037/038 Clinical observations and pain assessment
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
clinical observations AKA obs/vitals
T - temperature
P/HR - pulse or heart rate
R or RR- respirations or respiratory rate
BP - blood pressure
O2 sats/SpO2 – oxygen saturations
other common assessments - clinical observations
neurological and neurovascular observations
breath sounds
bowel sounds
peak flow
blood glucose
height and weight
limb and girth measurements
when are vital signs taken
on admission to establish a reliable baseline
routine times (QID, TDS or BD - then reviewed)
onset of adverse event/unwell
pre and post surgery/procedure - RPAO
pre- and post-certain medications
before discharge
when you’re worried or not sure
if in doubt, do a set of obs
observations - in general
Before:
explain to client
position and privacy
equipment - dedicated to this client
wash hands - gloves needed
has client just exercised? had a hot shower? had a hot or cold meal/drink? pain levels, psychological state
After:
document and compare to client’s previous readings
wash hands
equipment - cleaning & storage
what controls body temp
Hypothalamus receives info about temp of the blood and also from thermo-receptors in the skin and some internal organs
Body temp is the balance between the heat produced and the heat lost from the body.
Heat is produced by cellular metabolic activity and muscle contraction and lost by radiation and evaporation
The body keeps temperature within a narrow, safe range despite large variations in temperatures outside the body.
normal adult temp: 35.8-37.2°C
regulatory mechanisms when the body is too hot
vasodilation - blood vessels in the skin dilate to carry excess heat to the skin's surface
sweating - as the sweat evaporates, it helps cool the body
We assist the process by being less active, wearing less and taking cool drinks
regulatory mechanisms when the body is too cold
vasoconstriction - blood vessels constrict and blood flow to the skin is reduced, which conserves body heat
shivering - involuntary, rapid contraction of muscles to generate more heat.
We assist ourselves by wearing more clothes, hot food, heating and exercise.
what increases temp
Dehydration
Infection – hypothalamus resets internal thermostat; we feel cold and shiver even if our temperature is over 38°C. Fevers have a cold, hot and sweat stage.
Medications – metabolic reaction.
Severe trauma or injury – follows head injury, CVA, or inflammation.
Medical conditions – tumours, arthritis, gastritis, hepatitis.
common terms for increased temp
Pyrexia: Temperature above normal range
Hyperpyrexia: Excessive and unusual elevation of body temperature greater than or equal to 41.1° C
Febrile: Fever
Afebrile: Normal body temperature
Hyperthermia: Body produces more heat than it can dissipate to cool down (40°C or above). AKA heatstroke/sunstroke
what decreases temp
Environmental temperature/exposure
Alcohol or drug use
Metabolic disorders such as diabetes or hypothyroidism.
Shock
Hypothermia: core temperature of less than 35°C
Aged clients have less subcutaneous fat; more sensitive to cold environments
assessing body temp
2 most common:
scanning thermometers
ear/tympanic thermometers
older methods - not used routinely:
auxiliary
oral
groin
rectal
skin/chemical (liquid crystal - forehead)
DON’T use: glass thermometers - have mercury inside
forehead scanning thermometer
check manufacturing instructions – some models keep still whilst recording, others have a set movement

assessing tympanic thermometer
Tympanic membrane has abundant arterial supply from carotid artery
Always attach new disposable cover to probe
Infants younger than 12M: Pull the earlobe down and back
Children older than 12M & adults: Pull the earlobe up and back.
Centre the probe tip in the ear and push gently inward toward the eardrum. Take care not to insert too far.
oral route
Wait 30 mins hot or cold fluids or after smoking
Clean the thermometer with alcohol wipe
Place under the tongue, to one side, and close the lips tightly around it
Leave in place the required amount of time.
DON’T use for young children or clients who are unconscious, uncooperative or have a history of fitting.
Must be able to breathe through the nose
rectal route
Very accurate
May be used for small infants and when an accurate measurement is essential
Not used for clients who have rectal surgery, diarrhoea, diseases of the rectum, or haemorrhoids
axilla route
Used to be the preferred site in newborns, infants, children
For those with oral inflammation, cannot breathe through nose, irrational clients
Least accurate way to measure body temperature.
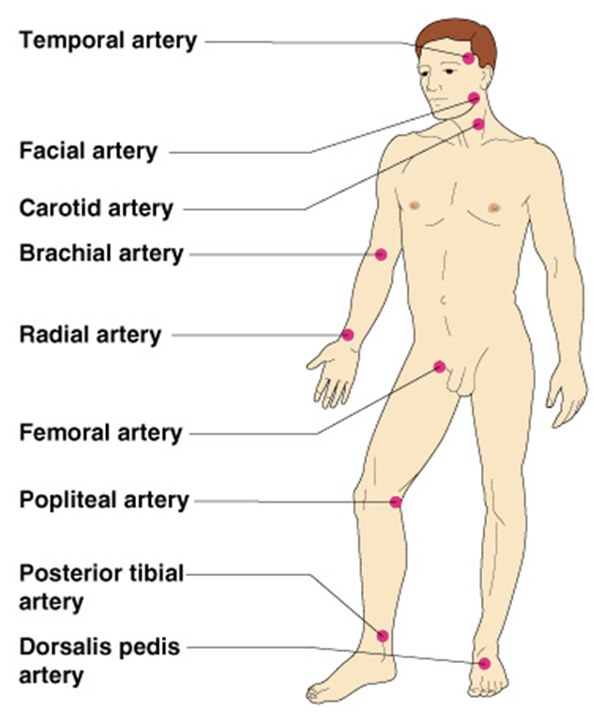
common site of pulse
temporal, carotid, brachial, radial, femoral, popliteal, posterior tibialias, dorsalis pedal
measured in BPM
DON’T use thumb b/c it has its own pulse
normal pulse range
healthy adult resting: 60-100 bpm
sleep: as low as 40 bpm
exercise: as high as 200-220 bpm
infants: 12-140 bpm
children: 90-120 bpm
older adults: ~elevated pulse to compensate ↓ cardiac output (CO)
factors that can affect pulse rate
medication
baseline data, e.g. fit person may have HR of below 60bpm
if client has been physically active, wait 15 minutes
pain
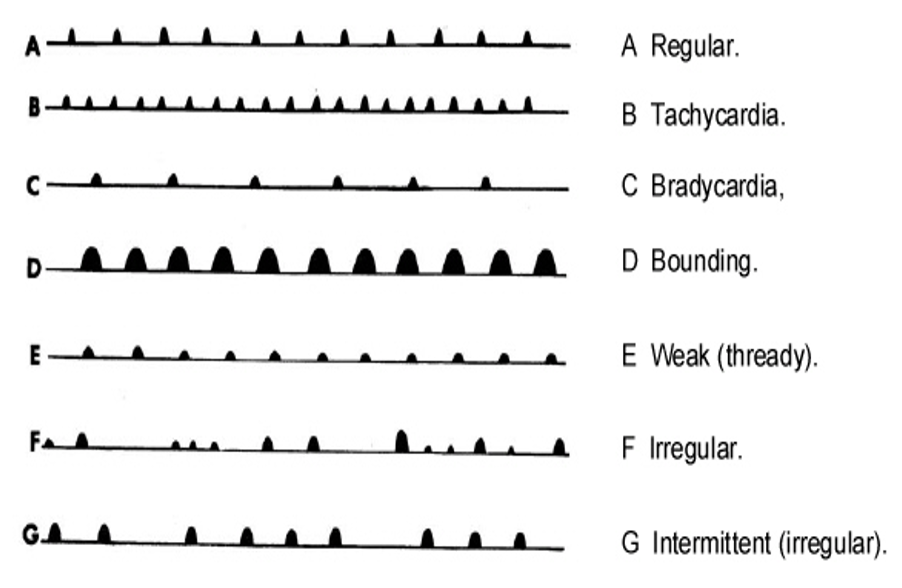
assessing pulse - 3 components
Rate
No. of beats per min.
Tachycardia, Bradycardia
Rhythm
Pattern and intervals between beats
Arrhythmia (dysrhythmia) – irregular rhythm.
May be random irregular beats, or a predictable pattern of irregular beats
Volume
Pulse strength – the force of blood with each beat
May be full or bounding pulse
Weak, feeble or thready
pulse patterns
respirations
breaths per minute
normal adult inspiration: 1-1.5 secs
normal adult expiration: 2-3 secs
asses when relaxed
exercise ↑ rate & depth
~assess after activity to identify tolerance
be aware of normal breathing pattern
respiratory rates - normal ranges
infants: 28-40 bpm
children: 20-28 bpm
adults: 12-20 bpm
assessing respirations
Rhythm
Refers to the regularity of breathing
Respirations should be evenly spaced
Quality
Aspects that are different from normal, effortless breathing
Laboured breathing – breathing with effort
Depth
Establish by watching the chest movement
Described as normal, deep or shallow
During normal breathing an adult takes in about 500ml of air. This volume is known as the “tidal volume”
Body position affects the amount inhaled
facors affect respirations
Increase the rate:
–exercise
–stress
–increased environmental temperature
–low oxygen concentration (increased altitudes)
Decrease the rate:
–decreased environmental temperature
–medications e.g. narcotics (morphine)
–increased intracranial pressure (head injuries)
–health states
–age, elderly residents
assessing respirations
Sound:
Normal breathing is silent
Some sounds are audible e.g. wheeze
Many sounds occur as a result of the presence of fluid in the lungs
common breath sounds
Wheezing
Rhonchi – low-pitched wheezes
Stridor
Crackles – fine and coarse (aka Rales)
Pleural friction rub
wheezing
Caused by narrowing of the airways, associated with
Asthma
Bronchitis
Pneumonia
COPD
Smoking
Heart failure
inhaling a foreign object into the lungs
allergic reaction
Rhonchi
Occur in the bronchi
Snoring or moaning sound
Continuous, snoring, gurgling or rattle–like quality
Occur as air moves through tracheal-bronchial passages coated with mucous or respiratory secretions
Often heard in pneumonia, chronic bronchitis or cystic fibrosis
Usually clear after coughing
Stridor
Air is moving roughly over a partially obstructed upper airway; Caused by something blocking the larynx
•choking on an object
•infection
•throat swelling
•laryngospasm
Crackles – fine
High-pitched, brief, discontinuous popping lung sounds
Sounds like wood burning
Usually start at the base of the lungs, where there is fluid in the lungs
As fluid fills the lungs more, it can be heard closer to the top of the lungs
Crackles – coarse
Coarse, rattling, crackling sounds – louder, longer and lower in pitch than fine crackles
Described as a bubbling sound, as when pouring water out of a bottle or like ripping open Velcro
Often heard just in certain spots in the lungs, possibly only one side or in different spots on both sides
Usually caused by mucous/fluid in the bronchi
Respiratory distress
Physically laboured ventilation or respiratory efforts
Dyspnoea
shortness of breath/difficulty breathing
Tachypnoea
greater than normal respiratory rate
Work of breathing (WOB)
muscle use, visible effort to breathe
Hyperventilation
Deep, rapid respirations
Apnoea
Cessation of breathing for a period
Cheynes - Stoke
Hyperventilation followed by apnea
Oxygen saturation/pulse oximetry
O2 saturation: a measure of how much O2 the blood is carrying as a % of the maximum it could carry.
1 haemoglobin carries max. 4 molecules of O2,
E.g. 3 molecules of O2 = 75% of the maximum amount of oxygen it could carry
measuring oxygen saturation
Estimate of oxygen saturation = Pulse oximeter
Clip shines a light through one side of the finger; a detector measures the light that comes through the other side.
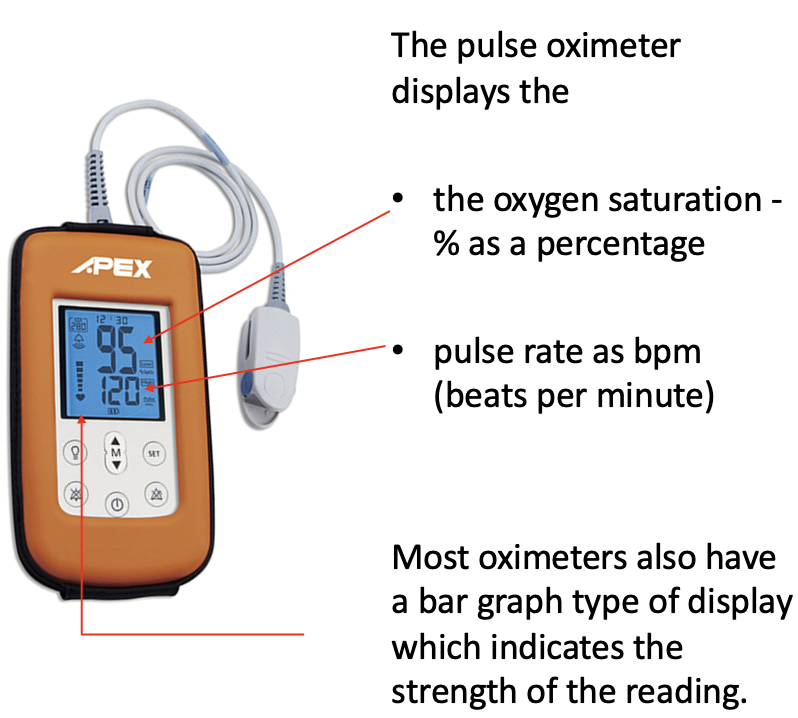
desired pulse oximetry reading: 98 and 100%
95-98% = ask them to slow down breathing
oximeter probe sites
fingers
ear lobe
bridge of nose
toes/feet
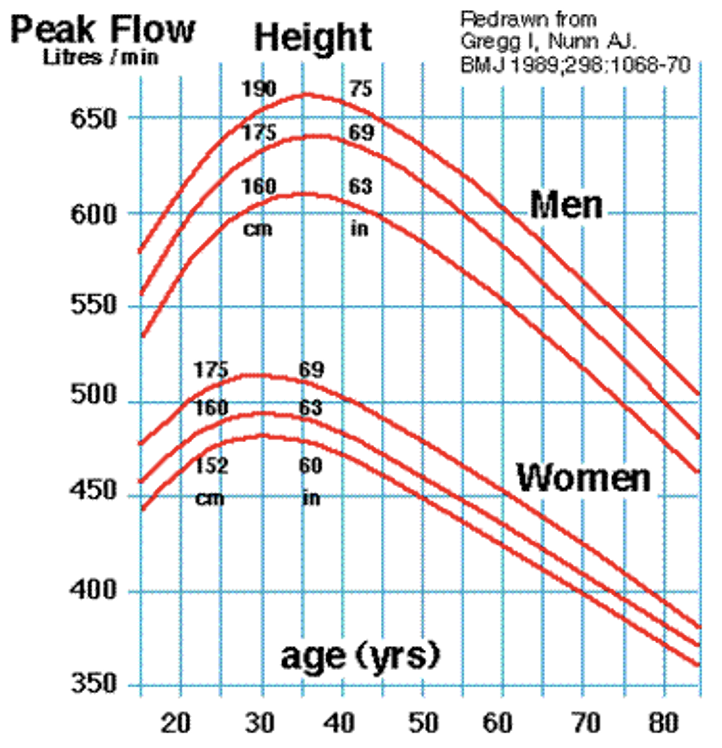
peak flow meters
measures forced expiratory reserve volume (V)
Client inhales fully and then exhales as quickly and completely as they can
Typically, do 3 readings before and after ventolin to gauge the effectiveness of the bronchodilating medication

BP
Measures the pressure exerted by the blood as it flows through the arteries
measured in millimetres of mercury (mmHg) and recorded as a fraction
avg. BP = 120/80mmHg; however, it is important to know what is normal for a client as they go from rest to physical exertion
Systolic and diastolic pressure
Systolic: amount of pressure exerted against the arterial wall as the left ventricle contracts
Systolic pressure range: 100-140 mmHg
Diastolic: amount of pressure exerted against the arterial wall as the left ventricle relaxes
Diastolic pressure: 60-90 mmHg
Normal range: 100-140/60-90 mmHg
factors affecting BP
Pumping action of the heart:
Weak heart pump = less blood is pumped into the arteries, and BP ↓
Strong heart pump and the V of blood pumped into the circulation increases = BP ↑
Peripheral vascular resistance:
Smaller space within a vessel = greater resistance
Increased vasoconstriction = BP ↑
Decreased vasoconstriction = BP ↓
Blood volume (V):
Dehydration & haemorrhage will ↓ blood V and BP because of decreased fluid in the arteries
When V ↑ = BP ↑ because of greater fluid volume in the circulatory system
Blood viscosity:
BP higher when blood is highly “viscous” (thicker)
BP may change due to:
(These factors often cause falls & faints)
↓ blood V – hypovolaemia, always think of dehydration & haemorrhage (also fluid intake, urine output)
> Is the client dehydrated?
> Are they bleeding?
Changes in position/posture – postural hypotension
Changes in temperature – vasodilation/vasoconstriction
The effects of medication – new or increased doses
stress/anxiety
pain
nutritional factors
drugs
disease
older adults tend to have elevated systolic blood pressure
Hypertension: blood pumps w/ more force than normal = approx. 150/100mmHg
Hypotension: more likely seen by specific symptoms, but approx. 100/50mmHg
equipment to measure BP


manual BP assessment - preparation
Cuff size is appropriate
Patient is sitting or lying comfortably, choose appropriate arm to perform BP – if required, support arm with pillow
Access patient’s upper arm – remove clothing or roll up sleeve
manual BP - step 1: determine radial systolic BP
Palpate the brachial artery
Place cuff 2.5cm above antecubital fossa (bend in elbow) to allow room for stethoscope diaphragm in fossa
Whilst palpating radial pulse, slowly inflate cuffs until pulse cannot be felt, inflate a further 5mmHg
Slowly deflate cuff & note where pulse returns
Leave cuff on arm for step 2
manual BP - step 2: auscultate BP
Place stethoscope diaphragm over brachial artery
Inflate cuff 200-30mmHg above palpated radial systolic read
Whilst deflating cuff slowly, note reading on sphygmo gauge when pulse beat is 1st heard
Continue to slowly deflate cuff & note reading when pulse sound disappears
Allow remaining air in cuff to escape
Remove cuff, adjust patient’s clothing & position if required
Document, hand hygiene & follow-up action if required
BP is usually measured on the arm using the brachial artery and stethoscope except if:
Client has removed axillary nodes on that side – common with mastectomies
IV infusion on that arm
Arterio-venous fistula (renal dialysis)
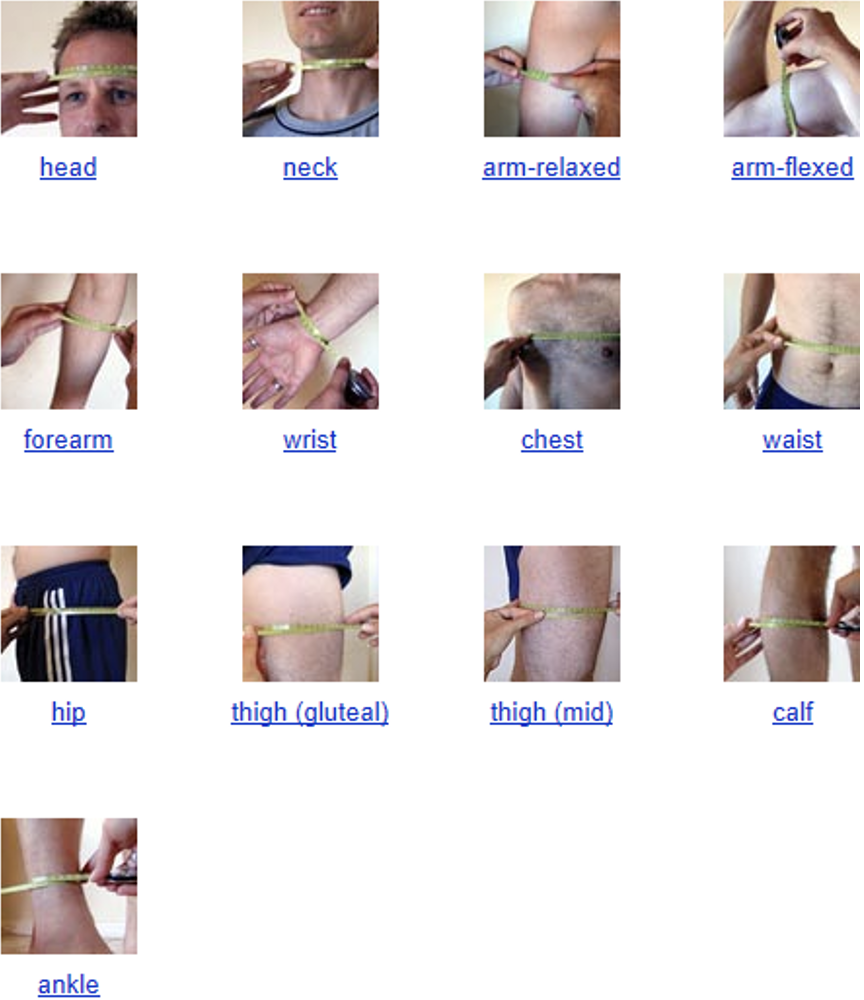
limb and girth measurements
girths are circumference measures using tape measure
determines body size and composition, & monitor changes
assessing bowel sounds
Empty bladder
Lie supine with pillow under head
Expose abdomen (maintain privacy) from above xiphoid process to the symphysis pubis
Picture abdomen in 4 quadrants
Stand on right side, look at abdomen from side and above, & xiphoid process to symphysis pubis to determine if it’s flat, scaphoid, rounded or protuberant
If protuberant, ask if it’s normal for them
Place diaphragm over RLQ & listen for bowel sounds
If you don’t hear any, continue listening for 5 mins in RLQ
Then, listen to RUQ → LUQ → LLQ
Describe sounds as absent, normoactive, hypoactive or hyperactive
Absent ~indicate ileus or peritonitis
Hyperactive ~early intestinal obstruction or gastrointestinal hypermotility
definition of pain + types
an unpleasant sensation occurring in various degrees of severity as a consequence of injury, disease or emotional disorder
types: acute or chronic
physiological effects of pain
↑ catabolic demands → poor wound healing, weakness & muscle breakdown
↓ limb movement → ↑ risk of DVT/PE
respiratory effects: shallow breathing, tachypnea & cough suppression → ↑ risk of pneumonia & atelectasis
↑ sodium & water retention (renal)
↓ gastrointestinal mobility
tachycardia & elevated BP
negative emotions: anxiety, depression
sleep deprivation
what does pain mean to clients?
poor prognosis or impending death – esp. when pain worsens
↓ autonomy (independence/freedom)
impaired physical or social functions
↓ enjoyment & quality of life
challenges to dignity
threat of ↑ physical suffering
neuropathic pain
pain transmitted over damaged nerves
described as burning, electric, searing, tingling & migrating
causes: amputation, shingles, diabetic neuropathy, fibromyalgia & cancers that affect spinal cord, etc.
principles of pain assessment
assess & reassess
use methods appropriate to cognitive status & context
assess intensity, relief, mood & side effects
use verbal report when possible
document in a visible place
accountability
include the family
client pain history
site/s of pain
severity of pain
date of onset
duration
what aggravates or relieves pain
impact on sleep, mood & activity
effectiveness of previous meds
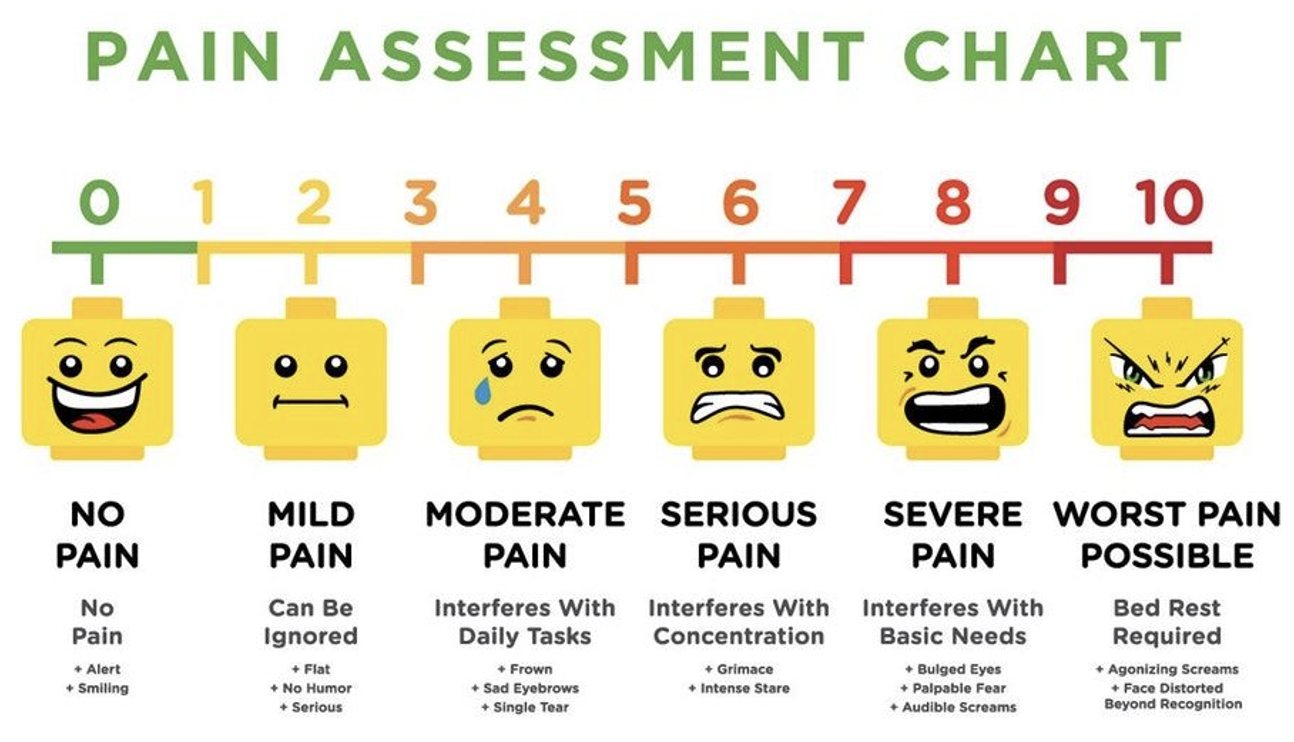
0-10 pain assessment method
PQRST method of pain assessment
P = Provocation/Palliation
Cause? Trigger? Stress? Position? Certain activities?
Relieves? Meds, massage, heat/cold, position, active, rest?
Aggravates? Movement, bending, lying, walking, standing?
Q = Quality/Quantity
Describe pain: sharp, dull, stabbing, burning, crushing, throbbing, nauseating, shooting, twisting or stretching.
R = Region/Radiation
Location? Radiate? Where? Travels/moves around? Start elsewhere and now localised to one spot?
S = Severity Scale
0-10? How bad is it at its worst? Does it force you to sit down, lie down, slow down? How long does an episode last?
T = Timing
When start? How long last? How often does it occur? Sudden or gradual? When occur? Awakened by it? Lead to anything else? Accompanied by other symptoms? Occur before, during or after meals?
Pharmacological management of pain
Mild to moderate pain:
•NSAID’s (nonsteroidal anti-inflammatory drugs) eg
paracetamol (Panadol), ibuprofen (Nurofen)
•Cox 2 inhibitors are a form of (NSAID) that directly targets COX-2, (cyclooxygenase-2) an enzyme responsible for inflammation and pain eg Celecoxib (Celebrex)
Moderate to severe pain:
•Morphine sulphate
•Oxycodone
•Codeine
•Oxycontin
•Methadone
•Fentanyl
•Hydromorphine
•
Principles of opioid analgesic use in acute and cancer pain
•Individualise route, dosage, and schedule
•Administer analgesics regularly (not PRN) if pain is present most of day
•Become familiar with dose / time course of several strong opioids
•Give infants / children adequate opioid dose
•Follow clients closely, particularly when beginning or changing analgesic regimens
Important principles
•Round the clock dosing for predictable pain
•start Low, go Slow
•the client is the ultimate authority on their pain – do not second guess them
Barriers to opioid use
•Fears about addiction
•Underestimating pain
•Normalising pain
Non pharmacologic management of pain
Do not teach these when the client is in an acute pain episode
Use in conjunction with, not instead of pharmacologic methods
•Exercise
•Heat/cold application – use with caution
•Lotions/massage therapy – use with caution
•Positioning – including pillows and pressure relieving devices/aids
•Aqua-therapy, including showers/baths
•Transcutaneous electrical nerve stimulation (TENS)
•Acupuncture/acupressure