Lecture 4 - childhood and adolescent psychological problems
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
conduct disorder (CD)
-ongoing pattern of behaviour where the rights of others or social norms are infringed
-show at least 3 features over 12 months
-CD before 10 years and after is adolescent CD
-if patients is over 18 then condition is better explained by antisocial personality disorder
features of CD
-bullying or threatening others
-starting fights
-weapon to do serious physical harm
-physical cruelty to people or animals
-forcing another into sexual activity
-fire setting
-deliberate destruction of property
-lies to get goods or favours
-run away from home twice or once for long period of time
-often misses school
oppositional defiant disorder (ODD)
angry and irritable mood
argumentative defiant behaviour
vindictiveness
angry and irritable mood (ODD)
-often easily loses temper
-frequently touchy and easily annoyed by others
-is often angry and resentful
argumentative defiant behaviour (ODD)
-often argues with adults or people in authority
-actively defies or refuses to comply with adults’ requests or rules
-deliberately annoys or upsets people
-often blames others for mistakes or behaviours
vindictiveness (ODD)
-often spiteful or vindictive
-shown spiteful or vindictive behaviour at least twice in the past six months
medicalising bad behaviour
-12% children have mental disorders, 5% of 2-4 years have mental health issues
-NHS accused of medicalising bad behaviour when such behaviour is normal in children
-however disorders are long-term and chronic with aggressive impulses and difficulties with authority → issues with schools, employment and long-term relationships
quality of life (CD)
-physical and mental problems
-hospitalised
-criminal behaviour
-going to prison
-difficult relationships with peers and partners
-unemployed, homeless, dependent on benefits
-difficulties being a carer
incidence of CD
1-2% women
2-2.5% men
heritability of CD
-5-74%
-very variable
-could be heritability is irrelevant for CD and diagnosis is not actually defining anything
-diagnostic criteria is very broad → 32000 symptom profiles for CD
-if include CU traits as part of diagnostic criteria have more stable heritability → most extensive find 40-50%
-often comorbid with ADHD
callous and unemotional traits
-persistent pattern of behaviour that reflects a disregard for others, lack of empathy and generally deficient affect
-distinct problems in emotional and behavioural regulation that distinguish them from other antisocial youth → similar to adult psychopathy
-distinctive cognitive characteristics → less sensitive to punishment cues and keen for rewards
maternal factors (environmental risk factors for CD)
-smoking, alcohol, drug use
-stress
birth factors:
-birth complications
-parental psychopathology
-malnutrition
-gene-environment interplay
familial factors (environmental risk factors for CD)
-during childhood and adolescence
-harsh and inconsistent discipline
-parent-child conflict
-low socio-economic status and poverty
-gene-environment correlations
extra-familial factors (environmental risk factors for CD)
-community violence
-association with deviant peers
-gene-environment correlations
genetic factors (dispositional risk factors for CD)
-during childhood
-autonomic
-neurocognitive
-social information processing
-temperament
-personality traits
passive gene-environment correlation
-environment and genes from parents, surrounding or extra familial environments
active gene-environment correlation
-genetic predisposition to something and then go out and seek it
-peer groups most pertinent to CD and anti-social behaviour
-CD mediated longitudinally by seeking out anti-social peer group
evocative gene-environment correlation
-behave in certain manner and this evokes responses from people in the environment and then tendency from genes is reinforced
-creates circular effect
issues with genetic influences on CD
-not particularly well-defined terms
-with large heritability might be higher than if thinking about what genes do in isolation or if cohort is larger, small genetic predisposition but multiplies across life then heritability looks higher in older cohort
genome-wide association study (GWAS)
-observational study of genome-wide set of genetic variants in different individuals to see if any variant is associate with a trait
-typically focus on associations between single-nucleotide polymorphisms (SNPs) and major human diseases
-can be applied to any genetic variants and other organisms
phenotype first (GWAS)
-compare DNA of participants having varying phenotypes for particular trait
-may be people with a disease and similar people without the disease
-participants are classified by their first clinical manifestations → opposed to genotype-first
-gives sample of DNA → genetic variants read using SNP arrays
-if one type of the variant is more frequent in people with the disease the associated SNPs then considered to mark a region of the human genome linked to the disease
single nucleotide polymorphism (SNP)
-AT pairs and CG pairs
-single nucleotide is different across people → compare across people
-difficult to repeat as have to do a t-test about 20,000 times with very stringent p value to reduce false positives
CD and genes
RBFOX1 → fox-1 homolog A, A2BP1, HRNBP1 is a protein that is encoded by RBFOX1 gene linked to development
GABRA2 → gaba, inhibitory
SLAC6A4 → serotonin transporter
oxytocin receptor OXTR
C1QTNF7 → glucose metabolism and insulin signalling
MAO gene (CD)
-enzyme breaks down mono-amine neurotransmitters
-MAO-L is less active → leads to increase in sensation seeking behaviour
-want more of it as having more of neurotransmitter linked to CD
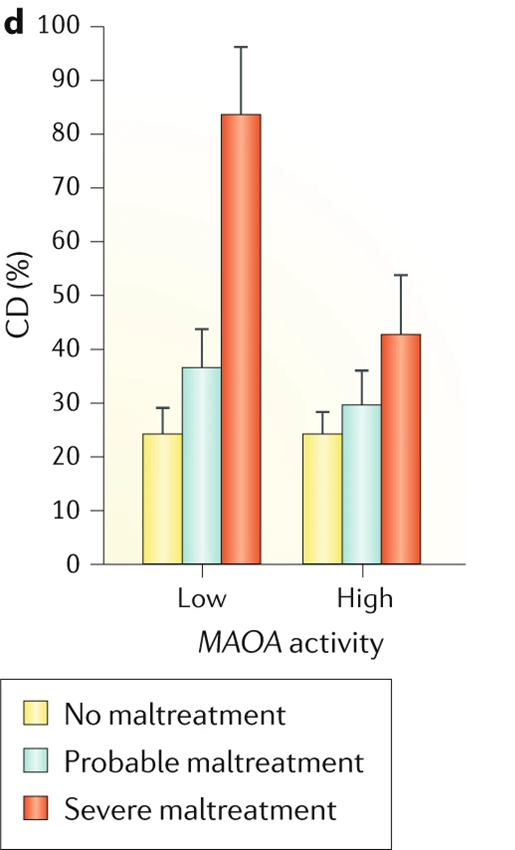
gene-environment interaction and CD
-low form of MAO gene and severe maltreatment leads to very high cases of CD
-low levels of maltreatment have lower incidence of CD
-normal MAO gene still have increase CD relating to maltreatment but do not have massive increase associated with low MAO gene
neurocognitive factors
-verbal IQ, WM, EFs, emotion recognition
-less sensitive to punishment cues → overly sensitive to reward
brain function and CD
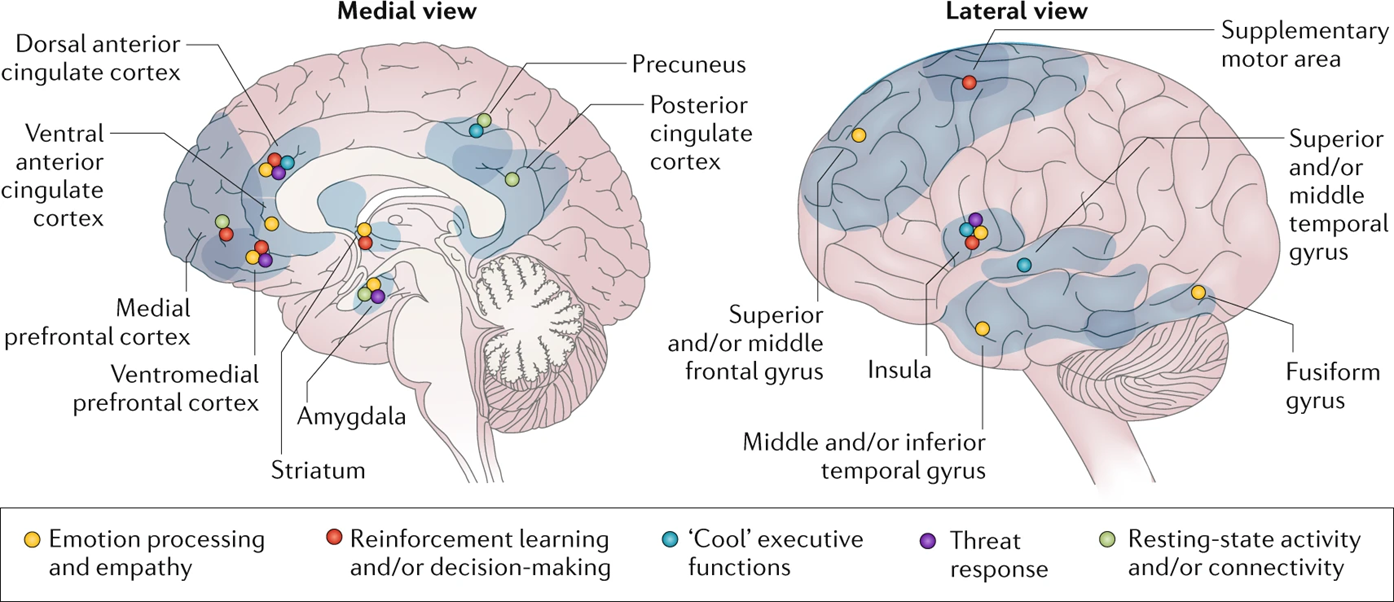
EF and decision making (brain function and CD)
-front parts of brain
-dorsal anterior cingulate cortex, ventral anterior cingulate cortex, medial PFC, ventromedial PFC
amygdala (brain function and CD)
-threat response and emotional processing and empathy
striatum (brain function and CD)
-basal ganglia involved in reinforcement learning and/or decision-making
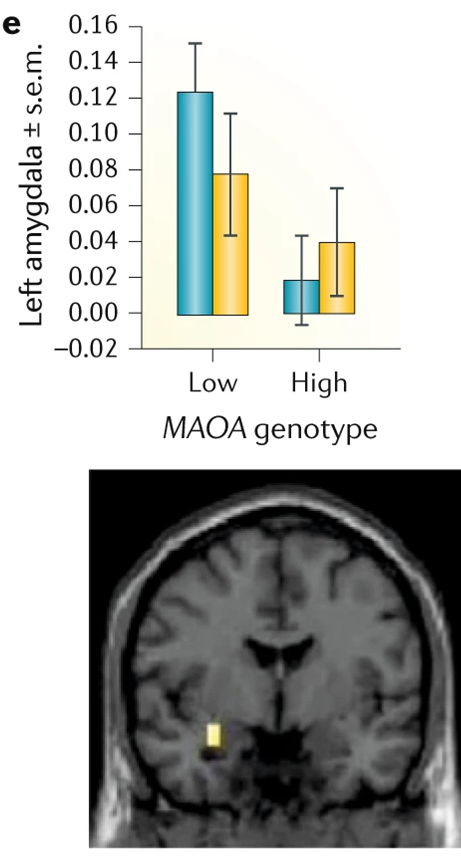
meyer - method (brain function and CD)
-people with low and high MAOA genotype
-observe amygdala response to different facial expressions
meyer - results (brain function and CD)
-if have low form of MAOA then amygdala overresponds to fearful/angry faces
-bias for negativity → overrespond to threat leading to hostile attributional bias
-interpret not only ambiguous cues as signalling hostility but also cues generated with harmless intentions
-deactivation of anterior cingulate cortex → linked to decision making and emotion processing
-if have low form of gene tend to have a 0 response
differences in neuronal density (CD)
-caudate nucleus
-putamen
-anterior insula
-amygdala
-ventromedial/lateral PFC
-orbitofrontal cortex
LPE (management of CD without comorbid disorders)
-limited prosocial emotions
-helping parents not reward poor behaviours
early to middle childhood without LPE (management of CD without comorbid disorders)
-psychosocial intervention
-social-learning theory based
late childhood and adolescence without LPE (management of CD without comorbid disorders)
-psychosocial intervention
-social learning theory based parent training and child skills training
early to middle childhood with LPE (management of CD without comorbid disorders)
-social learning theory based parent training with additional training focussing on parental warmth
-child skills training focussing on empathy
late childhood and adolescence with LPE (management of CD without comorbid disorders)
-social learning theory based parent training focussing on parental warmth
-general child skills training with additional skills training focussing on empathy
ineffective psychological interventions (management of CD without comorbid disorders)
-poor response and impulsive-aggressive behaviour
-add medication → risperidone, psychostimulants and/or risperidone (CD with comorbid ADHD)
internalising comorbidity (management of CD in those with comorbid disorders)
-anxiety, depression or PTSD
-psychosocial intervention for CD
-if comorbid disorder persists add evidence-based disorder-specific psychosocial intervention and/or disorder-specific medication
externalising comorbidity (management of CD in those with comorbid disorders)
-ADHD or ODD
-psychosocial intervention for CD
-first line:
stimulants for ADHD symptoms → may also reduce impulsive aggression
-second line:
risperidone for impulsive-aggressive behaviour and hyperactivity → but is first line in children with comorbid ID
comorbid developmental disorders (management of CD in those with comorbid disorders)
-elimination disorders or language disorders
-psychosocial intervention for CD
-if comorbid disorder persists add disorder-specific intervention for comorbid disorder
pharmacological therapies
-stimulants → ritalin
-antipsychotics