Increased ICP
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Altered Level of Consciousness (LOC)
when a patient is not oriented, does not follow commands, or needs persistent stimuli to achieve a state of alertness
Alert → Confused → Lethargic → Obtunded → Stuporous → Comatose
Usual continuum of LOC:
Confused
LOC where the patient is awake but disoriented or slow to understand
Lethargic
LOC where the patient is drowsy, easily aroused, answers but may fall asleep again
Obtunded
LOC where the patient is very sleepy, difficult to arouse, responds slowly
Stuporous
LOC where the patient only responds to strong or painful stimuli
Comatose
LOC where the patient does not respond even to painful stimuli
Akinetic mutism
unresponsiveness to the environment; the patient makes no movement or sound but sometimes opens the eyes
Persistent vegetative state
a type of coma in which the patient exhibits alternating sleep and wake cycles. Cortical functioning ceases while brainstem activity continues
Locked-in syndrome
Condition in which a patient is aware and awake but cannot move or communicate verbally because of complete paralysis of nearly all voluntary muscles except the eyes.
Neurologic, Toxicologic, or Metabolic
Causes of Altered LOC
restlessness or increased anxiety
Early signs of Altered LOC
Brain injury and Brainstem damage
What conditions can cause severe hyperthermia
Care of the Unconscious Patient
Hydration: turgor, mucosa, I&O, labs
Fluids: give slowly, may restrict to prevent ICP/cerebral edema
Nutrition: start early enteral feeding within 48 hrs
Oral care: keep mouth clean/moist, petrolatum on lips
Intubated: move ET tube daily, chlorhexidine for VAP prevention
Skin care: turn frequently, avoid dragging, check pressure areas
Positioning: proper alignment, foam boots/splints prevent foot drop
ROM: passive ROM prevents contractures
Eye care: saline cleanse, artificial tears, eye shield
Hyperthermia: fever may mean infection/brain damage/dehydration. increases brain metabolism, worsens prognosis
Temp route: do not take orally
the neurocranium, the sutures, and the facial skeleton.
The skull contains three main components:
Normal ICP is usually 0-10 mm Hg.
15 mm Hg is considered the upper limit of normal.
What is the normal ICP and what is considered the upper limit of normal
Monro-Kellie Doctrine
The skull is a rigid closed space, so if one component increases, another must decrease. To compensate for rising volume, the body may:
Shift CSF
Increase CSF absorption
Decrease CSF production
Reduce cerebral blood volume
If compensation fails, ICP rises.
Lowers cerebral perfusion
Worsens cerebral edema
Can cause brain herniation, which is often fatal
Why is high ICP dangerous
Rising blood pressure
Slow, bounding pulse
Irregular respirations
Early signs of reduced cerebral blood flow to the brain
Cerebral edema
swelling from the inflammatory response, may compress and kill brain tissue. As swelling increases, the brain tries to compensate through Autoregulation or Reduced CSF production and flow
Autoregulation
means the brain adjusts blood vessel diameter to keep blood flow stable, but this can fail when ICP remains high.
Cerebral Perfusion Pressure (CPP)
CPP = MAP - ICP
70-100 mm Hg.
normal CPP that should be maintained for adequate brain perfusion
<50 mmHg
Irreversible neurologic damage can occur when CPP falls below what level
cerebral circulation stops.
what happens when ICP = MAP
Mean Arterial Pressure (MAP)
(SBP + 2DBP)/3. the average pressure in a person's arteries during a single cardiac cycle and is considered a key indicator of organ perfusion
60 mmHg
What MAP is essential to ensure enough blood flow to vital organs. A drop below this threshold for an extended period can lead to ischemia and organ failure.
70-100 mmHg
A normal MAP range
Cushing's Response / Cushing's Reflex
When brain blood flow drops a lot, the body tries to compensate by increasing arterial pressure. This causes Increased systolic blood pressure, Widened pulse pressure, and Slowing of heart rate. This is a late sign of increased ICP and needs immediate treatment.
Cushing's Triad
.the clinical manifestation—the specific set of symptoms (hypertension, bradycardia, and irregular respirations) caused by this reflex. A serious, grave sign of worsening ICP.
Brain Herniation
when the brain becomes compressed and forced into another region
Early clinical signs of Increased ICP
Agitation
Restlessness without obvious cause
Slowing of speech
Delayed response to verbal stimuli
Confusion
Increasing drowsiness
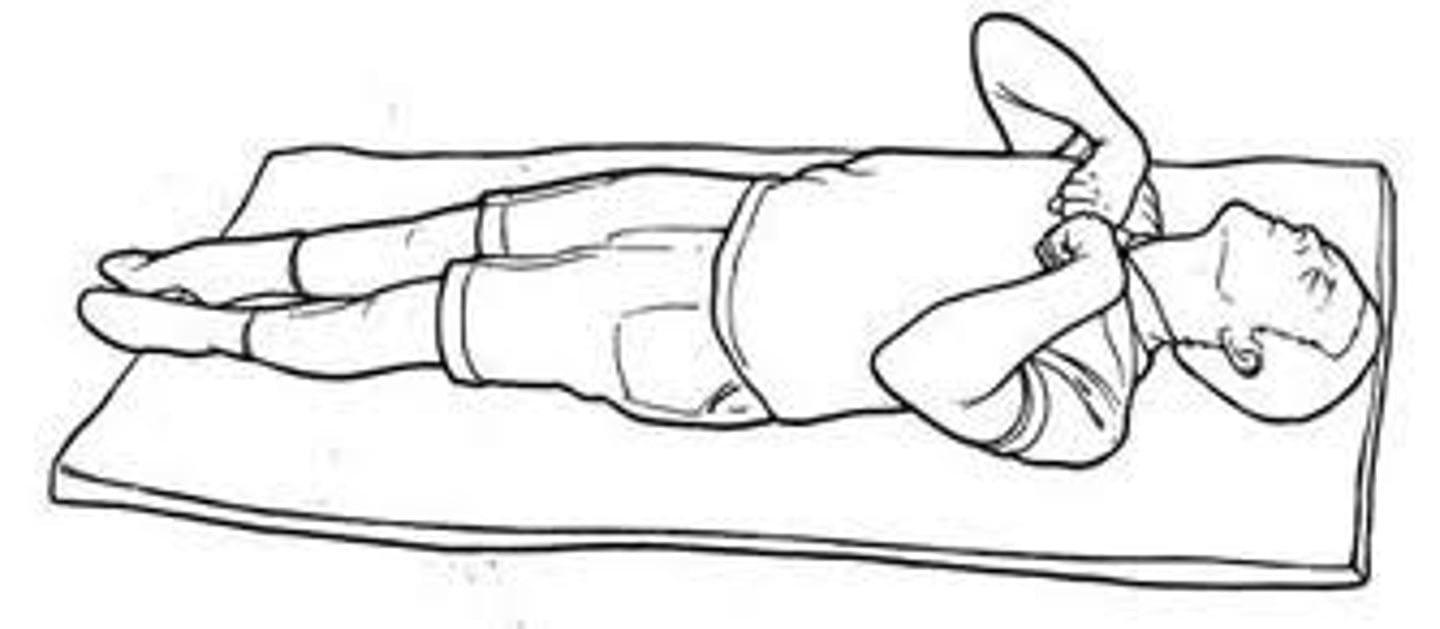
Decorticate posturing
Abnormal flexion of upper extremities. Extension of lower extremities. Indicates severe damage above the brain stem usually involving the cerebral hemispheres
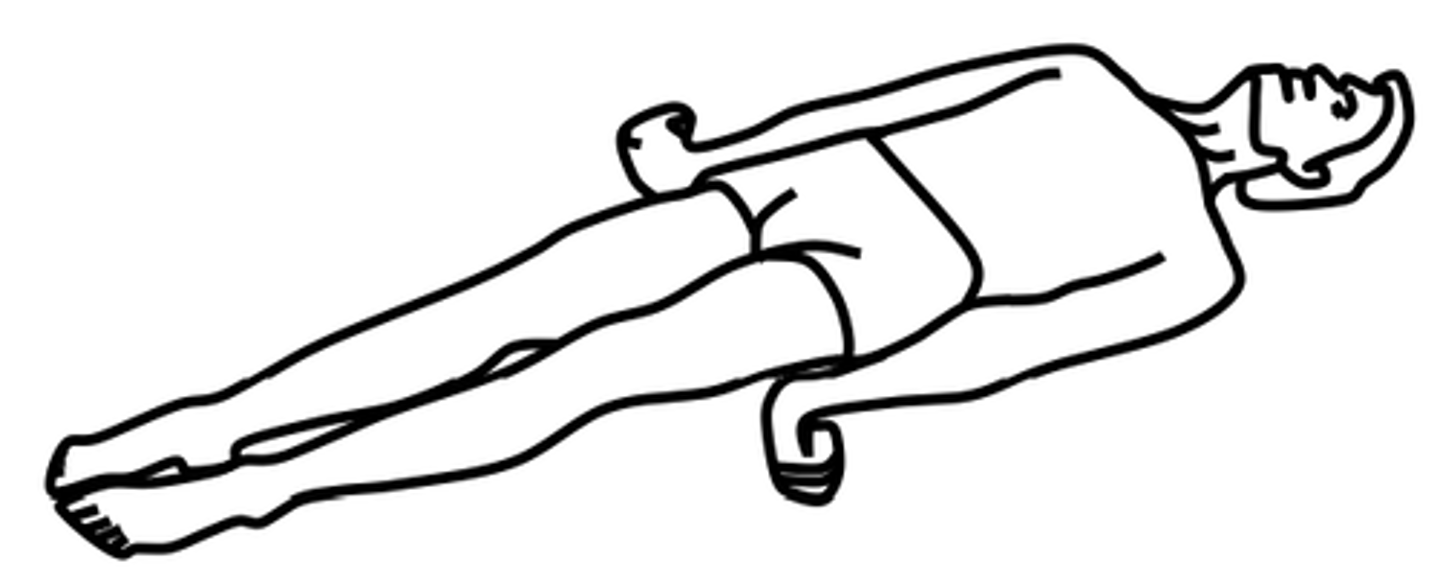
Decerebrate posturing
Extreme extension of both upper and lower extremities. More serious and Often indicates dysfunction at the brain stem level
Sudden release of pressure in the lumbar region can trigger brain herniation
Why is Lumbar puncture is avoided in patients with increased ICP
Brain Stem Herniation
Occurs when ICP rises excessively and pressure within the cranial vault forces brain tissue downward onto the brain stem. Can lead to Irreversible brain anoxia and Brain death
Brainstem herniation, Neurogenic DI, SIADH
Complications of Increased ICP
Neurogenic Diabetes Insipidus
↑ ICP → compression/damage to hypothalamus or posterior pituitary resulting in extreme thirst and high volumes of dilute urine. It is managed primarily with desmopressin (dDAVP).
SIADH
↑ ICP → irritation/stimulation of hypothalamus/pituitary resulting in increased secretion of ADH causing water retention and low blood sodium levels (hyponatremia)
Intraventricular catheter (ventriculostomy)/ External ventricular drain
A fine-bore catheter is inserted into a lateral ventricle, preferably in the nondominant hemisphere of the brain. It is connected through a fluid-filled system to a transducer that converts pressure into an electrical signal for continuous monitoring. it allows Continuous ICP monitoring, Drainage of CSF during acute pressure increases, Drainage of blood from the ventricle, Intraventricular medication administration, Occasional instillation of air or contrast agent for ventriculography. Can be diagnostic or therapeutic
Subarachnoid Screw / Bolt
A hollow screw or bolt is inserted through the skull and dura into the subarachnoid space. It is connected to a pressure transducer, and the output is displayed on an oscilloscope. Does not require ventricular puncture. Avoids complications related to Brain shift, or Small ventricle size. Can cause blockage by clot or brain tissue which can cause loss of pressure tracing and Decreased accuracy, especially at high ICP readings
Epidural Monitor
uses a pneumatic flow sensor to detect ICP. Low incidence of infection, Fewer complications, Appears to measure pressure accurately, Automatic calibration, Alarm system for abnormal pressure waves. Cannot withdraw CSF for analysis. This is safer in some ways, but it lacks the therapeutic and diagnostic flexibility of ventricular access.
Fiberoptic Monitor / Transducer-Tipped Catheter
A miniature transducer at the catheter tip detects pressure changes, which are converted into electrical signals and displayed on a digital monitor. If inserted into the ventricle, it may also be used with a CSF drainage device. This is a flexible alternative to other monitoring systems.
A miniature transducer at the catheter tip detects pressure changes, which are converted into electrical signals and displayed on a digital monitor.
Possible sites of insertion with a transducer-tipped catheter
Interpreting Intracranial Pressure Waveforms
ICP monitoring does not only involve a number; it also includes waveform interpretation. Pressure waveforms are recorded on an oscilloscope and classified into:
A waves (plateau waves)
B waves
C waves
A Waves (Plateau Waves)
are very important because they indicate changes in vascular volume inside the intracranial compartment that are starting to compromise cerebral perfusion. Transient, Paroxysmal, Recurring elevations of ICP that Last 5 to 20 minutes, Amplitude ranges from 40 to 100 mm Hg. Increase in amplitude and frequency may reflect cerebral ischemia and brain damage.
B waves
Less significant than A waves But if they occur in a series in a patient with depressed consciousness, they may precede A waves.
Duration: 30 seconds to 2 minutes
Smaller amplitude: up to 50 mm Hg
Seen in intracranial hypertension and decreased intracranial compliance.
C Waves
Small rhythmic oscillations Frequency: 4 to 8 per minute. Appear related to rhythmic changes in Systemic arterial blood pressure and Respirations
Mannitol
Hypertonic saline (3%)
osmotic diuretics that are commonly used to reduce fluid in brain tissue.
Dexamethasone
Used if the cause of increased ICP is a brain tumor to reduce the edema surrounding the tumor
Decompressive Hemicraniectomy
involves removal of part of the skull so the swollen brain can expand without being compressed by the rigid cranial vault. This is to relieve pressure and help manage severe ICP that does not respond to other treatments
ventricular collapse, and brain herniation
Excessive CSF drainage may cause
Supratentorial craniotomy
Infratentorial craniotomy
Transsphenoidal approach
There are three major approaches for craniotomy
Supratentorial Craniotomy
performed above the tentorium, entering the supratentorial compartment of the skull. Usually involves the cerebral hemispheres or upper brain regions
Infratentorial Craniotomy
performed below the tentorium, often involving the posterior fossa and potentially the brain stem. Often involves the posterior fossa, cerebellum, and the brain stem area
Pseudobulbar affect
disorder involving inappropriate or exaggerated emotional expression, most commonly episodes of laughing or crying. These outbursts are often not consistent with the patient's actual feelings or the situation.
Halo Test
is a medical check for cerebrospinal fluid (CSF) leaking from the ears or nose following a head injury. It works by placing a drop of bloody fluid onto cloth or paper; a clear ring forming around the blood indicates a potential CSF leak, which is a sign of a possible base-of-skull fracture
Elevate head of bed 30-45 degrees. Maintain head in neutral midline position to facilitate venous drainage from the brain and prevent jugular vein compression.
Create a calm, therapeutic environment with dim lighting and minimal noise.
Cluster Care Strategically
Educate patient to avoid coughing, sneezing, straining during bowel movements, or bearing down.
Nursing management for ICP management
Level transducer at the tragus of the ear (Foramen of Monro). Maintain aseptic technique, monitor drainage amount, color, and clarity. Never raise or lower drainage system without physician order
EVD Nursing care & Key responsibilities
Mannitol
Hypertonic Saline (3% NaCl)
Dexamethasone
Phenytoin (Dilantin)
Pharmacologic therapy for Increased ICP