Lecture 09: Neuro Differential Diagnosis
1/102
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
103 Terms
Parkinson's disease (PD)
- Depletion of dopamine from substantial nigra
- Results in structural changes
Cardinal clinical signs of PD
- Tremor
- Rigidity
- Akinesia
- Posture and balance
Resting tremor
- Shaking, usually starting on one side
- Resembles the motion of rolling a pill between the thumb and forefinger
Rigidity
- Stiffness of the limbs, neck, or trunk
- Cogwheel and lead pipe
Akinesia/bradykinesia
- Loss or impairment in power of voluntary movement
- Hesitation, slow movement
- Difficulty rising from a sitting position is a common sign of disordered control over movement
Cogwheel rigidity
- Ratchet-like response to quick passive movement
- Catches releases catches
Leadpipe rigidity
- Constant resistance as limb is moved
Postural instability
Leaning forward or backward when upright reflects impairment of balance and coordination
Which stages of Hoehn and Yahr are usually seeing in outpatient PT?
3-4
Hoehn and Yahr stage 1
- Mild symptoms
- Able to go about day-to-day life
Hoehn and Yahr stage 2
- Symptoms such as tremors and stiffness begin to worsen
- May develop poor posture or have trouble walking
Hoehn and Yahr stage 3
- Movement begins to slow down
- Loss of balance
Hoehn and Yahr stage 4
- Symptoms are severe and cause issues with day to day living
- Unable to live alone and will need care
Hoehn and Yahr stage 5
- Walking or standing may be impossible at this point
- People at this stage are often confined to a WC or bed
PD gait related impairments
- Festinating gait
- Freezing of Gait
- Difficulty turning
- Reduced stride length
- Reduced speed of walking
- Increased time in DL support
- Insufficient hip, knee, ankle flexion
- Insufficient heel strike with increased forefoot loading
- Reduced trunk rotation
- Difficulty with dual tasking
- Difficulty with attentional demands of complex environments
Medical management of PD
- Levodopa/carbidopa (Sinemet)
- Metabolized before reaching the brain, which requires high doses and therefore side effects
- L-dopa is commonly administered with carbidopa, which allows a higher % of L-dopa to enter the brain
L-dopa
- Gold standard drug for PD
"On" phase of L-dopa
30 minutes after taking it
Adverse effects of L-dop
- Dyskinesias
- Dystonia
Dyskinesias
- Dynamic involuntary choreoathetotic movement occurring at peak of dose
- Initially = face grimacing with twitching of the lips, tongue protrusion
- Severe = involves limbs, trunk, and neck
Dystonia
- Prolonged involuntary contraction that causes twisting or torsion of body segments
- Clawing of the toes or fingers, or cramping of the calf, neck, face or paraspinal muscles (i.e. dragging the leg)
- Associated with pain during "off" periods
- Will see this without medication
Parkinsonism
- Parkinson's disease-like extrapyramidal symptoms that are adverse effects associated with particular drugs or brain injuries
- No actual change in the basal ganglia
Huntington's disease (HD)
- Neurodegenerative (hereditary) disease
- An autosomal-dominant illness caused by an expansion of the CAG repeats on the short arm of chromosome 4, is clinically characterized by a combination of movement disorders, cognitive decline and behavioral changes.
Huntington's disease results in degeneration of:
- Basal ganglia
- Cerebral cortex
What differentiates Huntington's disease from PD?
Depressed, behavioral changes
HD symptoms
- Affects muscle coordination and leads to cognitive decline, psychiatric problem
- Involuntary jerking or writhing movement
- Muscle problems, such as rigidity or muscle contracture (dystonia)
- Slow or abnormal eye movements
- Impaired gait, posture and balance
- Difficulty with physical production of speech or swallowing
HD age on onset
35-55 years
A physical therapist is working with a 67-year-old male retired police officer. The patient displays rigidity, slowed movements, involuntary oscillatory movements, and instability that has led to a recentuptick in falls. Based on the patient's presentationwhich of the following neurological disorders could the patient MOST likely have?
A. Parkinson's Disease
B. Guillain-Barré syndrome
C. Multiple Sclerosis
D. Amyotrophic lateral sclerosis
A. Parkinson’s Disease
GBS- symptoms have to be bilateral/symmetrical; MS- UMN, rigidity has nothing to do with UMN (it would be spasticity); ALS- something related to both UMN and LMN disease
Cerebellar disorder presentation
Inability to control the distance, speed, ROM needed for coordinated movements
Signs of cerebellar disorder
"Vanished:"
- Vertigo
- Ataxia
- Nystagmus
- Intentional tremor
- Slurred speech
- Hypotonia
- Exaggerated broad based gait
- Dysdiadokinesia
Causes of cerebellar disorder
- Brain trauma
- Brain tumors
- Metabolic disease
- Demyelinating or degenerative disorders
Multiple Sclerosis (MS)
- Autoimmune characterized by inflammation, selective demyelination, and gliosis
- Chronic demyelinating disease of the CNS
- Any area of CNS can be affected: cortical, subcortical, cerebellum, spinal cord
Who does MS affect more men or women?
Women
Age of onset MS
- 20-40
- Peak onset = 30 years
Ethnicity affected more by MS
Caucasian
Etiology of MS
- White blood cells attack neurons
- Affect fatty tissues around the nerve fibers in brain and spinal cord
- Destroyed or damaged myelin leaves multiple scarring called sclerosis
- Nerve signals are slowed or blocked, causing MS symptoms
On of the first symptoms of MS
Optic neuritis
Signs and symptoms of MS
* Impairments vary based on location of lesion
- Visual impairments
- Sensory impairments
- Motor impairments
- Intention tremor
- Fatigue
- Cognitive impairments
- Bowel and bladder dysfunction
- Emotional disturbance
- Psychosocial problems
MS diagnosis
- MRI: usually two separate lesions in the CNS that are distinct
- CSF analysis: elevated immunoglobulins and presence of oligoclonal IgG bands, slight protein elevation
- Evoked potential -decreased nerve conduction velocity
Common types of MS
- Relapsing-remitting
- Secondary-progressive
- Primary-progressive
- Progressive-relapsing
Most common type of MS to see in an outpatient clinic
- Relapsing remitting
- Every time they relapse, their ability to do things will be impacted
Relapsing-remitting (RRMS)
- Short duration (days to months)
- May remain symptom free for months or years
- May or may not leave permanent deficits followed by periods of remission
Secondary progressive (SPMS)
- Slow, steady progression- with or without relapses
- Suddenly begin to have decline without remission
Primary progressive (PPMS)
- Steady worsening from the start
- Do not have relapses/remissions
Most individuals diagnosed with relapsing-remitting will eventually transition to which form of MS?
Secondary-progressive
Progressive-relapsing (PRMS)
- Steadily worsening from onset
- Decline with superimposed attacks
A 32-year-old female patient presents with the presence of abnormal reflexes. She also notes"weird" sensations throughout her body. Her labfindings indicate increased IgG in the cerebrospinal fluid. During the assessment, she asks the PT to decrease the temperature of the treatment room as she was heat intolerant. Considering the patient's presentation so far, which signs and symptoms are LEAST likely expected to be seen in this case?
A. Ataxia
B. Optic neuritis
C. Trigeminal neuritis
D. Rigidity
D. Rigidity
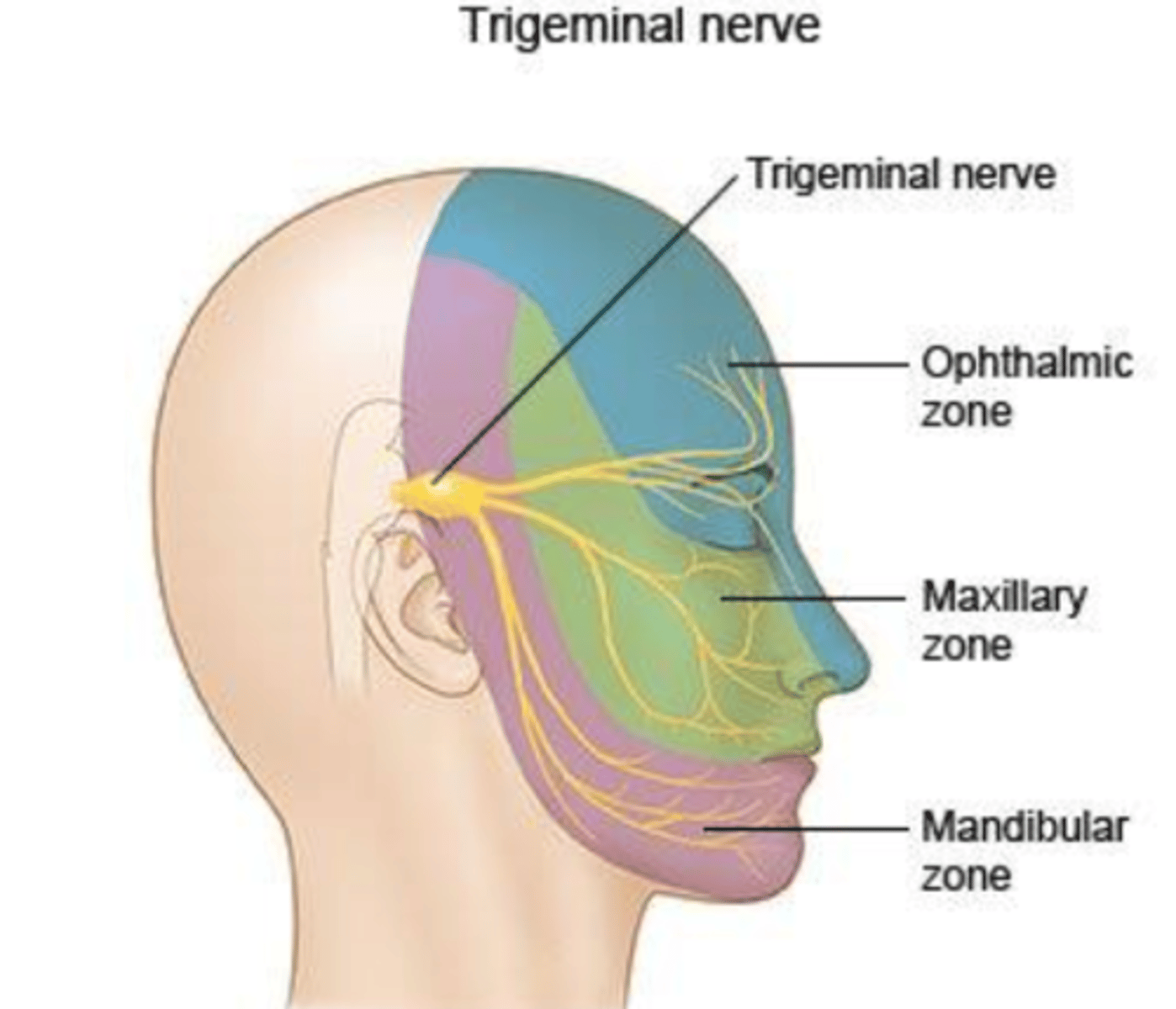
Neuropathic pain: trigeminal neuralgia
- Inflammation of trigeminal nerve
- Expect to find loss of sensation in all 3 zones
- Touch patient with cotton swab from one side to the other
- May describe feeling of sunburn, numbness, etc.
Clinical characteristics of MS
- Acquired demyelinating disease with an immunological cause
- Weakness, paresthesia
- Charcots triad
- Spasticity, hypertonicity, hyperreflexia, positive Babinski sign
- Incoordination, optic neuritis, ataxia, vertigo, dysarthria
- Diplopia, bladder incontinence, tremor, balance deficits, falls, cognitive deficits
Charcots triad
- Intentional tremor
- Scanning speech
- Nystagmus
Precautions when working with MS patients
- Give frequent rest breaks (fatigue and heat sensitivity)
- Drink water
- Central fatigue can last 1-2 days
Clinical characteristics of myasthenia gravis
- Neuromuscular junction disorder
- Caused by autoimmune mediated acetylcholine receptor damage, resulting in a deficit in neuromuscular transmission
- Weakness that worsens during periods of activity and improves after periods of rest
- Variable degrees of weakness, ranging from ptosis or diplopia to critical respiratory weakness
- Muscles that control speech, facial expression, mastication, swallowing, breathing, neck and limb movements may be involved
Early symptoms of myasthenia gravis
- Droopy eyelids (ptosis)
- Blurry or double vision (diplopia)
- Sometimes, these are the only symptoms
MS gait related impairments
- Weakness: foot drop, vaulting
- Spasticity
- Balance problem
- Sensory deficit
- Fatigue
MS visual impairments
- Optic neuritis
- Marcus Gunn
- Nystagmus
- Diplopia
Optic neuritis
- Inflammation of optic nerve
- S&S include CN 2 testing: visual field, visual equity (how much vision you have), pupillary light reflex
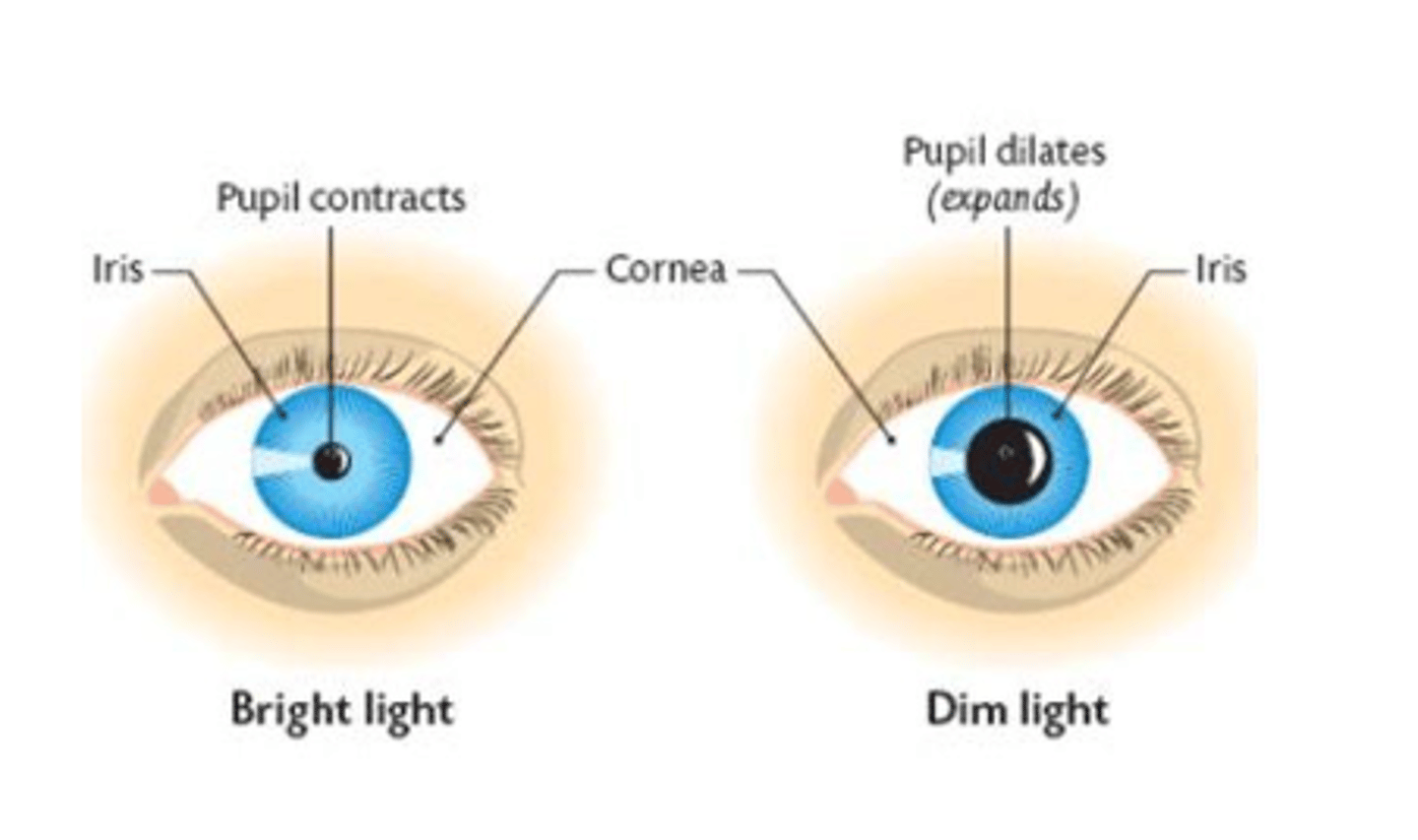
Marcus Gunn
Condition where the pupil dilates instead of constricting when a light is shined into the pupil
Nystagmus
Involuntary rapid eye movements
A 43-year-old female patient presents to a pro bono outpatient clinic for a maintenance program. Her past medical history includes multiple sclerosis (MS). The patient reports that over the past 2 years she has had significant flare ups and her functional mobility has been declining. Which subtype of MS does the patient LIKELY have?
A. Primary-progressive MS
B. Secondary-progressive MS
C. Progressive-relapsing MS
D. Relapsing-remitting MS
C. Progressive-relapsing MS
Steady decline with attacks.
A is not correct because not seeing a steady decline with disease progression; B is not correct because it is not relapsing and declining; D is not correct because it does not state anything about a remission period.
Pupillary light reflex
- For normal pupillary light reflex,
both pupils constrict simultaneously when light is shone into either eye.
- Light shone into one eye causes
ipsilateral direct pupillary light reflex and contralateral consensual pupillary light reflex
Loss of pupillary light reflex: lesion in ipsilateral CN 3
Direct response
Loss of pupillary light reflex: contralateral CN 3
Consensual response
Loss of pupillary light reflex: ipsilateral CN 2
Both direct and consensual responses
Loss of pupillary light reflex: contralateral CN 2
Affect the ipsilateral pupillary responses
MS special signs
- Lhermitte sign
- Uthoff's phenomenon
Lhermitte sign
- Flex neck
- Shock-like sensation goes down spine into hands
Uthoff's phenomenon
- Exposed to high temperatures
- Neurologic symptoms exacerbated
- Have more spasticity, etc.
A patient with normal sensation and reflexes presents to the clinic with decrease in muscle tone and asthenia. Which of the following other signs and symptoms are MOST likely expected to be seen during the patient assessment?
A. Bradykinesia
B. Synergy
C. Uniform resistance to passive range of motion
D. Truncal ataxia
D. Truncal ataxia
In cerebellar disorders, you see asthenia (weakness) and hypotonia = cerebellar disorders;
bradykinesia is associated with PD— would tell you about rigidty or tremors; synergy is in CVA.
Exercise consideration of MS
- Exercise in AM due to decreased core temperature and fatigue
- For every 15 min of exercise, give a 5 min break
- Work at sub-max level (50-70%)
A 45-year-old female presents to PT with a recent diagnosis of MS. Upon initial evaluation, she complains of eye pain, vision loss in one eye and visual field loss. Which of the following cranial nerves listed below is most likely involved?
A. Facial (VII)
B. Optic (II)
C. Abducens (VI)
D. Oculomotor (III)
B. Optic (II)
Involved in visual field and visual equity
A PT is performing cranial nerve testing on a 55-year-old male patient. When observing the patient's right pupillary response to light, the PT observes that there is no constriction of the right pupil but the left pupil does constrict. Which cranial nerve is the MOST likely cause of this impairment?
A. Left Oculomotor nerve (CN III)
B. Right Optic nerve (CN II)
C. Right Oculomotor nerve (CN III)
D. Left Trochlear nerve (CN IV)
C. Right Oculomotor nerve (CN III)
One constricts and one dilates, which indicates CN 3. Direct nerve because that eye is not responding.
Guillain-Barré syndrome (GBS)
- Autoimmune response as the patient's antibodies attack its own peripheral nerves
- Syndrome is typically observed after respiratory infection, GI infection characterized by diarrhea, surgery, vaccination, or childbirth
GBS pathogenesis
- LMN
- Demyelinating disorder of the spinal nerve roots and peripheral nerves
- Rapid onset of weakness (distal to proximal) with bilateral symptoms peaking at approximately 2-3 weeks, but progressing no greater than 4 weeks
- Severity and course of the disease varies widely
Cases of GBS with recovery and time frame
70% have full recovery within 3-6 months
GBS diagnosis
- Clinical examination: symmetrical, bilateral, ascending
- Blood and urine tests
- Lumbar puncture
- MRI, CT scan, nerve biopsy
- Stool test
- Nerve conduction velocity test
- EMG
Lumbar puncture will reveal what in a patient with GBS?
Increased protein levels
GBS sensory symptoms
- Initially bilateral and symmetrical "glove and stocking" distribution
- Pain in large muscles of the body such a snack, thighs, and buttock
- Stiffness, cramping, and "deep aching" pain
- Burning, tingling, pins and needles, and numbness
GBS motor symptoms
- Decreased signal strength of peripheral nerves
- Muscle weakness and atrophy
- DTR diminished
- Partial or full paralysis (functional dependence)
- Respiratory muscle involvement- mechanical ventilation
- Facial and oral-motor weakness- vision, speech, and swallowing problems
When observing a patient ambulating, a PT notices that the patient's gait has the following characteristics : impaired trunk control and ataxic gait. There is also circumduction to assist with foot clearance due to weakness of dorsiflexors of the right foot. This gait pattern is often observed in patients with diagnosis of:
A. Multiple Sclerosis
B. Parkinson's Disease
C. Duchenne Muscular Dystrophy
D. Guillain Barre Syndrome (GBS)
A. Multiple Sclerosis
MS usually affects one side of the body more. Not GBS because have to have bilateral symptoms, symmetrical, and ascending.
Amyotrophic lateral sclerosis (ALS)
- UMN and LMN symptoms
- Bulbar
- Respiratory
- Frontotemproal dementia
- Cognitive impairments
- Behavioral impairments
ALS LMN symptoms
- Muscle weakness
- Hyporeflexia
- Hypotonicity
- Atrophy
- Muscle cramps
- Fascilutations
ALS UMN symptoms
- Spasticity
- Pathological reflexes
- Hyperreflexia
- Muscle weakness
ALS bulbar symptoms
- Bulbar muscle weakness
- Dysphagia
- Dysarthria
- Sialorrhea
- Pseudobulbar affect
Sialorrhea
Excessive salivation
Pseudobulbar affect
Uncontrollable laughing or crying
ALS respiratory symptoms
- Respiratory muscle weakness (inspiratory and expiratory)
- Dyspnea
- Exertion dyspnea
ALS diagnosis
- Lou Gehrig's disease
- Most common and devastatingly fatal motor neuron disease among adults
- Presents with denervated muscle
- Cervical extensor weakness is typical
Difference between MS and ALS
MS is purely an UMN while ALS presents with both UMN and LMN symptoms
A PT is treating a patient with a diagnosis of ALS. The patient has weakness of all extremities and gets fatigued very easily while doing ADLs. His main goal is to maintain mobility and function as much as possible. Which of the following will be LEAST appropriate for this patient?
A. Recommending soft foam collar for neck
B. Taking frequent breaks during activities
C. Recommend KAFO and walker for ambulation
D. Slow, prolonged stretches and ROM exercises for UE and LE
C. Recommend KAFO and walker for ambulation
KAFO and walker is cumbersome and adds more weight to muscles that are already growing weaker.
A 42-year-old female patient presents with chief complaints of asymmetrical weakness of lower and upper extremities. There is presence ofmuscle fasciculations and impaired speech, but her sensations seem relatively intact. Her husband mentions that she randomly starts laughing or crying for "no reason at all". Which of the following signs and symptoms should the therapist LEAST likely expect to be positive in this case?
A. Presence of memory impairments
B. Presence of foot slap while walking
C. Cervical flexor muscle weakness
D. Reduced vital capacity
C. Cervical flexor muscle weakness
Can see memory impairments, foot slap, reduced vital capacity. Would NOT see cervical flexor weakness because they are in flexed position — it is cervical extensor weakness.
ALS signs
UMN and LMN
GBS signs
LMN
MS signs
UMN
ALS age/sex
Mid to late 50s
GBS age/sex
- Any age
- Men and older adult at risk
MS age/sex
- 20-40 years old
- Women > men
ALS characteristic presentation
Fasiculation and loss of dexterity
GBS characteristic presentation
- Symmetric progression of paralysis from LEs to UEs
- Ascending progression
- Bilateral, symmetrical progression
MS characteristic presentation
- Optic neuritis
- Blurred or double vision
- Fatigue
- Weakness
- Trigeminal neuralgia
- Bladder incontinence
- Heat intolerance
- Paresthesia (most common)