H7: Guest lecture cancer screening
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
health promotion
Encouragement of activities that facilitate healthy living and well-being
Disease prevention
Assessment of health risks and development of interventions that halt disease progression
Burden of disease of cancer
2nd leading cause of death worldwide
Europa high number but not many die (compared to other countries)
Mortality trends: general decrease across whole population
cancer-specific example of primary prevention
Tobacco cessation programs to prevent lung cancer
cancer-specific example of secondary prevention
Mammography screening for breast cancer
cancer-specific example of tertiary prevention
Pain management during cancer therapy
Screening
checking for disease in individuals who have no symptoms
Two major approaches of screening
opportunistic screening = test is offered during consultation for other reason
population screening = systematic, organized invitation of population (subset) (
Why screen for cancer? (4)
High disease burden (urgency!)
Availability of tests and treatment (is it ethical to screen if we don’t have treatment?)
Possibility of detection before symptoms appear (pre-clinical stage)
Improve health outcomes
What is the goal of cancer screening? (3)
Reduce cancer mortality
Reduce cancer incidence
Improve survival and quality of life
Example: colorectal cancer screening
Takes 15 years = BIG WINDOW for detection and do something about it
Can keep growing and spread
Screening itself: All individuals aged 55-75 are invited every two years
- Receive a stool test by mail (fecal immunochemical test, FIT)
- Recognizable purple envelope
- Examination in the lab → results
If the stool test contains more blood than the cut-off value = positive test
→ a follow-up diagnostic test is needed: colonoscopy
Harms of screening?
Balance between benefits and harms!
- Physical
- Psychological
- Economical
→need to be considered for before implementation and continuously evaluated
example of screening harm: false positive stool test in colorectal cancer screening : potential harms on 3 lvls
Physical: Unnecessary colonoscopy and bowel preparation, small risk of complications
Psychological : Anxiety/distress due to positive test, altered self-perception
Economical: Colonoscopy costs, wasted medical capacity, transportation, productivity loss
example of screening harm: false negative stool test in colorectal cancer screening : potential harms on 3 lvls
Physical : Missed findings, worse survival outcomes and quality of life
Psychological : Emotional burden, false reassurance, potential continuous engagement in risk factors
Economical: High treatment costs in late cancer stages, productivity loss
Other potential harms and considerations of screening (5)
Overdiagnosis
Diagnosing disease that would not negatively affect an individual during their lifetime
Equity
Access to screening: socioeconomic, geographic, health insurance coverage (less in EU, but like US health reassurance companies)
Racial/ethnic disparities in health outcomes
Health literacy
maybe some ppl don’t understand etc: display and phrased very important
for example; the letter and envelop for colorectal screening
Cultural barriers
Environmental impact
Cancer screening: PARTICIPATION
Decreasing trend observed in various European countries over last few years
Lowest point during COVID-19 pandemic and only slight recovery of participation in the Netherlands
=> Low screening participation meaningfully reduces the effectiveness of screening programs!
Multiple factors influence screening participation (3)
Fear (can work in 2 ways: motivator or avoidance)
perception of risk
social influence
Fear as influence of screening participation
Can be a powerful motivator (intention to participate)
«»
Too much fear can lead to avoidance (lower participation)
Perception of risk as influence in screening participation
People with higher perceived risk of cancer are more likely to participate
Emotional sensitivity to probabilities and bias for action
Commission bias = tendency to choose active treatment even when watchful waiting is less risky
People are bad at interpreting risks (relative vs. absolute risks)
Absolute risks are generally easier to interpret
Visualizations are helpful and often used in information material
social influence in screening participation
o Social norms and influence from family, friends, and doctors can significantly impact a person’s decision to get screened
o Family support may be particularly important in younger individuals
o Interaction with health professionals may positively affect screening behavior in older individuals
o High-profile events can meaningfully influence behaviors in other health domains (e.g., COVID-19 pandemic)
Different strategies are used to increase awareness and attendance (5)
Research, education and information
adressing cultural barriers (language, aversians, …)
general opportunities for counseling and to resolve questions (conversation, more info, specialized phone line)
motivational interviewing
social marketing
How to implement and improve cancer-screening programs in other countries?
Ideally, conduct large, RCTs to investigate which screening strategies are effective
However, this would be:
o difficult to set up
o take a long time (decades)
o extremely expensive
o unethical
a way around problems of conducting large RCTS to investigate screening strategies
simulation modelling
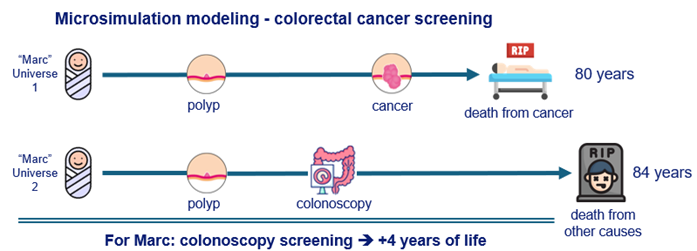
simulation modelling (microsimulation)
a way around problems of conducting large RCTS to investigate screening strategies
Computer program to simulate the life of individuals (from birth to death)
Uses data such as life expectancy, cancer incidence, screening attendance
For the simulation we aggregate and use many information that exists like life expectancy
Ok 2 babies, eventually they die, but difference in when they die, life varies
Simulate many individuals, count outcomes (life-years, colonoscopies, cancer deaths…)
=> Compare strategies
(example: If we go back to savepoint and act what if he does a screening
→ See what is effect of screening: has 4 additional years of life )
EU-TOPIA
Online platform to use country-specific data in a simulation model
Quantify future harms and benefits of different cancer screening scenarios in their country
→ Help governments and medical societies to make better decisions
EU-TOPIA-EAST 3 steps
1. Implement feasible interventions in some regions and monitor short-term screening performance (participation and detection)
2. Estimate resources, health outcomes and cost-effectiveness of scaling up the interventions to a national level
3. Communicate good implementation practices from participating countries to other MIC in Eastern Europe and the Mediterranean
How can we improve screening?
- Develop and implement better screening tests in current screening programs
- Develop effective tests for diseases without current screening programs
- Improve the balance of harms and benefits
Personalization of screening
Goal: Reducing the burden for people with low risk and focus on high-risk groups
«» Now: everyone has same criteria etc → personalize more
Challenges with the personalization of screening
Requires extensive pilot testing to show benefits
Focus on high-risk individuals → screening some people more and some people less!
Screening programs become more difficult to understand for participants
Some changes may take a long time to be implemented