis (NASH)
Alcoholic liver disease
Initial stage—fatty liver
Enlargement of the liver
Asymptomatic and reversible with reduced alcohol intake
Second stage—alcoholic hepatitis
Inflammation and cell necrosis
Fibrous tissue formation–irreversible change
Third stage—end-stage cirrhosis
Fibrotic tissue replaces normal tissue.
Little normal function remains.
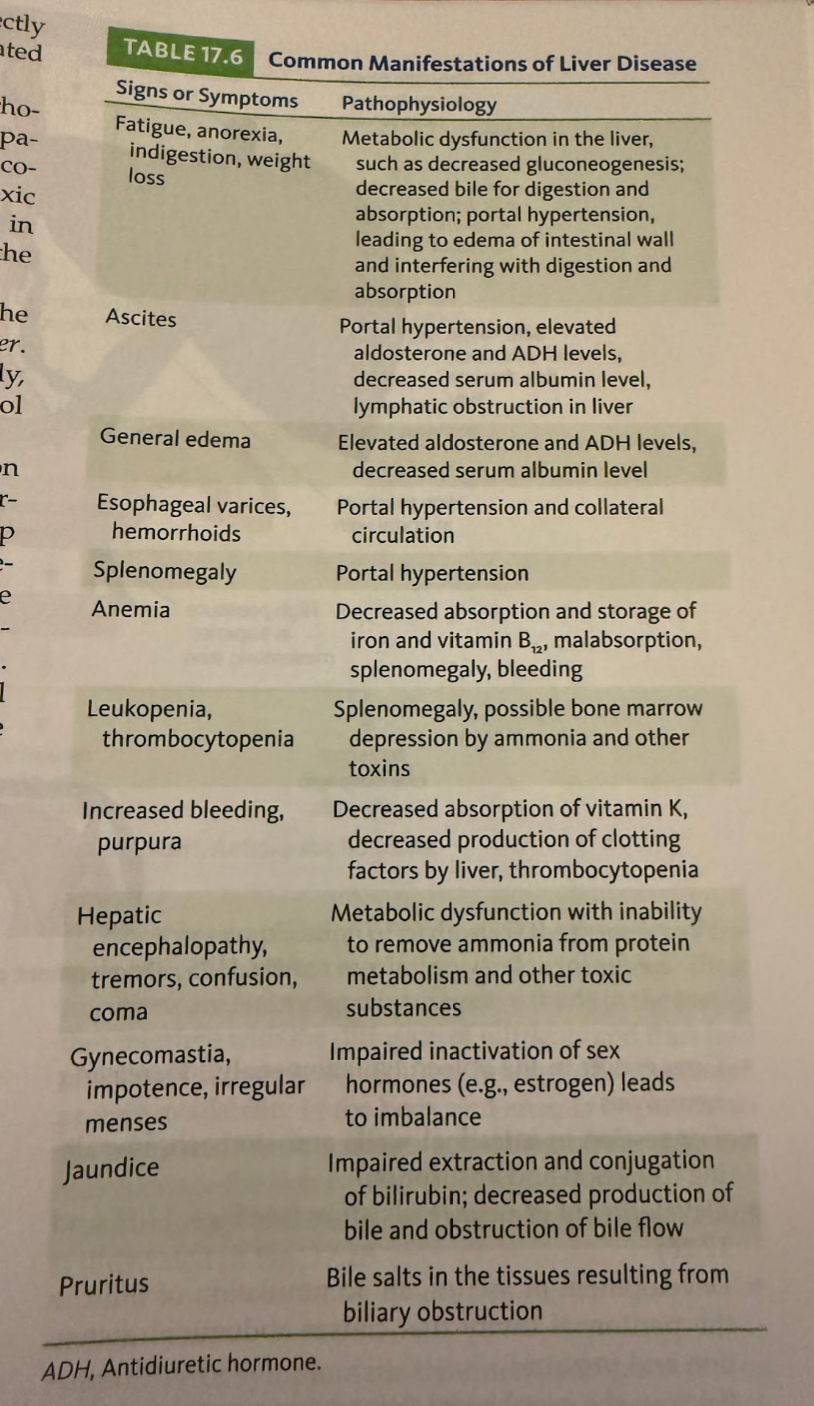
Cirrhosis & Liver Failure Manifestations
Fatty Liver
Slightly enlarged
Pale yellow
Excessive build-up of fat
Excessive fat impacts normal cell function
Obesity & alcoholism
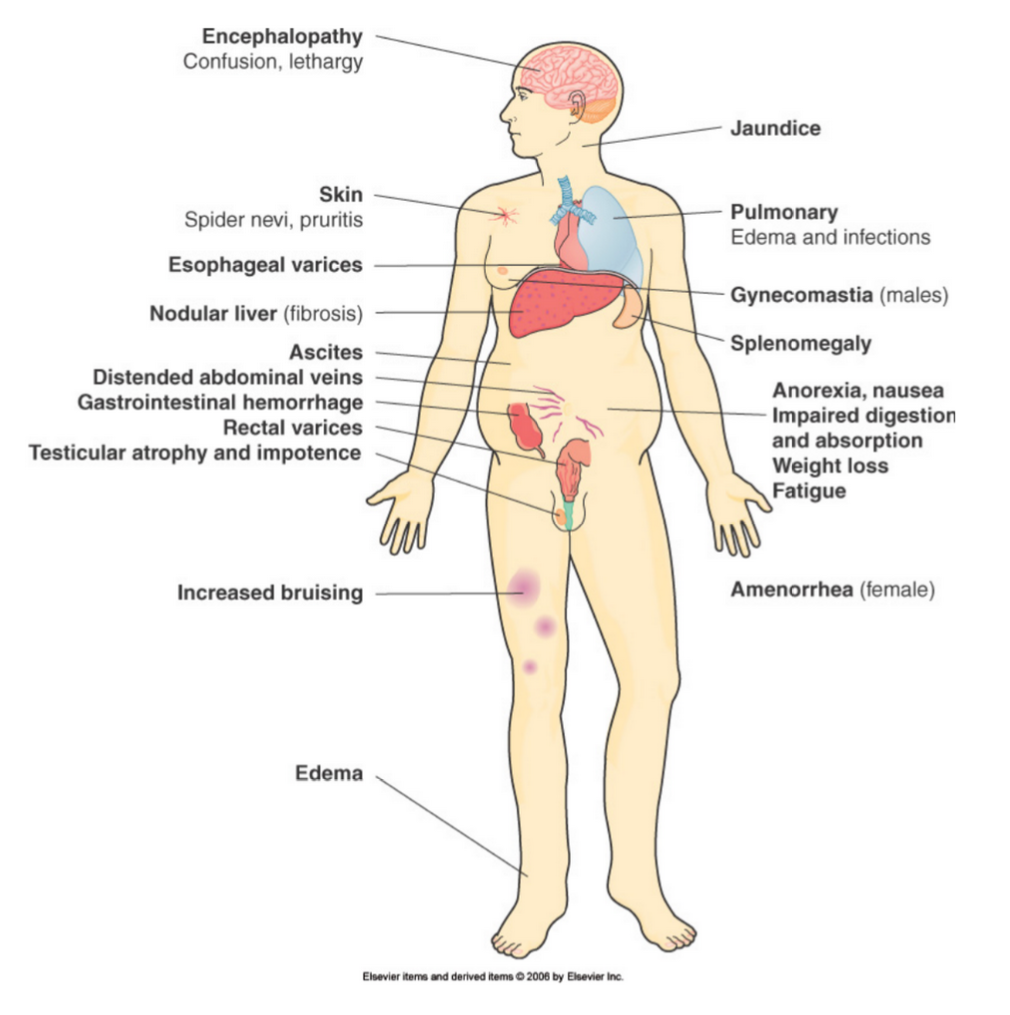
Portal hypertension
Related to liver failure
Increased pressure in portal system
Obstruction in liver causes back-up
Blood into other organs (swelling)
Varices
Causes:
Cirrhosis
Fibrosis
Esophageal varices
Due to portal hypertension
Blood backs up into vessels around esophagus
Potential for rupture & bleeding
Liver Failure
Due to variety of diseases including cirrhosis
Loss of function
Less albumin production (hypoalbuminemia)
Ascites
Fibrinogen & prothrombin decrease
Blood clotting
Detoxification fails
Hepatic encephalopathy - due to ammonia build-up
Primary vs Secondary Hepatic Cancer
Primary - starts in the liver
hepatocellular carcinoma most common
Secondary (metastatic) - starts elsewhere
Often arises from areas served by the hepatic portal veins or that spread along the peritoneal membranes
Pancreatic cancer
Adenocarcinoma
Very deadly (mortality about 95%)
Associated with
Smoking
Diabetes
Obesity
S/S: location dependent
Often: pressure on the duodenum and common bile duct cause early signs of obstructive jaundice
Males (60%)
blacks>whites
Pancreatic head in 66%
Infiltrates locally, obstructs ducts & encases vessels
Mets to liver, local nodes
Pancreatitis
Lots of swelling and inflammation around the pancreas
Digestive enzymes in pancreas begin to ‘eat self’ (autodigestion)
Normally pancreatic enzymes become active in the intestines
Causes enzymatic necrosis
Acute pancreatitis
S/S
Pain [moderate to severe] in the abdomen that is felt through the back (acute abdomen)
Rigidity [guarding]
nausea/vomiting
BP decreases
HR increases
Cold extremities
Possible LOC
Digestive effects
Maldigestion
Malabsorption
Most severe - acute hemorrhagic pancreatitis
Autodigestion (or autolysis)
Tissue destruction by an organ’s own secretions
Enzymatic necrosis
Tissue death brought on by enzymes
Pancreatic insufficiency
Often associated with chronic alcoholisms
Destruction of exocrine/endocrine glands
Gradual loss of normal function
Called pancreatic insufficiency
Permanent malabsorption and diabetes
Fats not absorbed
Steatorrhea
Fat-rich, foul smelling stool
Steatorrhea
Fat-rich, foul smelling stool
Celiac Disease
Aka sprue
Probably genetic etiology
Enzyme defect
Cant digest gliadin
Break down product of gluten
Toxic effect on villi
Malabsorption results
Signs and symptoms: steatorrhea, muscle wasting, failure to gain weight
Ulcerative Colitis - Chronic inflammatory bowel disease
Large intestine
Idiopathic
Ulceration, mucosal atrophy, polyps, adhesions, only lining of colon
30% lead to cancer
Crohn’s Disease - Chronic inflammatory bowel disease
Crohn’s disease
Small intestine
Idiopathic (genetic or autoimmune)
Entire wall thickening, fibrosis, lumen, stenosis, adhesions
Acute appendicitis
Fecalith (usually) obstructs opening
inflammation/swelling
Necrosis in wall
Bacteria leak into peritoneum
Localized peritonitis
Possible greater omentum abscess
May rupture
General periodontitis
Diverticular Disease - Know the difference between diverticula, diverticulosis, and diverticulitis
Diverticula - Large Intesine
Outpouchings of large intestine
Weakening of wall (straining, low fiber diet)
Fill up with feces and other debris → inflammation
Diverticulosis v diverticulitis
Diverticulosis
Asymptomatic or mildly symptomatic condition of having these pouches
Diverticulitis
Occurs when these pouches become inflamed or infected, causing severe abdominal pain, fever, and requiring medical treatment
Does not produce signs
Diverticulitis:
Abdominal pain
Tenesmus
Bloody stool
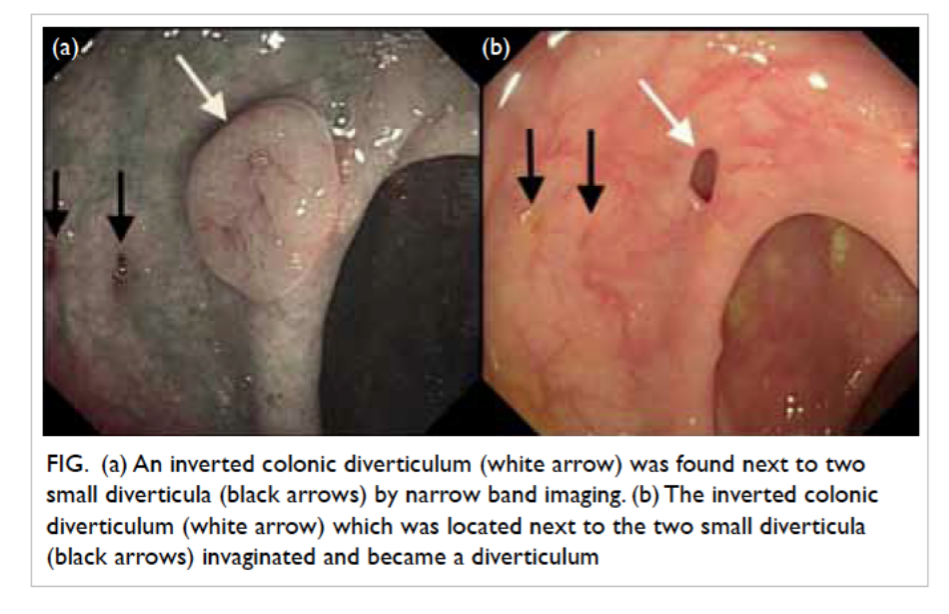
Diverticula and colonic polyps
Innie versus outie
Diverticula = pouch
Colonic polyps = growth
Colorectal cancer
Adenocarcinoma
Described as an apple core lesion
Lumen is narrowed due to constricting lesion
Common and surgically resectable
3rd leading type of cancer, 2nd leading cause of cancer death
Etiology: probably genetics, diet
Benign: polyps (though can predispose to cancer)
Ileus
Blockage of intestine (ileus) due to:
Mechanical
Paralytic (lack of normal peristalsis)
Hirschsprung’s disease
Back up, increased pressure (infarction/pressure necrosis)
Can lead to gangrene
Rupture
Contents spill into peritoneum (peritonitis)
Mechanical Ileus
Inguinal hernia
Volvulus
Twisting of the bowel
Imagine the impact on GI function as well as blood supply
It actually looks like a corkscrew
Infussuception
Telescoping of bowel into itself
Common in children
Can be reduced (fixed) with a barium enema
Tumor
Divertilitis
hernia
Paralytic (lack of nerve stimulation or exterior stifling of peristalsis)
Caused by
Severe pain - internal sphincters respond by spasm and restrict contents
Peritonitis - pus surrounds intestine and prevents peristalsis
Sever enteritis - inflammation neuromuscular transmission
Spinal cord trauma - portions of intestine are denervated
Effects of general anesthesia
Hirschprung’s disease (congenital megacolon)
Lack of PNS innervation
Peritonitis
Inflammation of peritoneal cavity
Infectious
Bacteria - often from GI tract
Chemical irritation
AKA sterile peritonitis
Bile in peritoneum
Pancreatic enzymes
Surgical materials
Ascites
Excess fluid in the peritoneal cavity
3 kinds
Transudate
Cirrhosis - from liver
Nephrotic syndrome - from kidneys
CHF - causes back-pressure in liver
Bloody exudate
Usually from metastatic cancer to the peritoneum
Chyle
Milky fat-containing fluid from blocked lymph flow
Ischemic bowel disease and its complications
Infarction
Atherosclerosis
Thrombosis
Shock - systemic hypotension
CHF - systemic hypoperfusion and hypotensive episodes
signs/symptoms
Intestinal angina (rigid abdomen due to pain)
Bloody diarrhea
Weight loss (from malabsorption)
Mild
Edema, some hemorrhaging, but heals with minimal fibrosis
Moderate
Scarring, cicatrization, stenosis or stricture
Severe
Can lead to infarction, necrosis, gangrene, and finally a strong possibility of rupture and death
Hernias
Tissue where it should not be
Inguinal - protrusion of abdominal tissue through a weak spot in the lower abdominal wall
Hiatal - occurs when the upper part of the stomach pushes through a weakened diaphragm into the chest cavity
Umbilical - soft bulge near the belly button caused by intestine or fatty tissue pushing through a weak spot in the abdominal wall
Congenital anal atresia
Congenital defect where a baby is born with a missing, blocked or mispositioned anal opening, preventing normal stool passage
Hemorrhoids
Varicose veins of rectum
Irritable bowel syndrome
Very common (up to 20% of the population in U.S)
Overactive large bowel
Peristaltic disturbance
Cramping, diarrhea, gas
Sometimes alternating diarrhea/constipation
Peyronie’s Disease
Condition resulting from development of fibrous scar tissue on the penis causing a significant bend during erection
Considered a form of erectile dysfunction (ED)
Can lead to painful/difficult intercourse
Cause is not fully understood but may be hereditary or through repeated injury to penis as well as possible connective tissue disorders
Cryptorchidism
Maldescent/failure of one or both testicles to descend into scrotum from abdomen in developing fetus
Congenital disorder
Cause not fully understood
Infertility results if both fail to descend
Increased risk for testicular cancer
Hydrocele
Excessive fluid collects in the potential space between the layers of the tunica vaginalis (layer of scrotum), may be a congenital defect
Inguinal Hernia
Opening in processus vaginalis allows for a loop of intestine to pass through the abnormal opening, leads to intestinal obstruction
Spermatocele
Abnormal cyst of fluid/sperm that develops between the testis and epididymis outside the tunica vaginalis
Varicocele
Dilated vein in spermatic cord usually on left side, frequently develops after puberty and results from lack of valves in the veins, varicose veins in spermatic cord
Testicular Torsion
When testis rotates on the spermatic cord, compressing the arteries and veins, ischemia develops, hospitalization needed, cuts off blood supply, leads to sterilization
Prostatitis
Has 4 categories:
1 - acute bacterial
2 - chronic bacterial
3 - nonbacterial
4 - asymptomatic inflammatory
Considered an ascending infection or inflammation with multiple causes
Pressure in lower abdomen
Usually seen in older men with incomplete bladder emptying
Fibrosis/inflammatory enlargement can lead to urethral obstruction
Signs include:
Burning urination
Pain
White blood cells in urine
Pus in urine/around urethra
Fever
Chills
Balanitis
Fungal infection of glans penis that can be sexually transmitted
Caused by candida albicans
Seen mostly in uncircumcised men
Vesicles develop into patches
Severe burning and itching
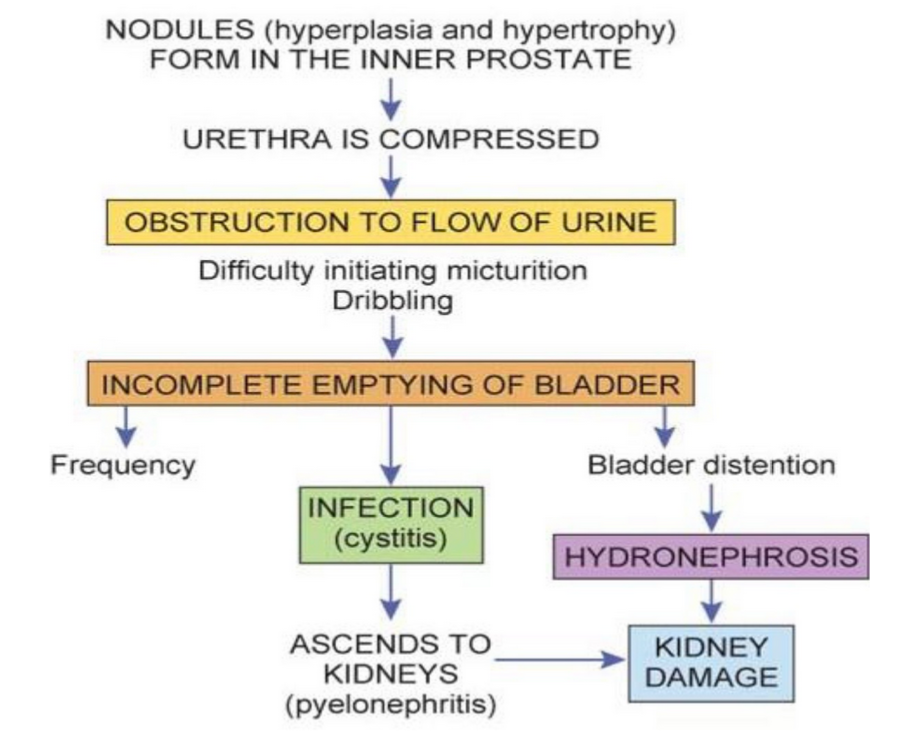
Pathophysiology and complications of benign prostatic hypertrophy (or hyperplasia) (BPH)
Actually hyperplasia not hypertrophy
Not cancer, common in older men (50% of those over 65 years)
Can vary from mild to severe
Hormonal change associated with aging
Prostate goes from smooth to bumpy, irregular, and enlarged
Some fibrosis
Losing testosterone
With frequent but difficult and possibly painful urination
Pathophysiology of prostate cancer and its complications
Common in men 50+ years of age
High cause of cancer related deaths
5-10% of prostatic cancers are caused by inherited mutations in the HPC1 gene
Most tumors are adenocarcinomas arising from the tissue near the surface of the gland
Invasive to regional tissues and metastatic to bone
Tumors vary in degree of cellular differentiation
Silent grower
Spreads quickly in prostate but slow to metastasize
Confined to posterior part of prostate
Signs come late
Treated with surgery and radiation
Seminomas
Malignancy of seminiferous tubules
Most common form
Does not metastasize
90% 5 year survival rate
Teratomas
Worse in men
Malignancy of germ cell
Metastasizes through blood and lymph to lungs, liver, and brain
Survival rate for 5 years is less than 50% if metastasis is present
Pathophysiology and prognoses for male breast cancer
Extremely rare (about 1% of breast cancer cases)
Similar to female breast cancer, usually detected very late because of no routine screening
Uterine Prolapse
AKA displacement
Descent of the cervix/uterus into the vagina, has 3 degrees:
1st degree - cervix drops into vagina
2nd degree - cervix lies at opening to the vagina and the body of the uterus is in the vagina
3rd degree - aka procidentia, if the uterus and cervix protrude through vaginal orifice
Cystocele
Protrusion of urinary bladder into the anterior wall of vagina
Rectocele
Protrusion of rectum into posterior wall of vagina
Amenorrhea
Lack of period
Primary: Never had a period, no menstruation at puberty, may result from genetic or congenital disorder, ovarian problem, hormonal development off
Secondary: Cessation of a period from someone who’s had them, confirmed after 12 months no period, hormone imbalance, pituitary disease, ovarian disease, endometrial disease, may be psychosomatic
Menorrhagia
Excessive bleeding (amount and duration)
Dysmenorrhea
Painful menstruation
Primary: No organic foundation, develops when ovulation commences
Secondary: Results from pelvic disorders
Premenstrual Syndrome (PMS)
Condition that begins a week before menstruation and ends with end of menstruation, cause is unknown but likely hormonal, if severe symptoms (3-8% of women), then it is premenstrual dysphoric syndrome
Endometriosis
The presence of endometrial tissue on the outside of the uterus on structures such as the ovaries, colon, and ligaments, ectopic tissue responds to hormones, dysmenorrhea is a common sign, adhesions/fibrous formation/blood filled cysts may result in infertility
Vaginitis
Inflammation of vagina, usually the result of infection or imbalance of normal bacteria flora
Cervicitis
Inflammation of cervix, usually caused by STDs but can also be imbalance of normal bacteria flora
Pelvic Inflammatory Disease
Infection of reproductive tract, particularly fallopian tubes and ovaries
Follows ascending path through vaginal entry
Can be caused by STDs/bad abortion or delivery practices
Originates as vaginitis or cervicitis and is often polymicrobial
Can cause lower abdominal pain/fever/vaginal discharge
Can lead to abdominal abscess and peritonitis, septic shock, death, adhesions/fallopian scarring causing infertility, ectopic pregnancy due to obstructed fallopian tube from scarring
Leiomyoma
Benign estrogen dependent tumor of myometrium (uterine muscle)
Unknown cause
Common in women during reproductive years (more than 30% of women)
Usually small but can enlarge, shrink after menopause (become fibroid mass)
Can cause pressure damage
Ovarian Cysts
Fluid filled enlarged corpus luteum or unruptured follicle
May become large enough to cause irritation
Bleeding may cause surgical intervention
Insufficient FSH and LH leads to polycystic ovary syndrome (AKA Stein-Leventhal Syndrome)
Teratoma
AKA terrible growth and dermoid cyst
Germ cell (ovum) contains DNA for all body tissues
Needs DNA from sperm to make complete set to form a human being
Develop on ovaries during reproductive years
Fibrocystic Breast Disease
AKA benign breast disease/fibrocytic change
Inappropriate response to estrogen/progesterone
Multiple cysts develop and accumulate fluid
Presence of nodules or masses in the breast tissue that change during the menstrual cycle in response to fluctuating hormone levels
Scar tissue surrounds cysts, has 3 categories based on risk
Fibroadenoma
First category of fibrocystic breast disease
Not considered precancerous
They are specific benign tumors that appear as single, moveable masses that are excised
Pathophysiology and complications of malignant breast carcinoma
Common malignancy and cause of death in women
20-40% of masses that become cancerous are not palpable
Mammography could prevent 30% of breast cancer deaths
Malignant tumors develop in upper outer quadrant of breast in about half of all cases, with the central breast being the next most common location, most tumors are unilateral, most carcinomas arise from cells of ductal epithelium, malignant cells spread at early stage to lymph nodes and blood then metastasize to bone, liver, lungs, and brain, most cases are in women 50 years of age and older, usual initial sign is small moveable nodule but becomes fixated after invading surrounding tissue, treatment is done with surgery/chemo/rad therapy, can be spread through genes (BRCA 1 and 2), hormonal influence, chemical, oncogenic viruses, radiation, history of other estrogen linked cancers
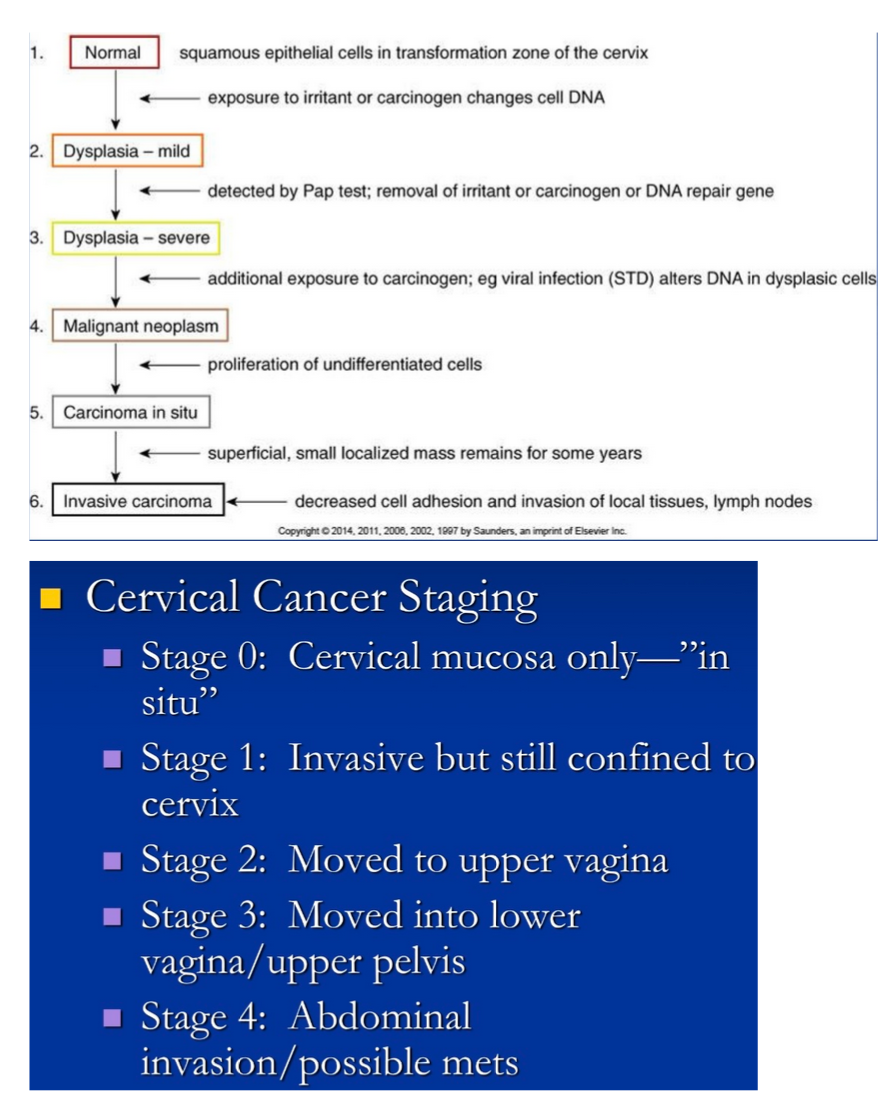
Cervical Carcinoma
Death rate has decreased by 74% with pap smear screenings, average onset for it in situ is 35 years of age, graded from 1-3, staged from 0-4, early changes consist of dysplasia which progresses from mild to severe, strongly linked to oncogenic STDs (HSV2 and HPV), is asymptomatic in early stage
Endometrial Carcinoma
AKA uterine cancer, most common reproductive tract cancer (not including breast), derived from connective tissue/muscle and termed leiomyosarcomas, poor prognosis, increased estrogen exposure leads to a higher incidence, graded from 1-3, majority are adenocarcinomas arising from glandular epithelium, relatively slow growing, unusual painless bleeding is an early warning sign, most commonly affects post menopausal women
Presentations of ovarian carcinoma
Known as a silent killer, only about 25% of cases diagnosed early, 2/3 diagnosed after 55 years of age, prognosis based off tumor type and time of diagnosis, genetic factors have a role in its development
Cystadenocarcinoma: May be benign or low or high malignancy
Endometroid carcinoma: Highly malignant
Chlamydia
One of the most common STDs, leading cause of PID, caused by chlamydia trachomatis, a gram negative obligate intracellular parasite that requires a host cell to reproduce
Men: Evident within several weeks as urethritis with whitish discharge from penis, epididymitis, proctitis
Women: Often asymptomatic until PID develops, sometimes urethritis or other reproductive tract infection
Gonorrhea
Caused by n. gonorrhoeae, a gram negative aerobic diplococcus (gonococcus)
Men: Most common site of inflammation is in the urethra, resulting in dysuria with purulent discharge and sometimes epididymitis, sometimes asymptomatic
Women: Often asymptomatic, may have infection in anus/rectum, involves the endocervical canal, PID, bacteremia and gonococcal arthritis, green/yellow/creamy white discharge
Bacterial STI syphilis
Caused by treponema pallidum, an anaerobic spirochete, systemic infection with 4 stages and the organism can be isolated from lesions in the first 2
Stage 1: Primary stage, identified by presence of chancre on genitalia (or cervix) about 3 weeks after exposure, lesion heals spontaneously without treatment within a few weeks and are asymptomatic
Stage 2: Secondary stage, the organisms have entered the general circulation by the time the chancre has healed, and if untreated, a widespread symmetrical rash appears on skin along with fever, malaise, sore throat, stomatitis, anorexia
Stage 3: Latent stage, may persist for years, skin lesions may recur, person is usually asymptomatic
Stage 4: Tertiary stage, gumma formation (area of necrosis and fibrosis leading to bone destruction and pathologic fractures), these affect the cardiovascular system by damaging the arterial wall and developing aortic aneurysms, also cirrhosis like liver damage, dementia, and blindness
Genital Herpes (HSV2)
Usually caused by HSV2, sometimes HSV1, blister like lesions appear (vesicles) on genital areas/buttocks/thighs, ruptures after several days and a crust eventually forms over it, and heals in about 3-4 weeks, systemic signs may present in acute stage (fever, headache, lymphadenopathy), then travels up dermatome to the spinal ganglia where it resides until it's triggered again (stress, respiratory infections), the migrated back to the mucosa or skin to replicate, may be transferred to infant during vaginal delivery and cause nervous system damage and even death, places women at high risk for cervical cancer
Human Papilloma Virus (HPV)
Certain types cause genital warts, increasing in frequency, incubation period is up to 6 months, may be asymptomatic, circular, double stranded DNA virus, several types also cause cervical cancer, appearance varies, usually appear on penis in men, found in vagina/on cervix in women, pregnancy promotes growth/spread
STDs
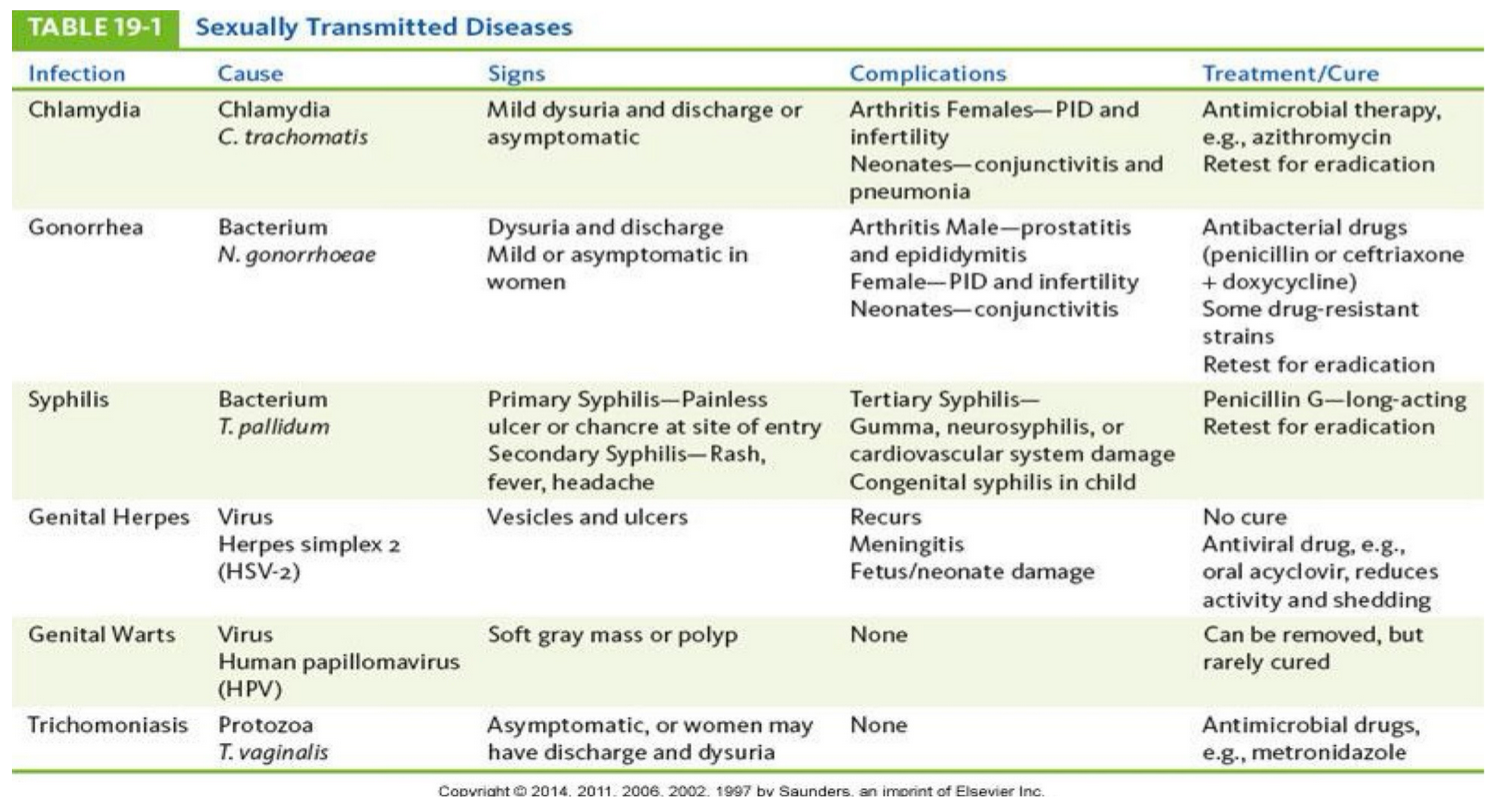
Trichomoniasis
Caused by trichomonas vaginalis, localized infection, an anaerobic flagellated protozoan, extracellular parasite
Women:
Vaginal, urethral, and Bartholin’s glands infected, produces inflammation, pruritus, foul smelling yellow discharge, may be subclinical then flare up when microbial balance of vagina shifts
Men:
Urethral infection, usually asymptomatic, can lead to other infections
Development and consequences of an ectopic pregnancy
AKA tubal pregnancy, occurs when fertilized ovum is implanted outside the uterus, often in fallopian tube, incidences increased within the past 20 years likely due to pelvic inflammatory disease (PID), may cause spontaneous abortion in early pregnancy, or fetus may continue to develop leading to severe hemorrhage or periodontitis, causes severe abdominal/pelvic pain, considered a medical emergency and requires hospitalization
Gestation
Length of time since the first day of the last menstrual period (LMP) and equals 280 days/40 weeks/10 lunar months
Parity (pregnancy)
Number of pregnancies in which the fetus has reached viability