Respiratory Assessment 2 Final Exam
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
An ECG is used to evaluate the-
electrical activity of the heart
Inherent Rates: Sinus node
60-100 bpm
Inherent Rates: AV junction
40-60 bpm
Inherent Rates: Ventricles
20-40 bpm
Pacemaker site with the fastest rate will generally-
control the heart
Irritability is a site along the conduction pathway
becomes-
irritable and speeds up, thus overriding higher pacemaking sites for control of the heart.
Escape Mechanism is the
normal pacemaker slows down or fails, and a lower pacing site assumes pacemaking responsibility
Autonomic Nervous System: Sympathetic
Affects the atria and ventricles
Increases:
-Heart rate
-Conduction
-Irritability
Autonomic Nervous System: Parasympathetic
Affects only the atria
Decreases:
-Heart rate
-Conduction
-Irritability
Electricity flowing toward positive electrode produces an
upright pattern
Electricity flowing toward negative electrode produces an
inverted pattern
What Voltage is measured by
Comparing the height of the spike to the horizontal lines on graph paper
What is Time measured by
Comparing the markings to the vertical lines on the graph paper
In order to analyze EKG rhythm strip you need to-
Use organized format to collect available clues
Compare information collected to rules for each arrhythmia
Calculating Heart Rate –Regular Rhythms: Count number of large squares between
Two R waves and divide into 300
Calculating Heart Rate –Regular Rhythms: Count number of small squares between
Two R waves and divide into 1500
Figuring Rates Based on the Number of QRS Complexes in a 6-Second Strip is where you
Count number of R waves in a 6-second strip and multiply by 10
Rhythm Strip Analysis Format
Regularity (Rhythm)
Rate
P Waves
PRI intervals
QRS Complexes
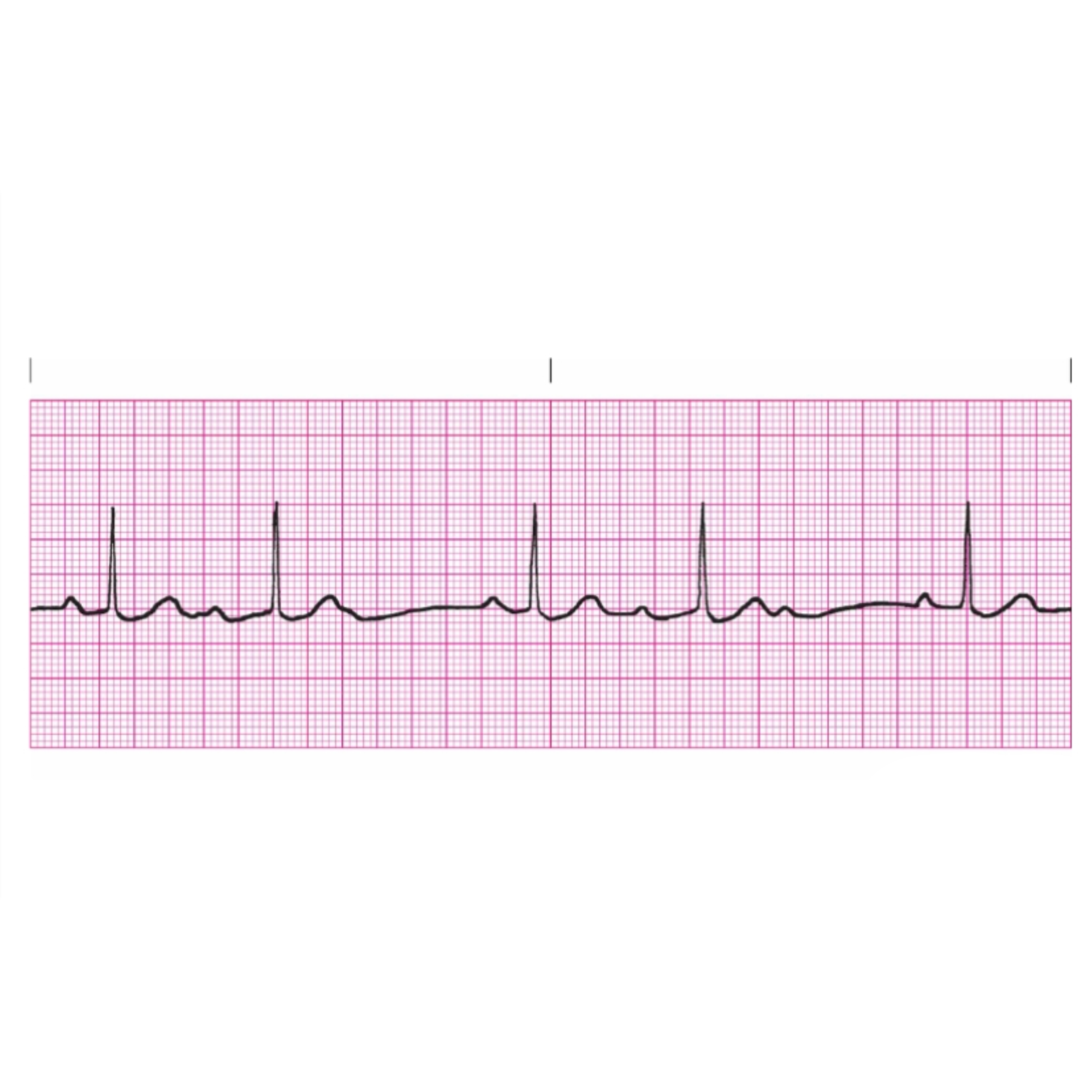
Mechanism of Normal Sinus Rhythm is when
sinus node initiates regular impulses at a normal rate. Each impulse is conducted normally to the ventricles
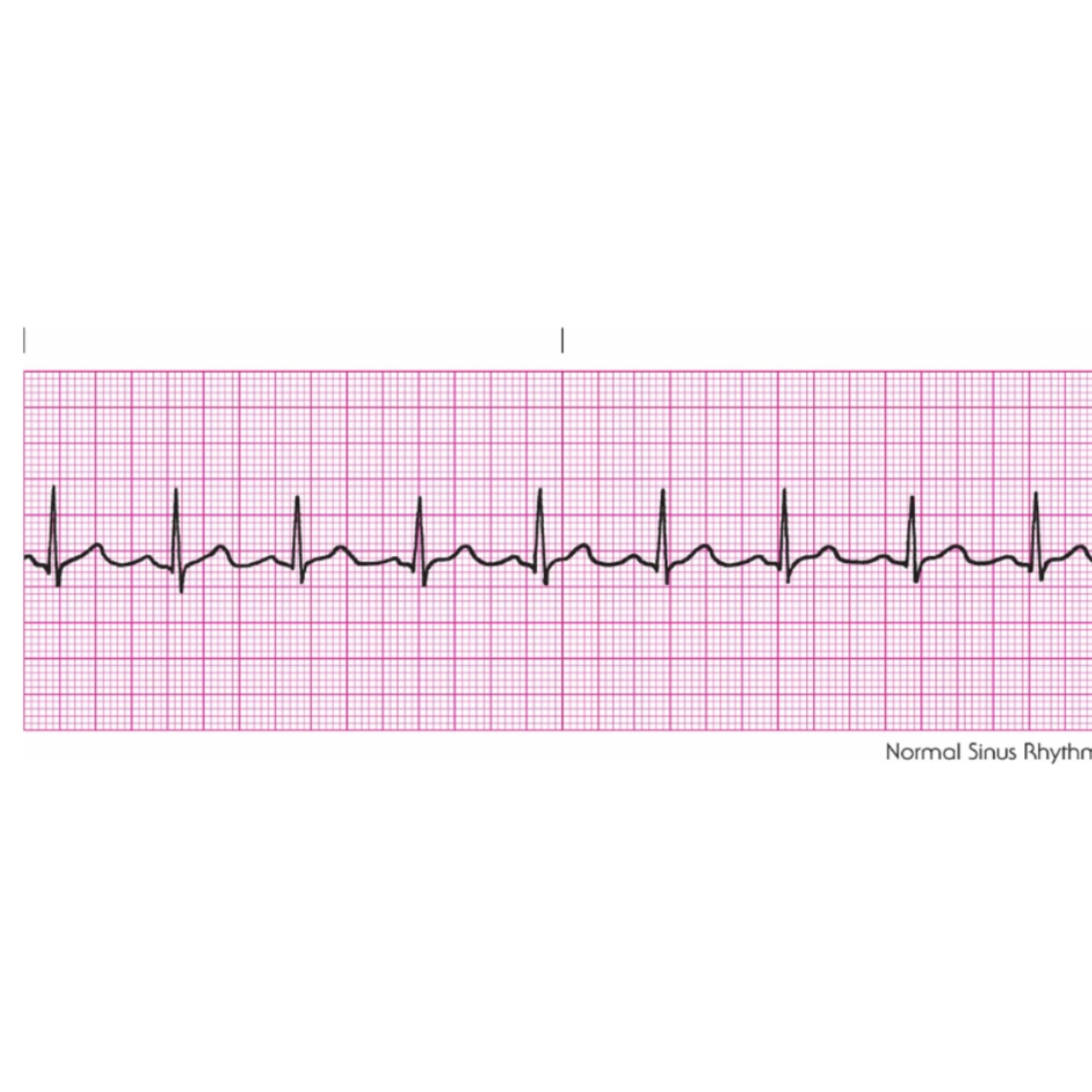
Rules for Normal Sinus Rhythm is when
Regularity: Regular
Rate: 60–100 bpm
P Wave: Uniform shape; one P wave in front of every QRS complex
PRI: 0.12–0.20 second and constant
QRS: Less than 0.12 second
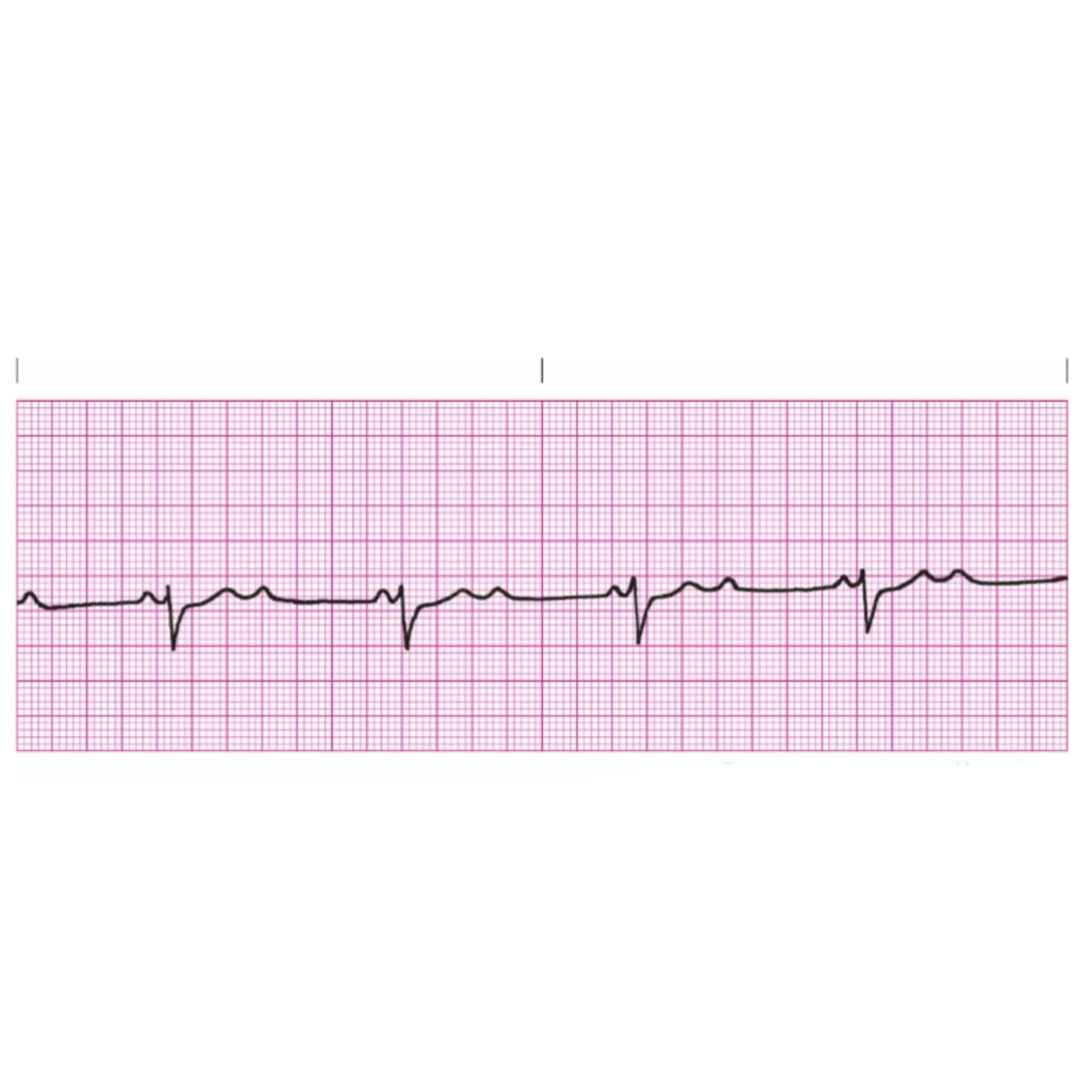
Mechanism of Sinus Bradycardia is when
the sinus node is the pacemaker, firing regularly at a rate of less than 60 times per minute. Each impulse is conducted normally through to the ventricles
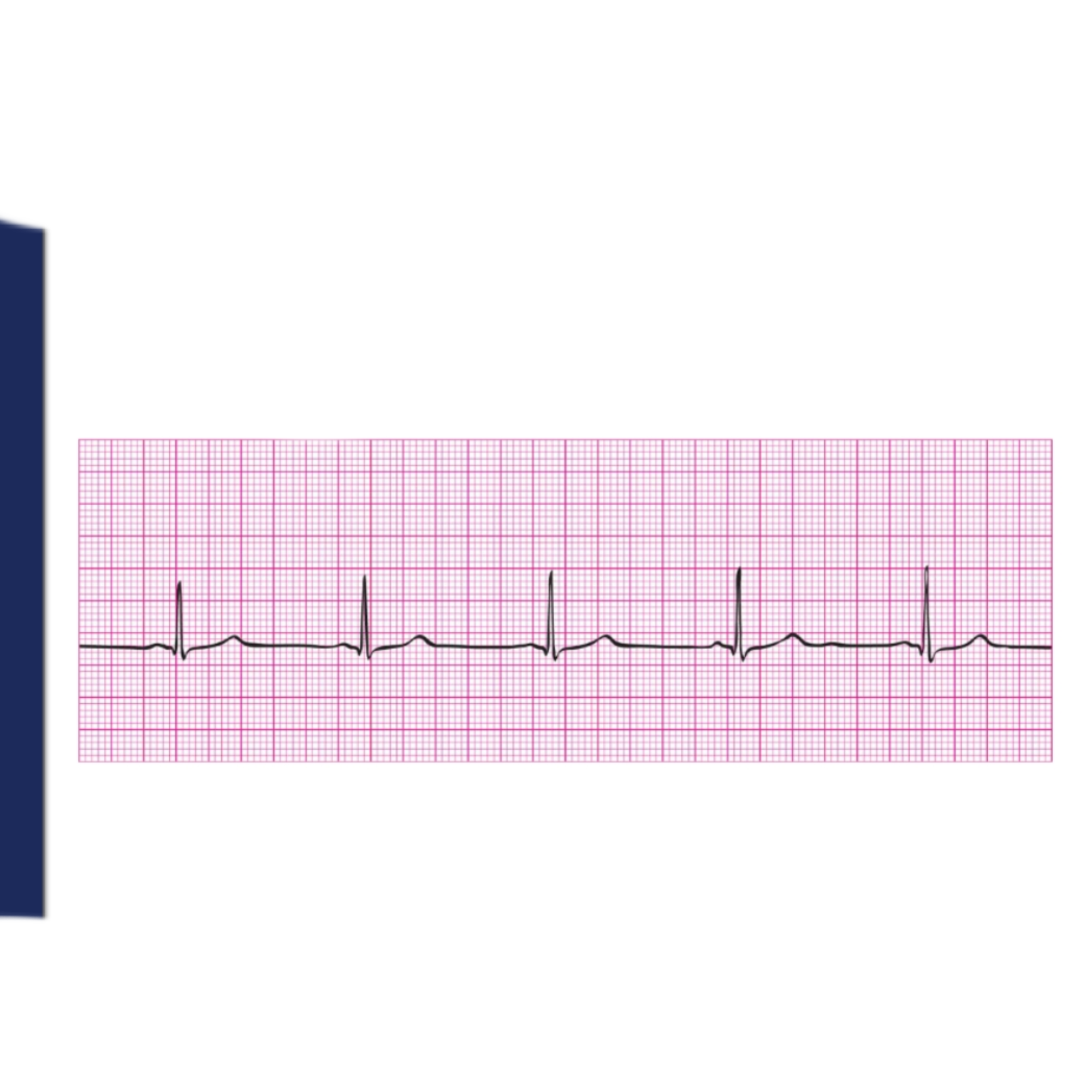
Rules for Sinus Bradycardia includes
Regularity: Regular
Rate: Less than 60 bpm
P Wave: Uniform shape; one P wave in front of every QRS complex
PRI: 0.12–0.20 second and constant
QRS: Less than 0.12 second
Mechanism of Sinus Tachycardia includes
the sinus node is the pacemaker, firing regularly at a rate of greater than 100 bpm. Each impulse is conducted normally through to the ventricles
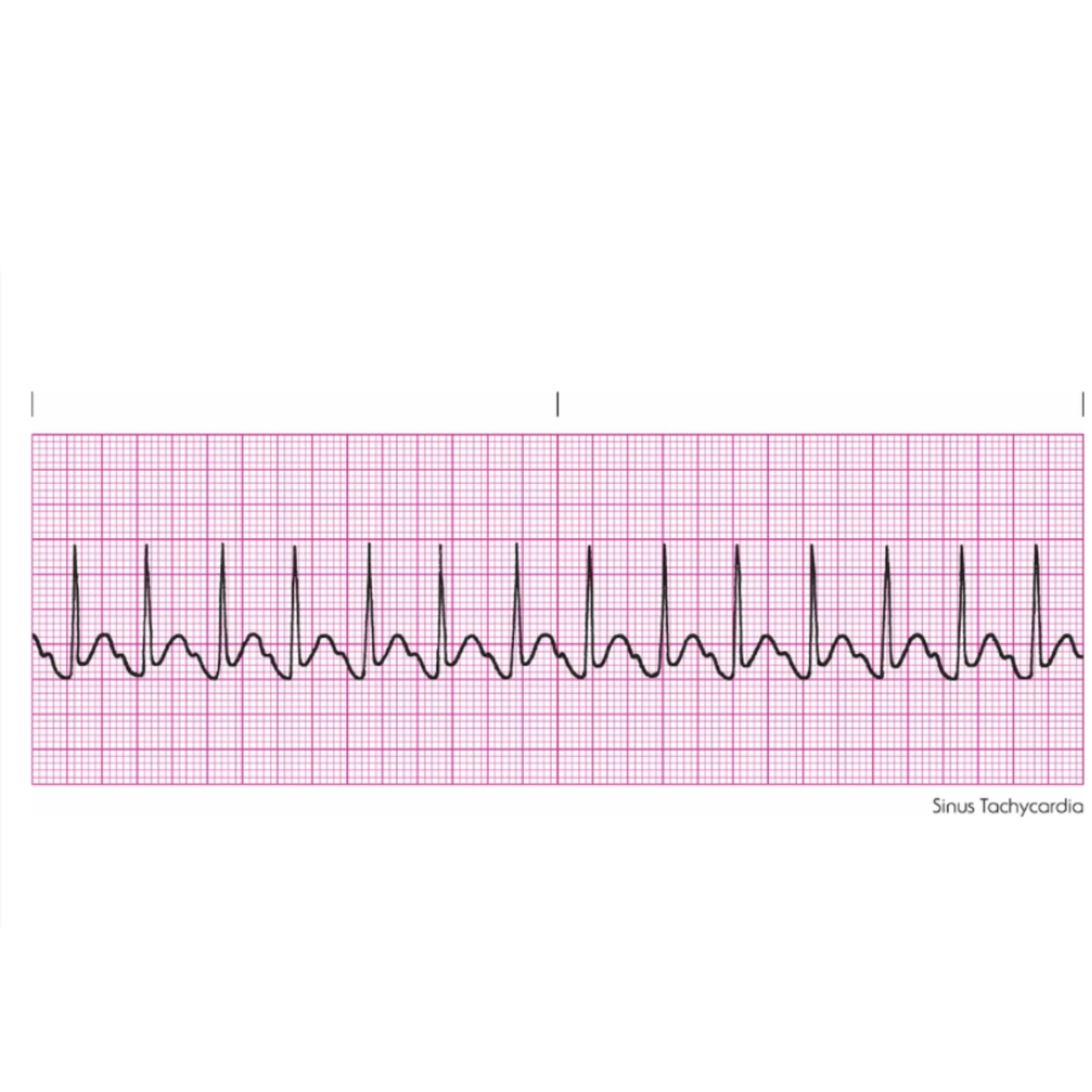
Rules for Sinus Tachycardia includes
Regularity: Regular
Rate: Greater than 100 bpm (usually does not exceed 160 bpm)
P Wave: Uniform shape; one P wave in front of every QRS complex
PRI: 0.12–0.20 second and constant
QRS: Less than 0.12 second
Mechanism of Sinus Arrhythmia includes
the sinus node is the pacemaker, but impulses are initiated in an irregular pattern. The rate increases as the patient breathes in and decreases as the patient breathes out. Each impulse is conducted normally through to the ventricles
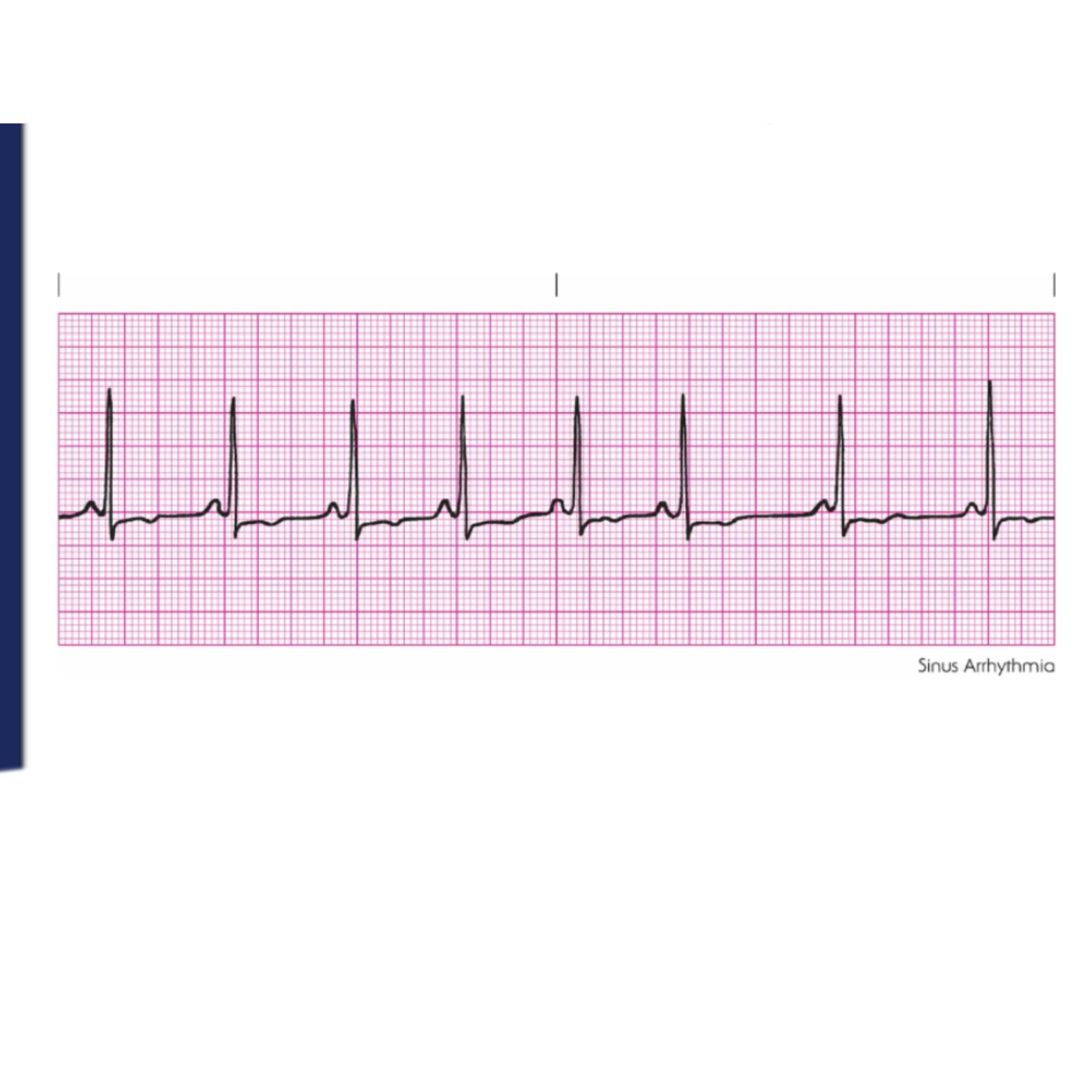
Rules for Sinus Arrhythmia includes
Regularity: Irregular
Rate: 60–100 bpm (usually)
P Wave: Uniform shape; one P wave in front of every QRS complex
PRI: 0.12–0.20 second and constant
QRS: Less than 0.12 second
Mechanism of Wandering Pacemaker includes
the pacemaker site wanders between the sinus node, the atria, and the AV junction. Although each impulse originates from a different focus, the rate usually remains within a normal range, but it can be slower or faster. Conduction through to the ventricles is normal
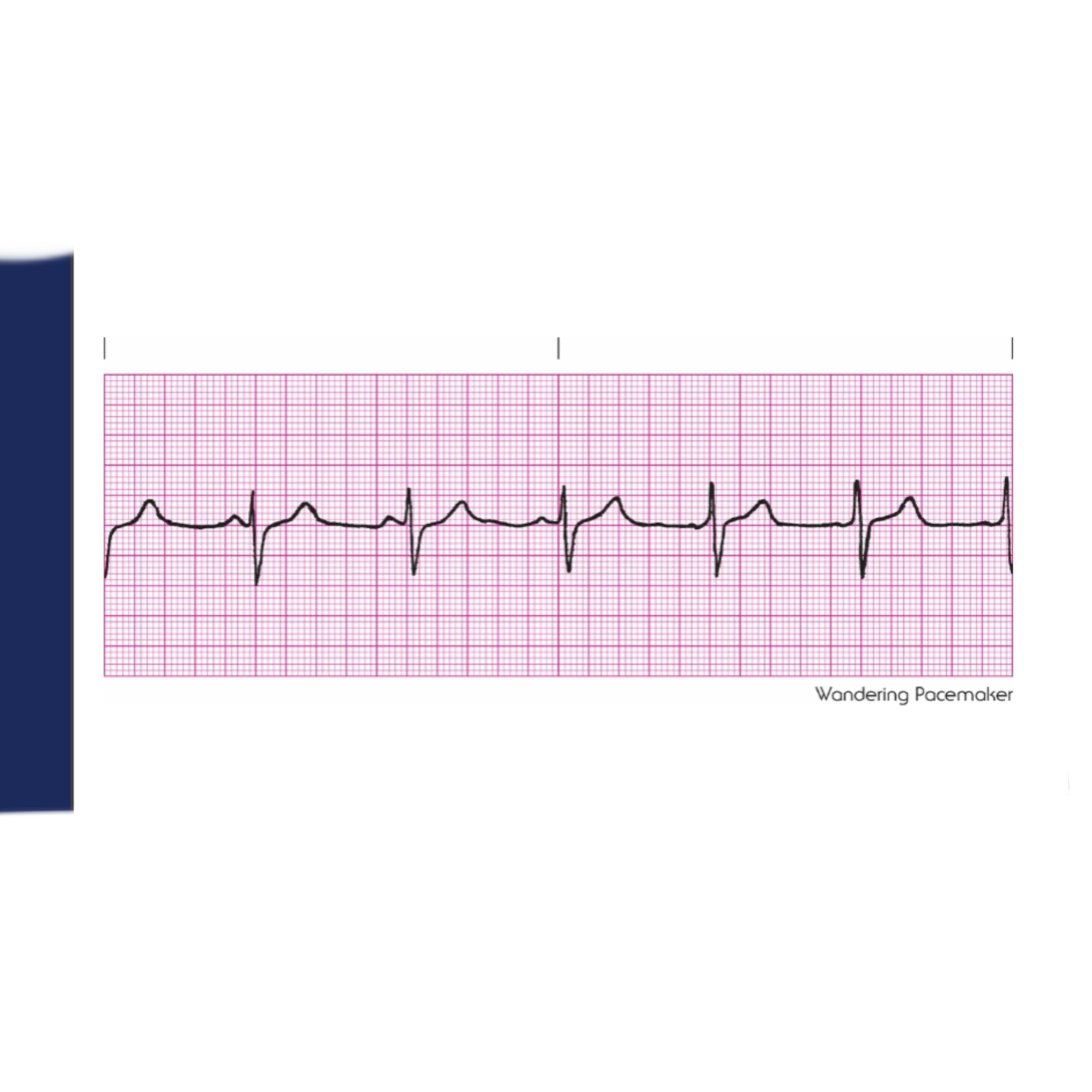
Rules for Wandering Pacemaker includes
Regularity: Slightly irregular
Rate: Usually normal, 60–100 bpm
P Wave: Morphology changes from one complex to the next
PRI: Less than 0.20 second; may vary
QRS: Less than 0.12 second
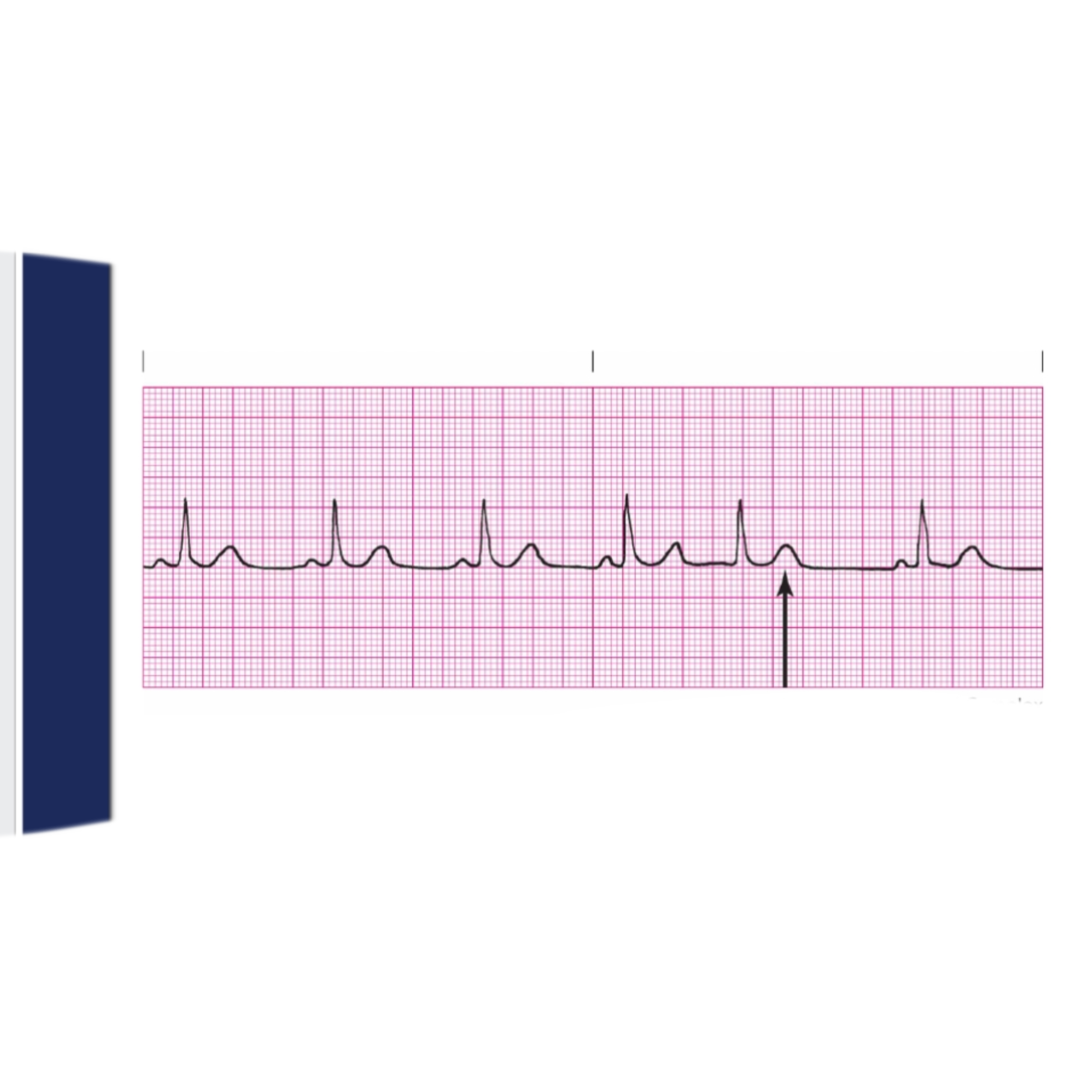
Mechanism of Premature Atrial Complex includes
the pacemaker is an irritable focus within the atrium that fires prematurely and produces a single ectopic beat. Conduction through to the ventricles is normal. This is a single beat, not an entire rhythm; the underlying rhythm also must be identified.
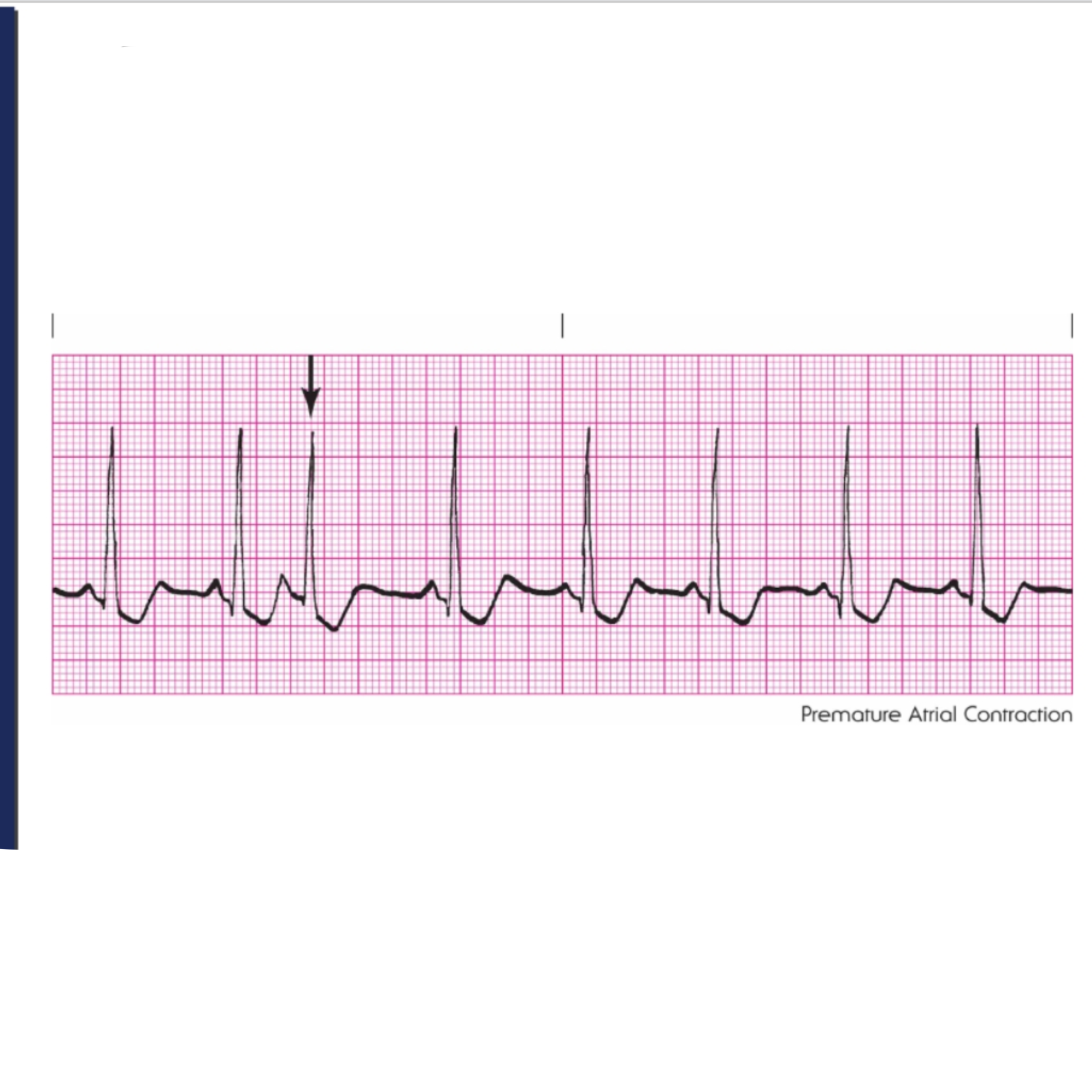
Rules for Premature Atrial Complex are
Regularity: Depends on the underlying rhythm;
regularity will be interrupted by the PAC
Rate: Depends on the underlying rhythm
P Wave: P wave of early beat differs from the sinus P waves; can be flattened or notched; may be lost in the preceding T wave
PRI: 0.12–0.20 second; can exceed 0.20 second
QRS: Less than 0.12 second
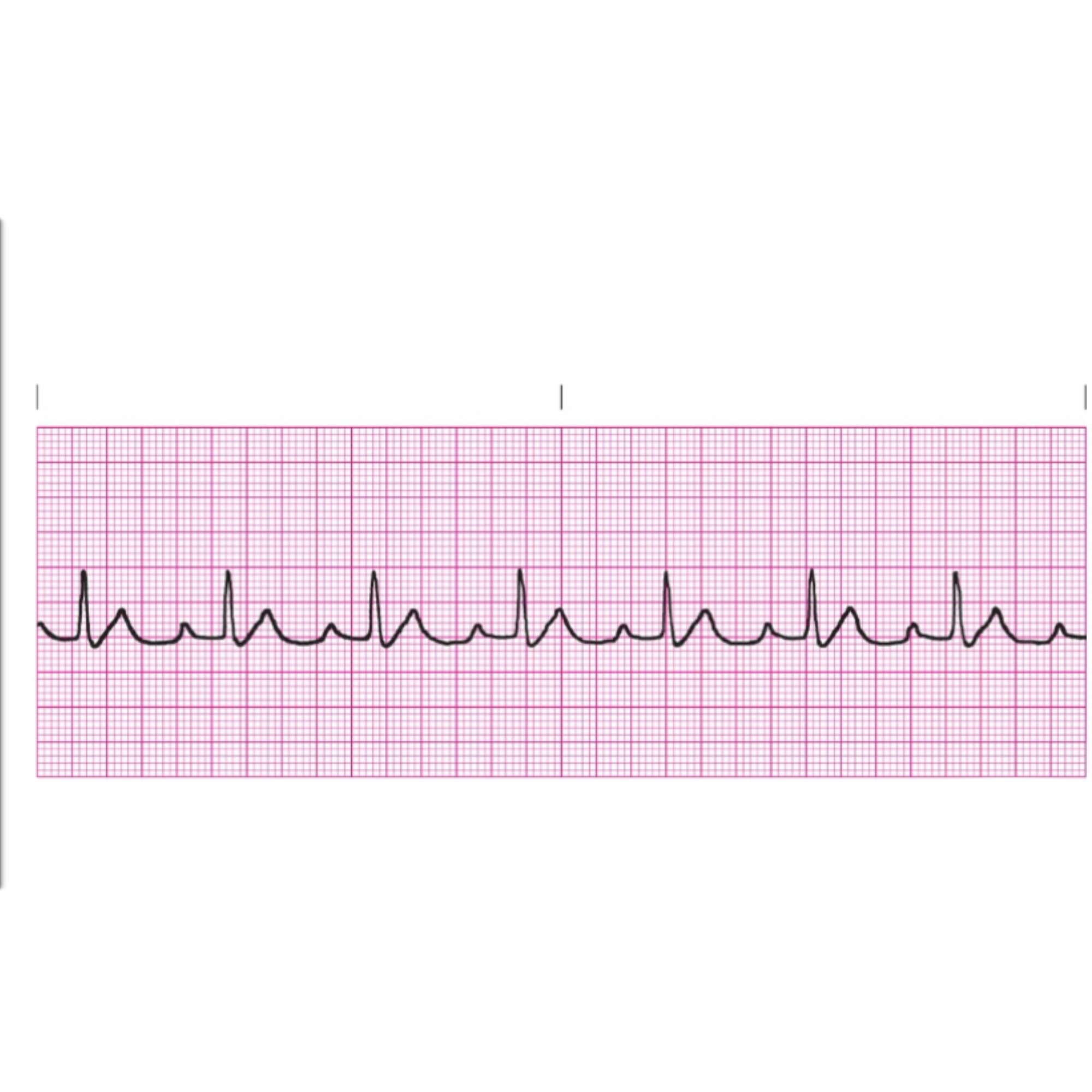
Mechanism of Atrial Tachycardia includes
the pacemaker is a single irritable site within the atrium that fires repetitively at a very rapid rate. Conduction through to the ventricles is normal
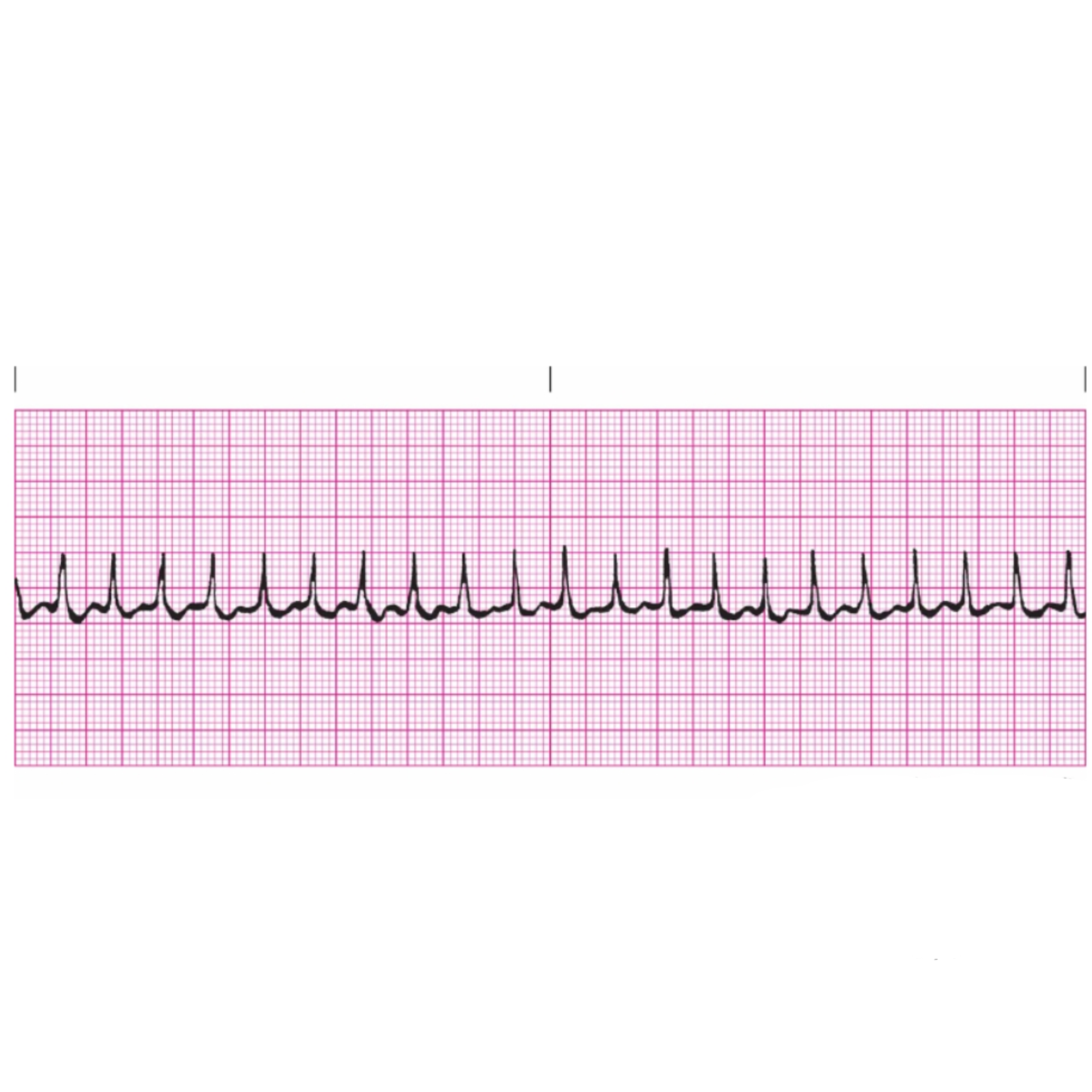
Rules for Atrial Tachycardia includes
Regularity: Regular
Rate: 150–250 bpm
P Wave: Atrial P wave; differs from sinus P wave; can be lost in T wave
PRI: 0.12–0.20 second
QRS: Less than 0.12 second
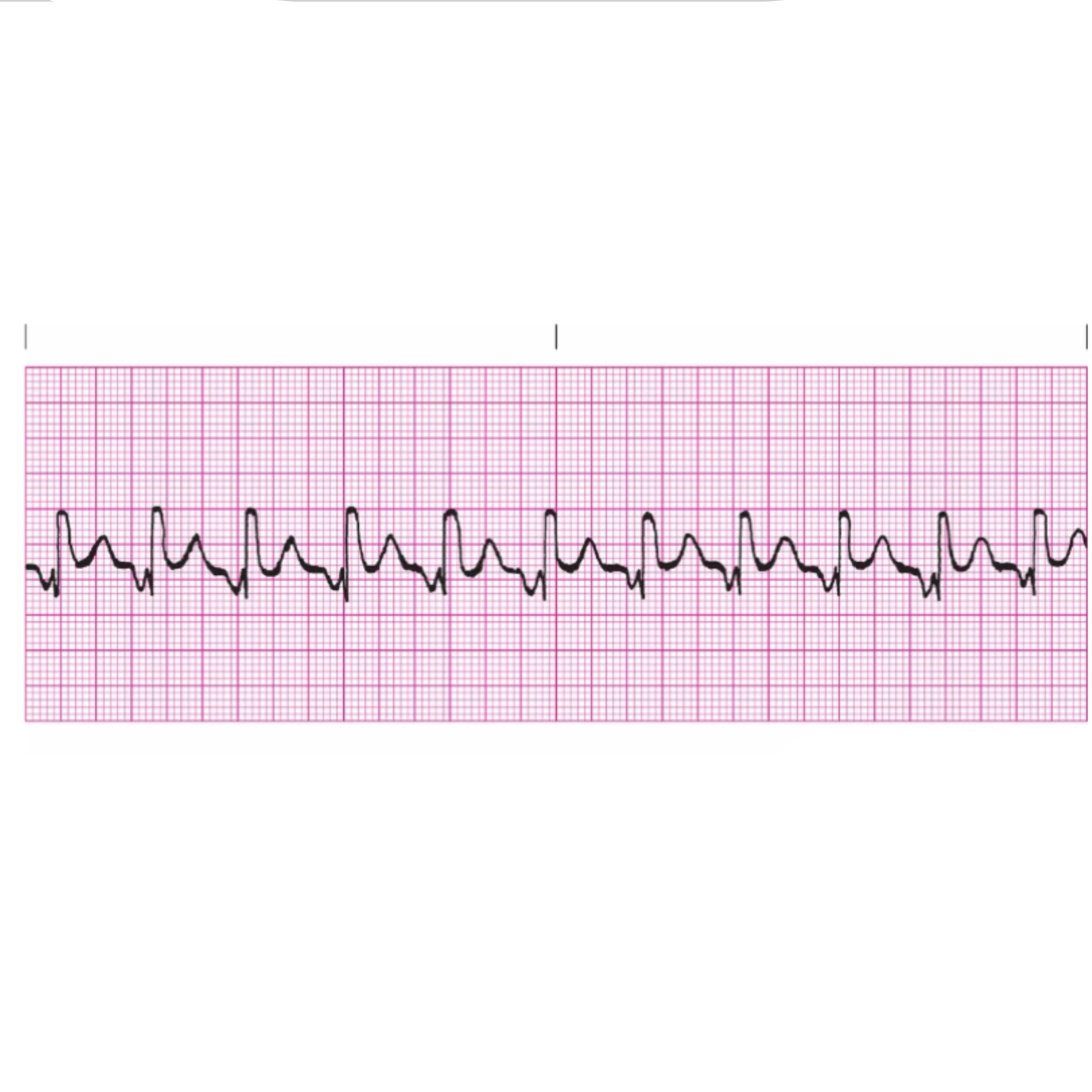
Mechanism of Atrial Flutter includes
a single irritable focus within the atria issues an impulse that is conducted in a rapid, repetitive fashion. To protect the ventricles from receiving too many impulses, the AV node blocks some of the impulses from being conducted through to the ventricles. Those that do get through are conducted normally
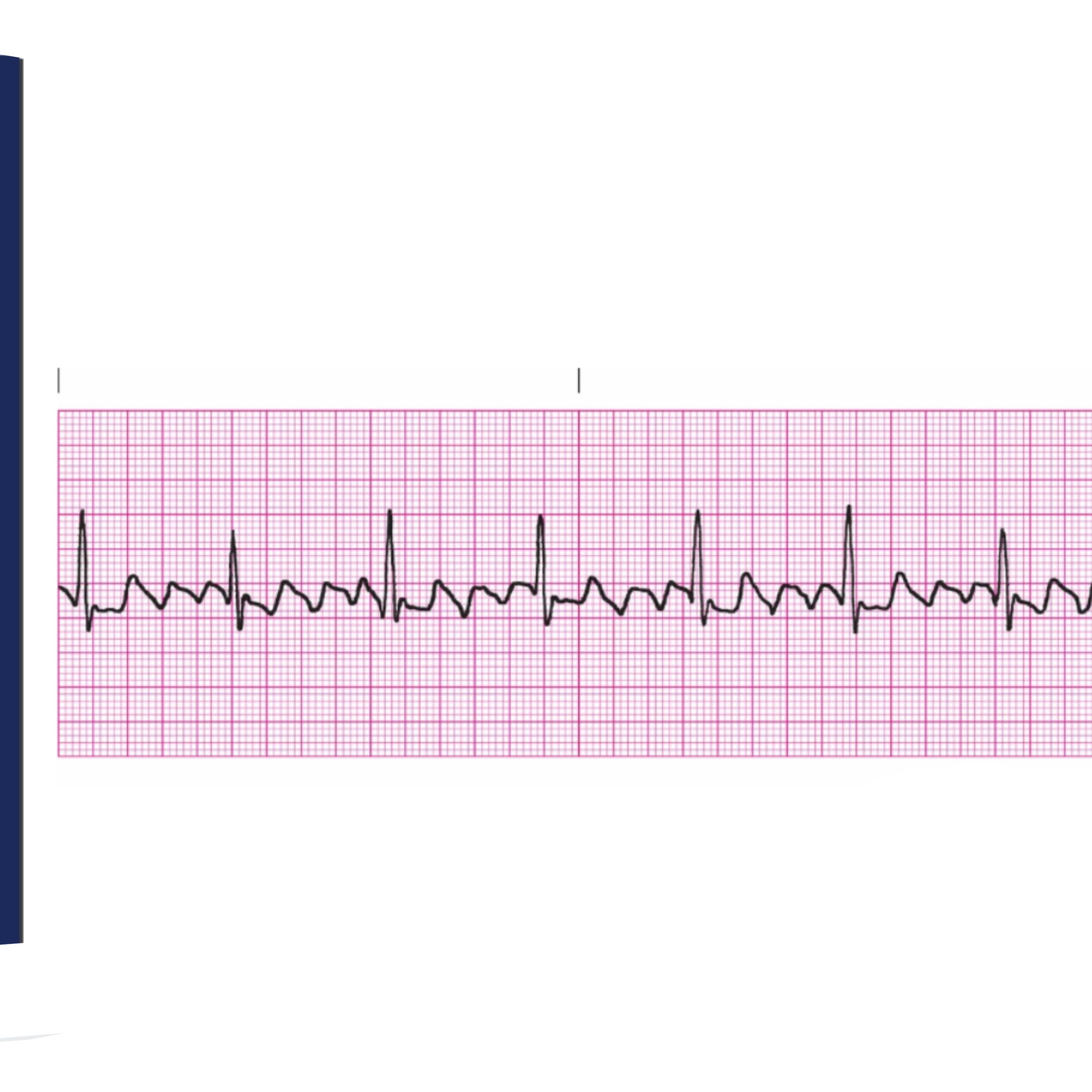
Rules for Atrial Flutter includes
Regularity: Atrial rhythm is regular; ventricular rhythm is usually regular but can be irregular if there is variable block
Rate: Atrial rate 250–350 bpm; ventricular rate varies
P Wave: Characteristic sawtooth pattern
PRI: Unable to determine
QRS: Less than 0.12 second
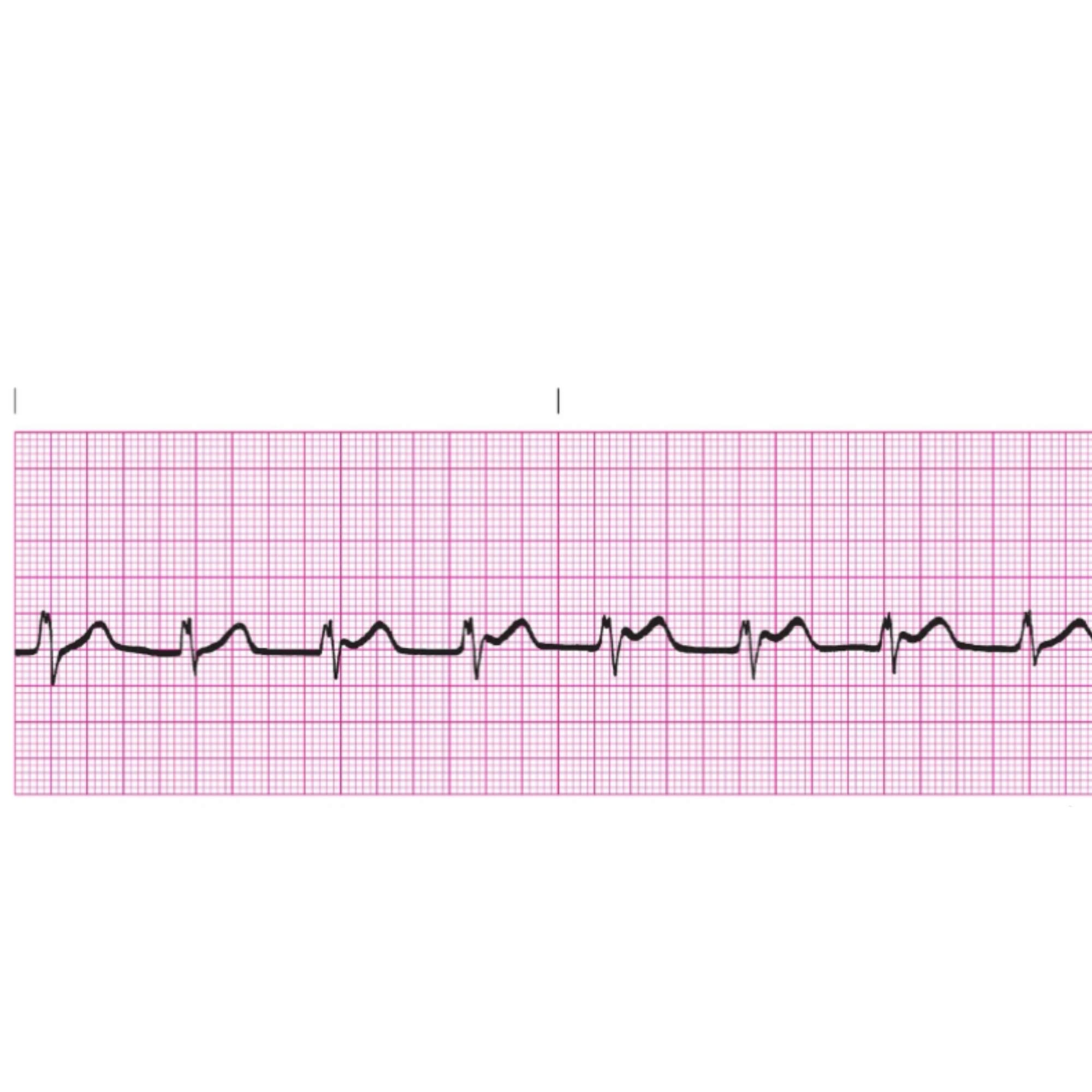
Mechanism of Atrial Fibrillation includes
the atria are so irritable that a multitude of foci initiate impulses, causing the atria to depolarize repeatedly in a fibrillatory manner. The AV node blocks most of the impulses, allowing only a limited number through to the ventricles.

Rules for Atrial Fibrillation includes
Regularity: Grossly irregular
Rate: Atrial rate greater than 350 bpm; ventricular rate varies greatly
P Wave: No discernible P waves; atrial activity is referred to as fibrillatory waves (f waves)
PRI: Unable to measure
QRS: Less than 0.12 second
Inverted P Wave includes
The P wave precedes the QRS complex if the atria are depolarized before the ventricles. In this case, the PRI will be less than 0.12 seconds
Inverted P Wave (Hidden) is if the
Atria and the ventricles are depolarized simultaneously, there will be no visible P wave, since it is hidden within the QRS complex
In the a inverted P wave, the P wave will
Follow the QRS complex if the ventricles are depolarized before the atria
Mechanism of Premature Junctional Complex includes
the pacemaker is an irritable focus within the AV junction that fires prematurely and produces a single ectopic beat. The atria are depolarized via retrograde conduction. Conduction through the ventricles is normal. This is a single beat, not an entire rhythm; the underlying rhythm also must be identified
Rules for Premature Junctional Complex includes
Regularity: Depends on regularity of underlying arrhythmia
Rate: Depends on rate of underlying arrhythmia
P Wave: Will be inverted; can fall before, during, or after the QRS complex
PRI: Can be measured only if the P wave precedes the QRS complex; if measurable, will be less than 0.12 second
QRS: Less than 0.12 second
Mechanism of Junctional Escape Rhythm includes
when higher pacemaker sites fail, the AV junction is left with pacemaking responsibility. The atria are depolarized via retrograde conduction. Conduction through the ventricles is normal

Rules for Junctional Escape Rhythm includes
Regularity: Regular
Rate: 40–60 bpm
P Wave: Will be inverted: can fall before or after the QRS complex or can be hidden within the QRS complex
PRI: Can be measured only if the P wave precedes the QRS complex; if measurable, will be less than 0.12 second
QRS: Less than 0.12 second
Mechanism of Accelerated Junctional Rhythm includes
an irritable focus in the AV junction speeds up to override the SA node for control of the heart. The atria are depolarized via retrograde conduction. Conduction through the ventricles is normal
Rules for Accelerated Junctional Rhythm includes
Regularity: regular
Rate: 60–100 bpm
P Wave: will be inverted; can fall before or after the QRS complex or can be hidden within the QRS complex
PRI: can be measured only if the P wave precedes the QRS complex; if measurable, will be less than 0.12 second
QRS: less than 0.12 second
Mechanism of Junctional Tachycardia includes
A very rapid irritable focus in the AV junction overrides the SA node for control of the heart. The atria are depolarized via retrograde conduction. Conduction through the ventricles is normal
Rules for Junctional Tachycardia includes
Regularity: Regular
Rate: 100–180 bpm
P Wave: Will be inverted; can fall before or after the QRS complex or can be hidden within the QRS complex
PRI: Can be measured only if the P wave precedes the QRS complex; if measurable, will be less than 0.12 second
QRS: Less than 0.12 second
Supraventricular Tachycardia is a phrase used to describe a-
rapid, regular supraventricular arrhythmia when more accurate identification is impossible because P waves aren’t visible and rate is common to other arrhythmias
SVTs with Overlapping Rate Ranges:
Sinus Tachycardia
Atrial Tachycardia
Atrial Flutter
Junctional Tachycardia
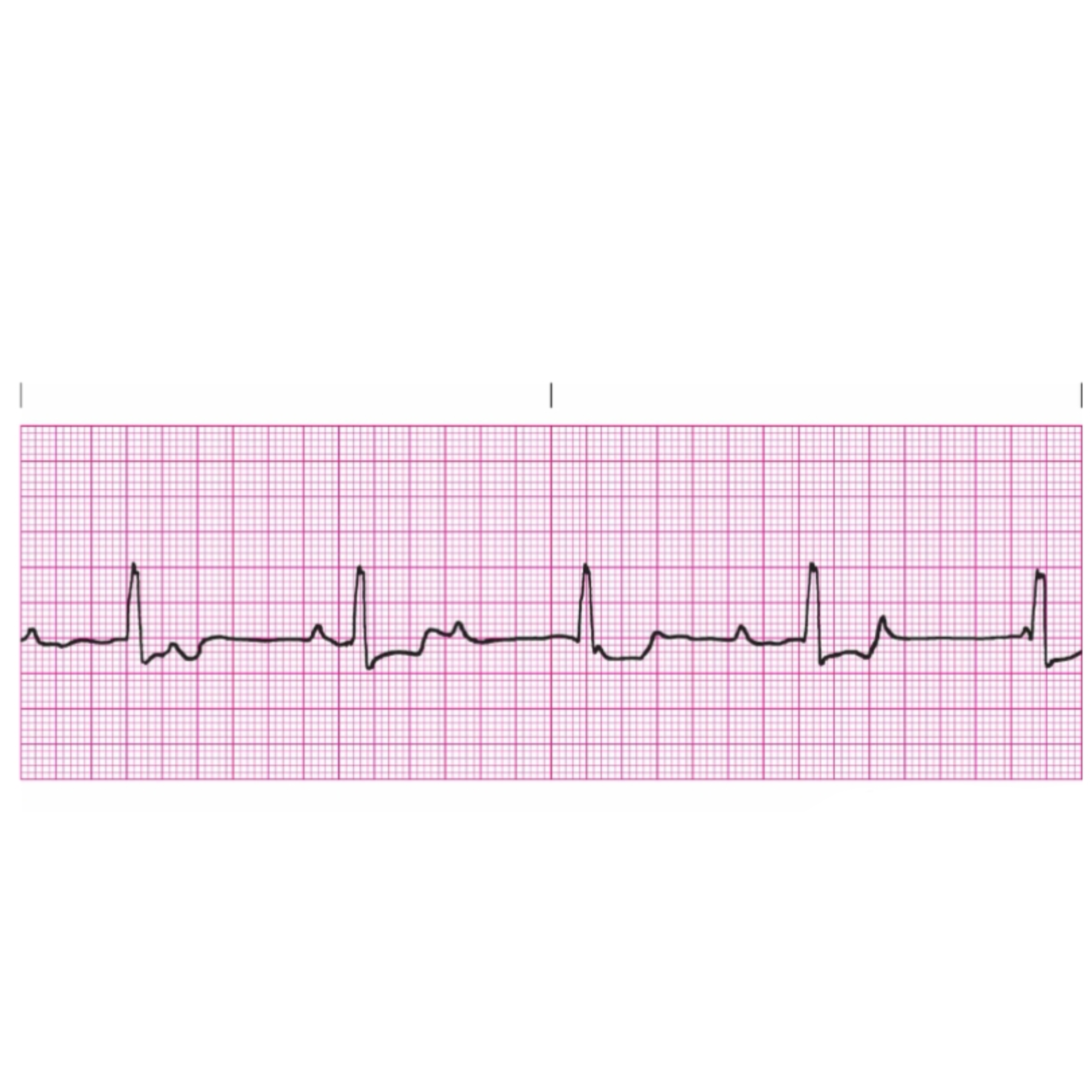
Mechanism of First Degree Heart Block includes
AV node holds each impulse longer than normal before conducting it to the ventricles. Each impulse is eventually conducted
Rules for First Degree Heart Block
Regularity: Depends on underlying rhythm
Rate: Depends on underlying rhythm
P Wave: Upright and uniform; each P wave will be followed by a QRS complex
PRI: Greater than .20 seconds; constant across strip
QRS: Less than .12 seconds
Mechanism of Type II Second Degree Heart Block including
The AV node selectively conducts some beats while blocking others. Those that are not blocked are conducted through to the ventricles, although they may encounter a slight delay in the node. Once in the ventricles, conduction proceeds normally
Rules for Type II Second Degree Heart Block includes
Regularity: If the conduction ratio is consistent, the R–R interval will be constant, and the rhythm will be regular. If the conduction ratio varies, the R–R will be irregular
Rate: The atrial rate is usually normal (60–100 bpm). Since many of the atrial impulses are blocked, the ventricular rate will usually be in the bradycardia range (< 60 bpm), often one-half, one-third, or one-fourth of the atrial rate
P Waves: P waves are upright and uniform. There are always more P waves than QRS complexes
PRI: The PRI on conducted beats will be constant across the strip, although it might be longer than a normal PRI measurement
QRS: The QRS complex measurement will be less than 0.12 second
Mechanism of Wenckebach (Type I Second-Degree Heart Block) are
As the sinus node initiates impulses, each one is delayed in the AV node a little longer than the preceding one, until one impulse is eventually blocked completely. Those impulses that are conducted travel normally through the ventricles
Rules for Wenckebach
Regularity: Irregular; R-R interval changes as PR interval gets longer; characteristic grouped beating
Rate: Usually slightly slower than normal
P Wave: Upright and uniform; some P waves not followed by QRS complexes
PRI: Progressively lengthens until one P wave is not conducted
QRS: Less than .12 seconds
Mechanism of Complete Heart Block (CHB) includes
The block at the AV node is complete. The sinus beats cannot penetrate the node and thus are not conducted through to the ventricles. An escape mechanism from either the junction or the ventricles will take over to pace the ventricles. The atria and ventricles function in a totally dissociated fashion
Rules for Complete Heart Block
Regularity: Regular
Rate: AR—usually normal (60–100 bpm) VR—40–60 if focus is junctional; 20–40 if focus is ventricular
P Waves: Upright and uniform; more P waves than QRS complexes
PRI: No relationship between P waves and QRS complexes; P waves can occasionally be found superimposed on the QRS complex
QRS: Less than 0.12 second if focus is junctional; 0.12 second or greater if focus is ventricular
Mechanism of Premature Ventricular Complex includes
A single irritable focus within the ventricles that fires prematurely to initiate an ectopic complex. This is a single beat, not an entire rhythm; the underlying rhythm also must be identified
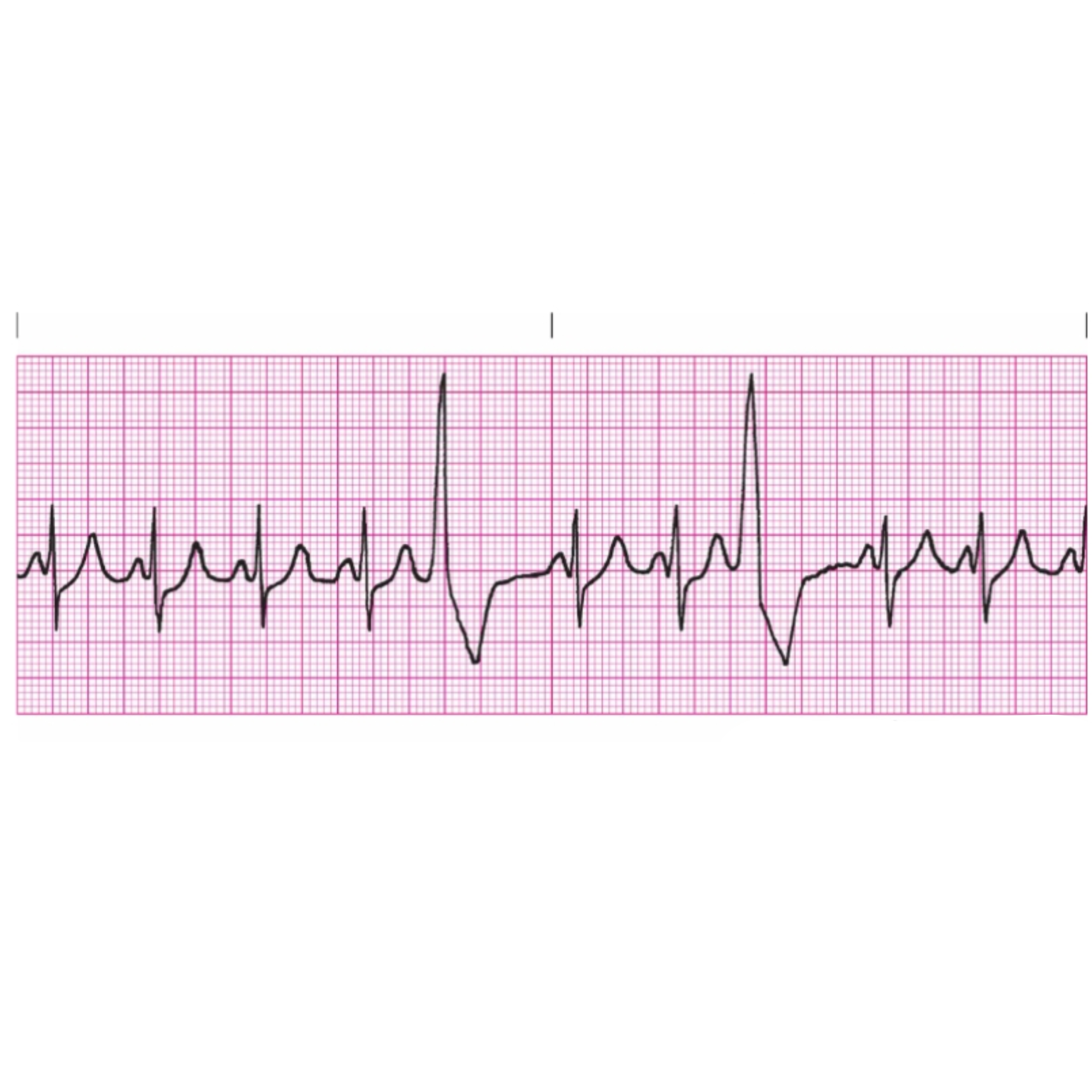
Rules for Premature Ventricular Complex includes
Regularity: Ectopics will disrupt regularity of underlying rhythm
Rate: Depends on underlying rhythm and number of ectopics
P Waves: Will not be preceded by a P wave; dissociated P wave may be seen near PVC
PRI: Since the ectopic comes from a lower focus, there will be no PRI
QRS: Wide and bizarre; 0.12 seconds or greater; T wave is usually in opposite direction from R wave
Ectopic A exhibits R on T phenomenon;
Ectopic B
does not
Mechanism of Ventricular Tachycardia includes
An irritable focus within the ventricles fires regularly at a rapid rate to override higher sites for control of the heart
Rules for Ventricular Tachycardia includes
Regularity: Usually regular; can be slightly irregular
Rate: 150–250 bpm; can exceed 250 bpm if the rhythm progresses to Ventricular Flutter; may occasionally be slower than 150 bpm, in which case it is called slow VT
P Waves: Will not be preceded by P waves; dissociated P waves may be seen
PRI: Since the focus is in the ventricles, there will be no PRI
QRS: Wide and bizarre; 0.12 second or greater; T wave is usually in opposite direction from R wave
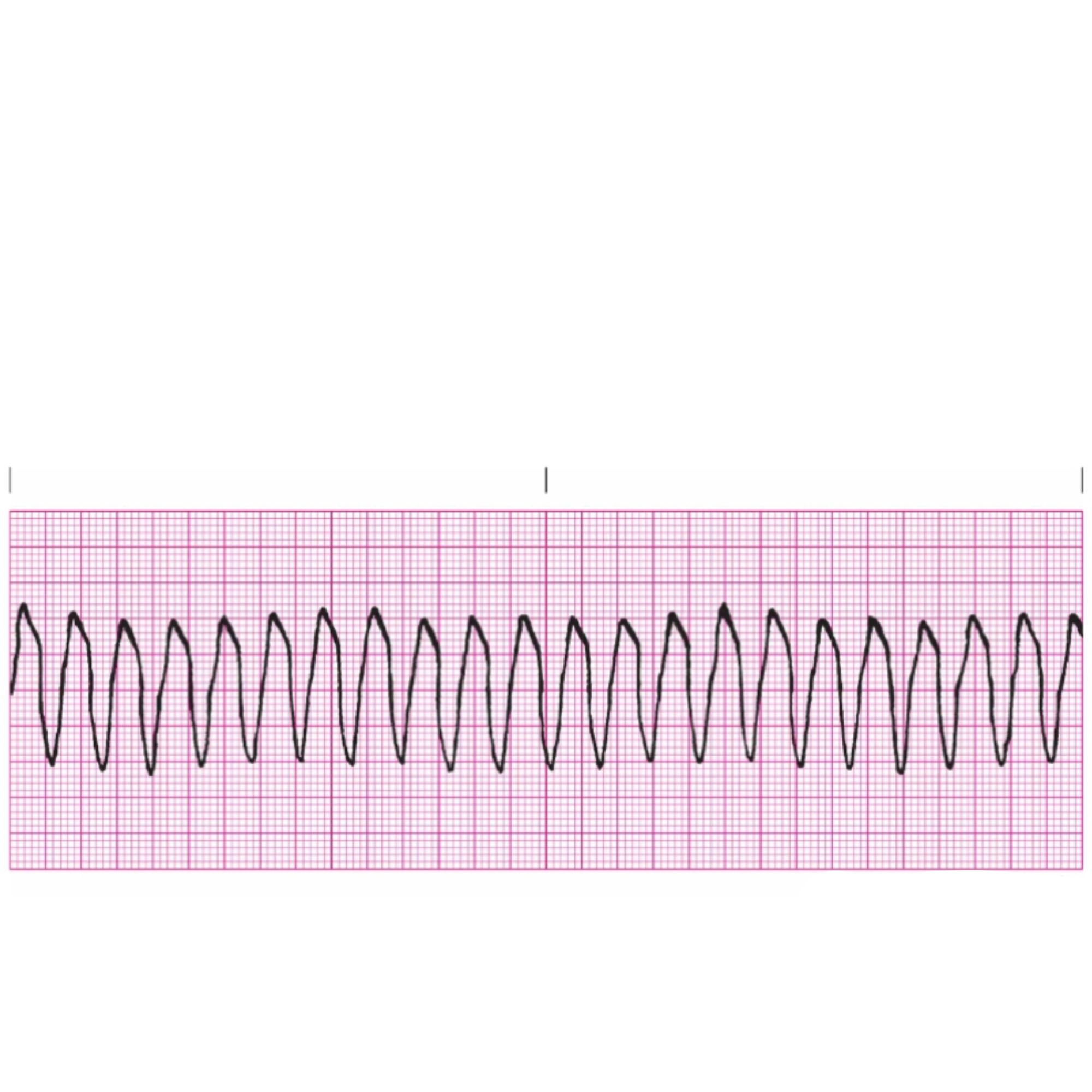
Mechanism of Ventricular Fibrillation includes
Multiple foci within the ventricles become irritable and generate uncoordinated, chaotic impulses that cause the heart to fibrillate rather than contract

Rules for Ventricular Fibrillation
Everything is totally chaotic with no discernible waves or complexes
Mechanism of Idioventricular Rhythm includes
In the absence of a higher pacemaker, the ventricles initiate a regular impulse at their inherent rate to take control of the heart
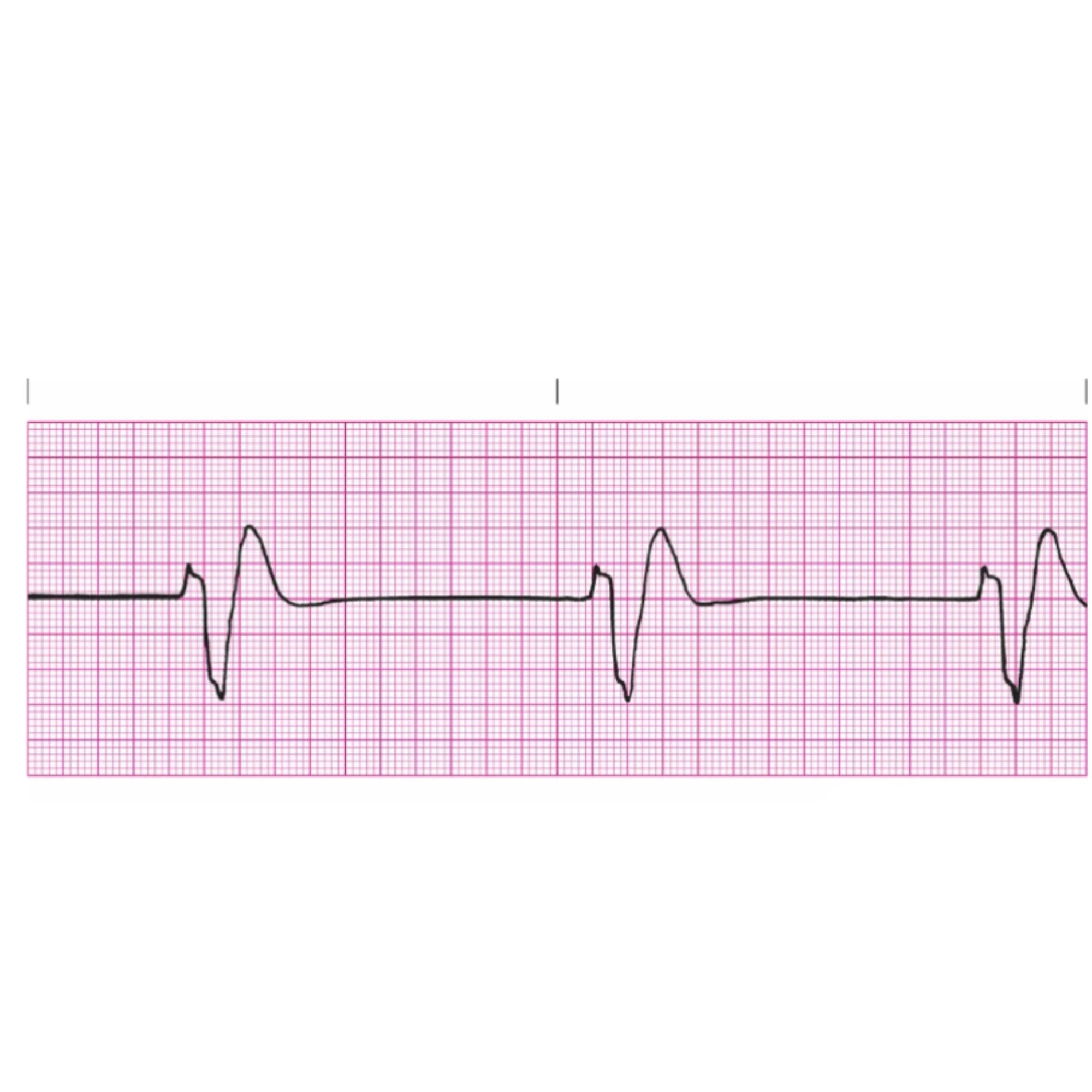
Rules for Idioventricular Rhythm
Regularity: usually regular
Rate: 20–40 bpm; can drop below 20 bpm
P Waves: none
PRI: none
QRS: Wide and bizarre; 0.12 seconds or more
Mechanism of Asystole includes
The heart has lost its electrical activity. There is no electrical pacemaker to initiate electrical flow
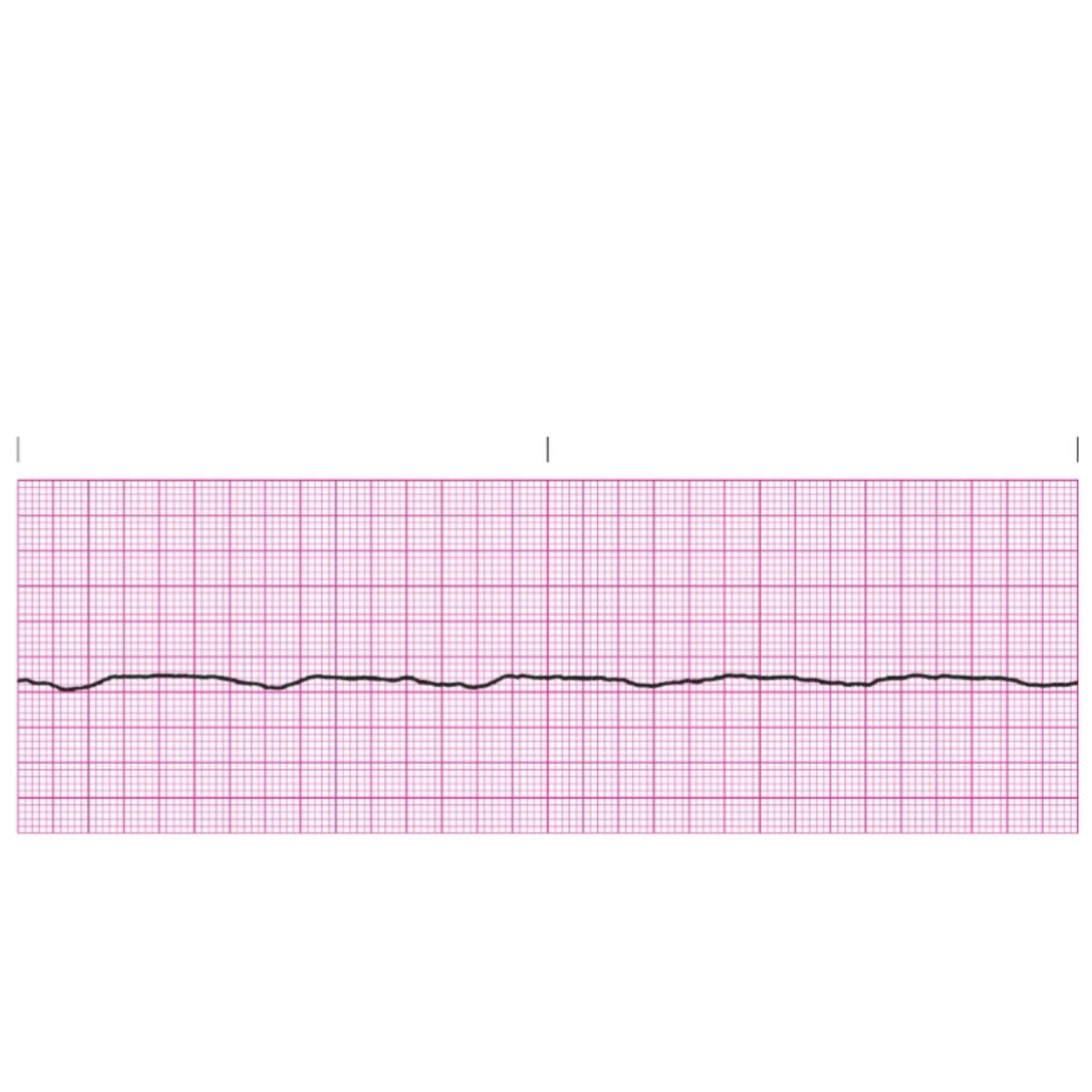
Rules for Asystole includes
Everything being a straight line indicates no electrical activity
Epinephrine is administered first
during resuscitation with asystole
Atropine and Epinephrine can be given
IV and via ETT
ACLS recommended dosage for Adenosine is
6 mg rapid IVP follow with 20 ml flush
ACLS recommended dosage for epinephrine is:
1mg IV/ET every 3-5 minutes
Epinephrine is given for
pulseless Vtach
Racemic epinephrine for
stridor
Polysomnography is the
the study of sleep. This is the testing used to diagnose sleep disorders.
To meet the definitive criteria for sleep apnea there needs to be
10 seconds of air flow cessation during sleep
must be documented
The first sign of sleep disordered breathing is
Snoring
What rhythms do you shock
Ventricular Fibrillation and Ventricular Tachycardia
What rhythms do you cardiovert
Ventricular Tachycardia (VT)
Atrial Fibrillation
Atrial Flutter
Supraventricular Tachycardia (SVT)
Atrial Fibrillation may cause or lead
to CHF
When would you have a dull percussion note
Pneumonia
Pleural effusion
Atelectasis
Tumor
When would you have a hyper-resonant percussion note
Pneumothorax
Emphysema / COPD
What is leukopenia
an abnormally low number of white blood cells (WBCs) in the blood, typically defined as falling below <4,000 cells per microliter
What is leukocytosis
an elevated white blood cell (WBC) count in the blood
What is a normal WBC
4,000 to 11,000 cells per microliter (mcL) of blood
Patients receiving corticosteroids are at risk for thrush- also called oral candida. Which medications contain these corticosteroids
Budesonide
Fluticasone
Beclomethasone
Ciclesonide
The affinity between carbon monoxide and hemoglobin is
240 times stronger than the affinity between hemoglobin and oxygen
According to the O₂Hb-dissociation curve, under normal conditions,
a PaO₂ of 60 mm Hg correlates to an SpO₂ of 90%
Calculate minute ventilation
Minute ventilation (VE)= Tidal volume (VT) × Respiratory rate (RR)
ETCO2 is measured at the peak of the curve on
the capnography tracing
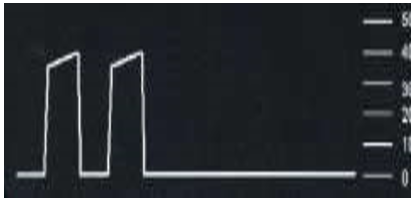
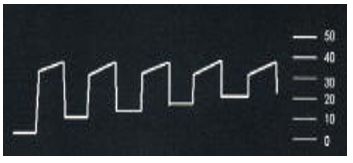
What is this ETCO2 waveform
Dislodged tube
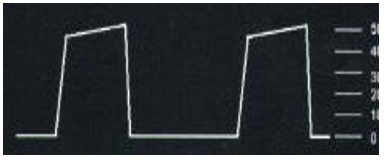
What is this ETCO2 waveform
rebreathing CO2
What is this ETCO2 waveform
Hypoventilation
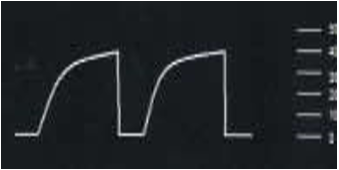
What is this ETCO2 waveform
bronchospasm
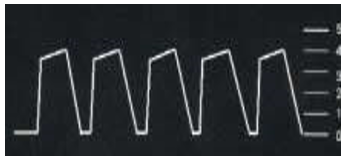
What is this ETCO2 waveform
Patient breathing around ET tube
In Junctional Rhythms, if conduction to the atria occurs simultaneously with conduction to the ventricles, the p waves will be
inverted, and lost within the QRS complex