10: Diabetes Lecture (Dr. Schaffhausen)
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
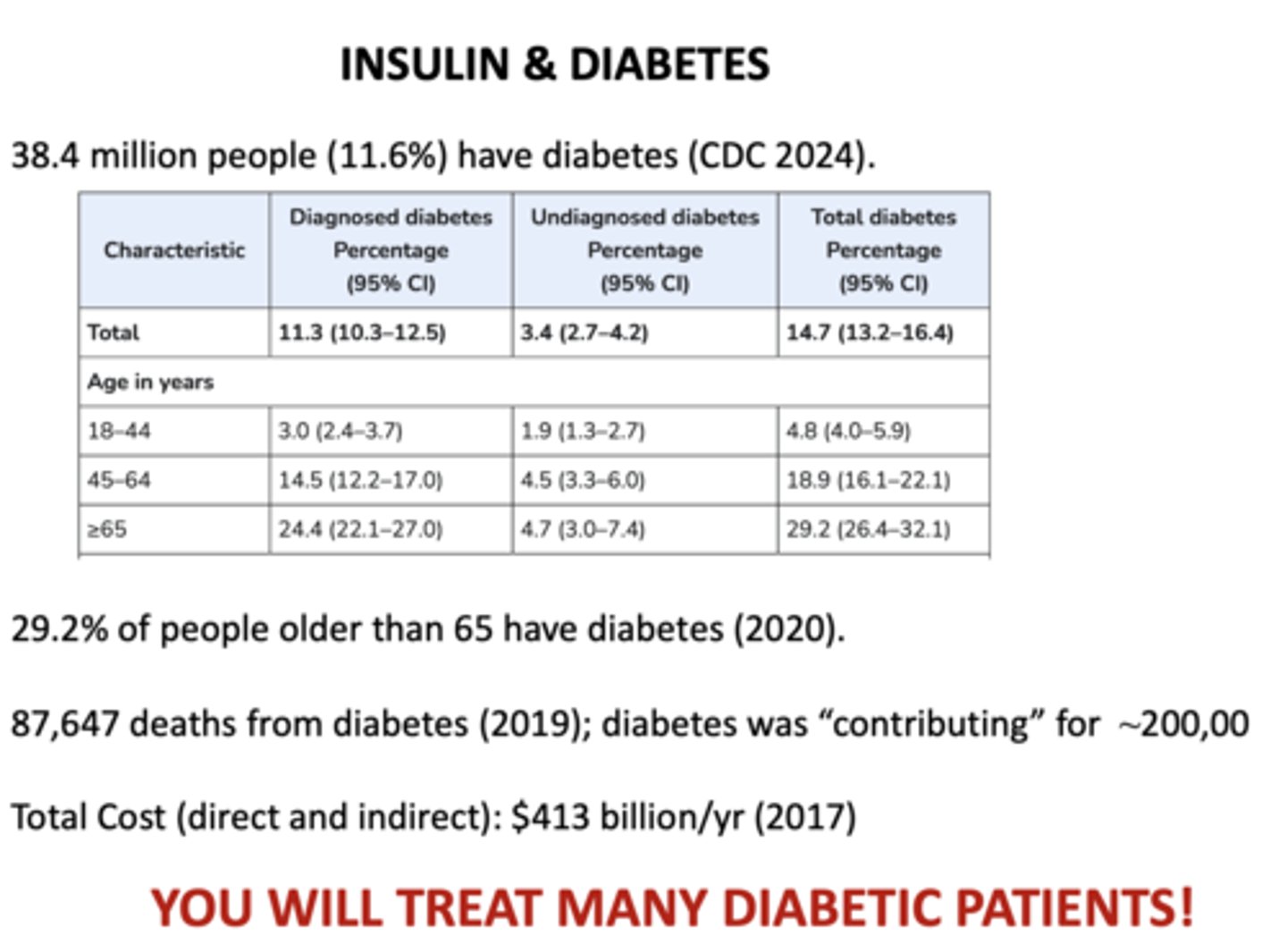
T/F: Dentists do not treat many diabetic patients
False! You will treat many!
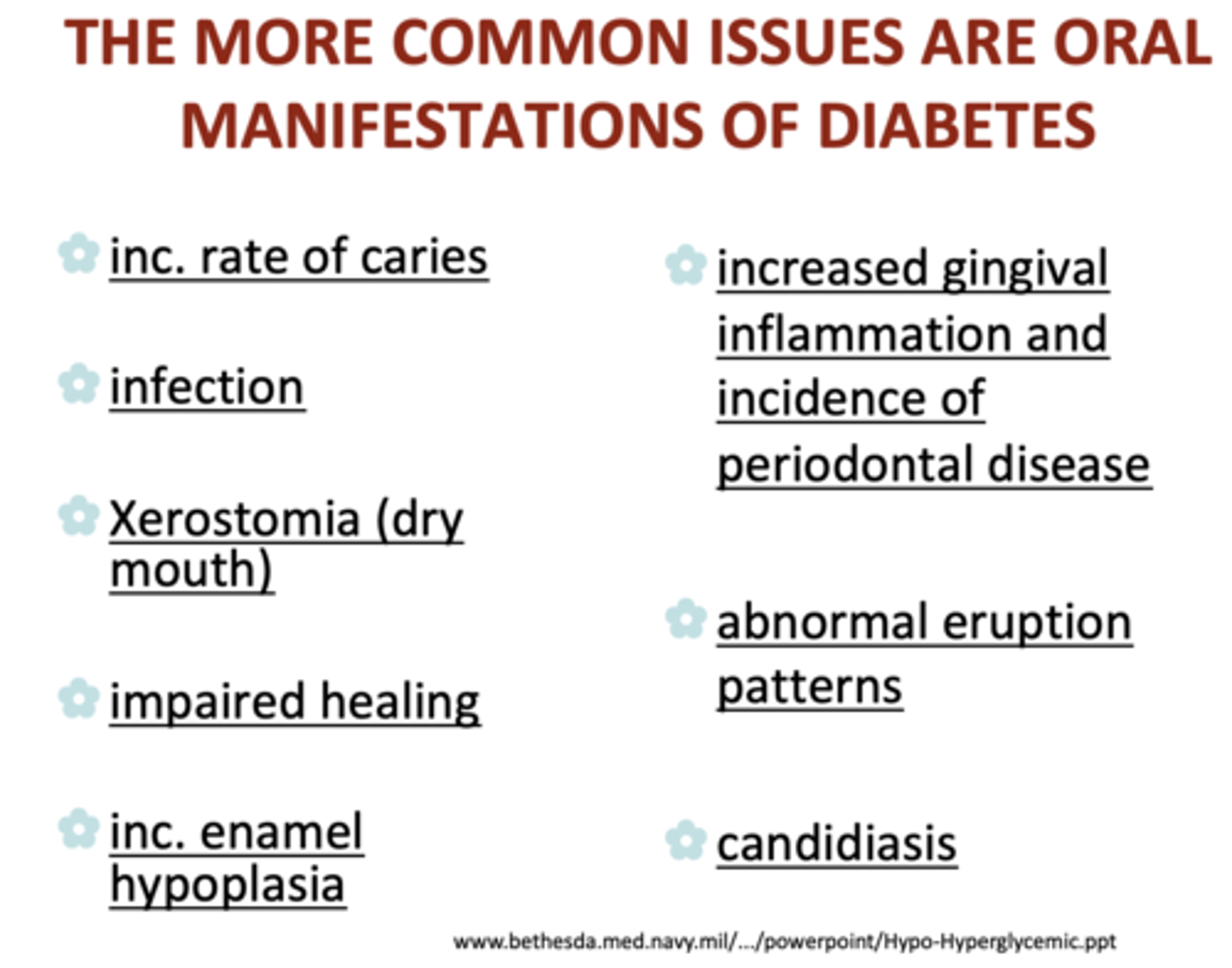
What are common oral manifestations of diabetes?
- Increased rate of caries
- Infection
- Xerostomia (dry mouth)
- Impaired healing
- Increased enamel hypoplasia
- Increased gingival inflammation and incidence of periodontal disease
- Abnormal eruption patterns
- Candidiasis
What are three serious acute problems that can be life-threatening in diabetic patients?
- Diabetic ketoacidosis (DKA)
- Hyperglycemic/ Hyperosmolar Syndrome (HHS)
- Hypoglycemia
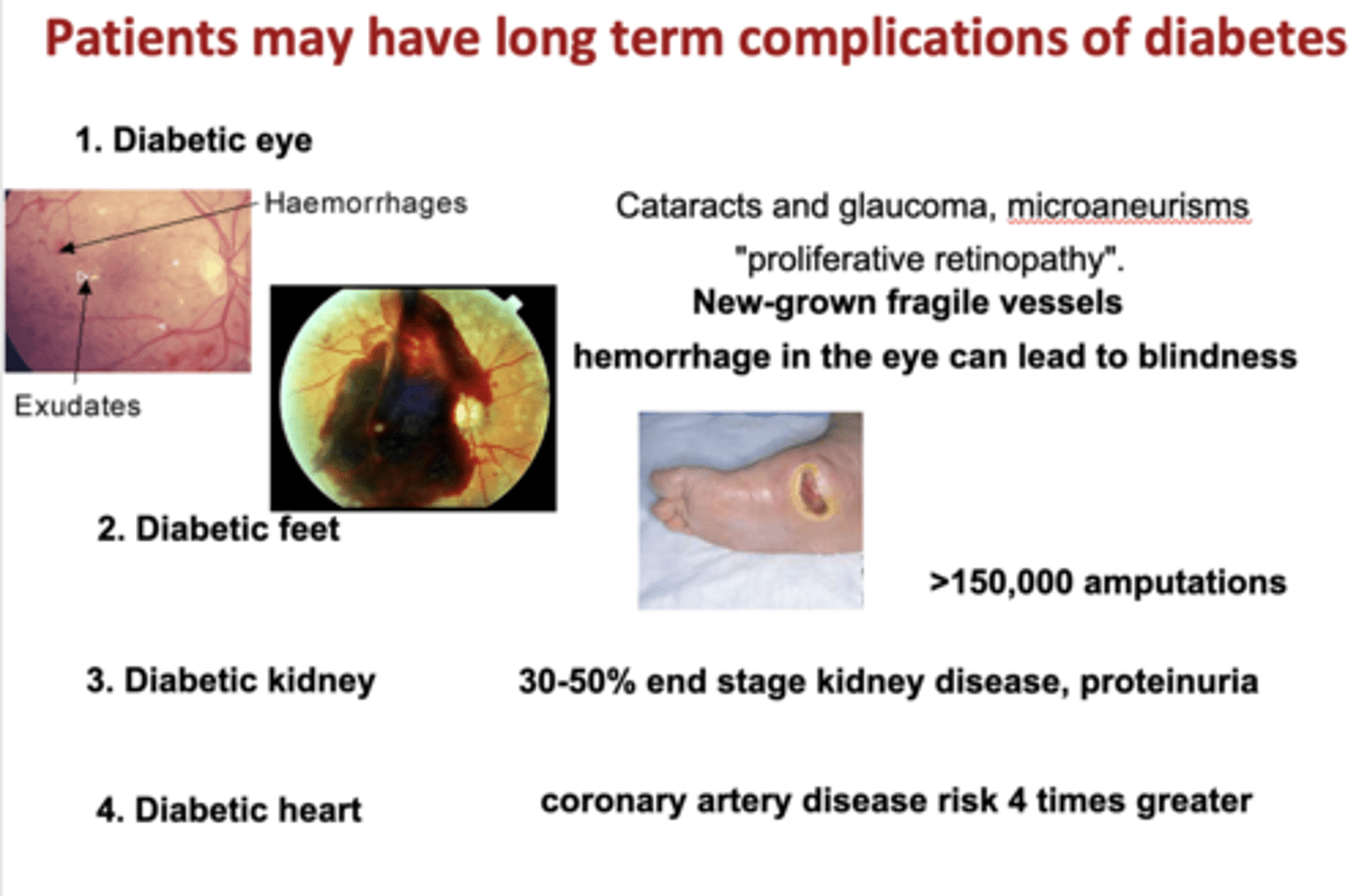
What are four long term organ complications of diabetes?
- Eyes (cataracts and glaucoma, microaneurisms)
- Feet (amputations)
- Kidneys (proteinuria)
- Heart (coronary artery disease risk)
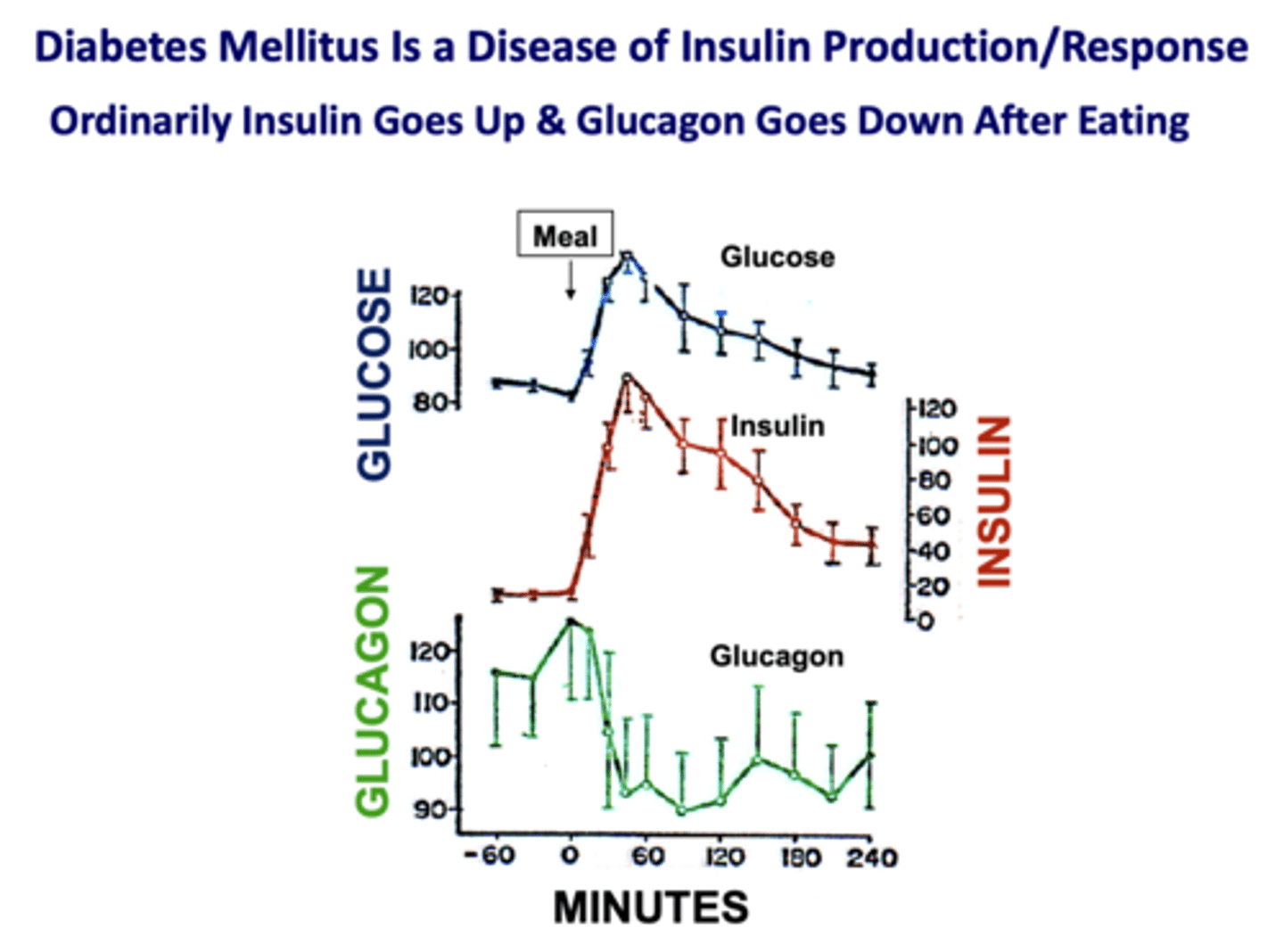
What is a disease of insulin production/response?
diabetes mellitus
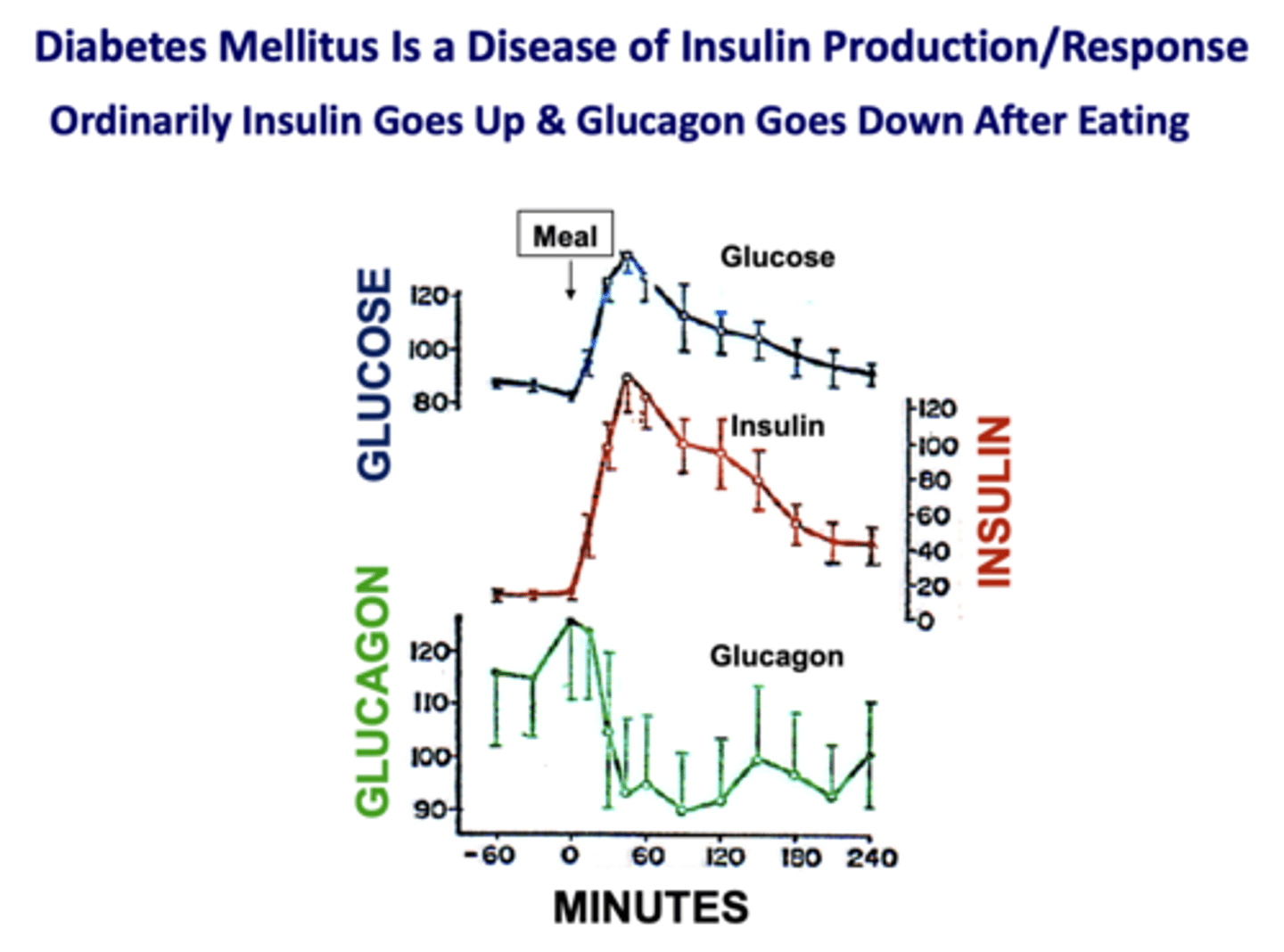
After eating, how do insulin and glucagon change?
- Insulin increases
- Glucagon decreases
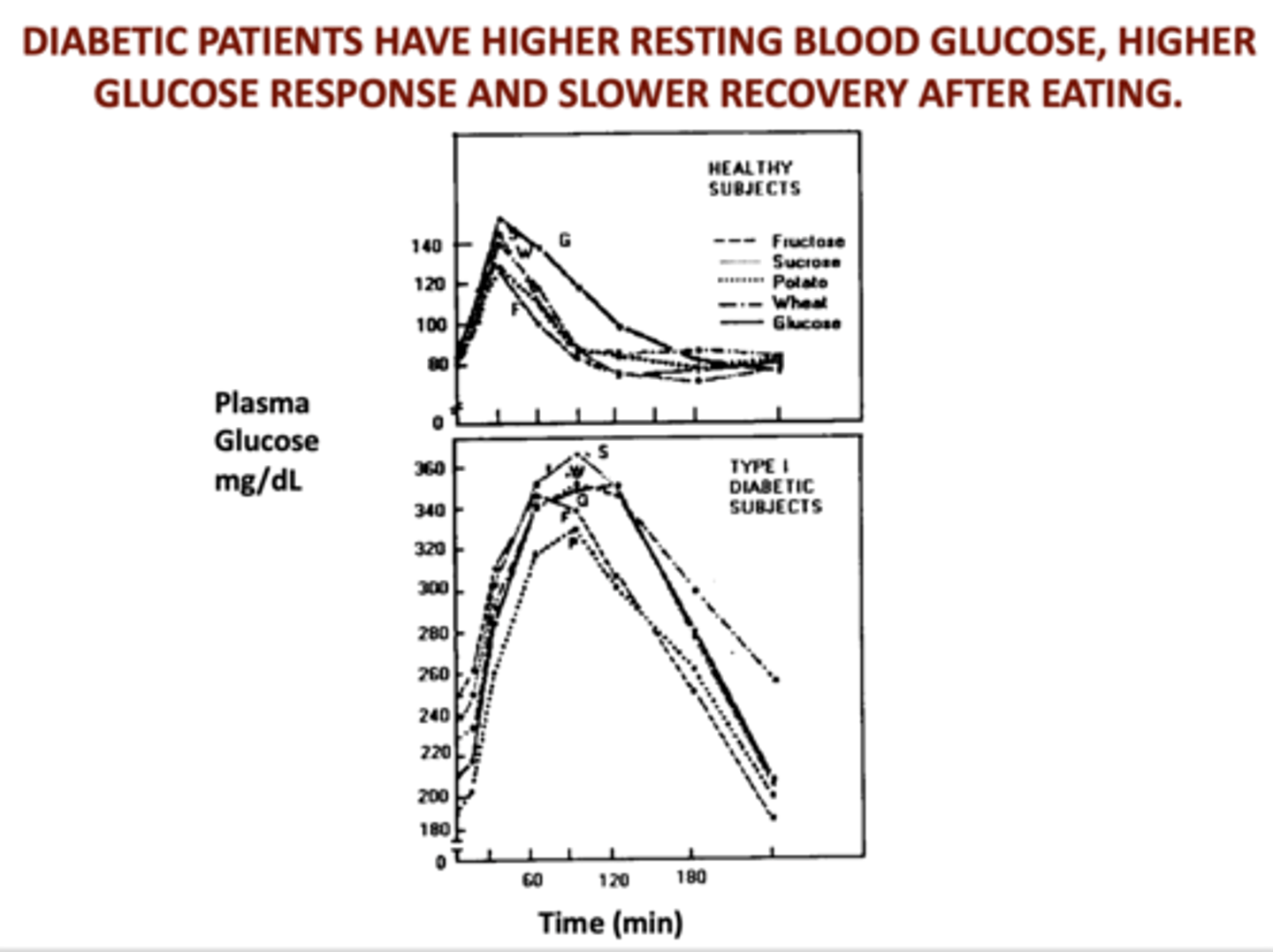
Diabetic patients have higher resting blood glucose, higher glucose response, and _____________ recovery after eating
Slower
What is the hormone of the well-fed state?
insulin
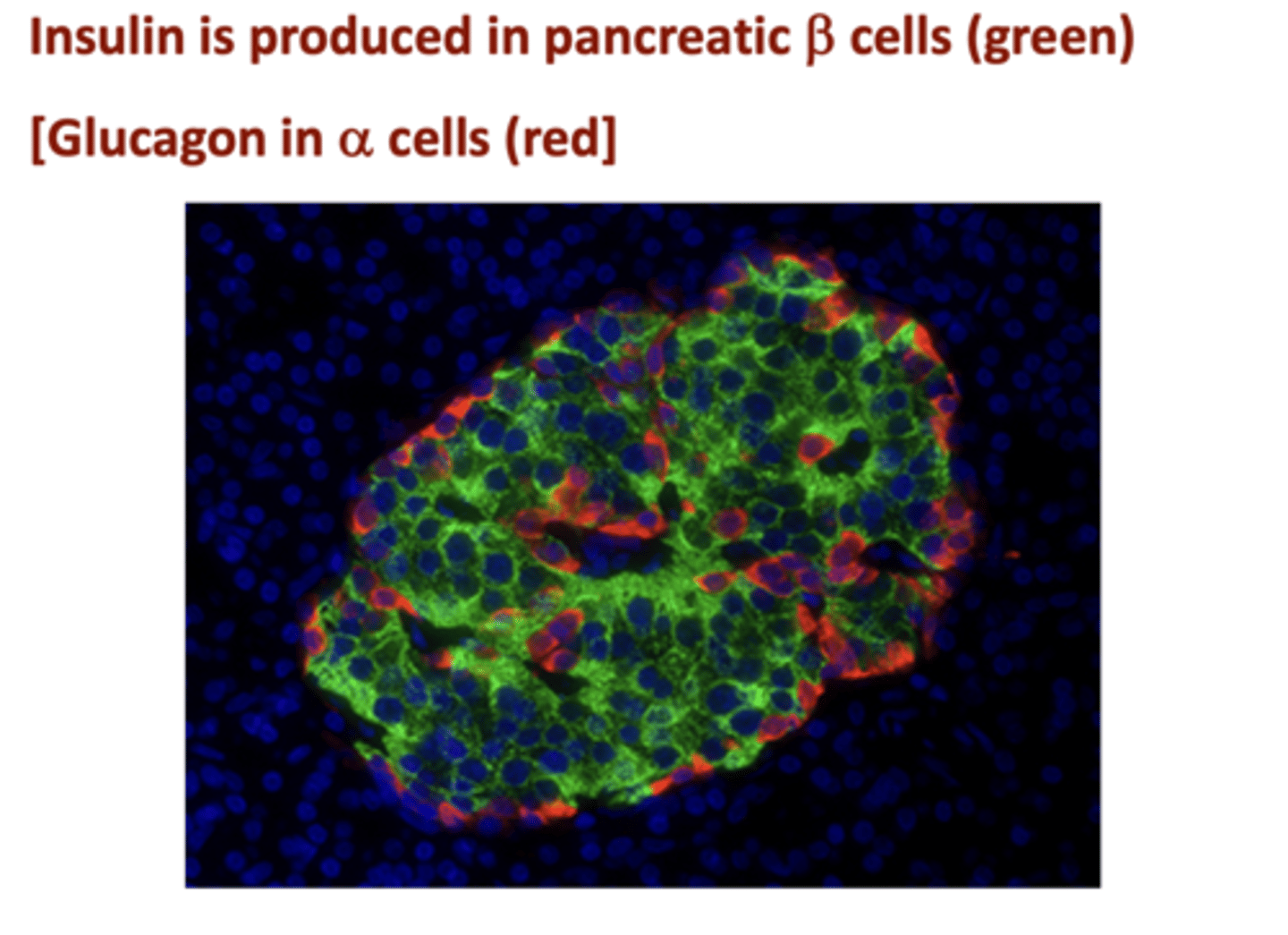
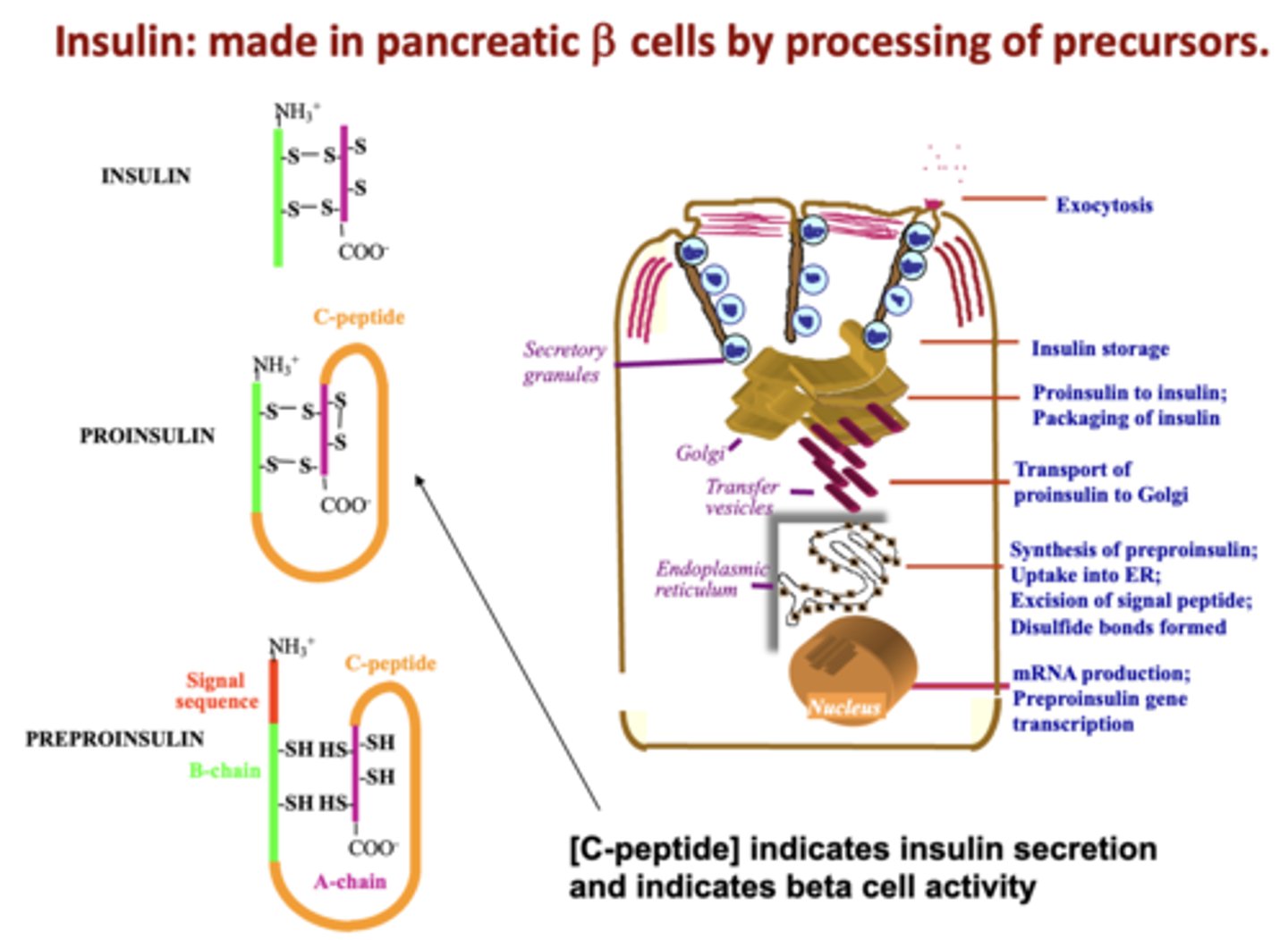
Where is insulin produced?
pancreatic beta cells
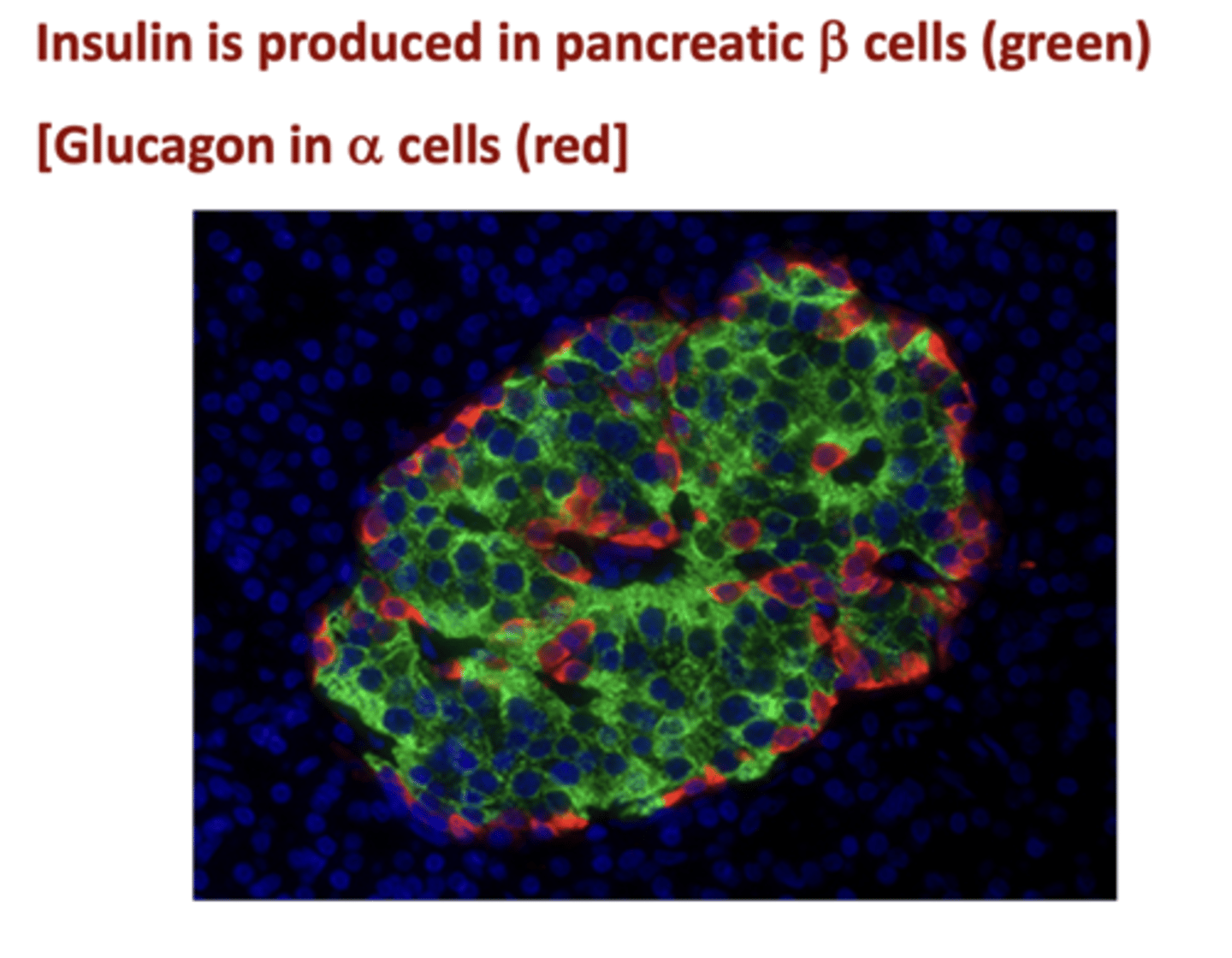
What cells make and store glucagon?
Alpha cells
What is measured to estimate the average blood glucose of the life of a RBC?
HbA1C (glycated hemoglobin)
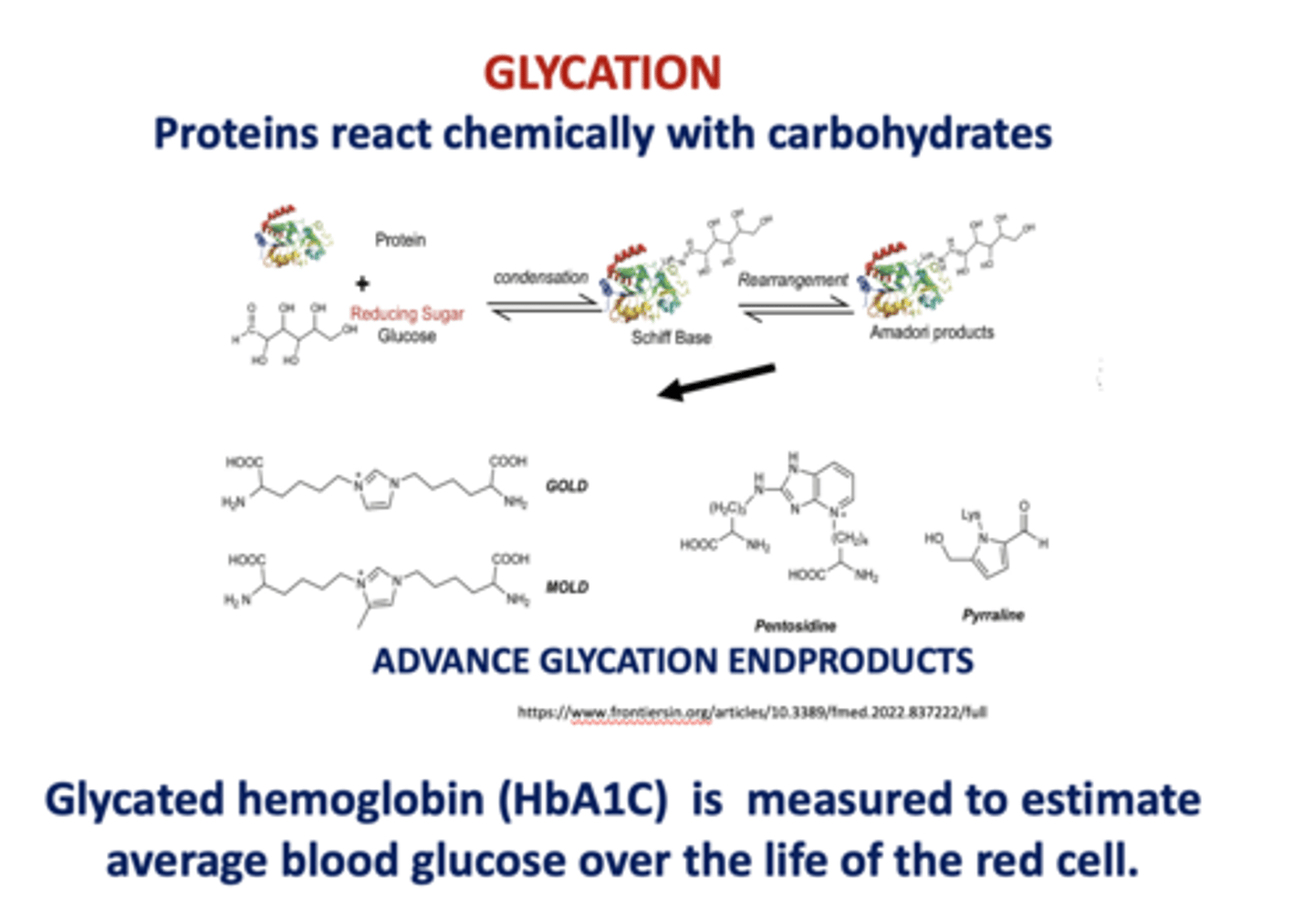
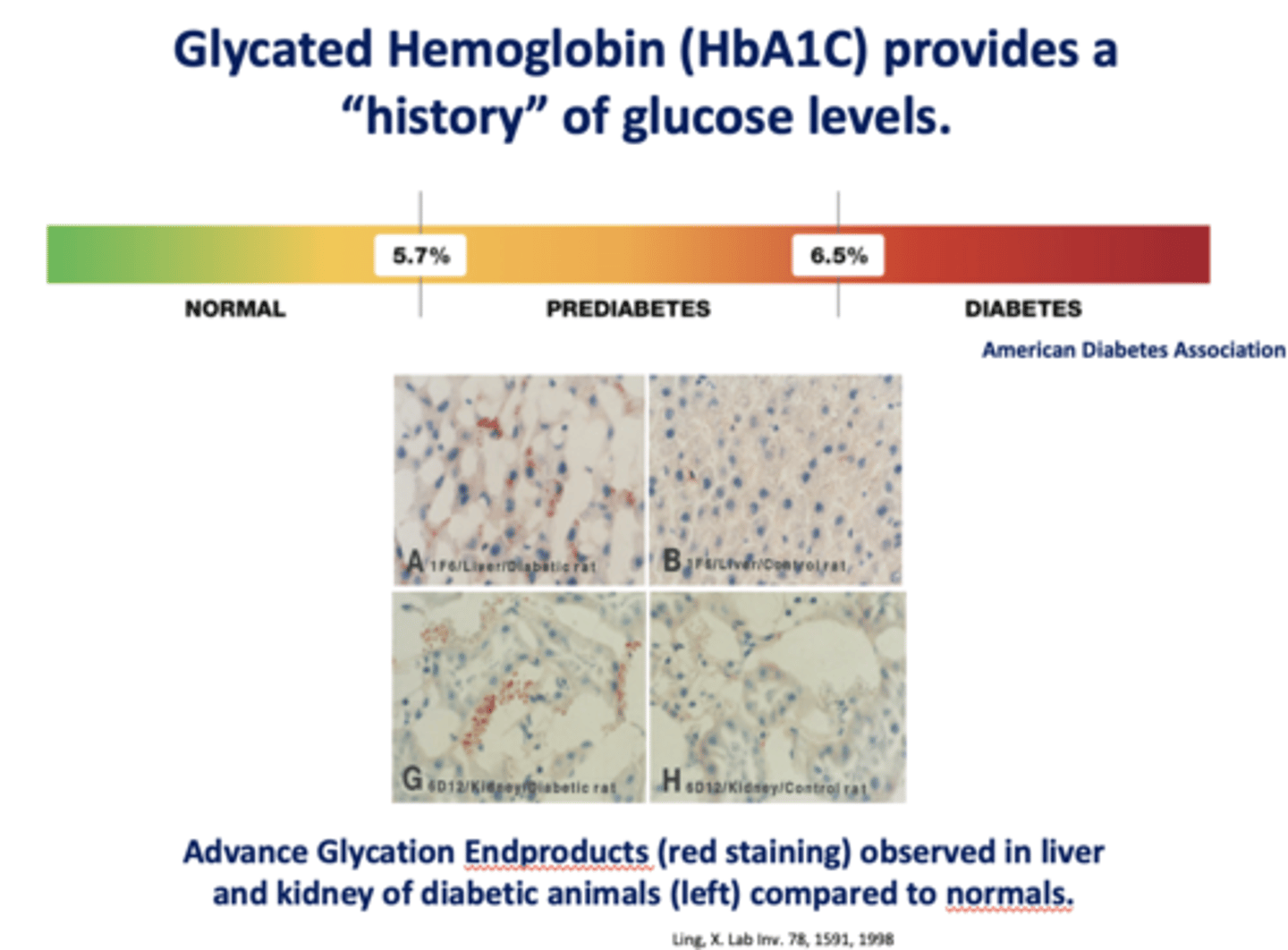
What provides a "history" of glucose levels?
HbA1C (glycated hemoglobin)
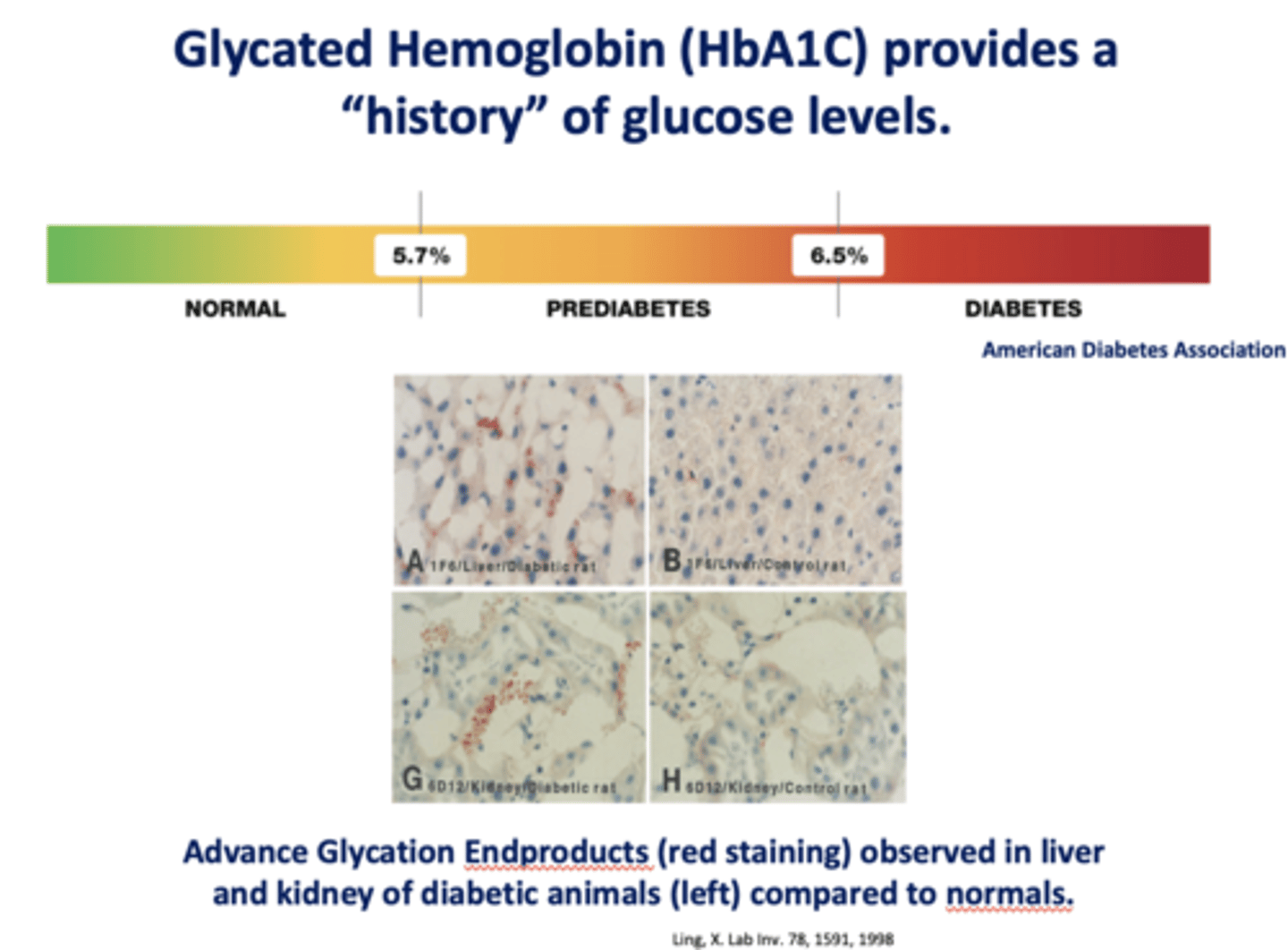
A HbA1C level of <5.7% would be...
A. Normal
B. Prediabetes
C. Diabetes
A. Normal
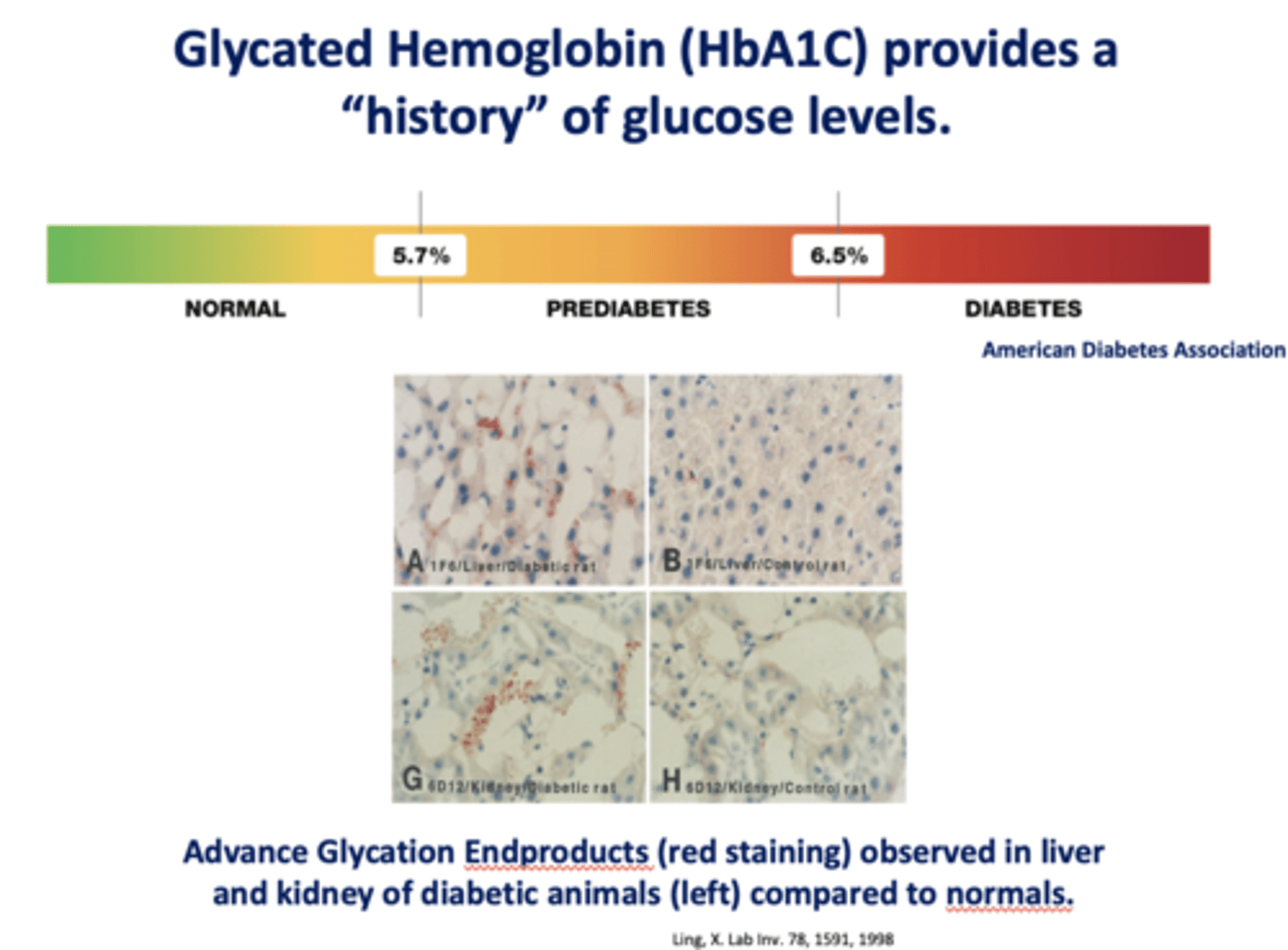
A HbA1C level between 5.7% and 6.5% would be...
A. Normal
B. Prediabetes
C. Diabetes
B. Prediabetes
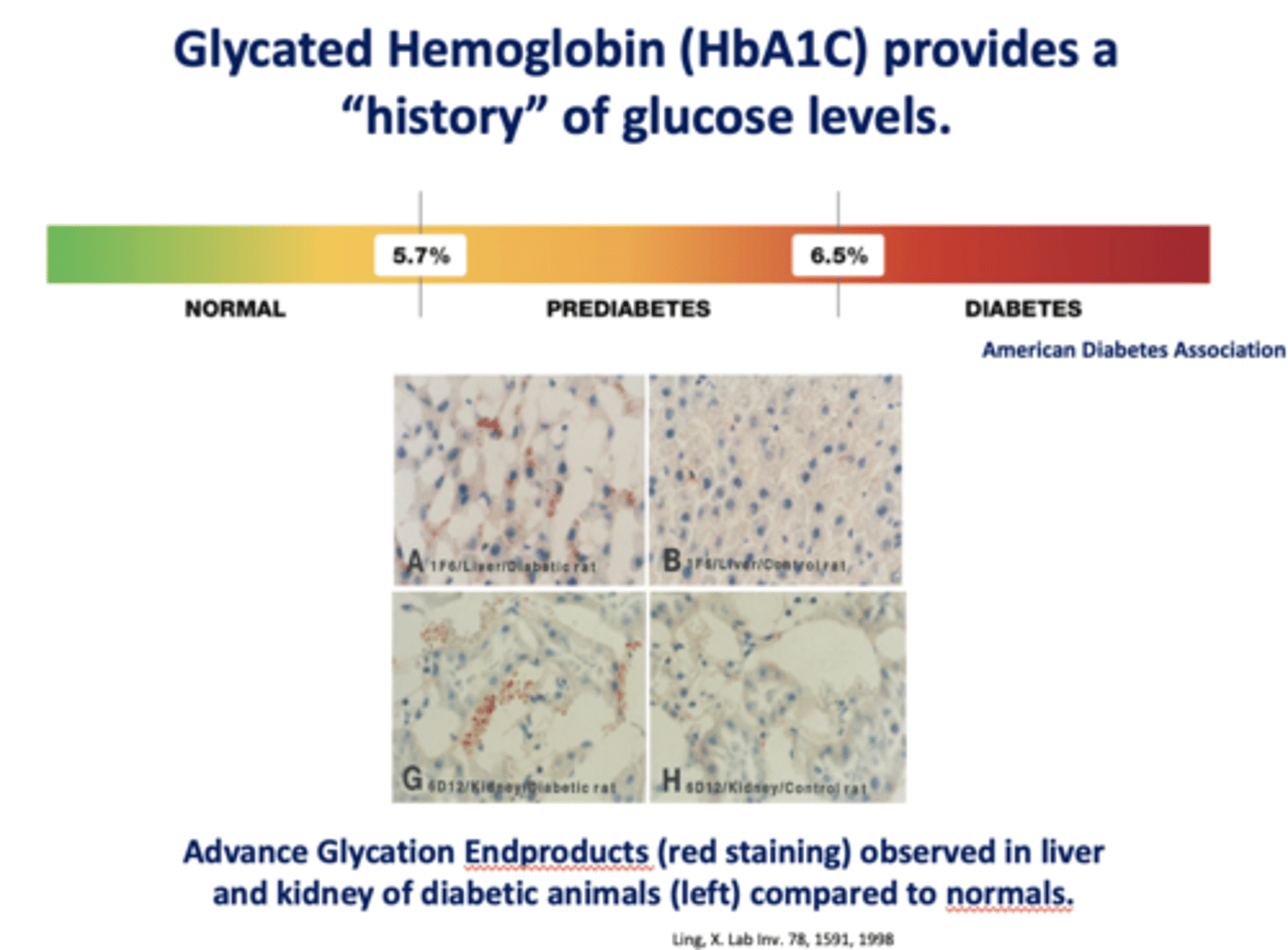
A HbA1C level of >6.5% would be...
A. Normal
B. Prediabetes
C. Diabetes
C. Diabetes
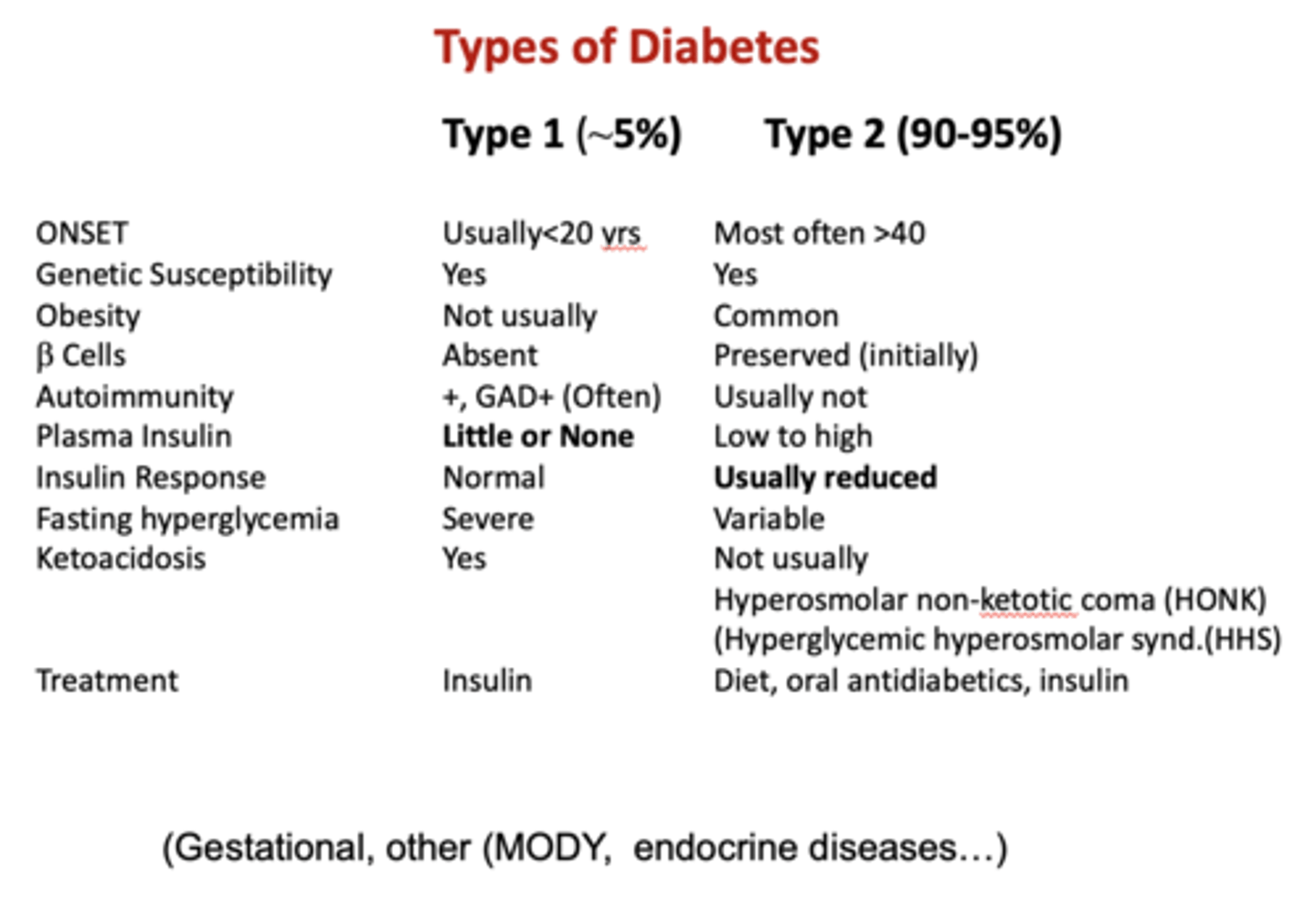
What type of diabetes is more common?
Type II (90-95%)
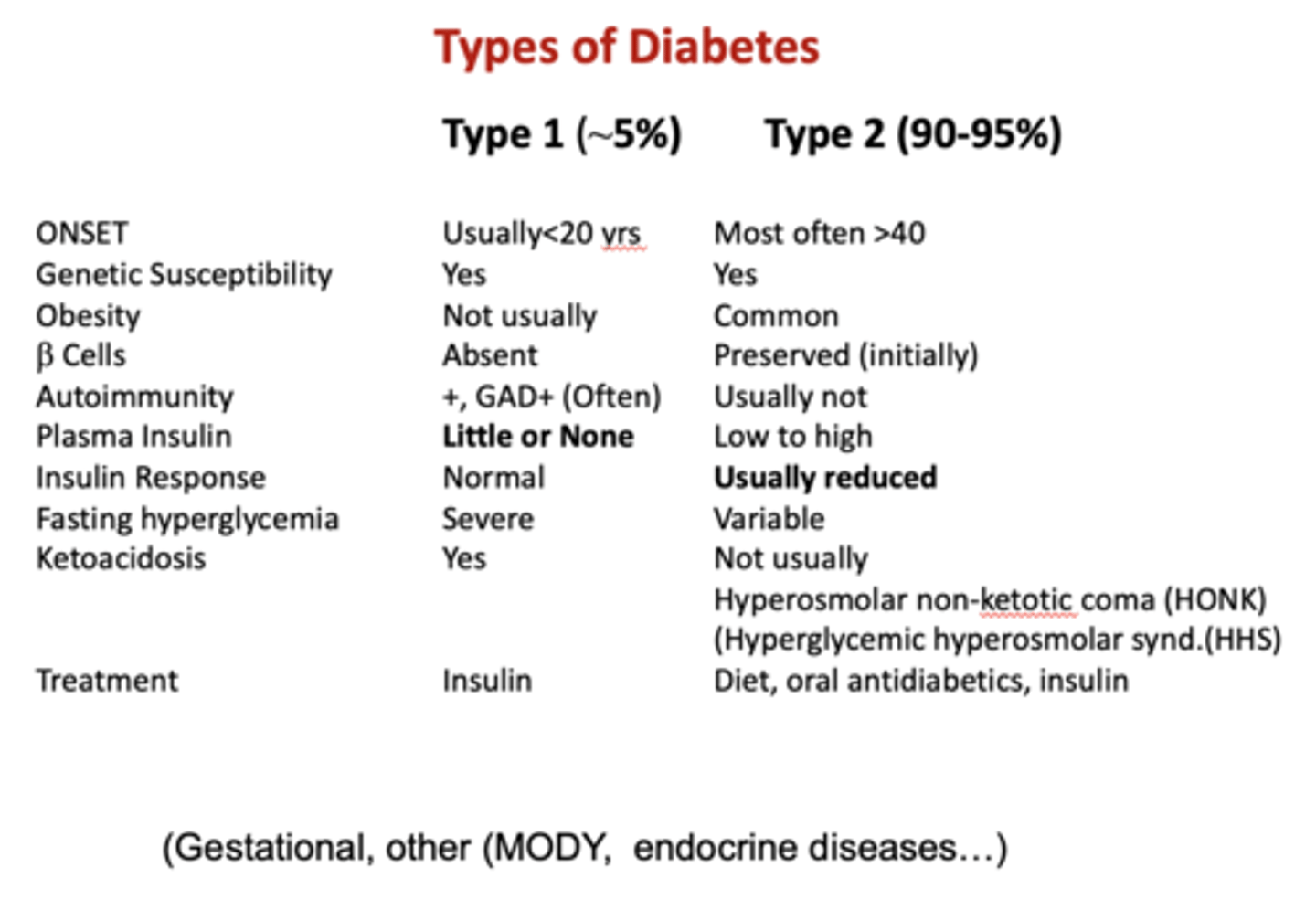
Does type I diabetes have B cell function?
No
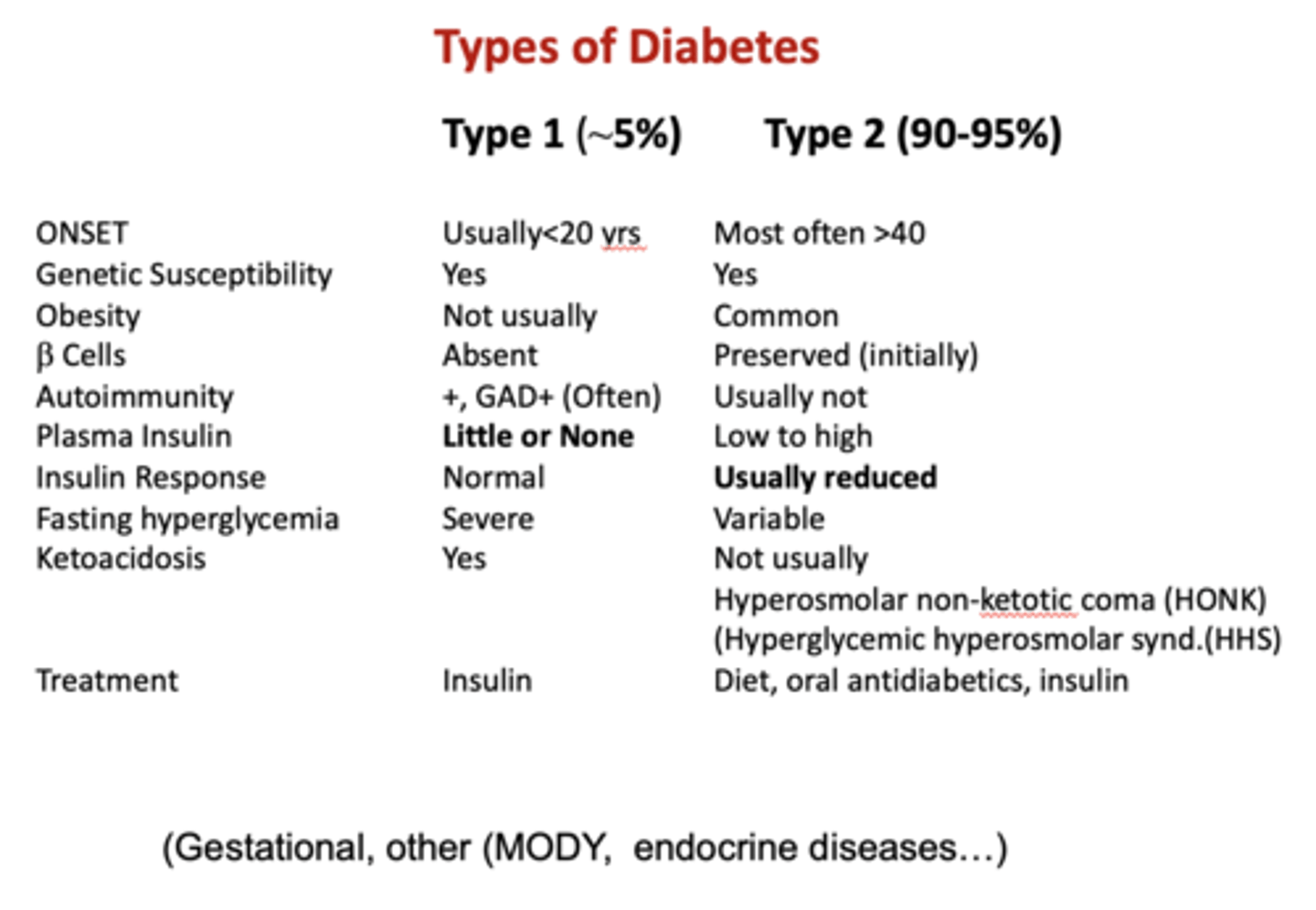
Does type II diabetes have B cell function?
Perserved (initially)
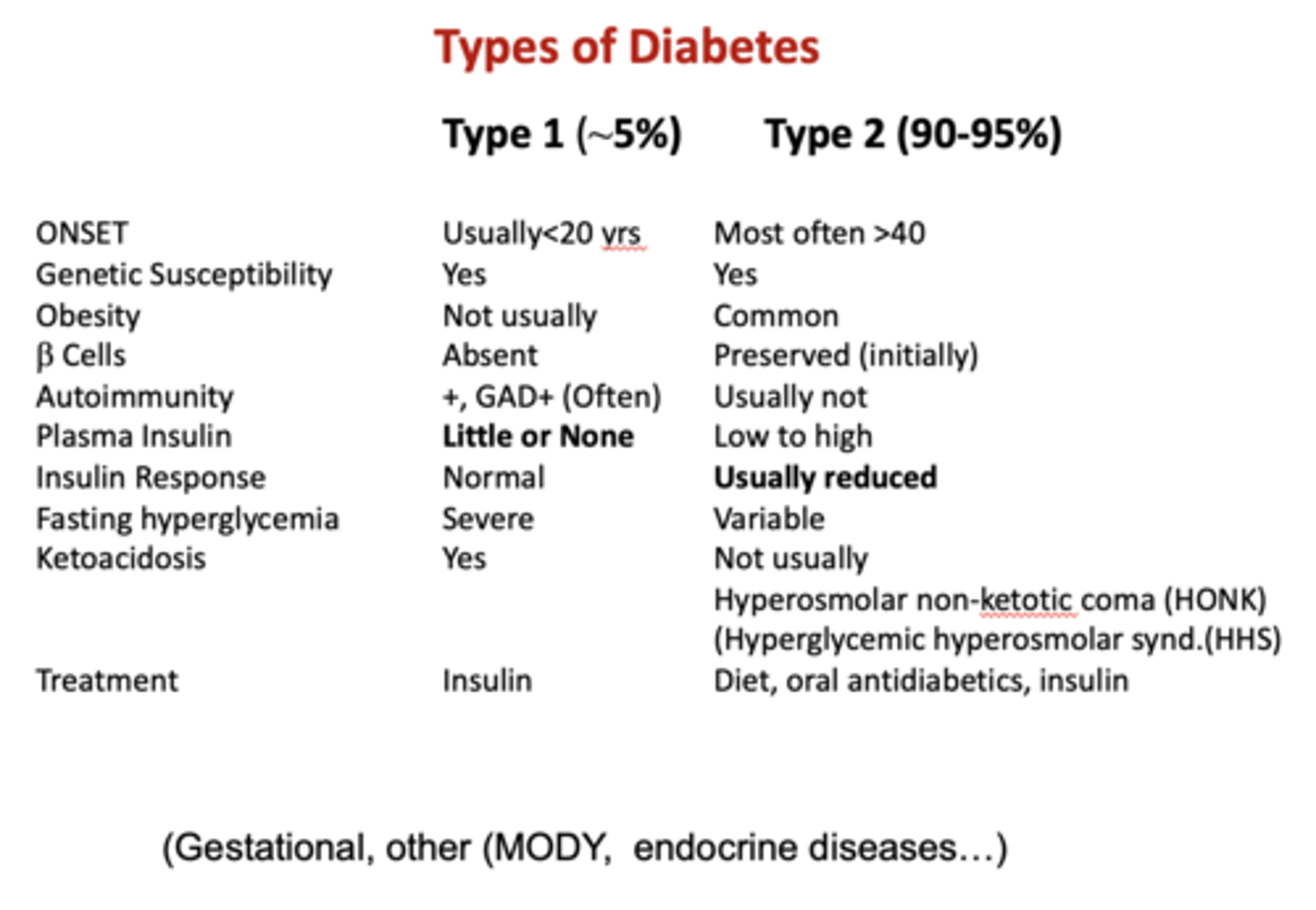
Does type I or type II diabetes have little or no plasma insulin?
Type I
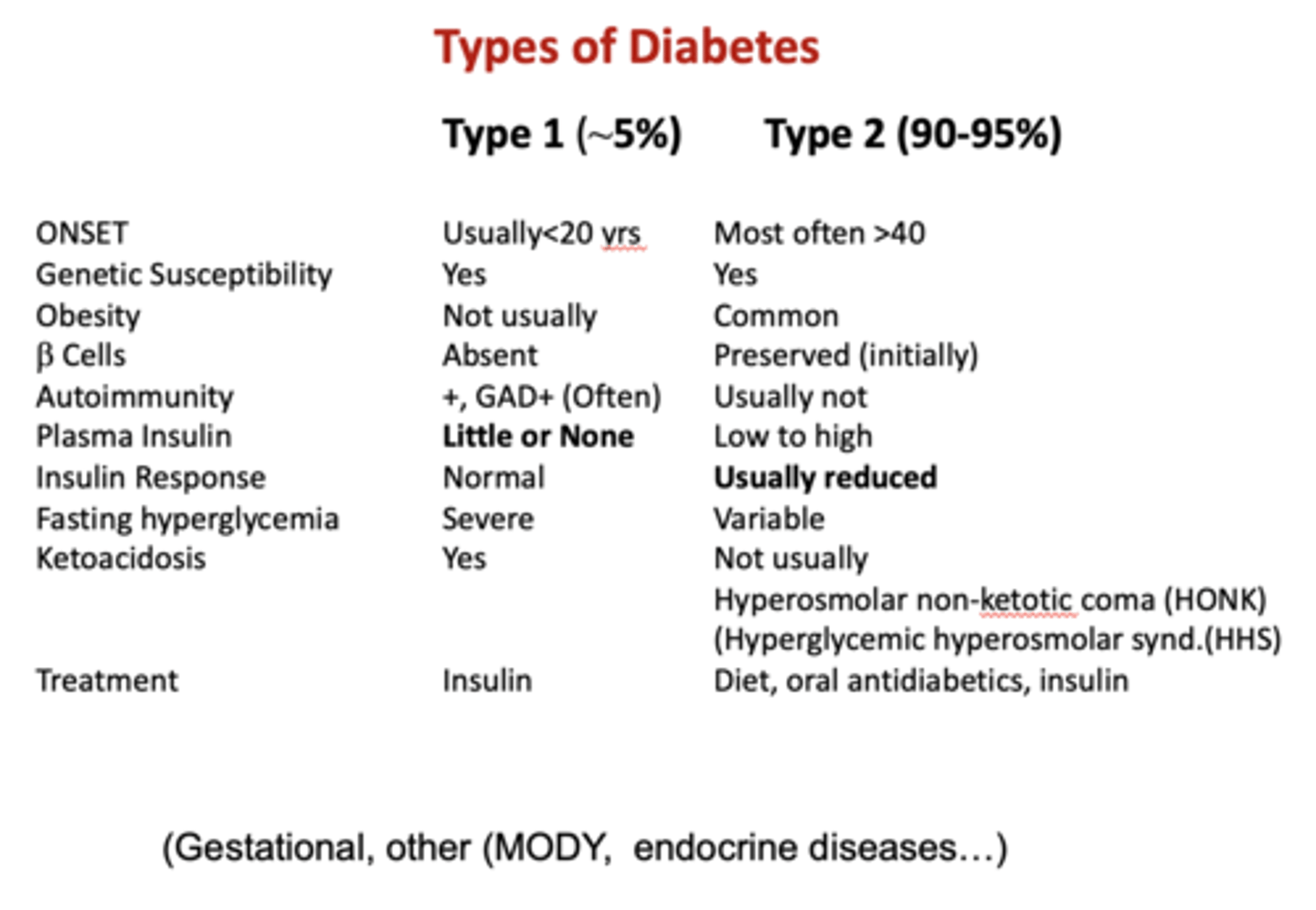
In type I or type II diabetes is the insulin response usually reduced?
Type II
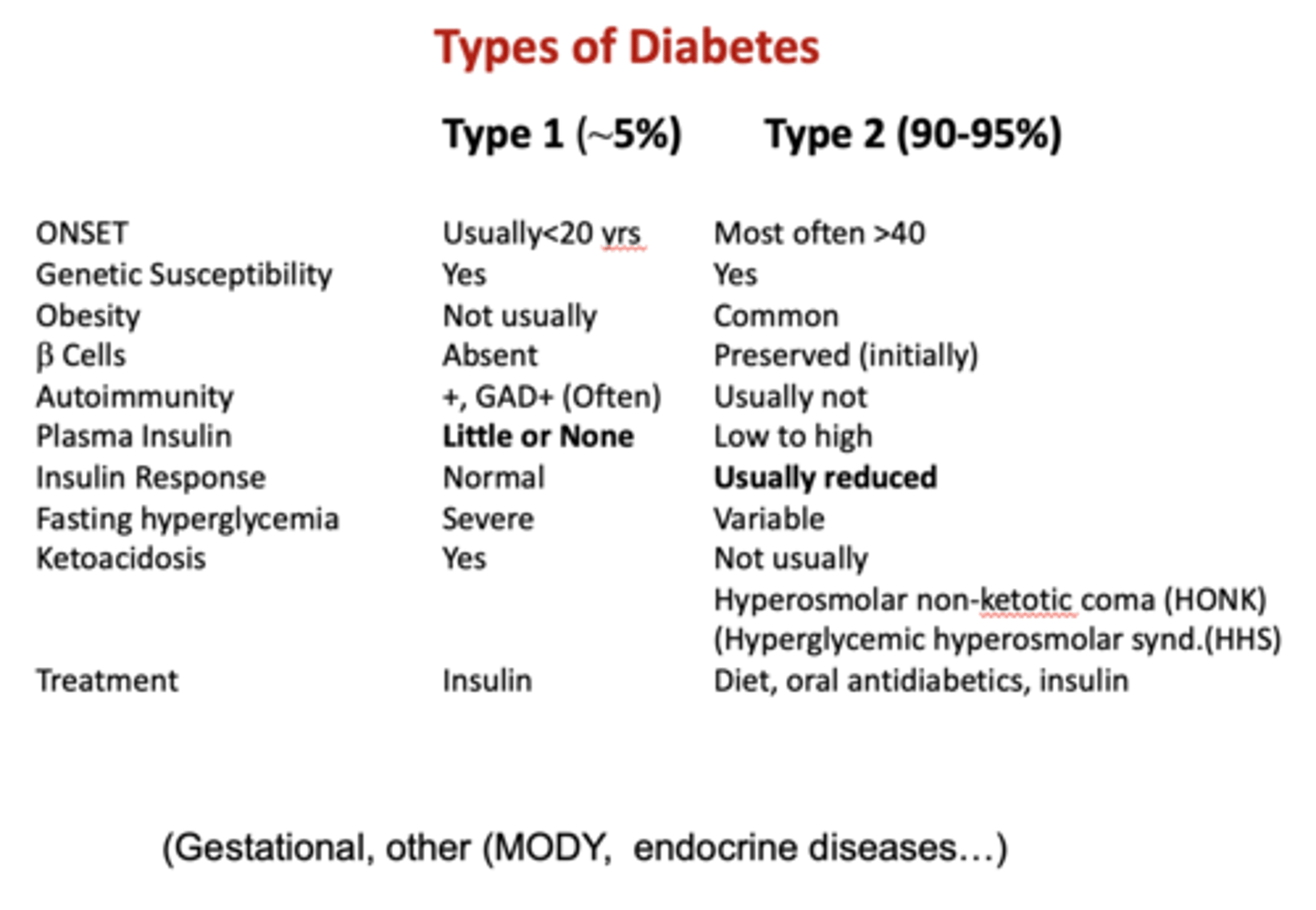
Do type I or type II have ketoacidosis?
Type I
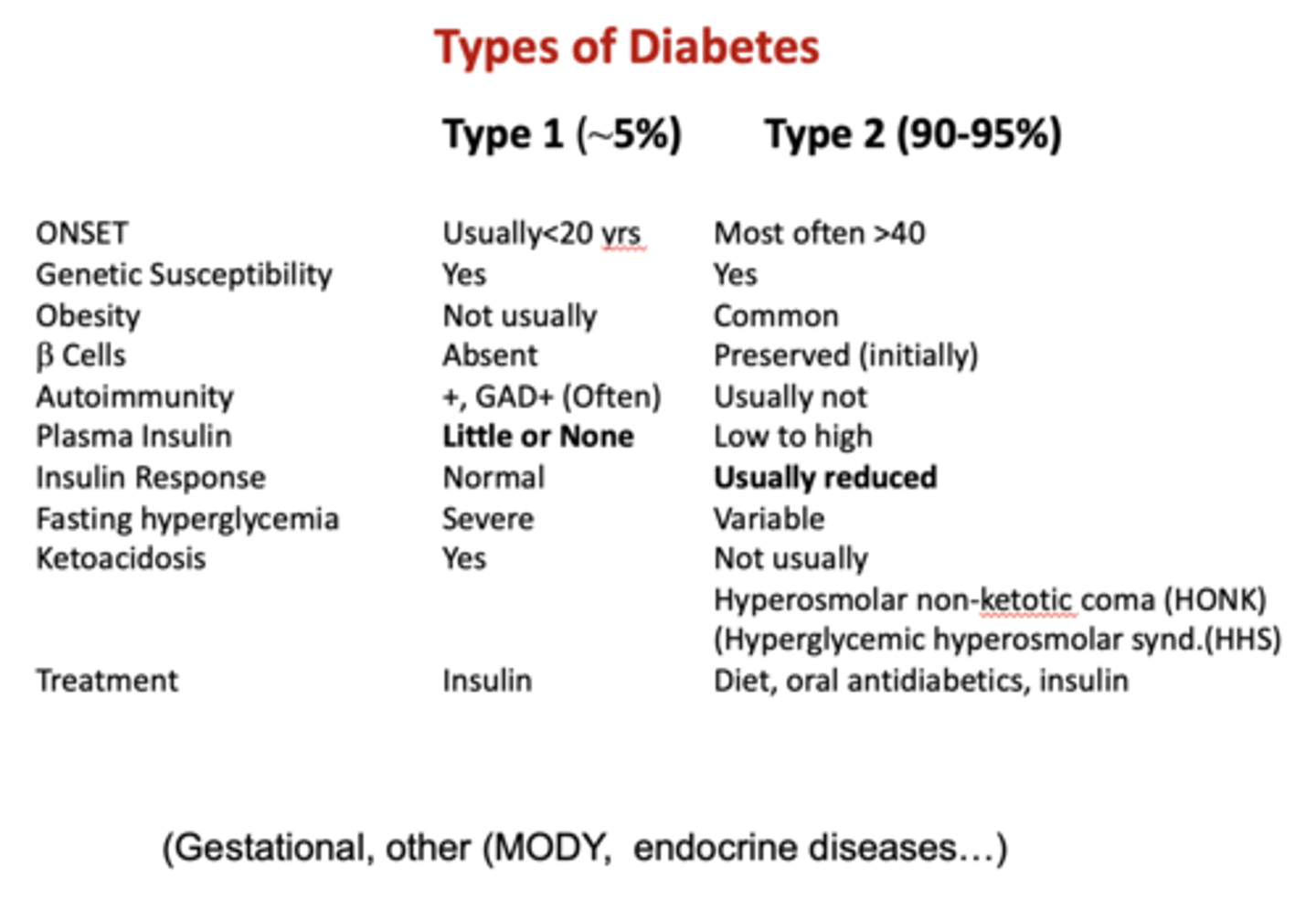
Do type I or type II have Hyperosmolar non-ketotic coma (HONK) or (Hyperglycemic hyperosmolar syndrome (HHS)?
Type II
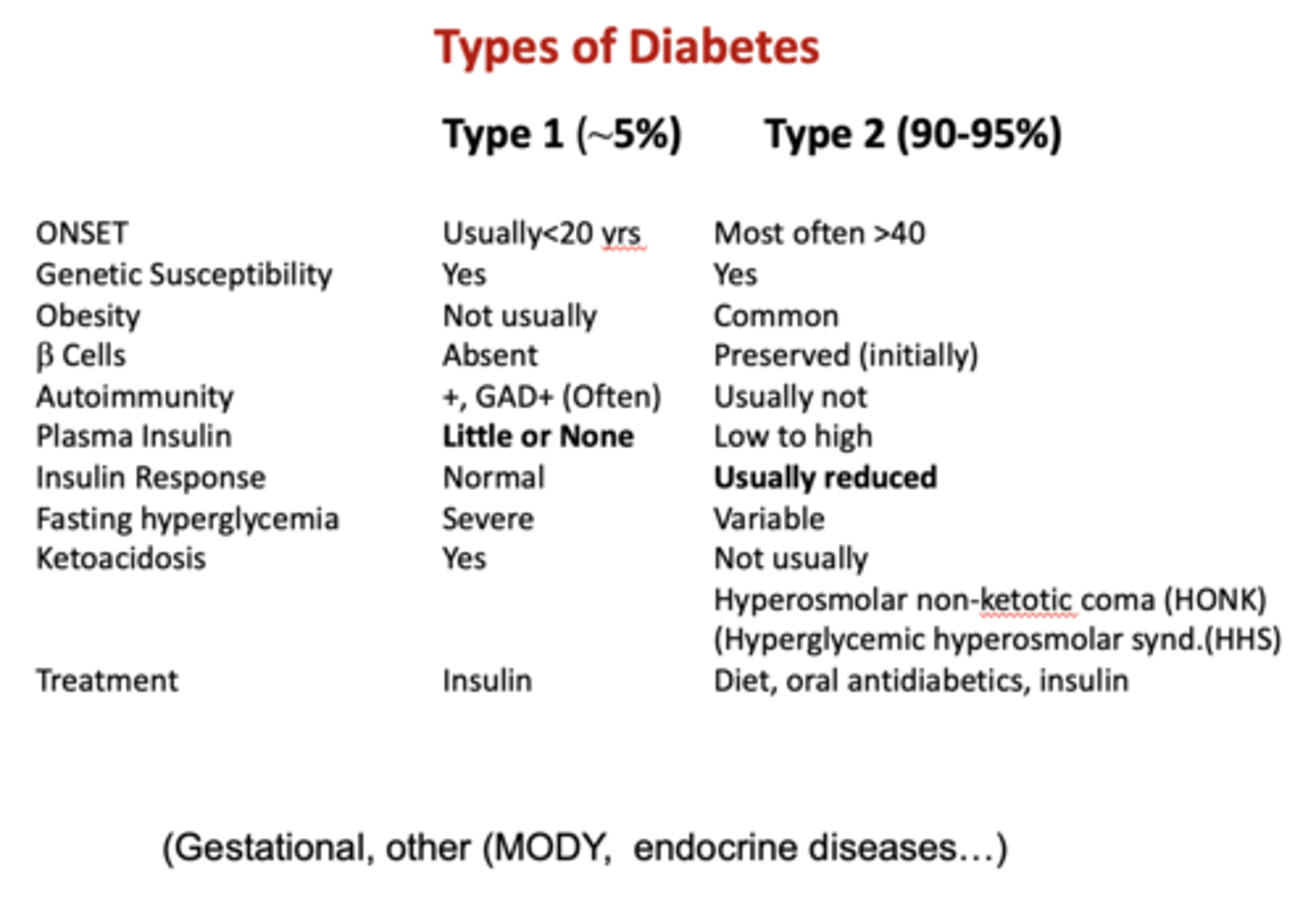
What is the treatment for type I diabetes?
Insulin

What is the treatment for type II diabetes?
- Diet
- Oral antidiabetics
- Insulin
What indicates insulin secretion and indicates beta cell activity?
C-peptide
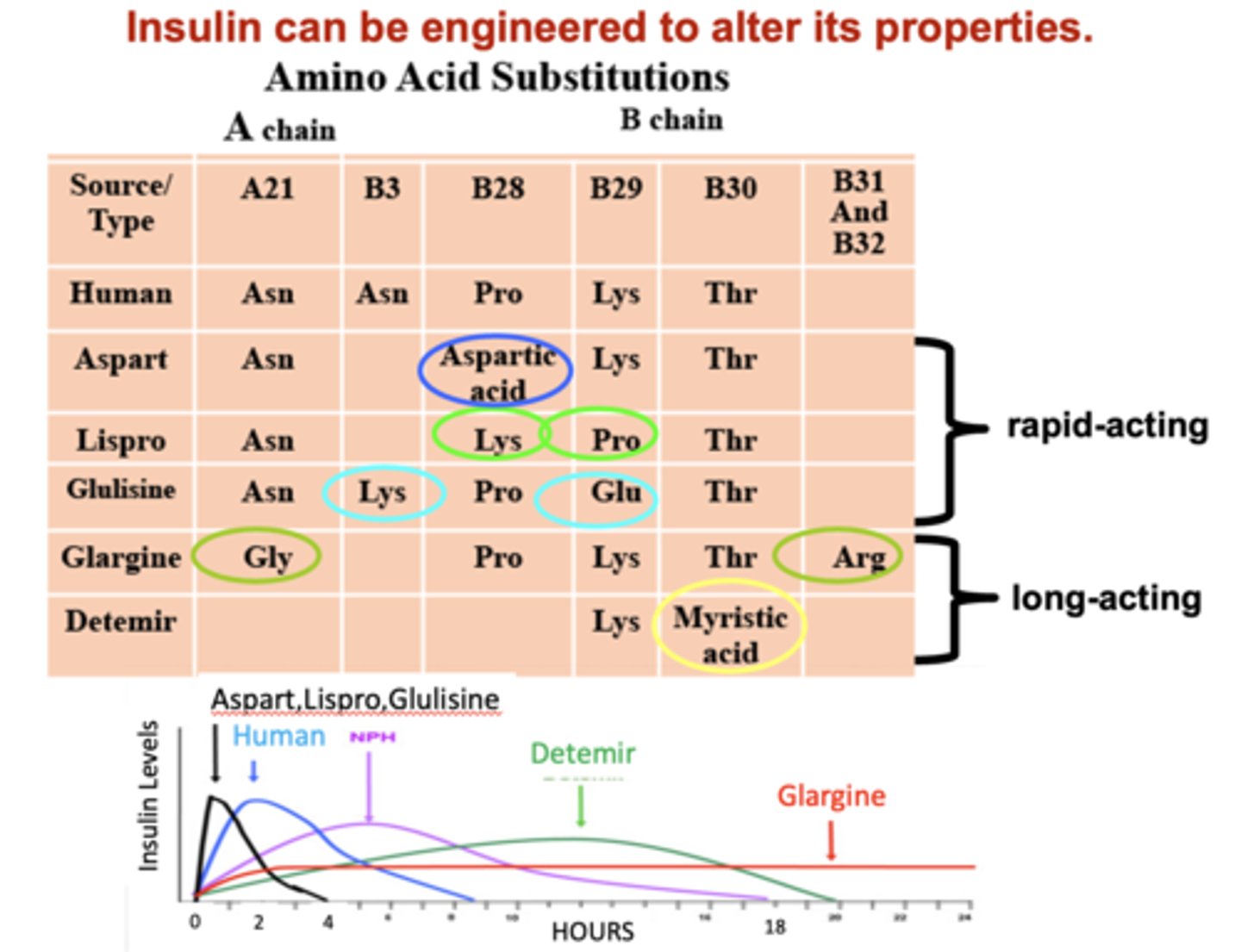
T/F: Insulin can be engineered to alter its properties
True
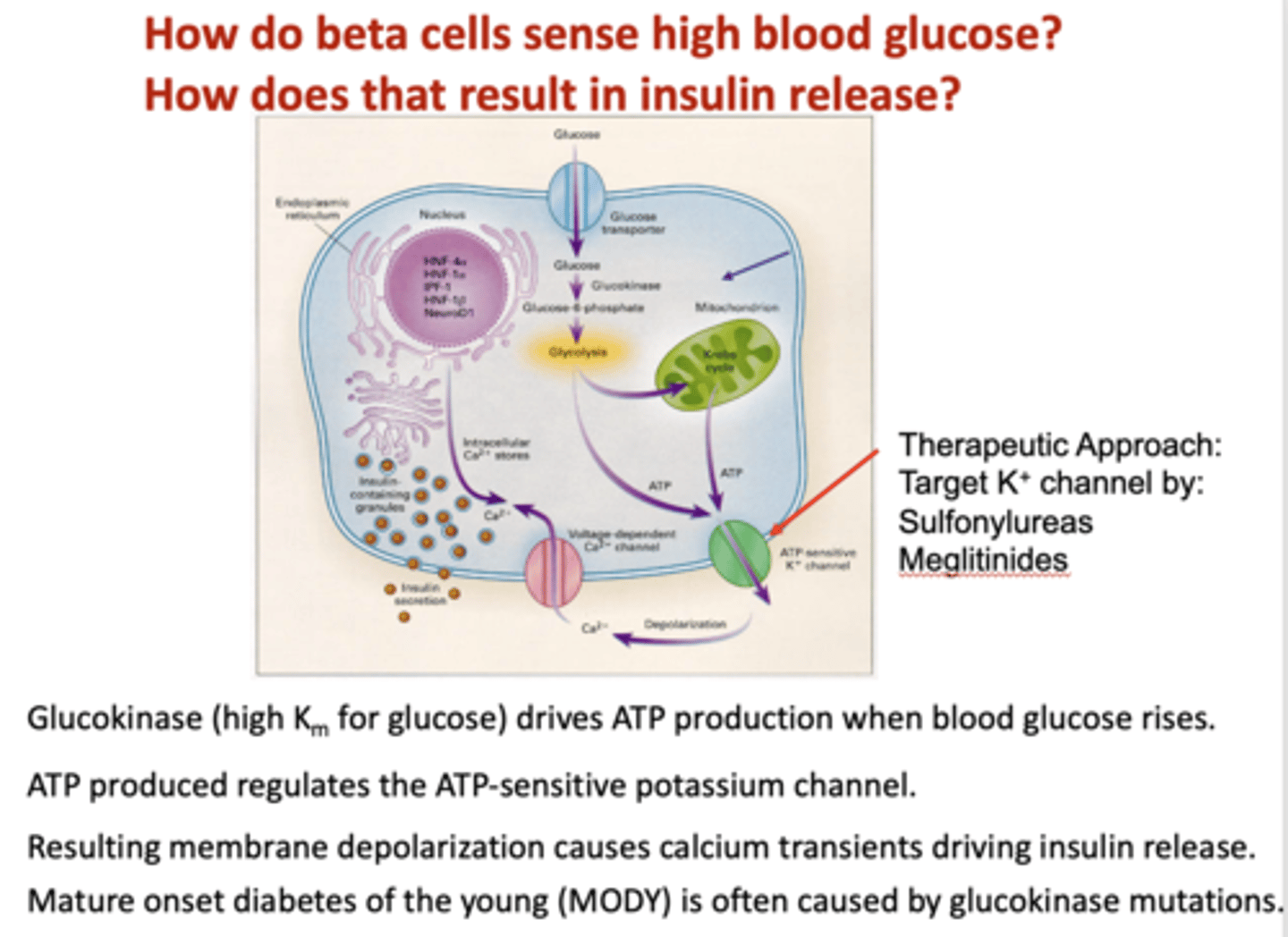
____________ (high Km for glucose) drives ATP production when blood glucose rises
glucokinase
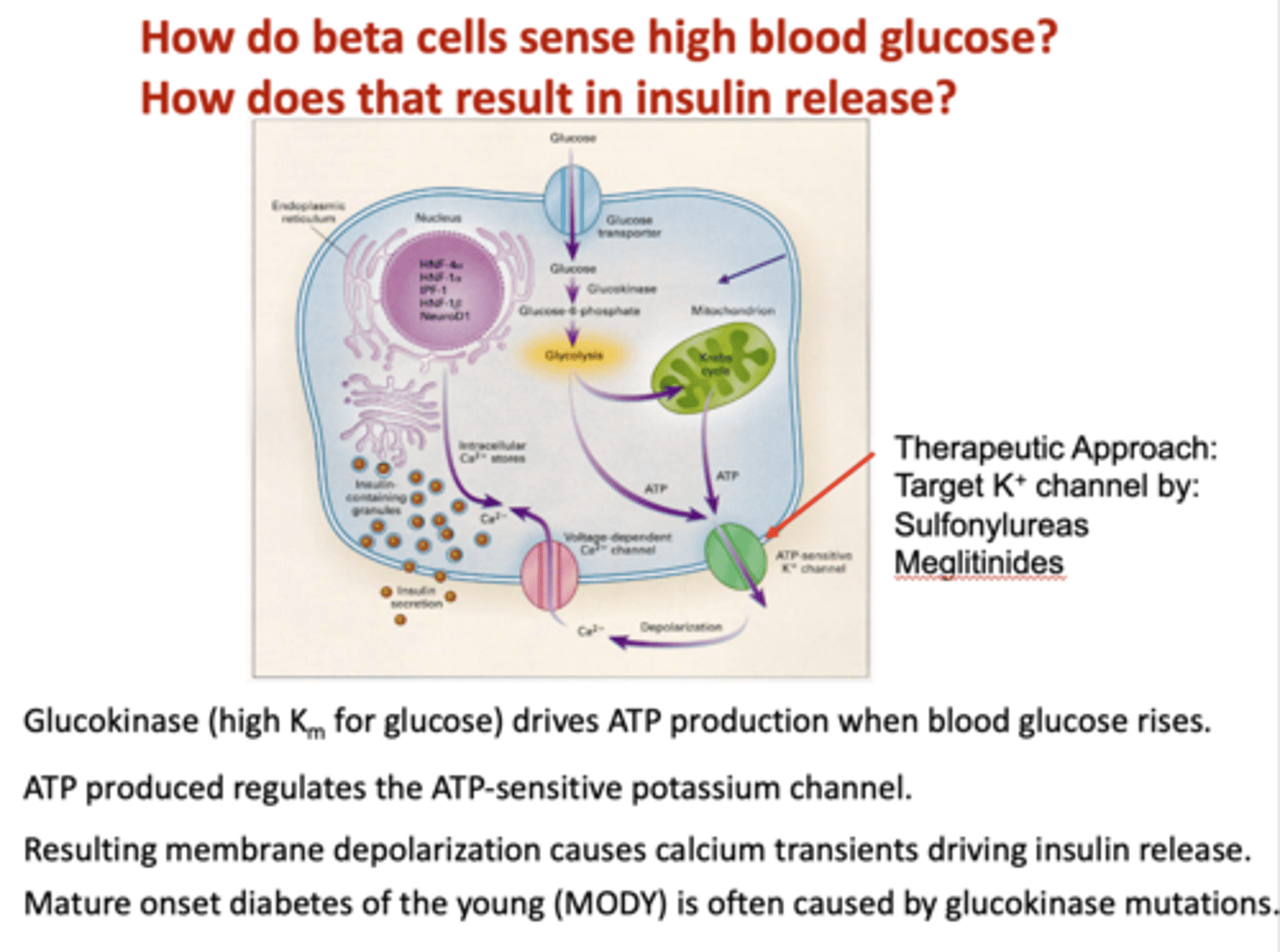
What drives insulin release?
calcium influx, depolarization
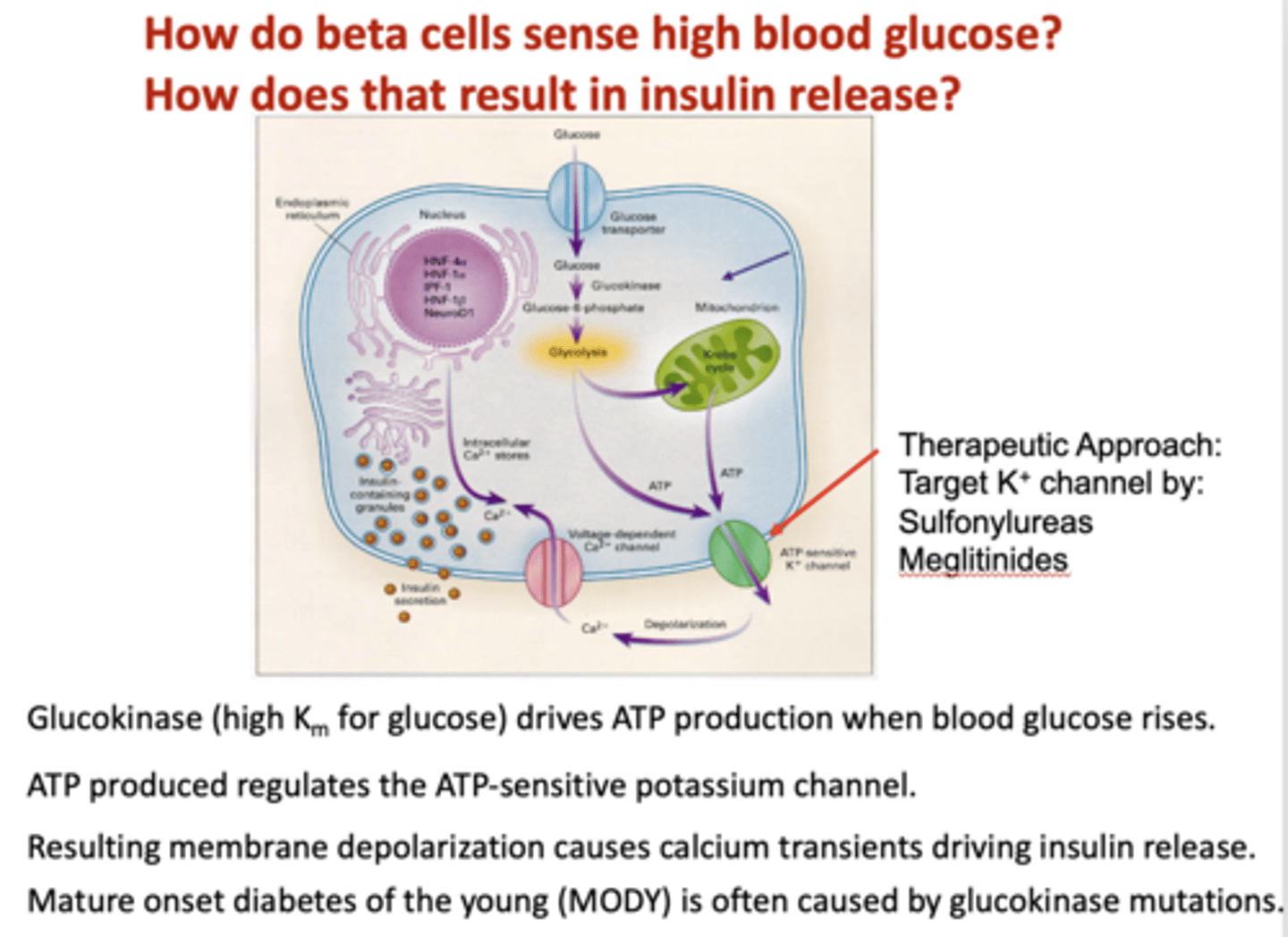
What is Ca2+ secretion indirectly controlled by?
ATP sensitive K+ channels
Mature onset diabetes of the young (MODY) is often caused by what mutation?
glucokinase
Does the dose of glucose have a greater response when given by mouth or by injection?
By mouth
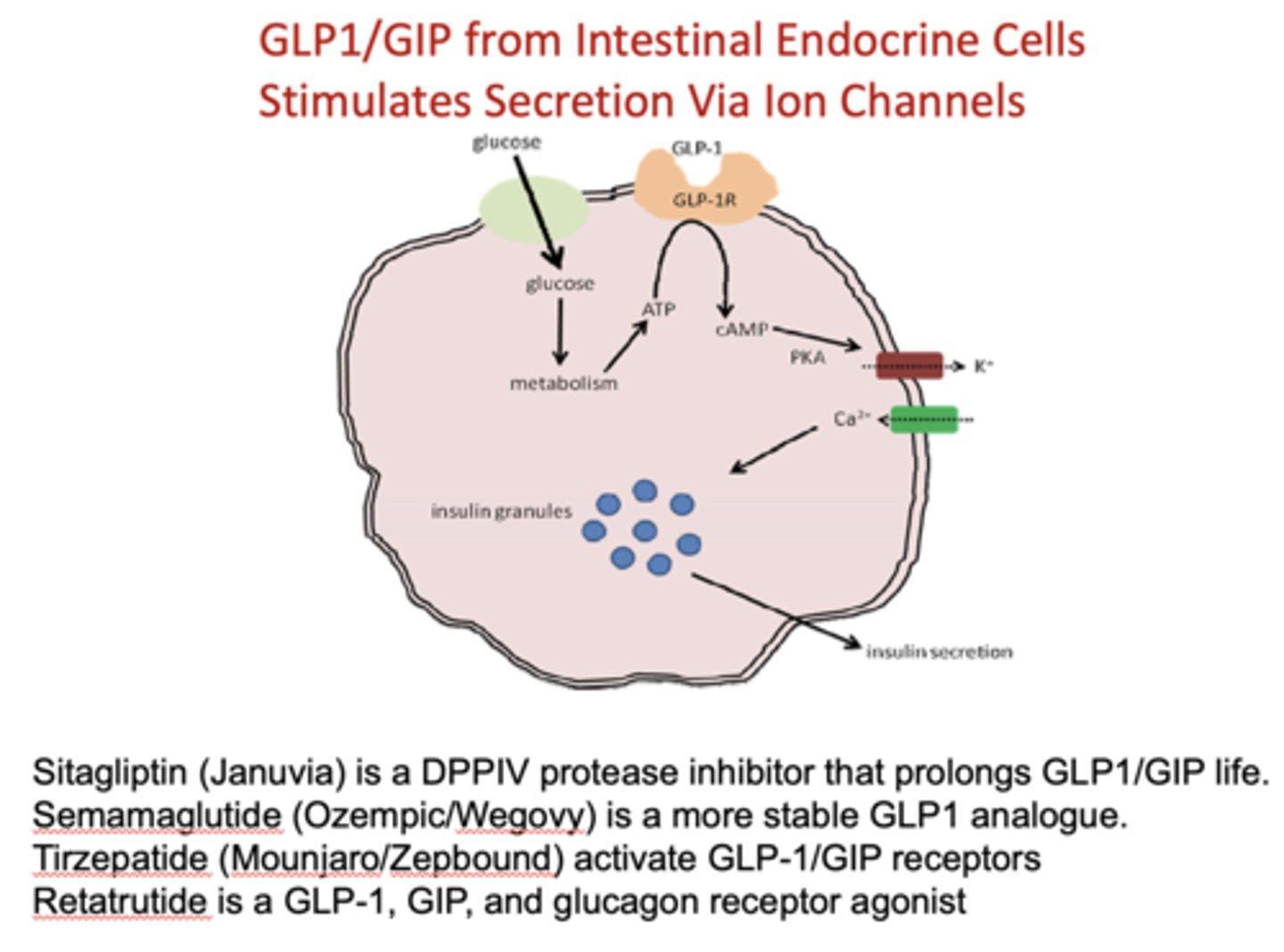
GLP1/GIP are found where and stimulate secretion of what?
Intestinal endocrine cells, insulin via ion channels
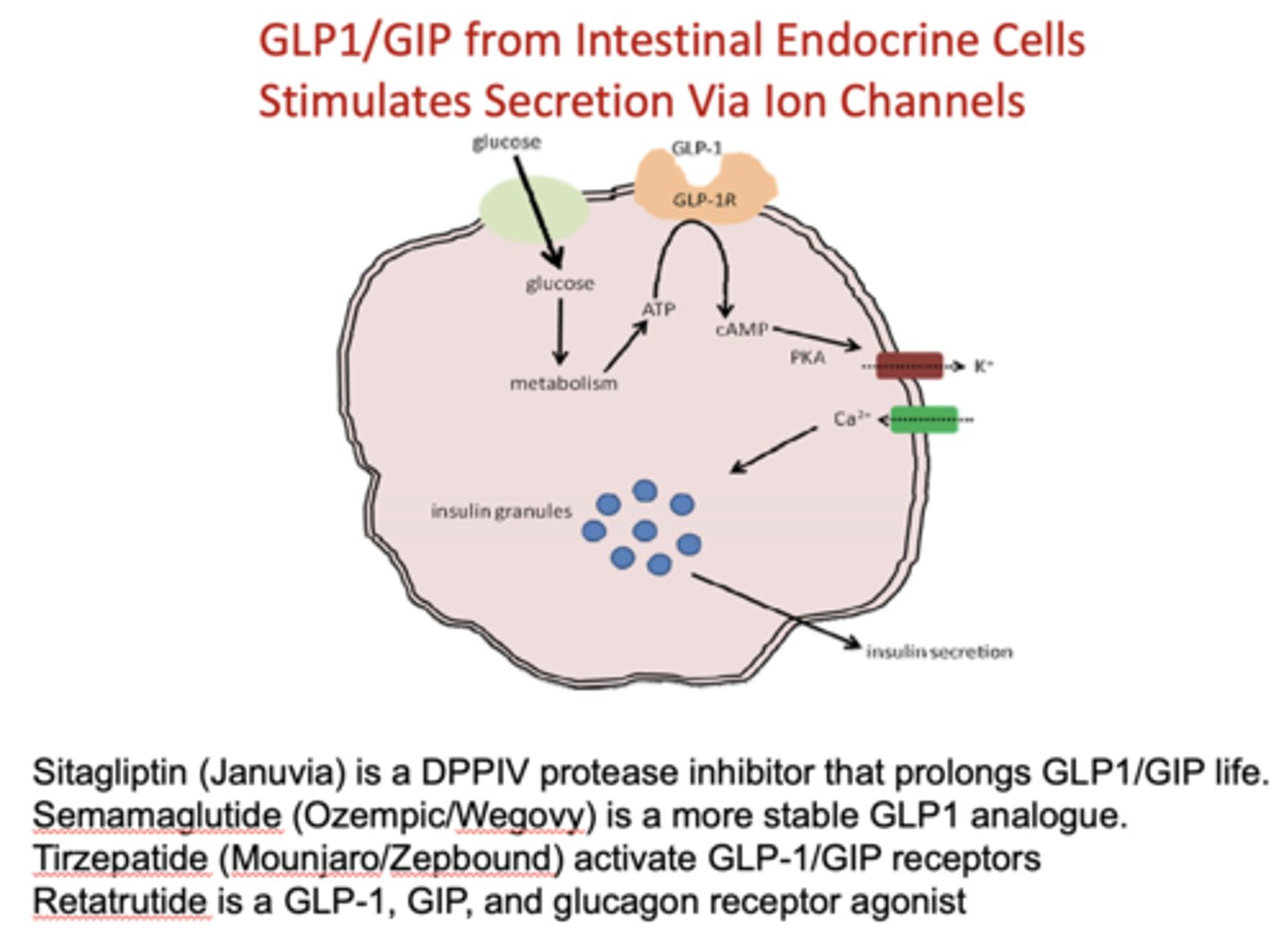
What do the following drugs work on?
- Sitagliptin (Januvia)
- Semamaglutide (Ozempic/Wegovy)
- Tirzepatide (Mounjaro/Zepbound)
- Retatrutide
GLP1/GIP
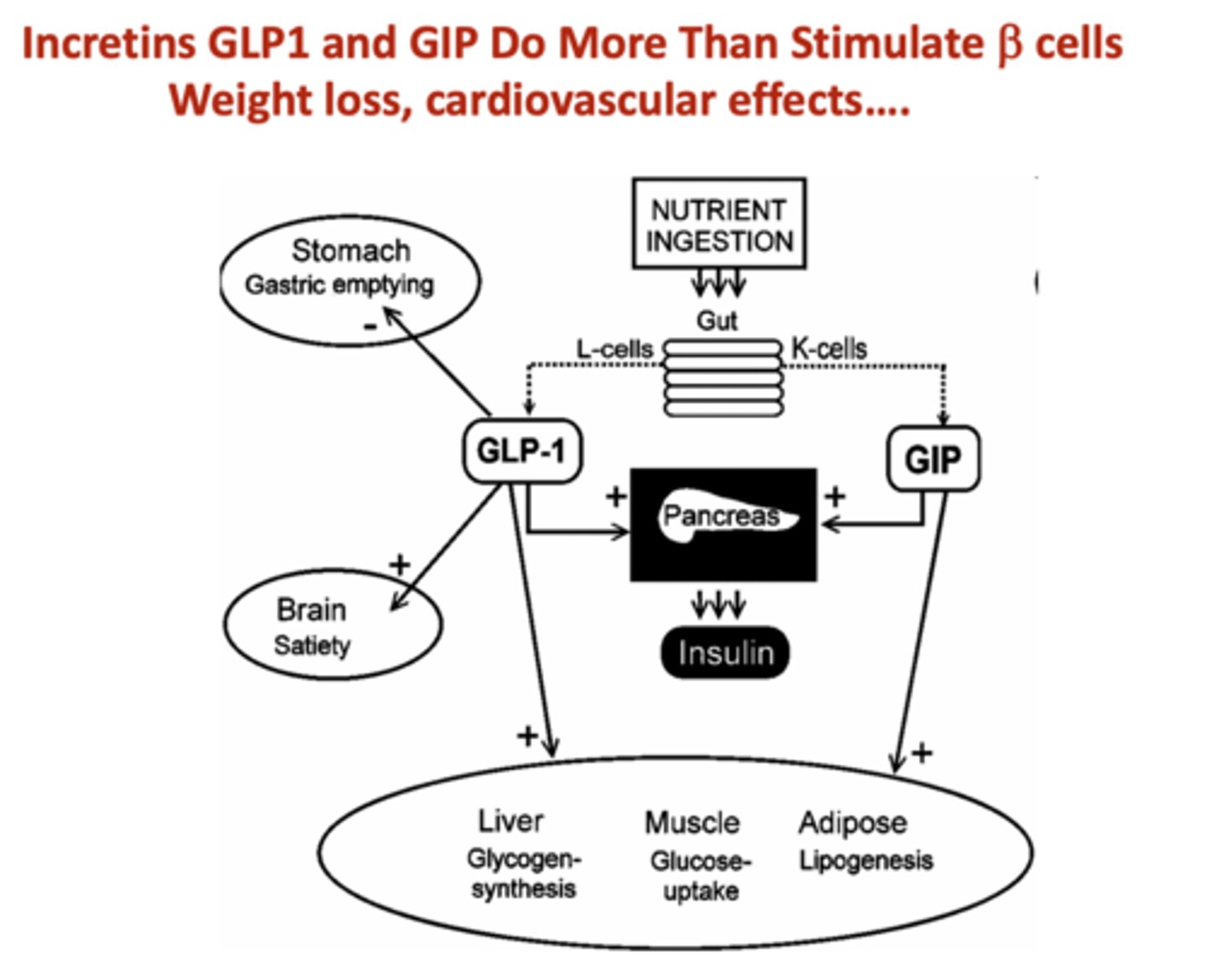
Incretins GLP1 and GIP do more than stimulate beta cells, including what?
- Slow gastric emptying
- Reduce appetite signals to brain
- Slow carbohydrate absorption (decrease glycemic index)
Insulin is released from beta cells as a response to what?
High blood glucose (high glucokinase) or incretins (GLP1, GIP) that affect K+ channels
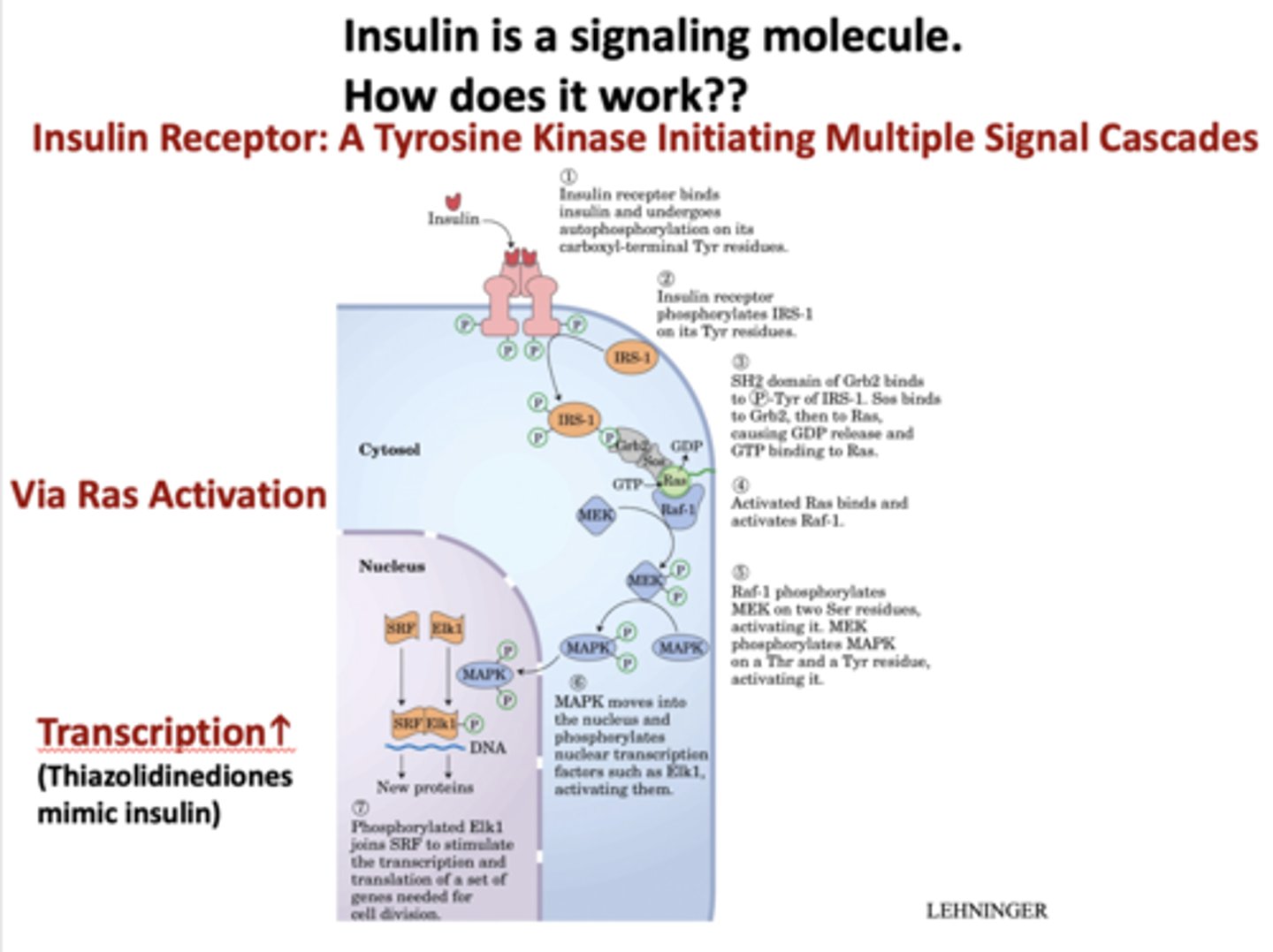
When insulin binds to a cell, what type of receptor does it bind to?
tyrosine kinase on cell surface
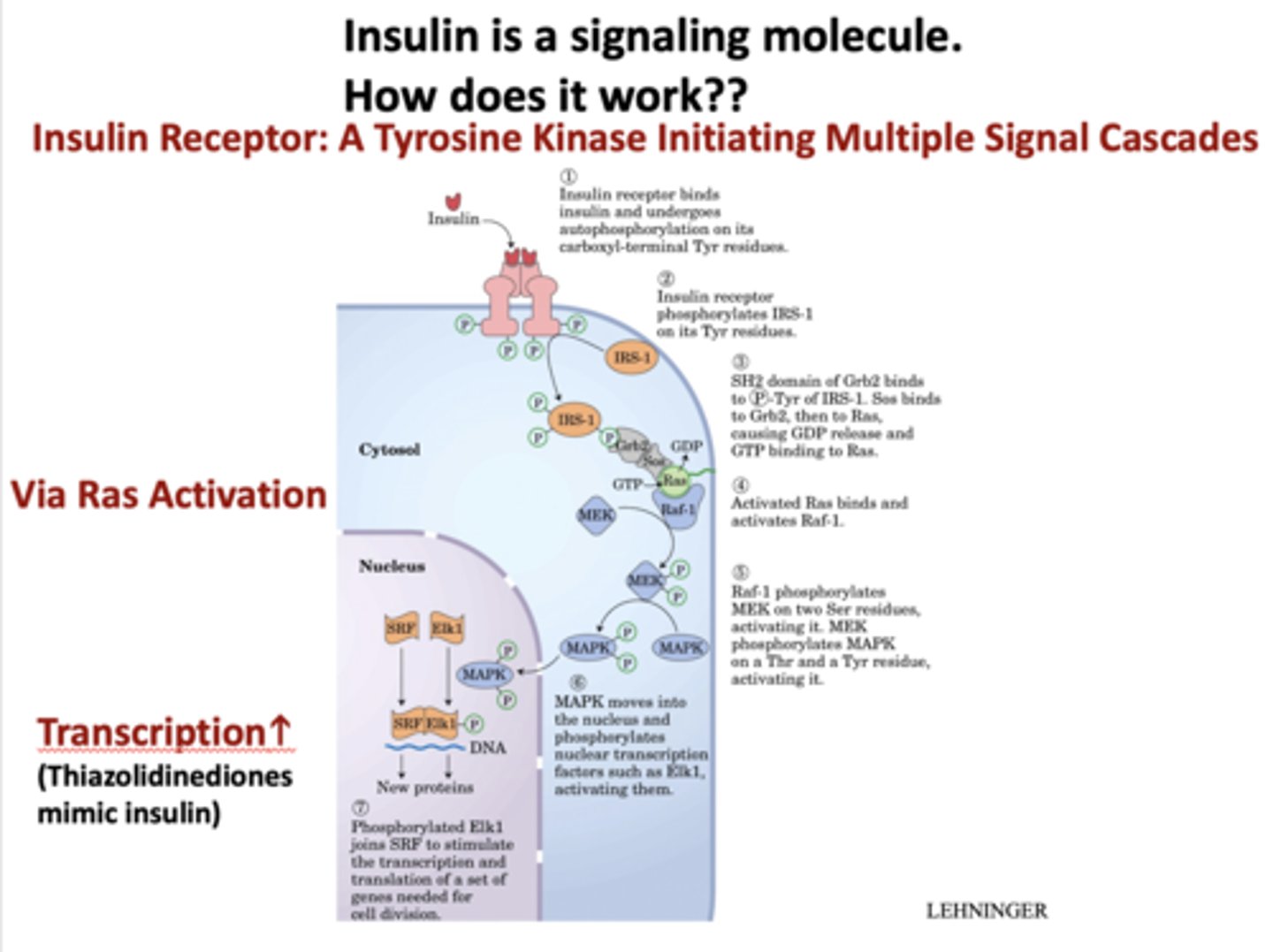
What does the insulin receptor set off?
signaling cascade (IRs, Grb2, Ras, Raf-1, MAPK, PI3 kinase)
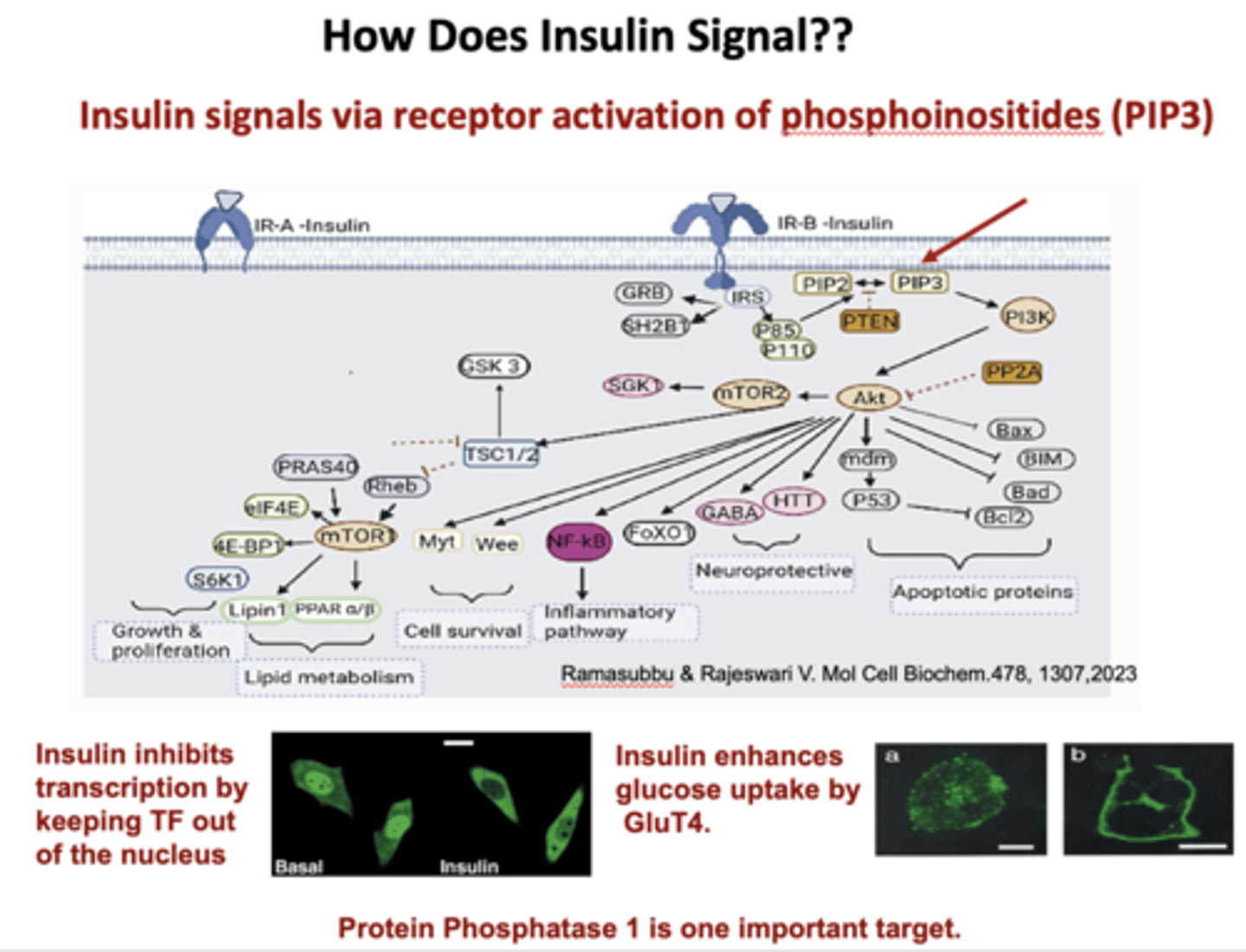
How does insulin signal?
via receptor activation of phosphoinositides (PIP3)
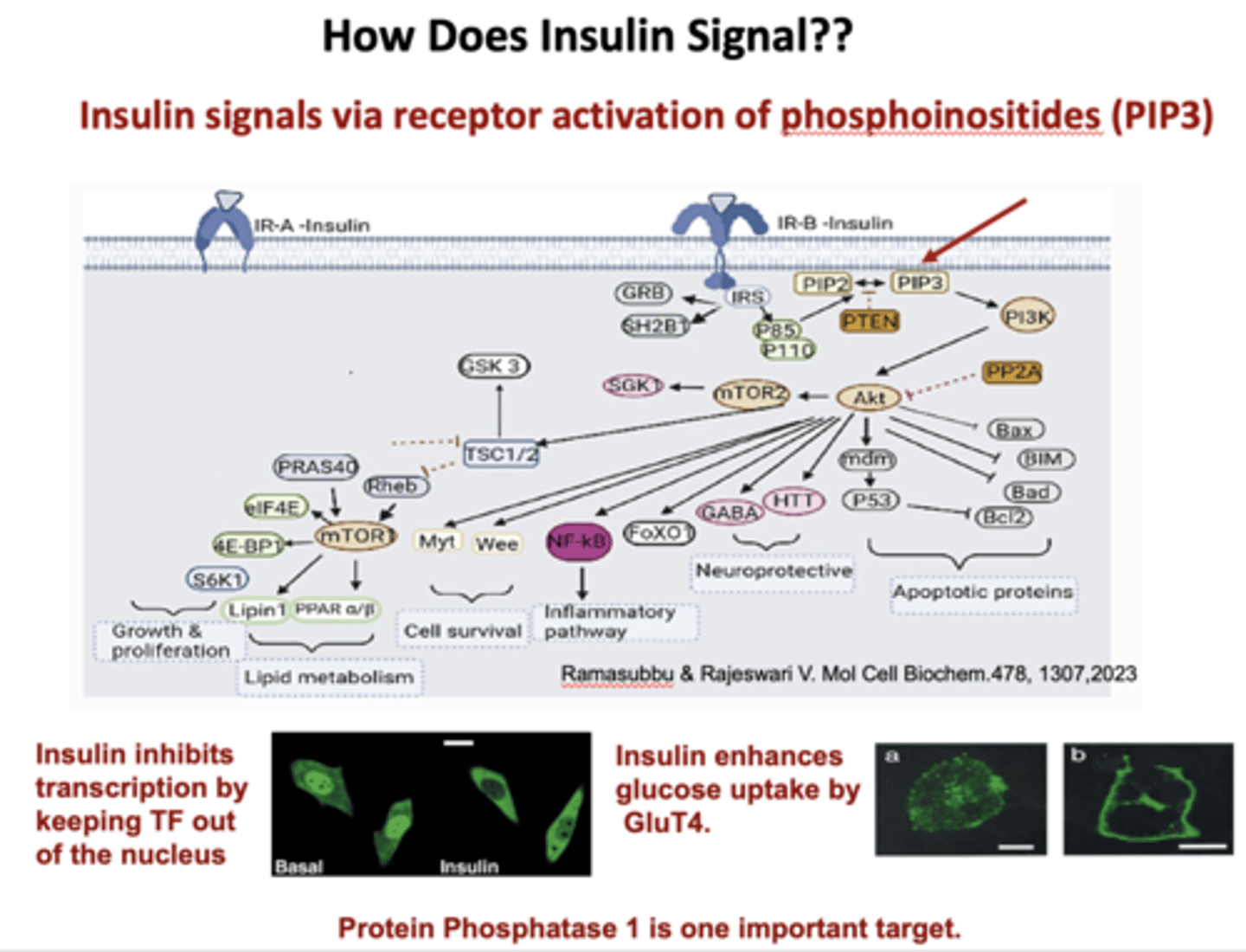
Insulin inhibits transcription by keeping __________ out of the nucleus
Transcription factor
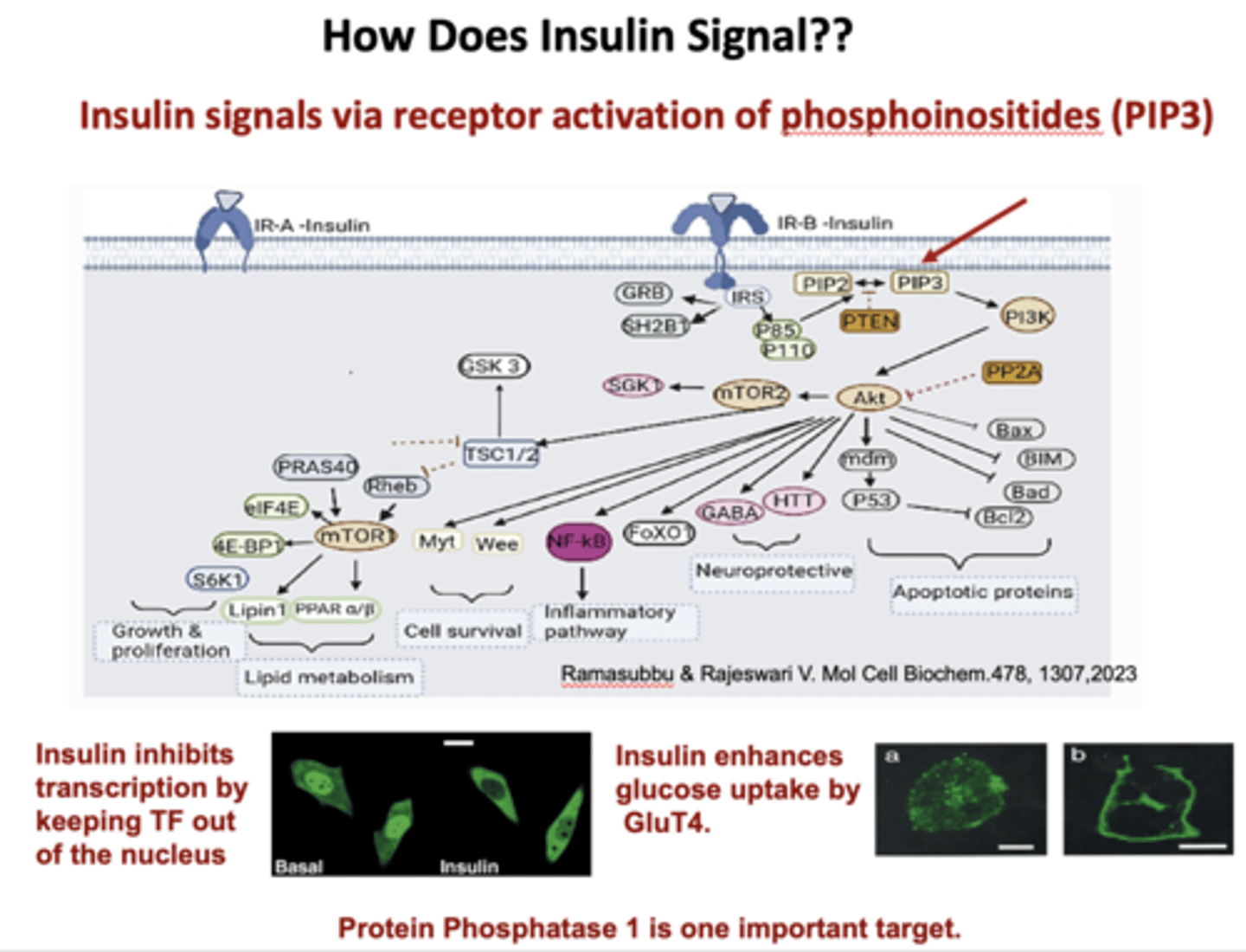
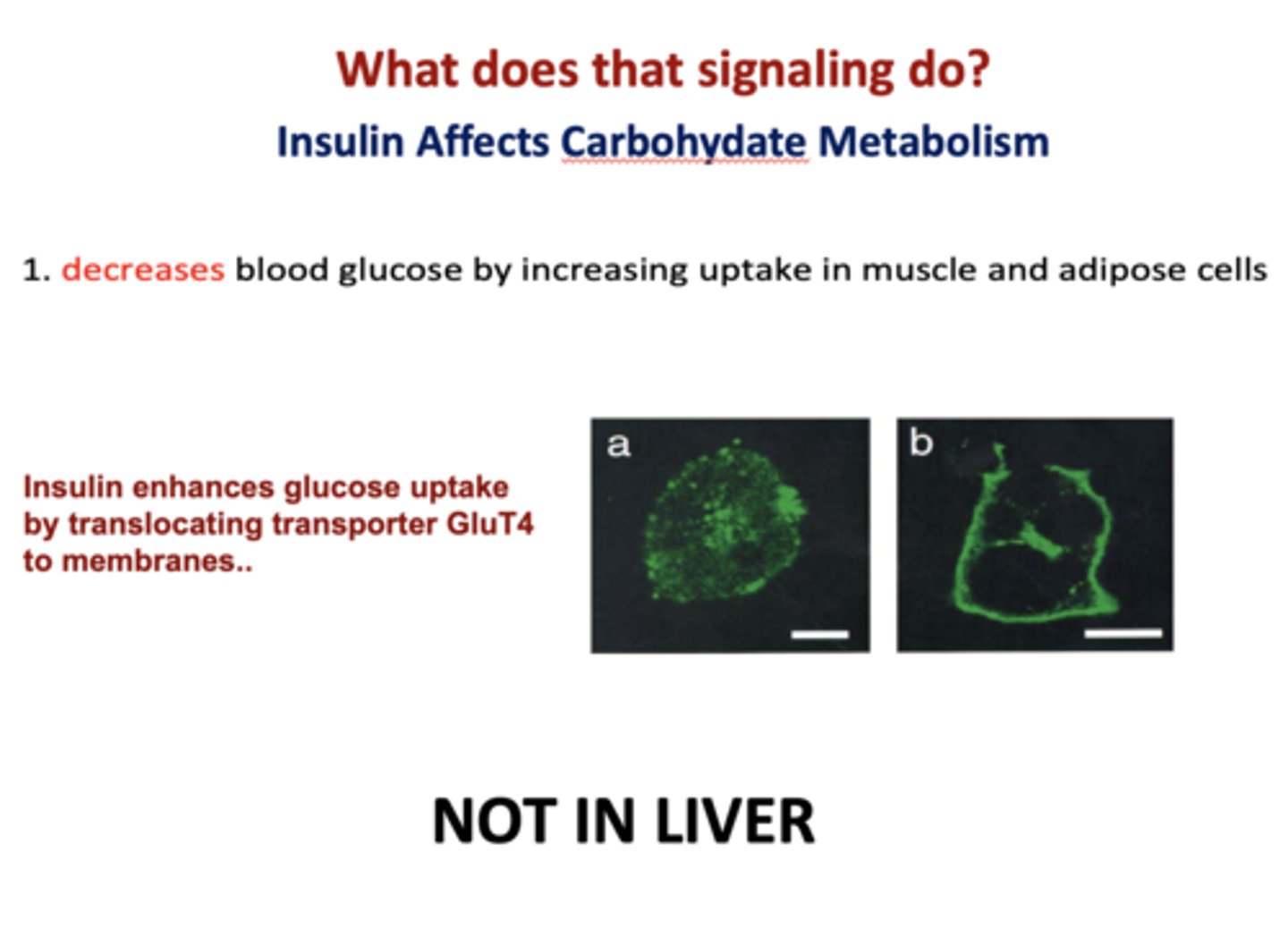
Insulin enhances glucose uptake via _______ in adipose and white cells
GluT4
Insulin decreases blood glucose by increasing uptake where?
Muscle and adipose cells
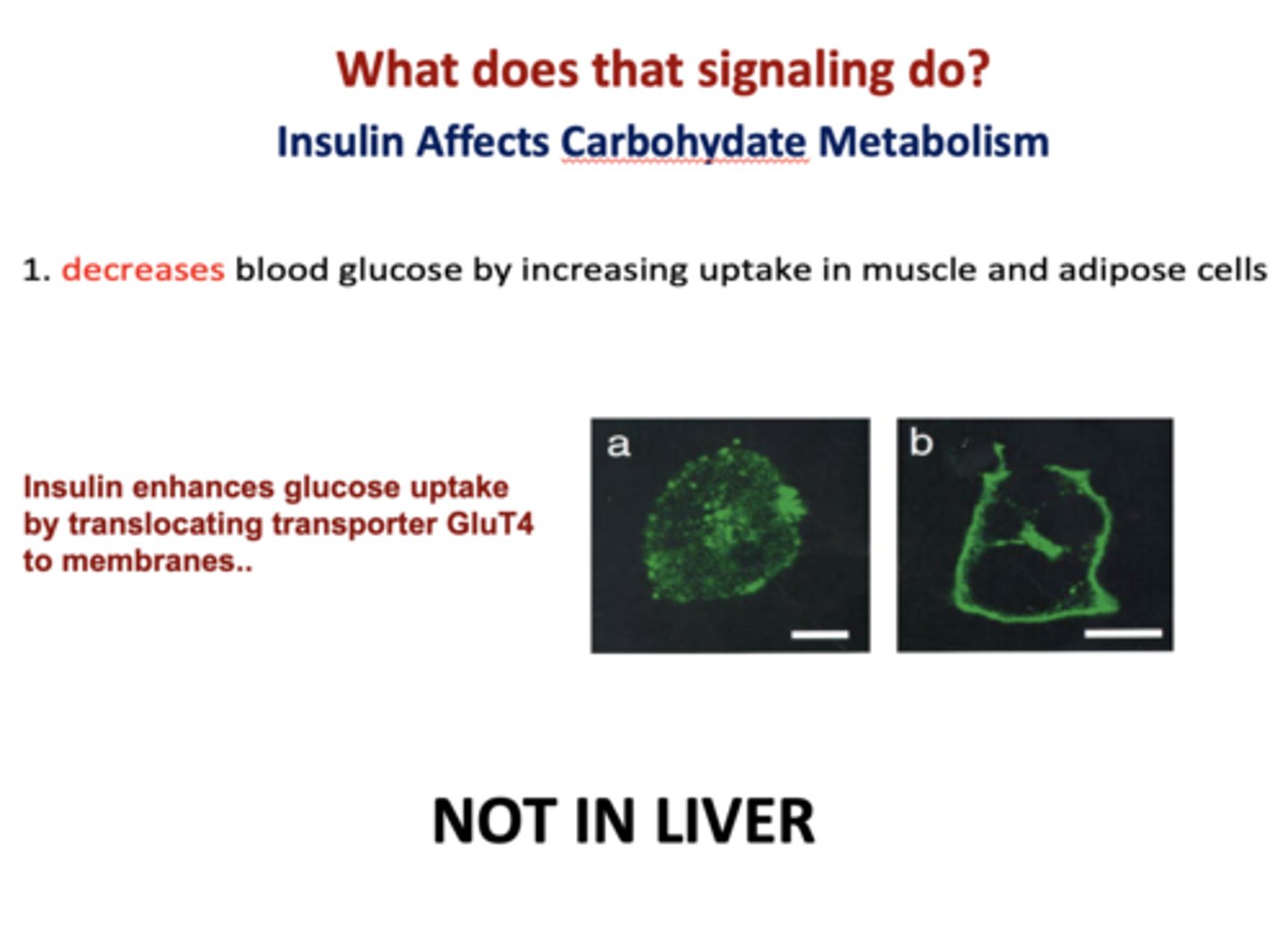
T/F: insulin decreases blood glucose by increasing uptake in liver cells
false (NOT IN LIVER)
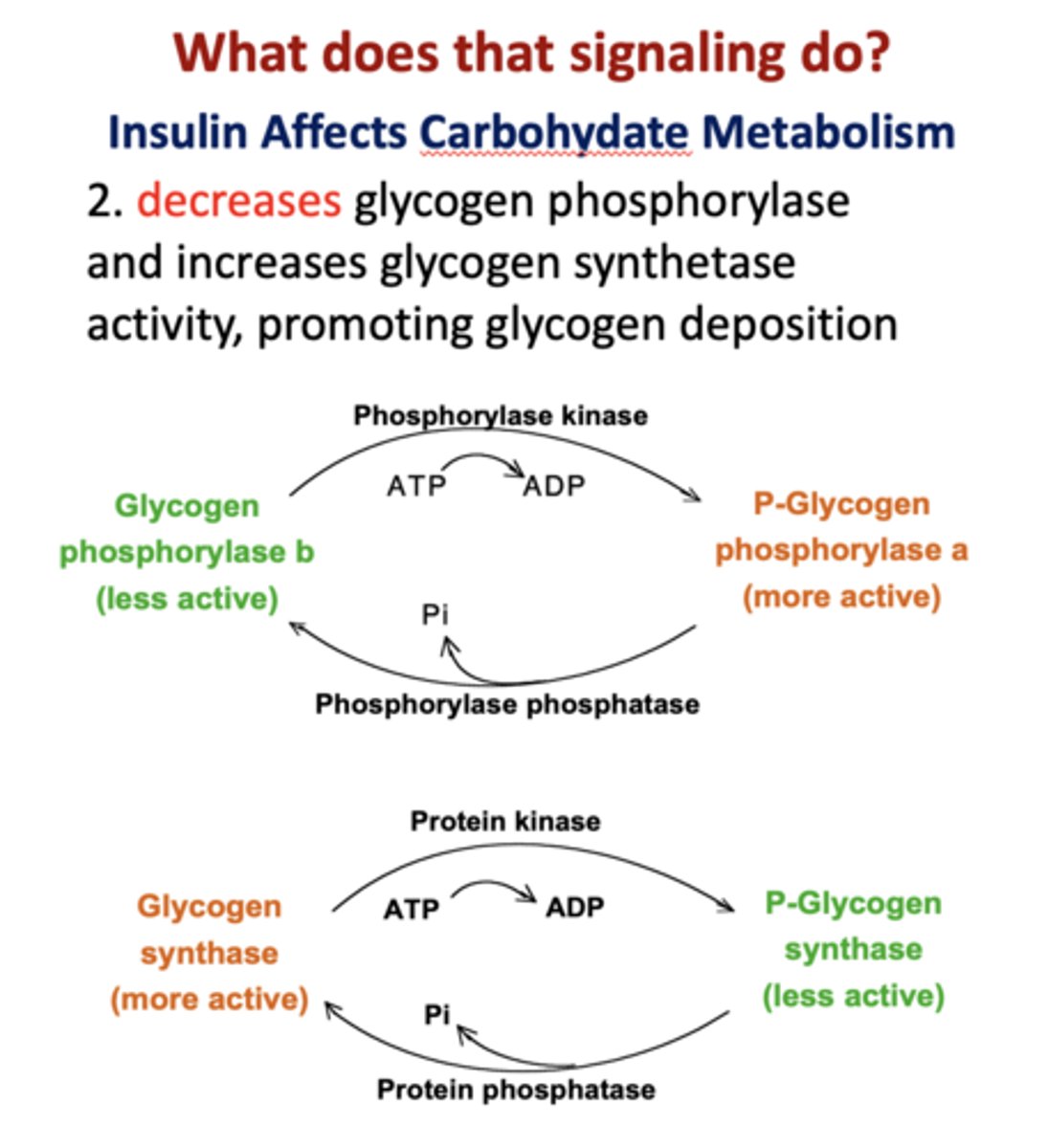
Insulin promotes glucose storage as glycogen by ________ glycogen synthase and _________ glycogen phosphorylase
activating, inhibiting
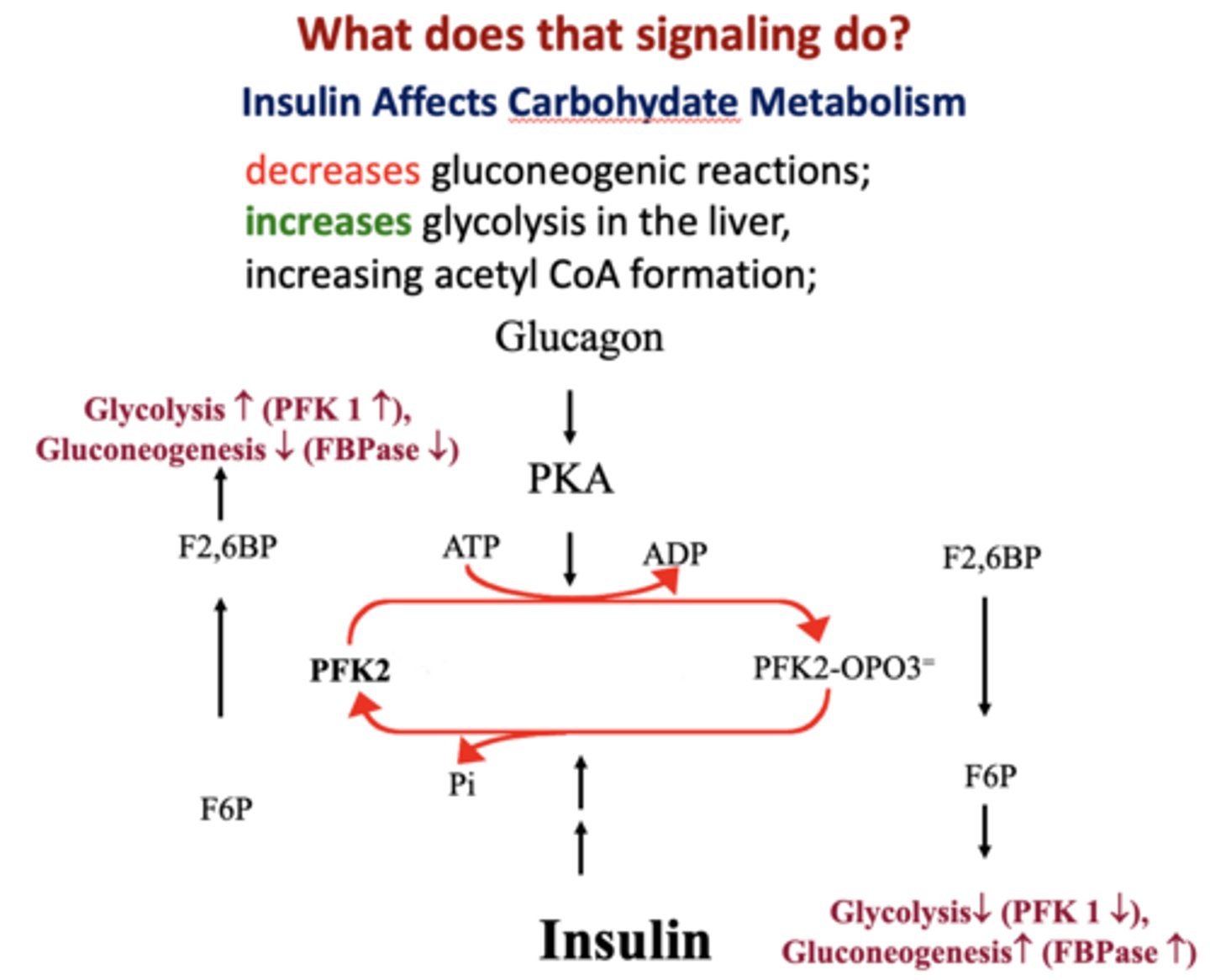
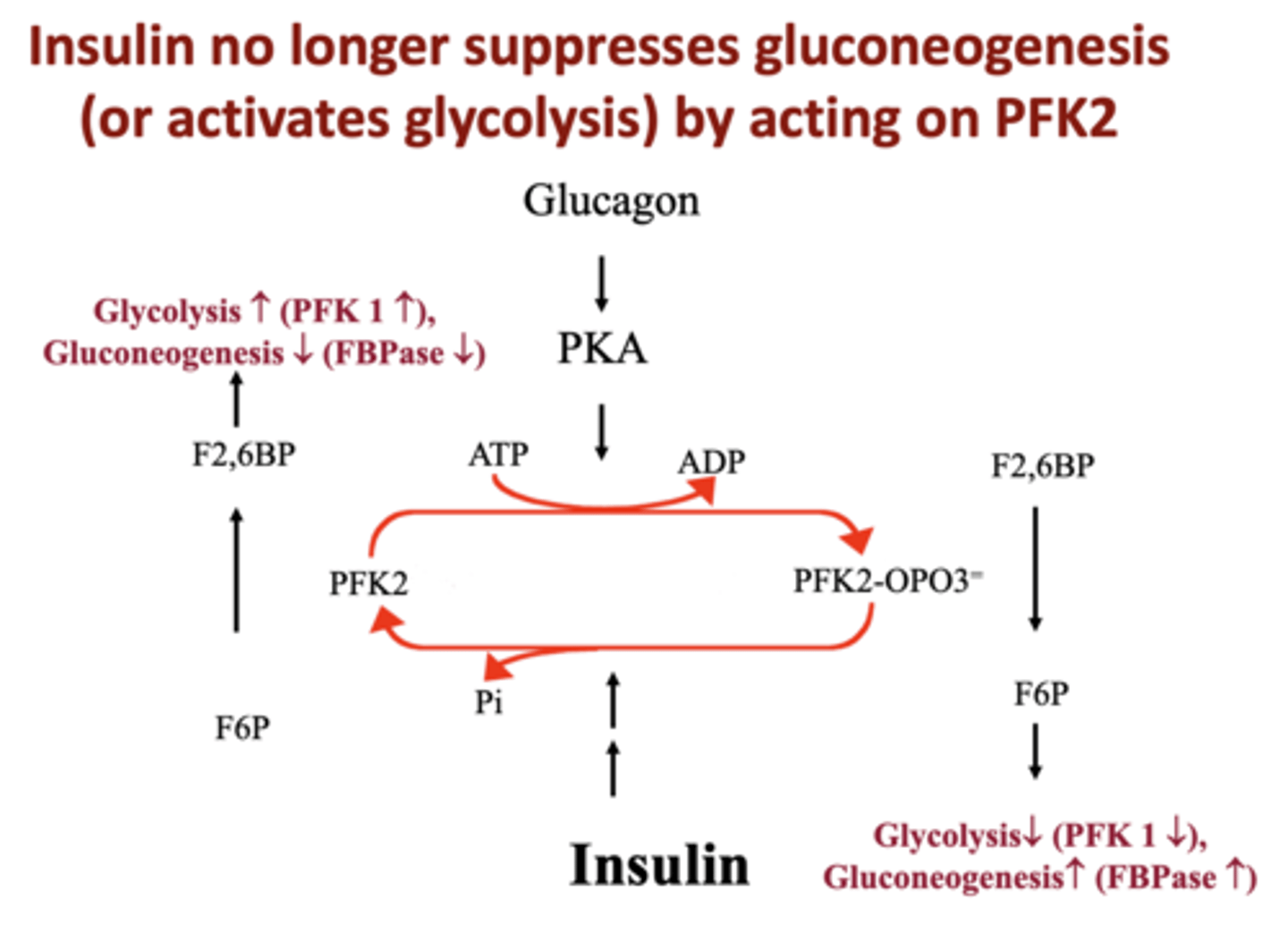
Insulin promotes glycolysis by affecting ______
PFK2
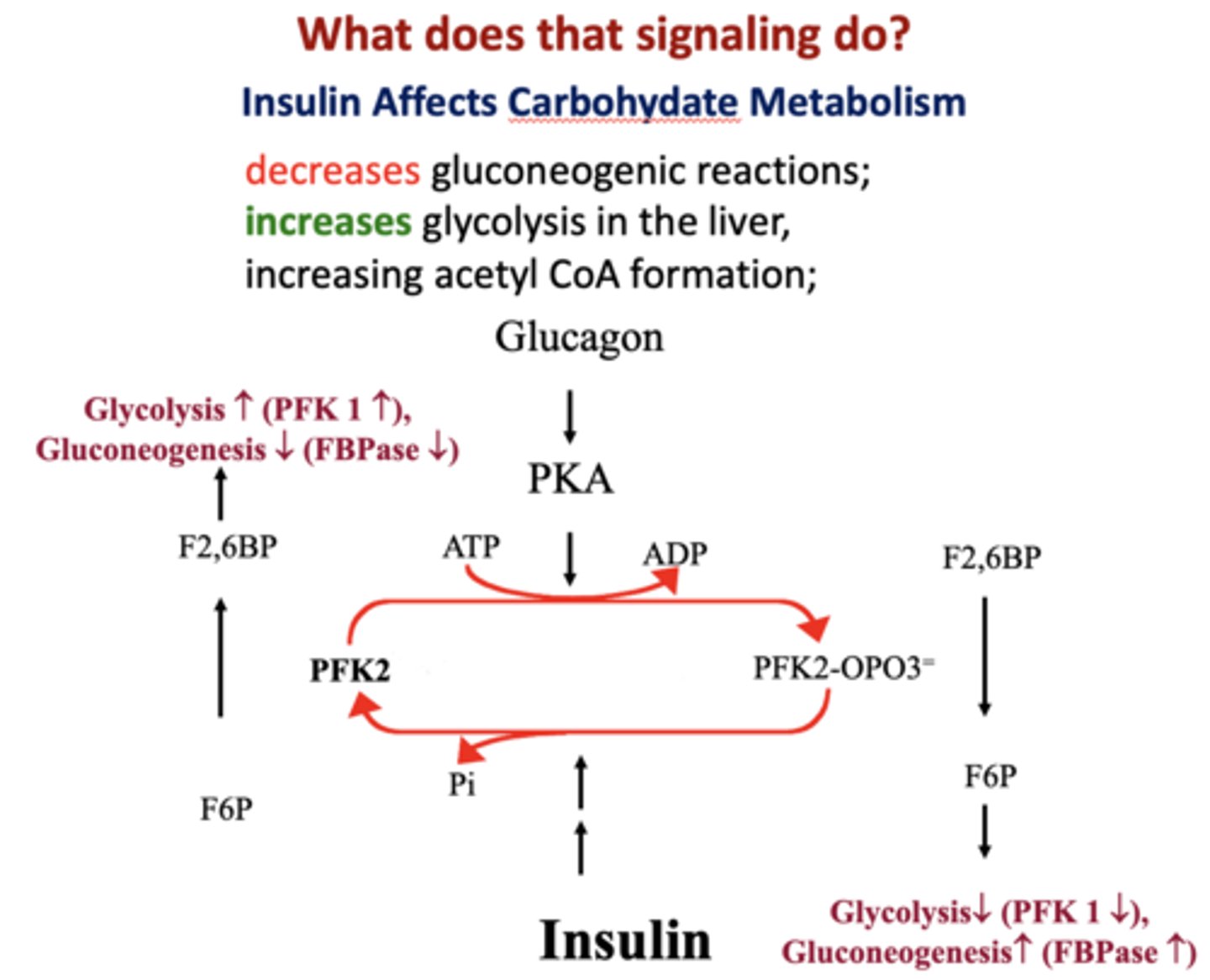
Insulin limits gluconeogenesis by affecting ___________ and ___________
- PFK2
- Pyruvate kinase
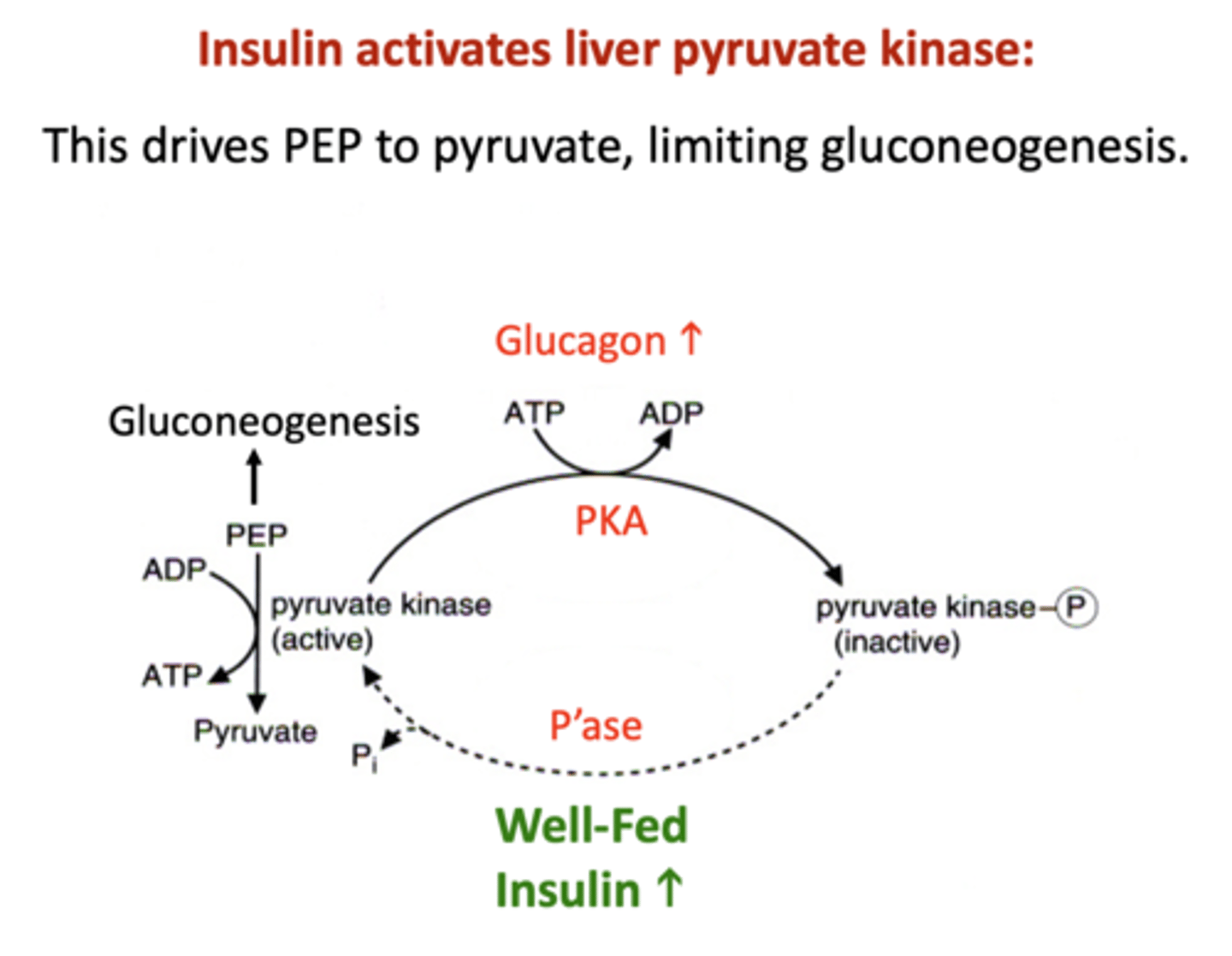
Insulin ______ gluconeogenic reactions and _______ glycolysis in the liver
decreases, increases
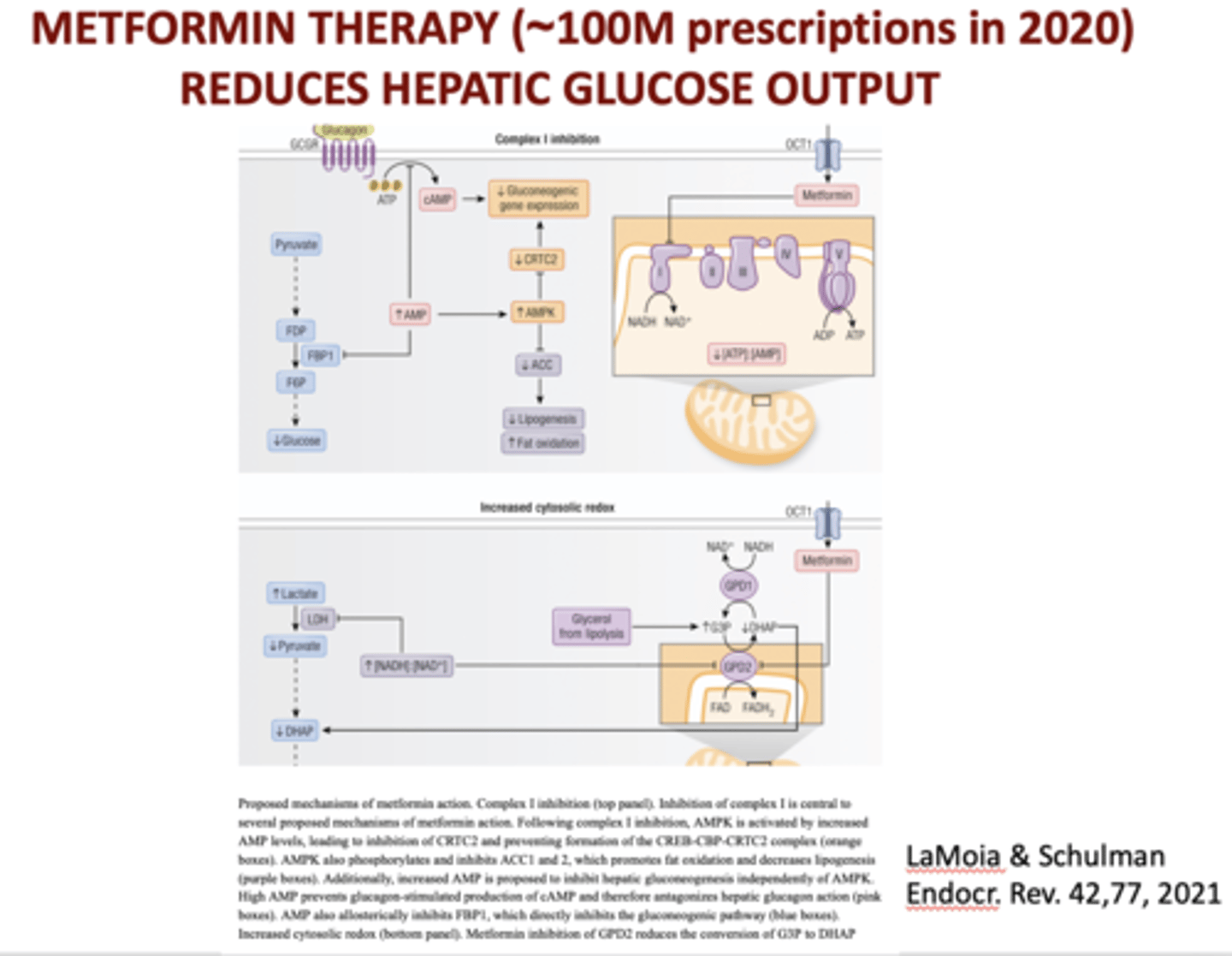
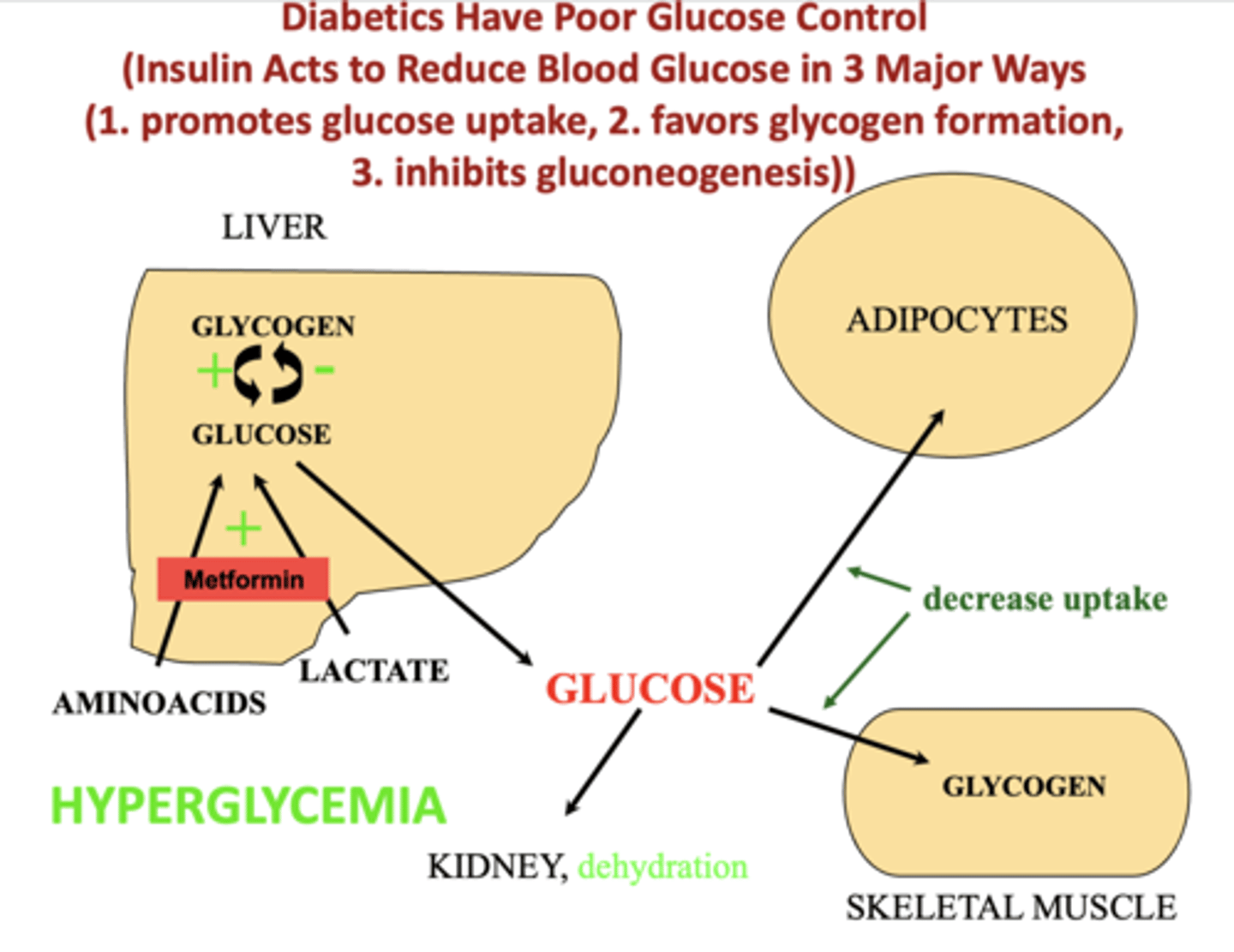
What therapy reduces hepatic glucose output?
Metformin
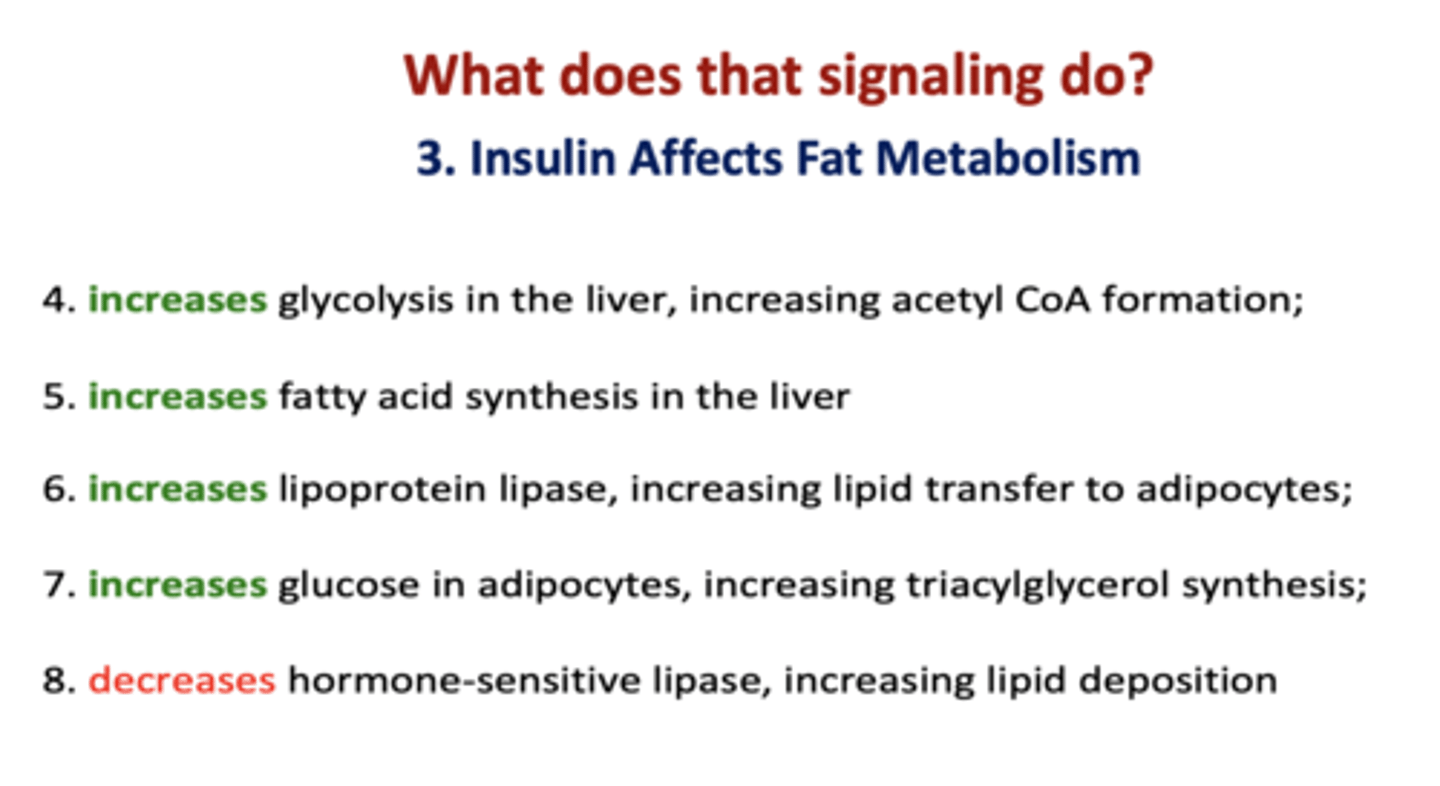
Insulin increases glycolysis in the liver, ___________ acetyl CoA formation
increasing
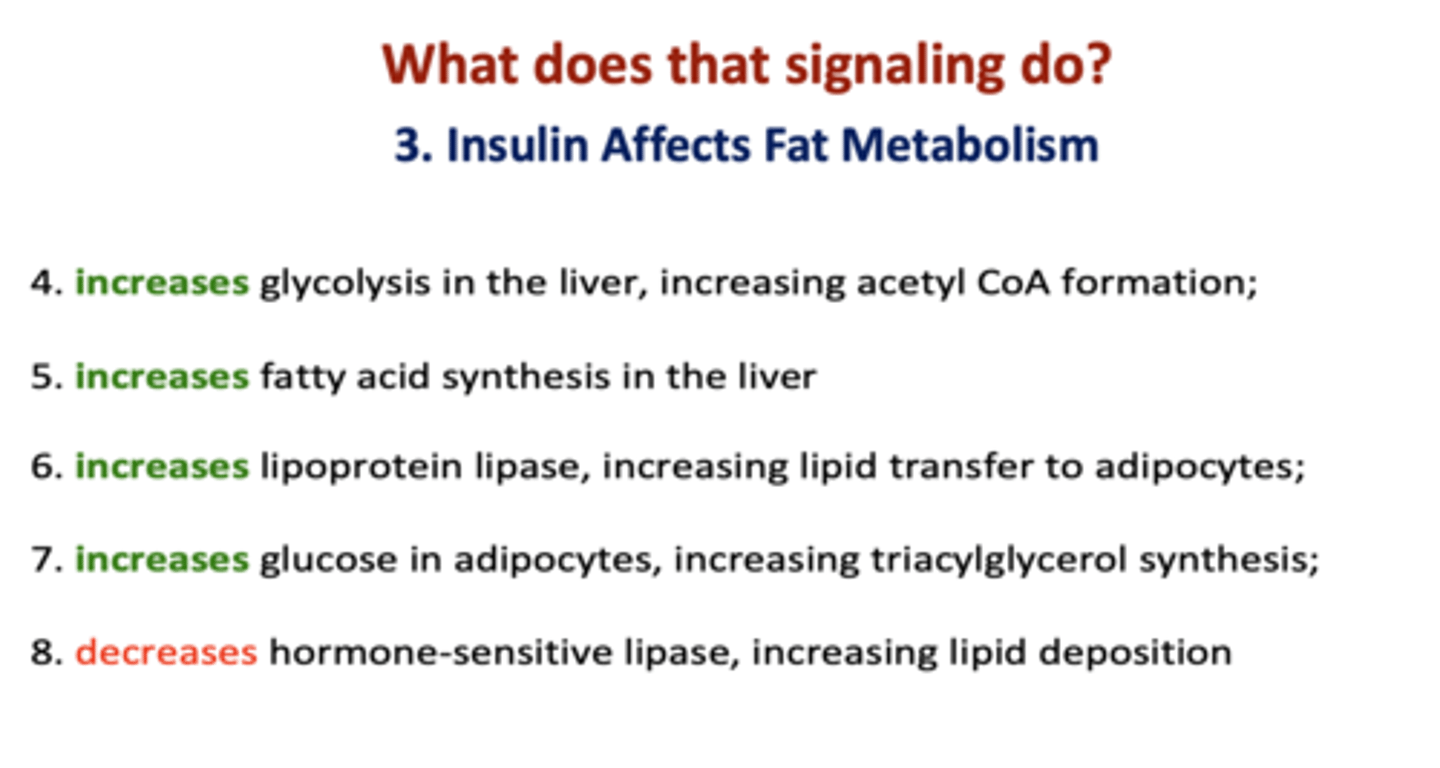
Insulin stimulates fatty acid _________
synthesis
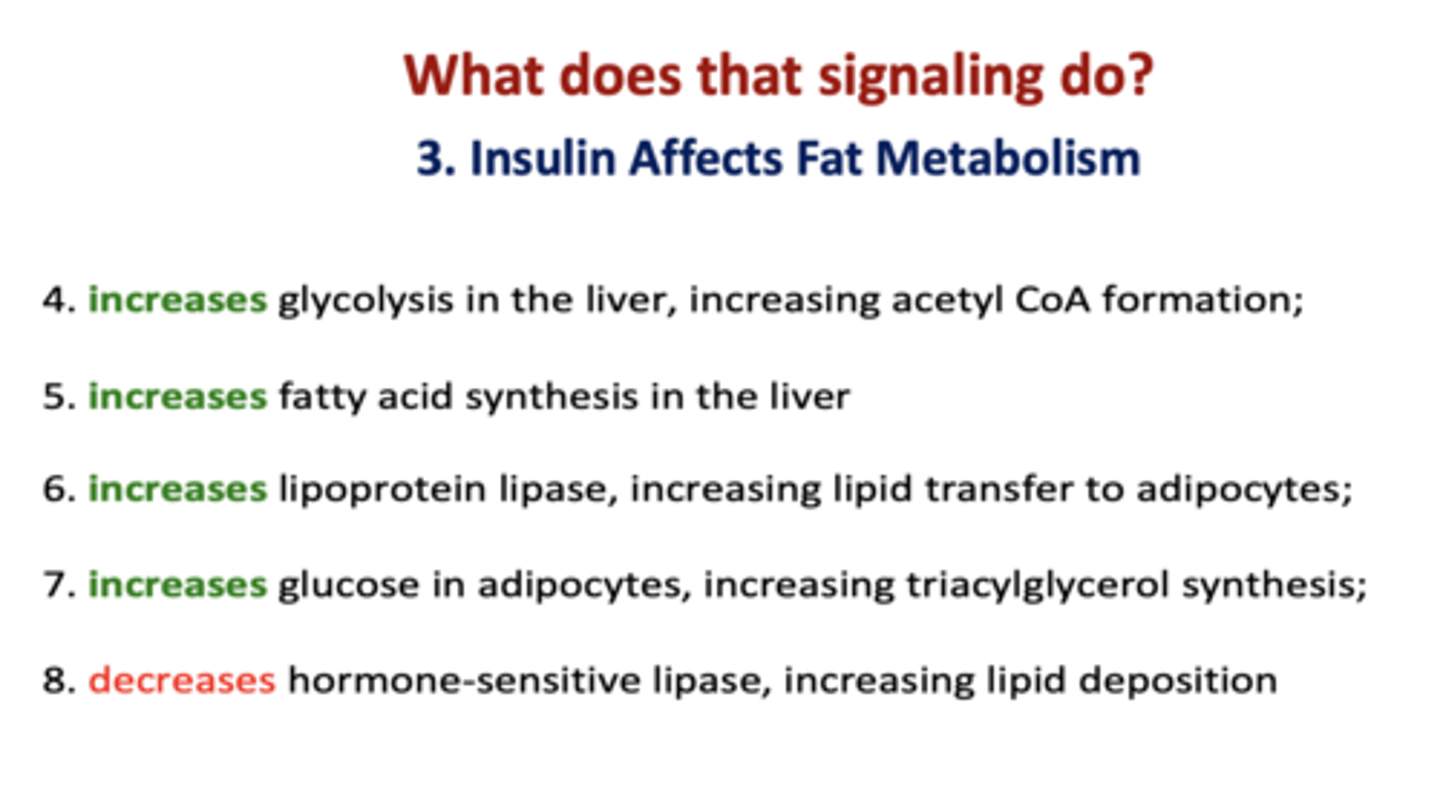
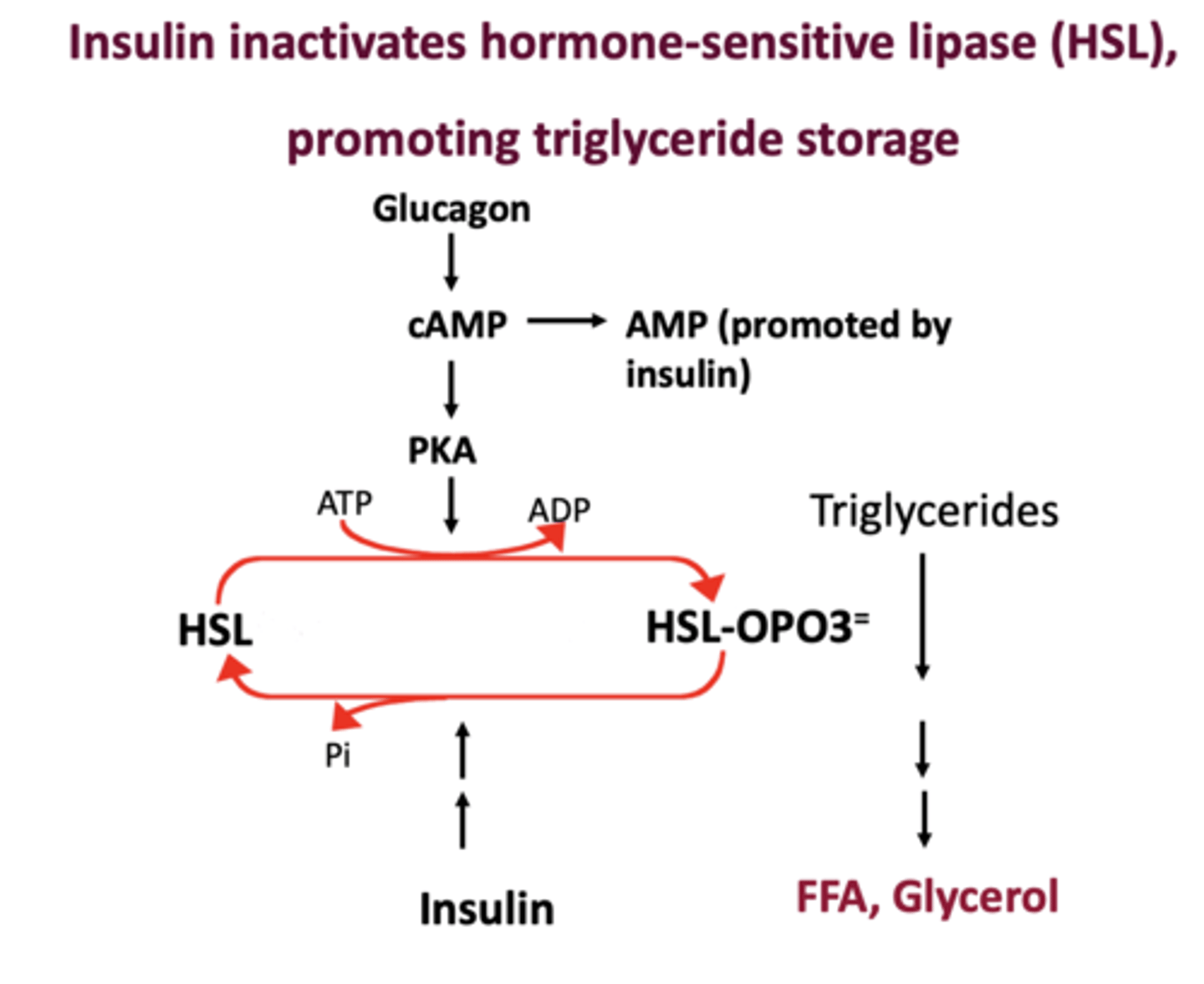
Insulin _________ hormone-sensitive lipase, increasing lipid deposition
Decreases
Insulin inhibits __________, promoting triglyceride storage.
hormone sensitive lipase
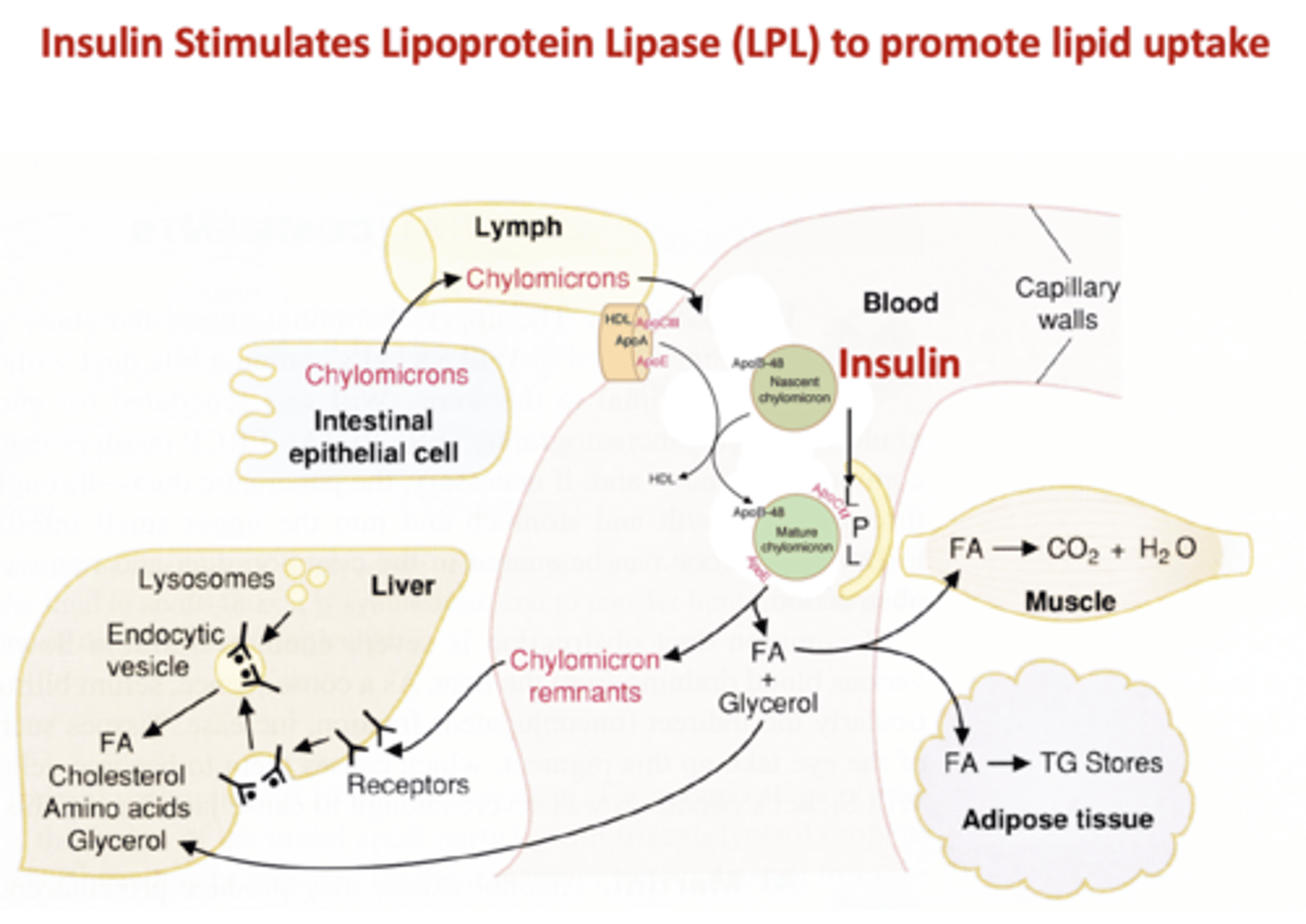
Insulin _______ lipoprotein lipase (LPL) to promote lipid uptake
Stimulates
Type 1 or Type 2?
Lack B cell function, but respond normally to insulin. It can be associated with autoimmunity. Onset is typically at a young age. Ketoacidosis is common
Type 1
Insulin ____________ amino acid uptake into cells, ____________ protein degradation and ____________ protein synthesis
Increases, decreases, promotes
Where does insulin resistance come from?
1. Genetics (e.g. IRS-1 mutation)
2. Changes in free fatty acid levels
3. Proinflammatory cytokines (TNFa, IL6...)
4. Alterations in adipokines (e.g adiponectin decreases and resistin increases)
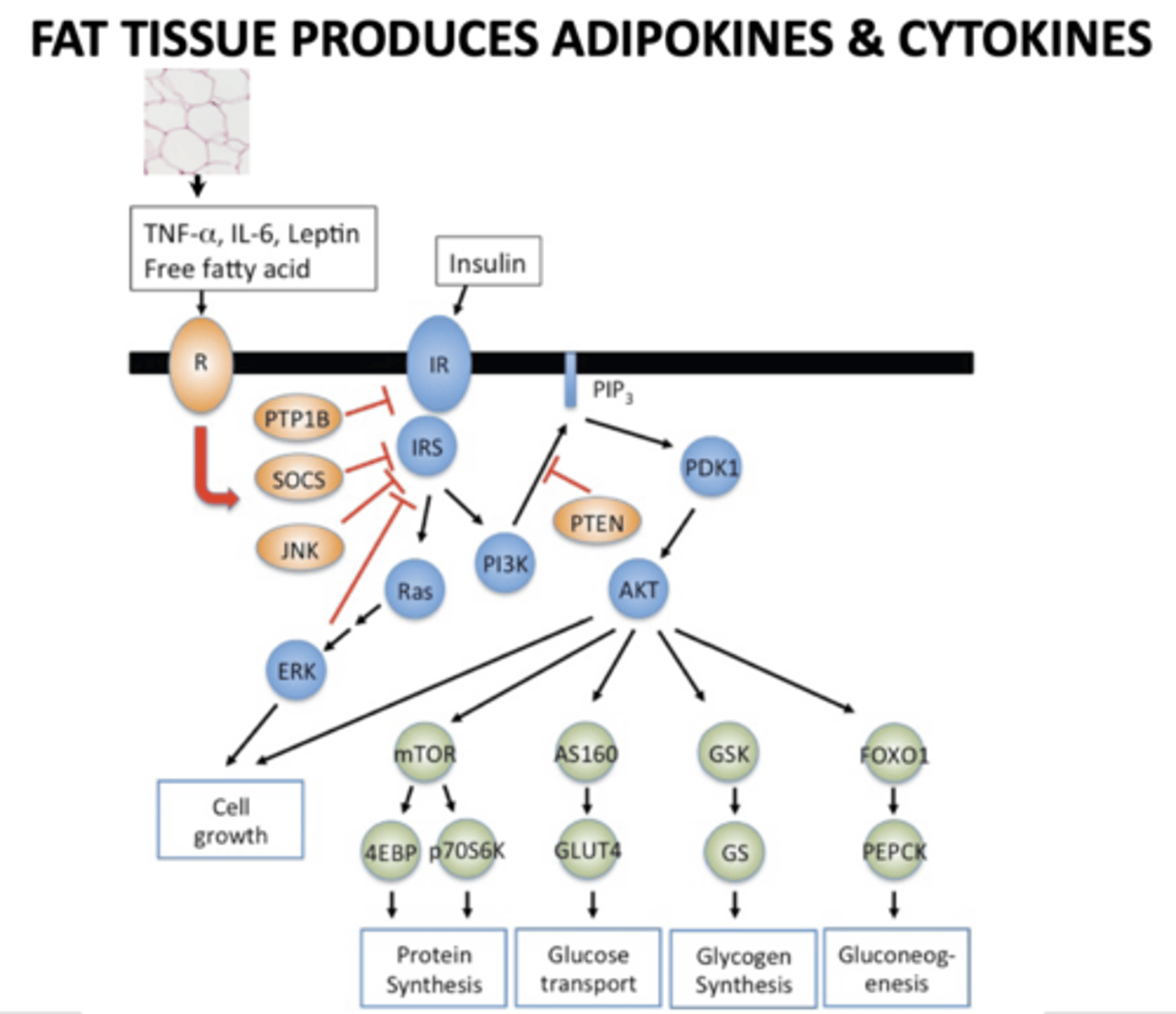
What produces adipokines and cytokines?
Fat tissue
Type 1 or Type 2?
Is a moving target. It is most often seen in older, higher BMI patients. It is characterized by problems in insulin response. Beta cell exhaustion, requiring insulin, may occur later. Hyperosmolar hyperglycemic state (HHS or) HONC is common
Type 2
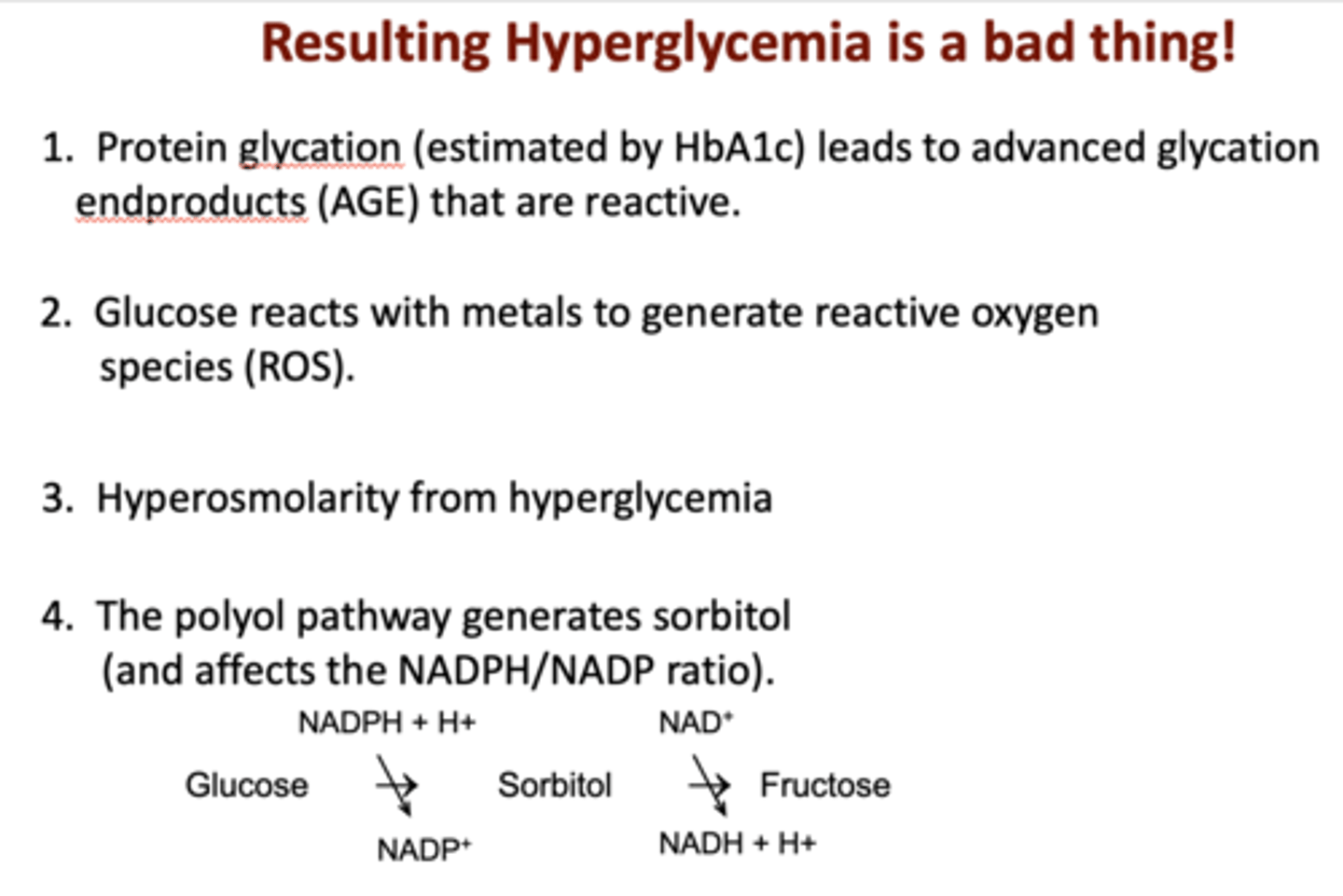
Why is hyperglycemia in diabetes a problem?
- Glucose reacts with metals (reactive oxygen species (ROS)).
- Osmotic issues (HHS, the polyol pathway generates sorbitol.)
- Hyperosmolar hyperglycemic state (HHS/HONC)
- Glycation generates protein adducts (HbA1c).
Insulin acts to reduce blood glucose in what three major ways?
1. Promotes glucose uptake
2. Favors glycogen formation
3. Inhibits gluconeogenesis
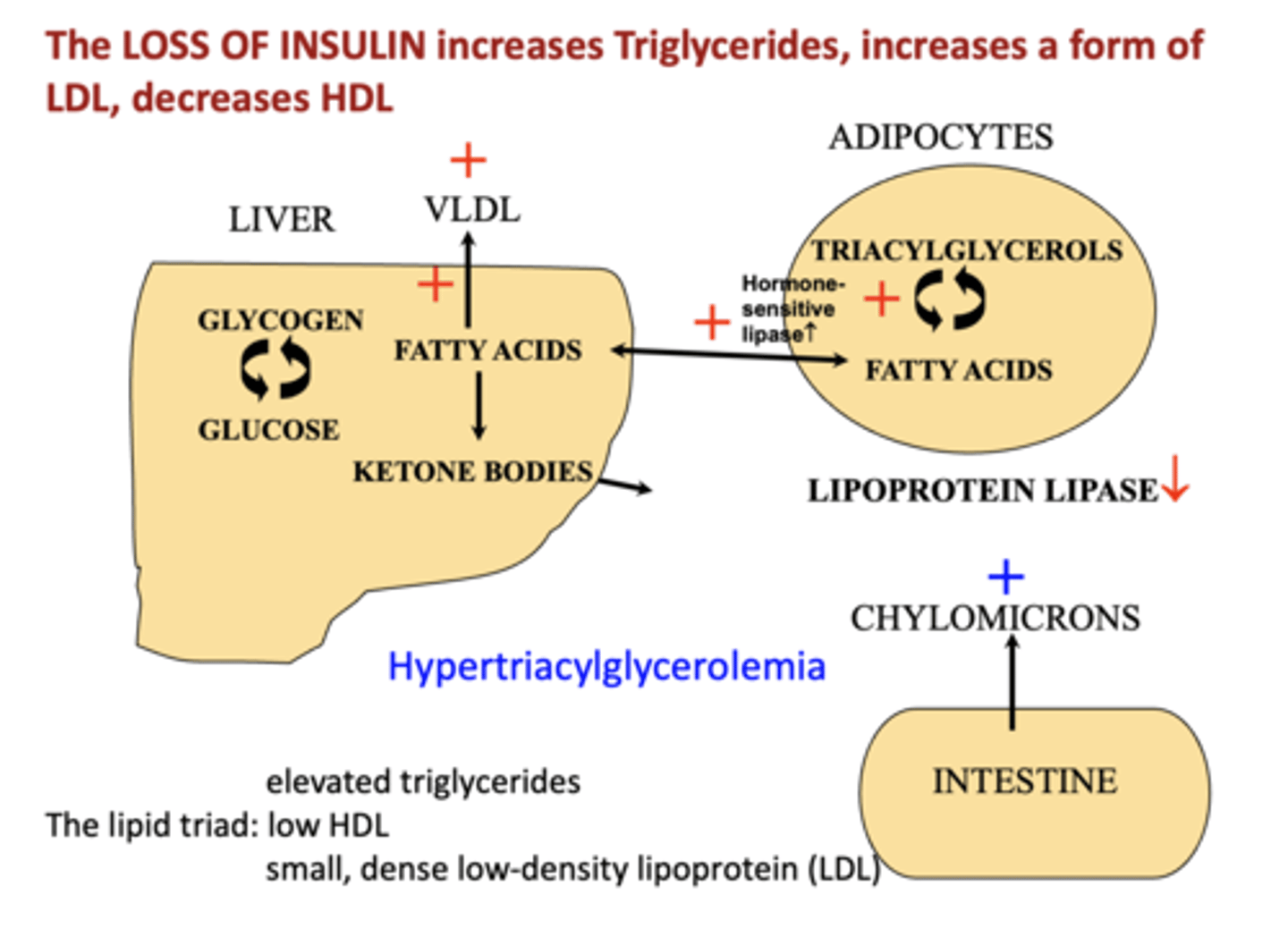
The loss of insulin has what effect on triglycerides?
increases
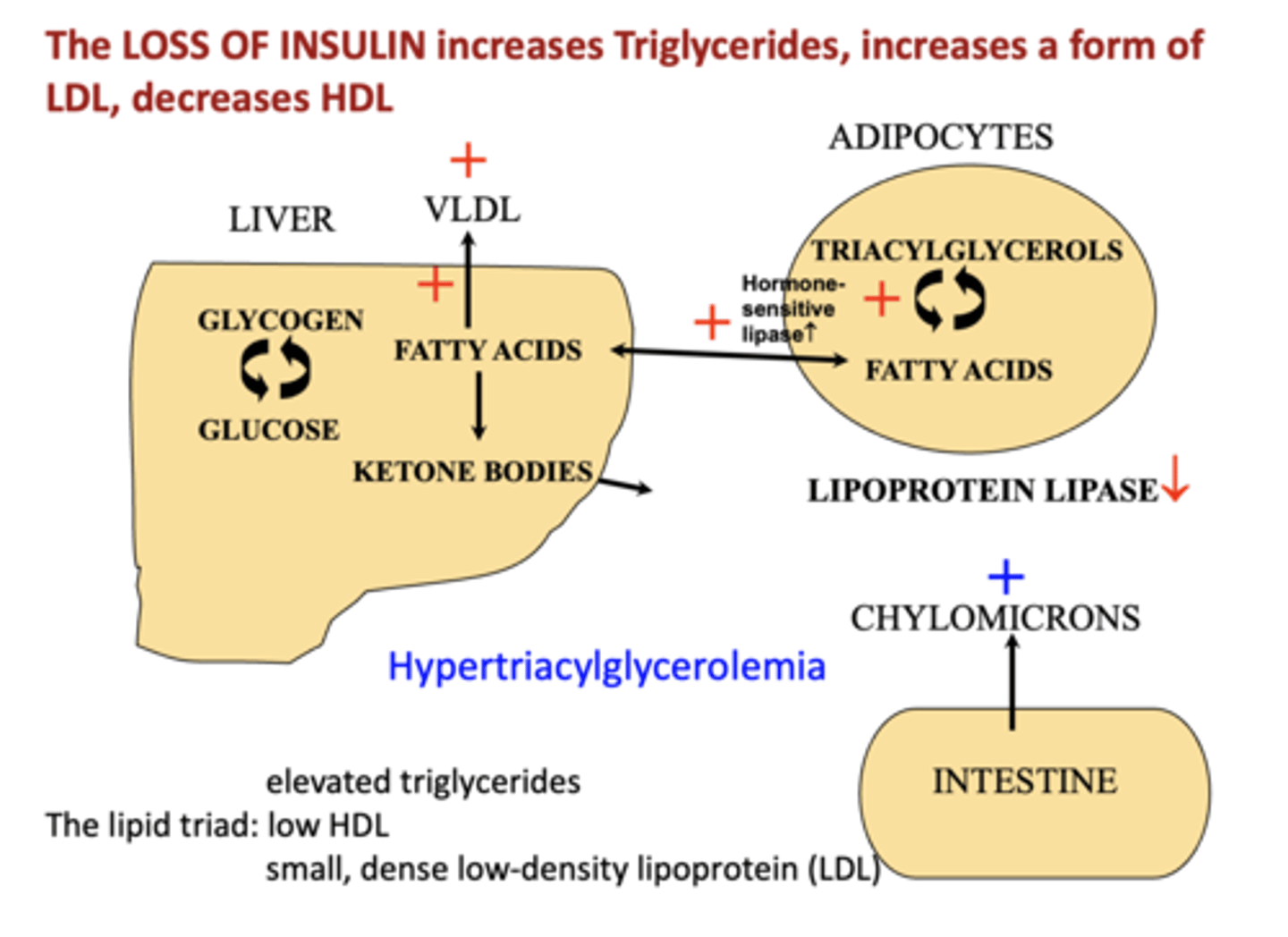
The loss of insulin has what effect on LDL?
increases
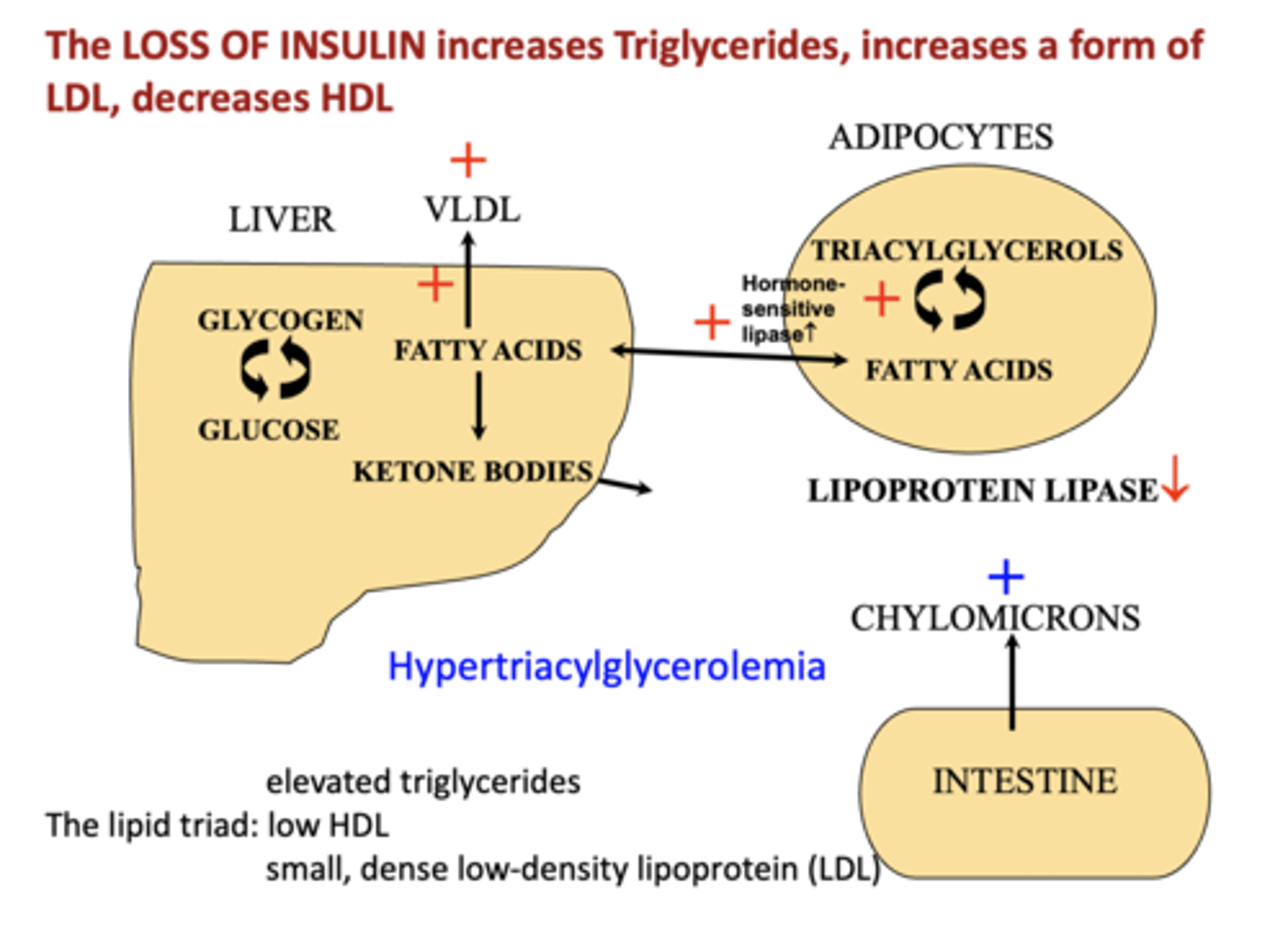
The loss of insulin has what effect on HDL?
decreases
Insulin no longer suppresses gluconeogenesis (or activates glycolysis) by acting on __________
PFK2
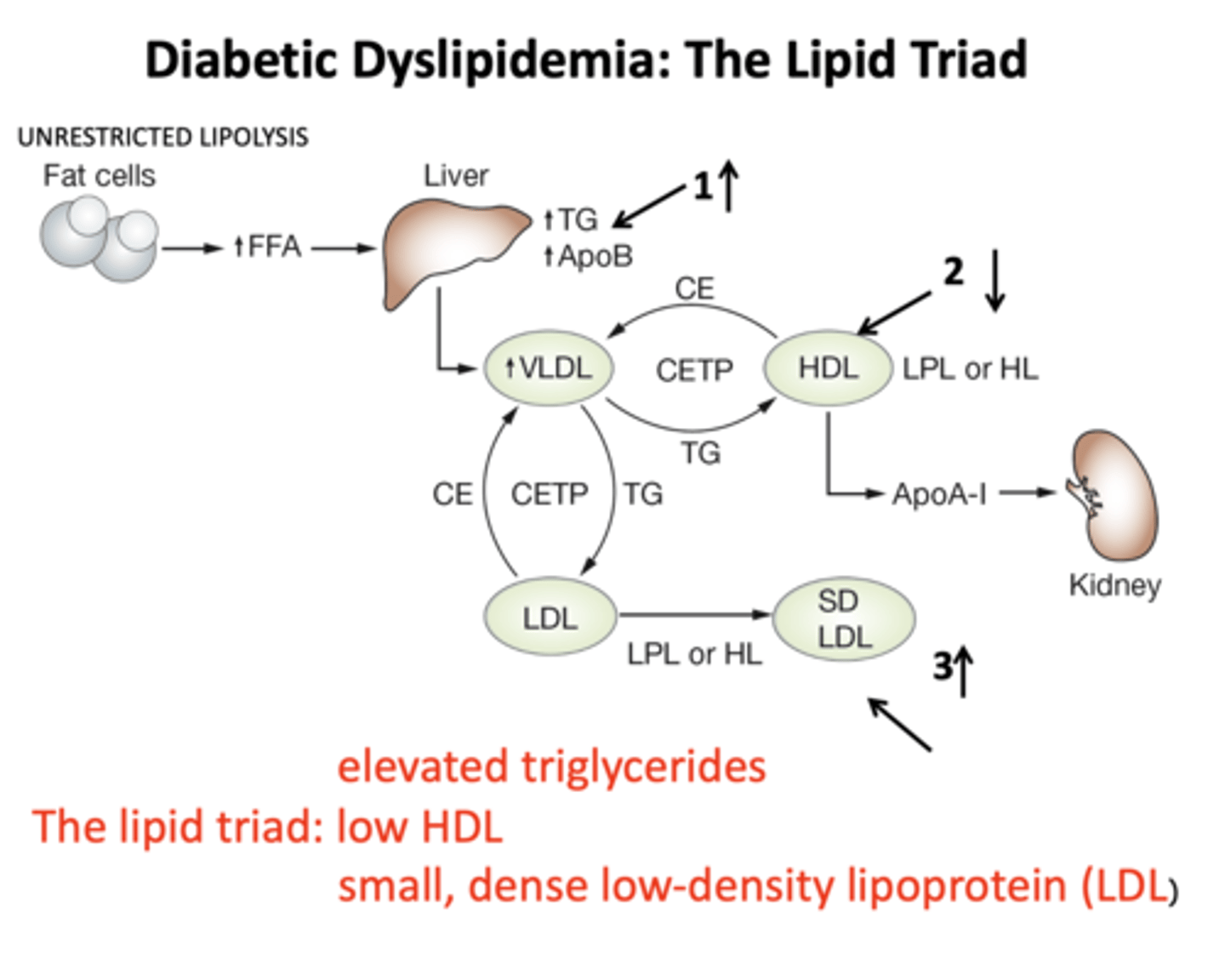
The lipid triad is composed of:
_______ triglycerides,
_______ LDL,
_______ HDL
high triglycerides
high LDL
low HDL
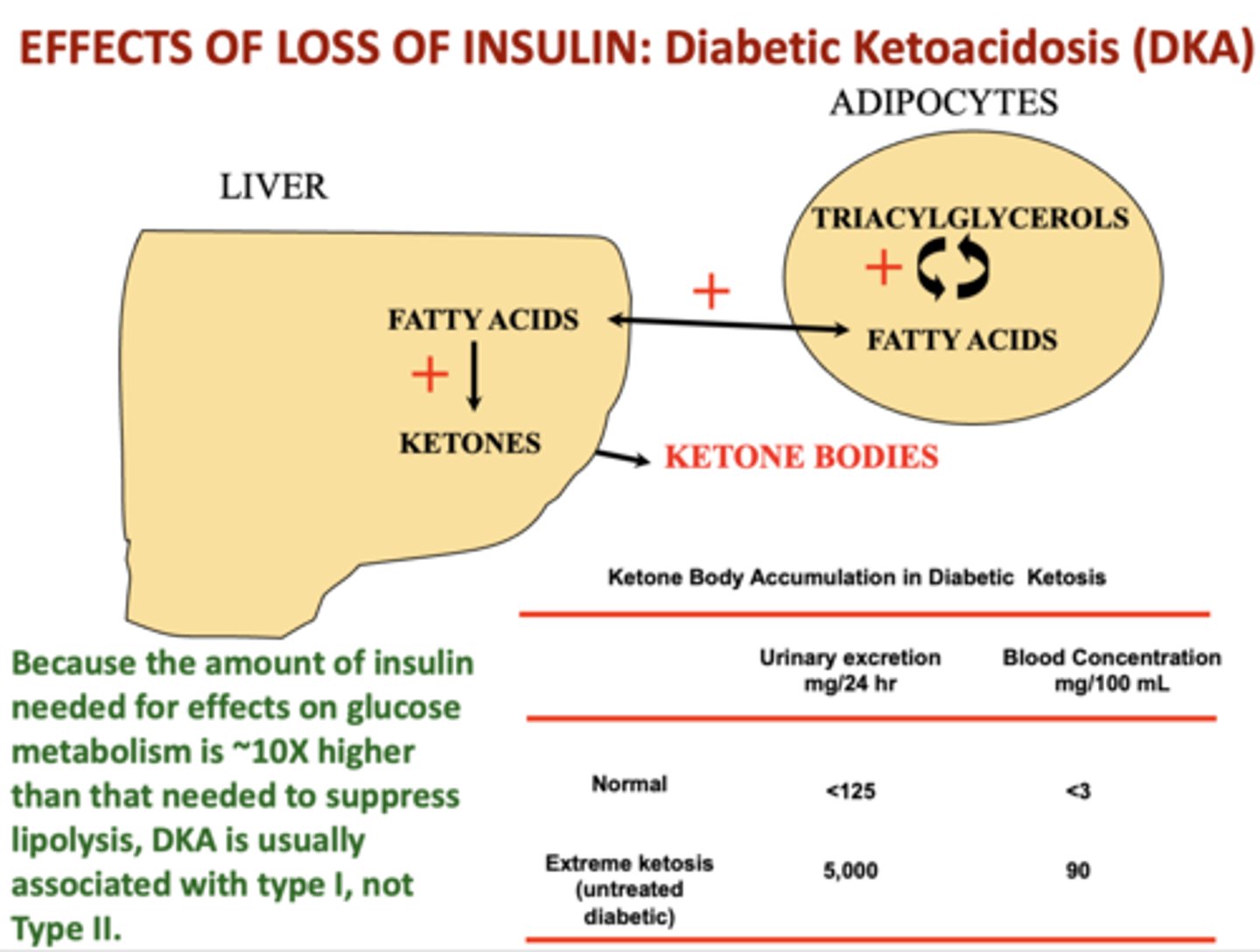
Why is ketone body production due to lack of insulin?
adaptation to starvation
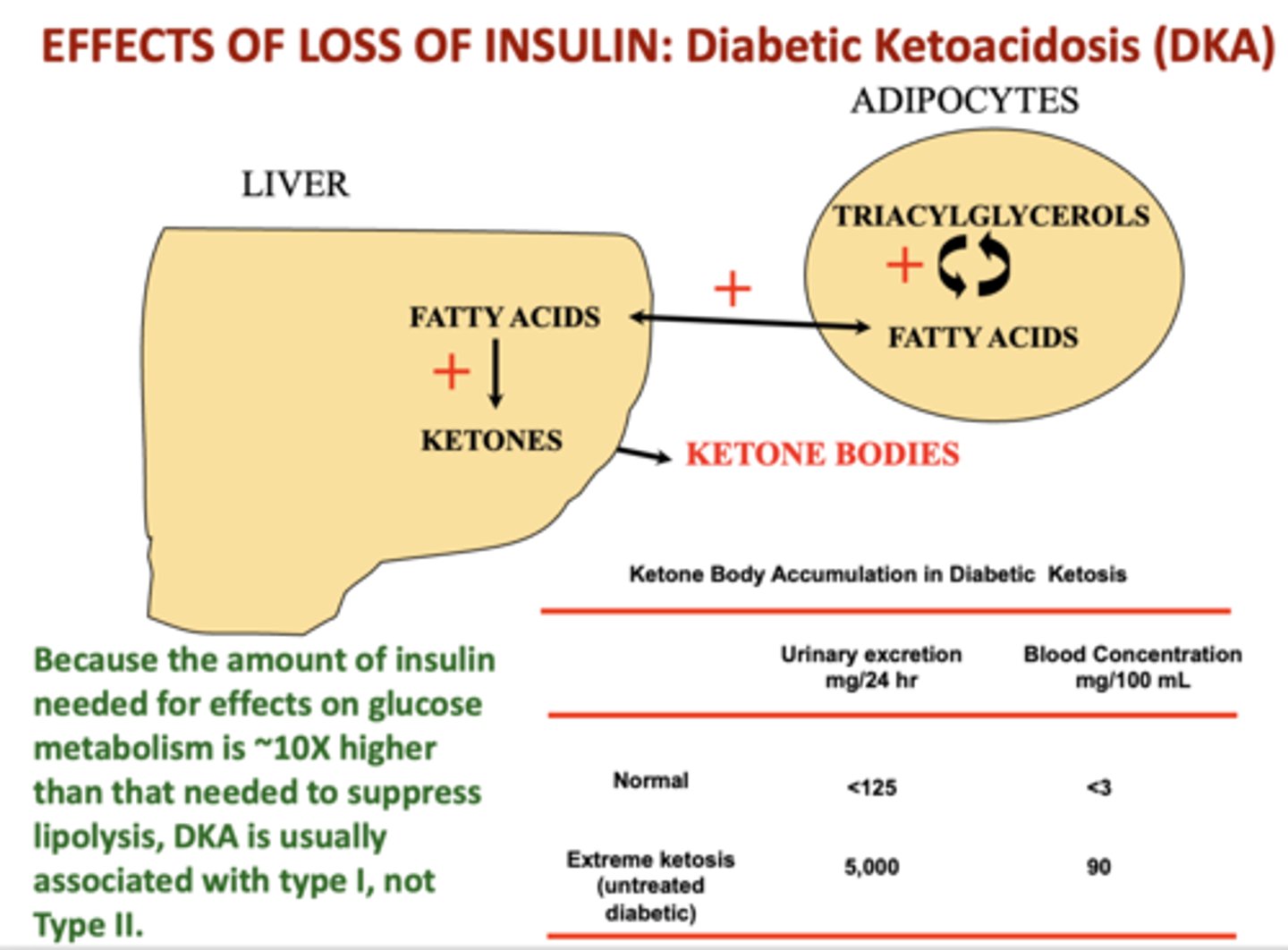
Diabetic ketoacidosis (DKA) is less common in what type of diabetes?
type II
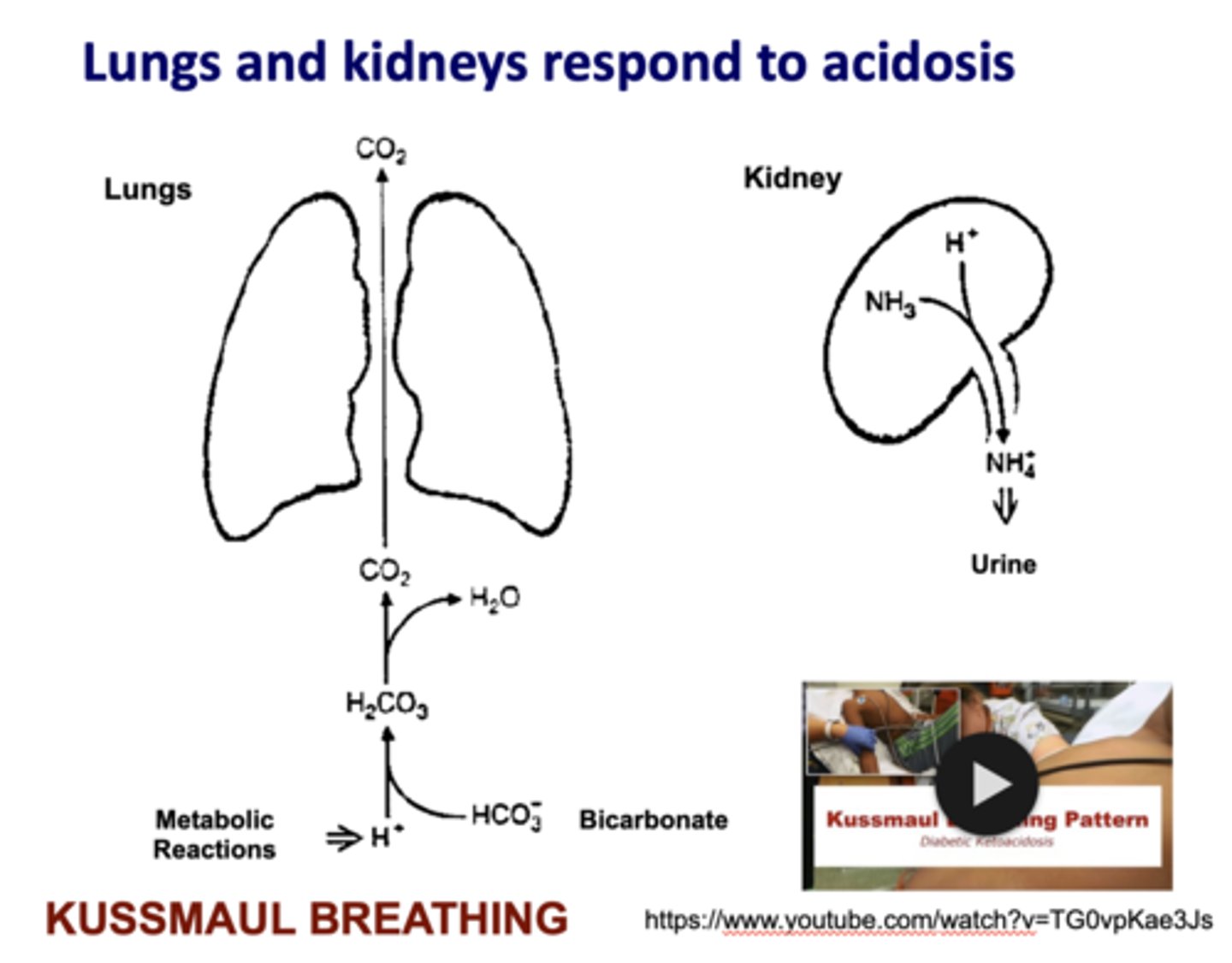
How do the lung and kidneys respond to acidosis?
kussmaul breathing
What has the following characteristics?
- Limit blood glucose after eating
- Is a glucosidase inhibitor
- It works by slowing down the enzyme that turns carbohydrates into glucose. This results in a smaller rise in blood sugar levels following a meal.
Acarbose
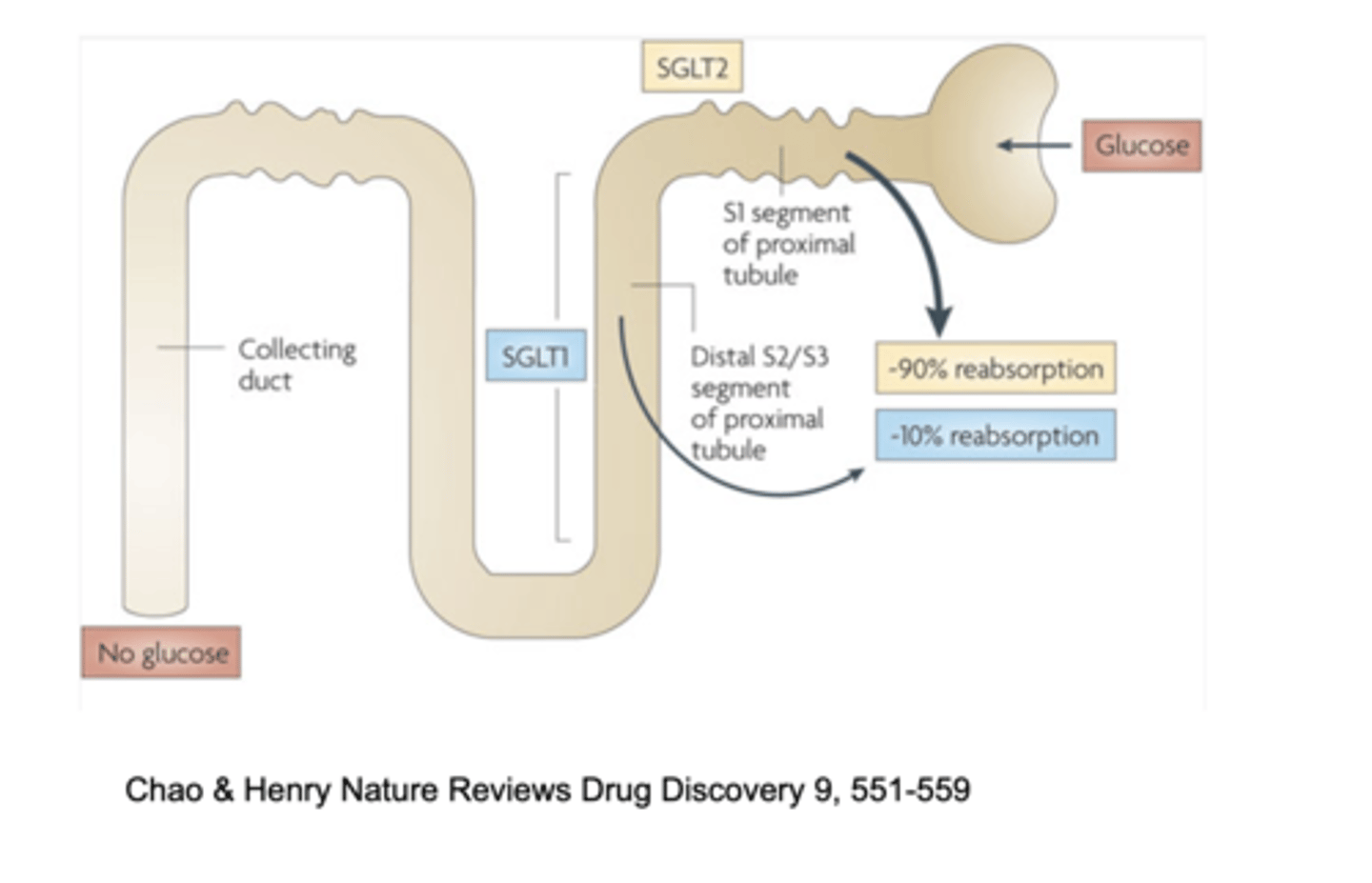
Jardiance is a type II diabetes pill that reduced deaths from heart complications by 38% by working on what?
SGLT2
T/F: Insulin affects carbohydrate, fat and protein metabolism
True
These are common therapeutic approaches for what?
- Diet and exercise
- Block carbohydrate uptake (acarbose)
- Insulins of different properties
- Activate insulin secretion
- Target incretins (stable GLP1/GIP analogs, DPPIV inh.)
- Inhibit ATP dep K+ channels (sulfonylureas, meglitinides)
- Block hepatic glucose output (metformin)
diabetes
Mature Onset Diabetes of the Young arises because a defect in glucokinase results in failure to regulate the:
A. ATP-dependent potassium channel
B. Malate/aspartate shuttle
C. Insulin receptor
D. Incretins
A. ATP-dependent potassium channel
When a dose of glucose is given by mouth, the insulin response is greater than the same dose given by injection. This is because:
A. Dietary glucose goes first to the liver
B. Intestinal endocrine cells secrete GLP-1/GIP in response to fed glucose
C. Intestinal endocrine cells secrete cholescytokinin in response to fed glucose
D. Injected glucose causes brain neurohormone secretion limiting insulin production
B. Intestinal endocrine cells secrete GLP-1/GIP in response to fed glucose
Lipid metabolism is disrupted in diabetes. Which of the following changes would NOT be expected in adipose tissue of diabetics?
A. Activation of hormone sensitive lipase
B. Activation of phosphofructokinase 1
C. Decreased activity of phosphofructokinase 2
D. Decreased lipoprotein lipase activity
B. Activation of phosphofructokinase 1
A 16-year-old female with abdominal pain, nausea, and vomiting. She has type 1 diabetes. 3 days ago she reduced her insulin dose as she had vomiting, diarrhea, and was unable to eat. The patient has dry mucous membranes, poor skin turgor, and her breath smells fruity. What is the most likely cause of the patient's condition?
A. Hypoglycemia
B. Diabetic ketoacidosis
C. Hyperglycemic hyperosmolar syndrome
D. Urinary tract infection
B. Diabetic ketoacidosis
A recent review states “In type 1 diabetics, severe hypoglycemia (requiring help for recovery) has an annual prevalence of 30–40% and an annual incidence of 1.0 – 1.7 episodes per patient per year.” This results from an ”insulin overdose”. Which of the following enzymes targeted by insulin signaling would be a major part of the explanation for this problem?
A. Adipose lipoprotein lipase
B. Liver phosphofructokinase 2
C. Kidney phosphofructokinase 1
D. Liver phosphatidylinositol 3 kinase
E. Muscle pyruvate kinase
B. Liver phosphofructokinase 2