UA Clinical Final Rotation Exam
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Anuria
Lack of urine production
Oliguria
Less than 400ml/day of urine production
Polyuria
More than 2500ml of urine production per day
Nocturia
Increase in nocturnal excretion of urine
How long can urine sit out?
Must be analyzed within 2 hrs of collection
If more, must be refrigerated, then brought to room temp to avoid amorphous crystals
Medulla
Inner portion of kidney, made of…
Pyramids (Striated tubular structures)
Papulla (pointed ends of pyramids)
Calyces (cuplike projects, collect urine)
Pelvis (Central region, collects urine)
Where does blood enter the glomerulus
Afferent arteriole
Where does blood leave the nephron
Efferent arteriole
Bowman’s capsule
main purpose: filtration
surrounds glomerular capillaries and acts like a bowl to catch the ultrafiltration
Basement membrane
Main purpose: Shield of negativity
influences which molecules can bass form capillaries to Bowman’s space
Mesangium
Main purpose: Structural support
Provides support for glomerulus, variable contraction to help control perfusion
Juxtaglomerular apparatus (JGA)
Main purpose: Vasoconstriction, Renin secretion, and structural support
Made of…
Macula Densa cells (Chemoreceptors in DCT which sense Na/Cl and triggers vasoconstriction)
Juxtaglomerular cells (sense cell shrinkage and secrete renin)
Extraglomerular mesangial cells (Provide support/contraction)
What makes up the glomerulus?
Bowman’s capsule
Basement membrane
Mesangium
JGA
Vasa recta
Vasa recta
Main purpose: Reabsorbs/secretes
specialized capillary network derived from efferent arteriole that are intertwined throughout the nephron
Proximal Convoluted Tubule (PCT)
Has cuboidal/columnar cells (brush border) to help with reabsorption
Performs Active transport (Reabsorbs 2/3 Amino acids, Na, Cl, K, HCO3) and Passive transport (Reabsorbs urea/water)
Loop of Henle
Concentrates urine using countercurrent multiplication
Descending loop: Only permeable to H2O (Reabsorption)
Ascending loop: Only permeable to Na/Cl (Reabsorption)
Distal Convoluted Tubule (DCT)
Located next to the JGA cells
Last step for reabsorption
Connects nephron to Collecting Ducts
Collection Ducts
Collects urine from several nephrons
Tubular secretion
Eliminates waste products not filtered out, regulates acid-base balance in the body via secretion of H+
H+ can combine with phosphate/ammonia to be excreted
H+ can combine with HCO3 to be reabsorbed
Erythropoietin
Glycoprotein Hormone
Released in response to low O2 levels
Stimulates erythropoiesis in bone marrow
Renin Angiotensin Aldosterone System (RAAS)
Angiotensinogen is released by the liver, cleaved by renin= Angiotensin 1
Angiotensin 1 travels to the lungs to be cleaved by ACE (Angiotensin Converting Enzyme)= Angiotensin 2
Angiotensin 2 travels the body, results in vasoconstriction, stimulates release of aldosterone, and stimulates the pituitary to release ADH (Anti-diuretic hormone)
What stimulates the RAAS
Decrease in Blood Pressure
Sympathetic nerve stimulation (Fight or Flight)
Decreased sodium concentration in DCT
What happens to unpreserved urine?
Physical: Darker color/clarity, increased odor
Chemical:
Increased: pH, Nitrite, Bacteria
Decreased: Glucose, Ketones, Bilirubin, Urobilinogen, RBCs, WBCs
Refractometry
Comparison of the velocity of light in the air with the velocity of light in the solution
Confirmation test for specific gravity >1.030
Specific Gravity terms/RI
RI: 1.003-1.035
Hyposthenuric <1.010
Hypersthenuric >1.010
Leukocytes
Reaction: Indoxycarbonic acid ester
False positive: Bleach
False negative: Ascorbic acid (Vit. C)
Nitrite
Greiss reaction (Diazonium salt)
False positive: Highly pigmented urine
False negative: Antibiotics/Ascorbic acid
Urobilinogen
Ehrlich reaction (P-dimethylaminobenzaldehyde)
False positive: Highly pigmented urines
False negative: High concentrations of nitrite
Increased in: Hemolytic anemia, liver disease, biliary disease
Decreased in: Biliary obstruction, liver dysfunction
Protein
Tetrabromophenol blue, protein error of indicators
False positive: Highly alkaline urines
False negative: Proteins other than Albumin
Microalbuminuria
Persistent elevation of albumin
Proteinuria
Pre-renal: Not detected by protein pad, made of Hemoglobin, myoglobin, Bence-Jones
Renal: Due to damage glomerulus= Increased albumin/WBCs/RBCs
Tubular renal: Due to Toxins, Heavy metals, Fanconi’s
Post-Renal: Due to normal tubular reabsorption failure can see bacteria, menstruation blood, or sperm
pH
Double- indicator system (Methyl Red and Bromothymol Blue)
No interferences (except runover from other pads)
If pH is >8.5 its probably bad collection
alkaline tide= alkaline urine pH after food ingestion
Blood
Pseudoperoxidase activity of hemoglobin
False positive: Menstrual contamination, Bleach
False negative: Ascorbic acid
Hematuria
Hematuria- typically due to renal/urinary tract disease (Calculi, glomerulonephritis, pyelonephritis, cystitis)
Hemoglobinuria- Due to intravascular hemolysis, hemolytic anemia, burns, infections
Myoglobinuria- Due to crush trauma, muscle destruction
Hemosinderinuria- Reabsorption by tubular cells of filtered Hgb
Specific Gravity Pad
pKa change of polyelectrodes
The higher the concentration of urine, the more H+ ions are released, causing the pH to be lower
Ketone
Sodium nitroprusside reaction
Reacts with Acetoacetate/acetone
False positive: Highly pigmented urine, levodopa
False negative: Breakdown of ketones
Bilirubin
Diazo reaction (bilirubin + Diazo salt= azo dye)
Only detects conjugated bilirubin
False positive: Highly pigmented urine
False negative: Exposure to light
Glucose
Double sequential enzyme reaction with glucose oxidase and peroxidase
False positive: Peroxides/Bleach
False negative: Ascorbic acid
Confirmatory Tests
Benedicts reaction- Confirmation for reducing sugars, not specific to glucose
Clinitest- Modified benedicts reaction, screens for galactose/other reducing sugars
Ictotest- confirmatory for bilirubin
Acetest- confirmatory for ketones
SSA/ Sulfasalycilic acid precipitation- confirmatory for albumin
Cyanide nitroprusside- confirmatory for cystine
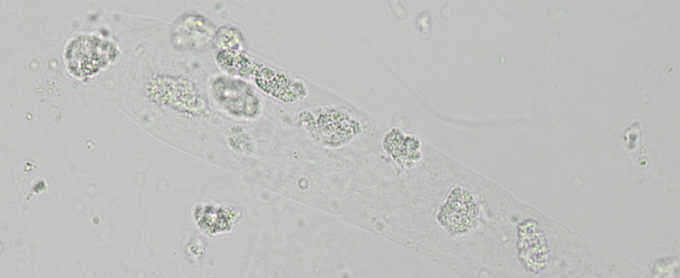
Squamous Epithelial Cells
Large, Irregular borders, Distinct nucleus
Causes: Normal Cellular Sloughing

Transitional Epithelial cells
Comes from Renal Pelvis/calyces/ureters/bladder
Increased post invasive procedure (Trauma/catheter)
Larger than WBCs, Central nucleus
Renal Epithelial Cells
Slightly larger than WBC, eccentric nucleus, 1:1 N:C
Seen with tubular injury (Slight increase is normal in neonates)

Oval Fat Body
Renal Epithelial cells that have absorbed lipids
Must be ID with Fat stains or polarizing microscopy
Seen with Diabetes mellitus, Tubular necrosis, Lipiduria (with nephrotic syndrome)

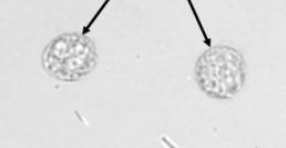
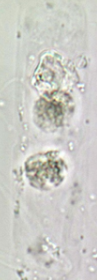
White Blood Cells
Multi-lobed nuclei
“Glitter cells”
Seen with tubular damage, Infection, or Inflammation
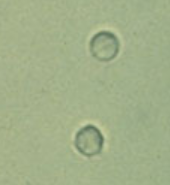
Red Blood Cells
Smaller than WBCs
Dimorphic RBCs= Problems with filtration membrane
Ghost cells- RBCs in alkaline urine (Alkaline urine causes cells to lyse)
Acetic acid- used to distinguish RBCs and Yeast, RBCs will lyse
Casts
Made of Tamm-Horsfall protein matrix (Uromodulin)
Formed in the lumens of DCT/CD
Hyaline Cast
Most frequently seen
Almost see-through, rounded edges
Normal, only pathological in large numbers

RBC Cast
Seen with glomerular damage
MUST have free floating RBCs to call
Group of RBCs with matrix around them
WBC Cast
Group of WBCs with cell matrix
Seen with Upper UTI’s, acute interstitial nephritis and glomerulonephritis
RTE Cast
Seen with tubular destruction
RTE’s in a clear matrix
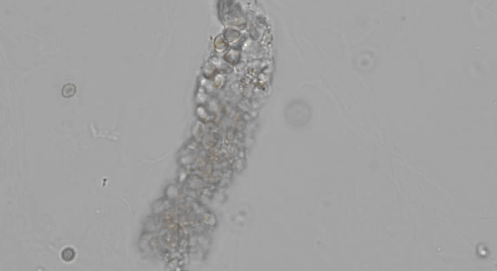
Granular Cast
Disintegration of Cellular casts

Waxy Cast
Seen with chronic renal failure
Slightly opaque, blunt edges

Fatty Cast
Seen with oval fat bodies/free fat droplets in lipiduria
Seen with nephrotic syndrome, Diabetes, and crush injuries

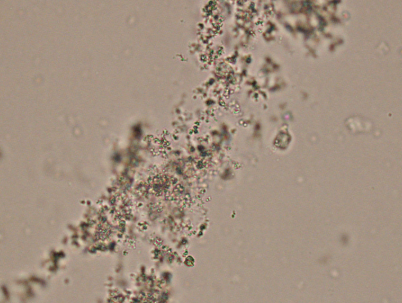
Amorphous urates
Normal Crystals
Acidic urine
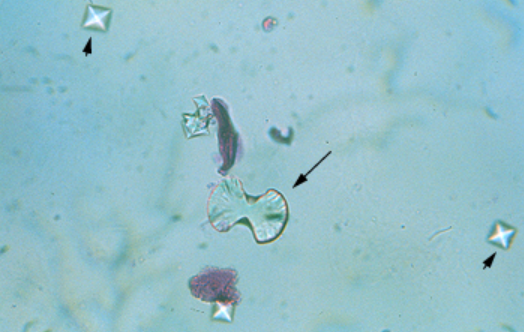
Calcium oxalate
Normal and Abnormal Crystals
Acidic to Normal Urine
Dihydrate-Envelopes
Monohydrate- Dumbells
Monosodium urate
Slender needles, typically antibiotic related
Normal, Seen in acidic urine
Uric acid Crystals
Colorless/yellow-brown, Rosette or Rhomboid form
Normal, Seen in acidic urine

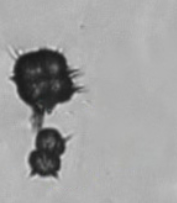
Ammonium biruate crystal
Yellow/brown, throny apples
Normal, Seen in alkaline urine
Calcium phosphate
Colorless, flat rectangles/rosettes
Normal, seen in alkaline urine
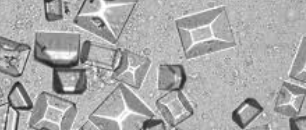
Triple Phosphate
Prism/Coffin-lid
Normal Crystals, seen in alkaline urine
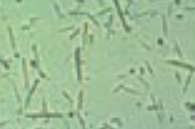
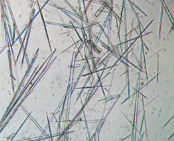
Ampicillin Crystals
Long thin clusters of needles
Due to high levels of antibiotics
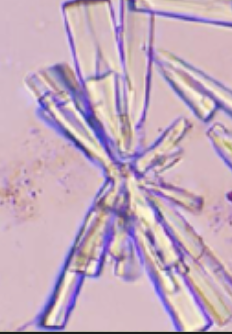
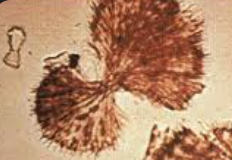
Sulfanimide crystals
Yellow/brown, Fan-shaped bow-ties
Abnormal, Drug-associated
Bilirubin crystals
Yellow/brown, fine amorphous needles
Abnormal, due to liver disease

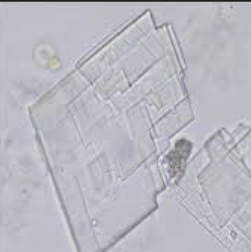
Cholesterol Crystals
Flat plates with corner notches
Abnormal crystals, seen with lipiduria/proteinuria
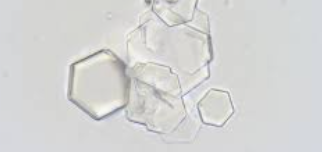
Cystine crystals
6-sided plates, refractile
Abnormal, seen with cystinosis/cystinuria
Hemosiderin
Brown, granules in clumps
Abnormal, seen post-hemolytic event
Leucine
Dark yellow/brown, spheres with concentric circles
Abnormal, seen with liver disease

Tyrosine
Colorless-brown fine needles (Pine needles)
Abnormal, Seen with liver disease

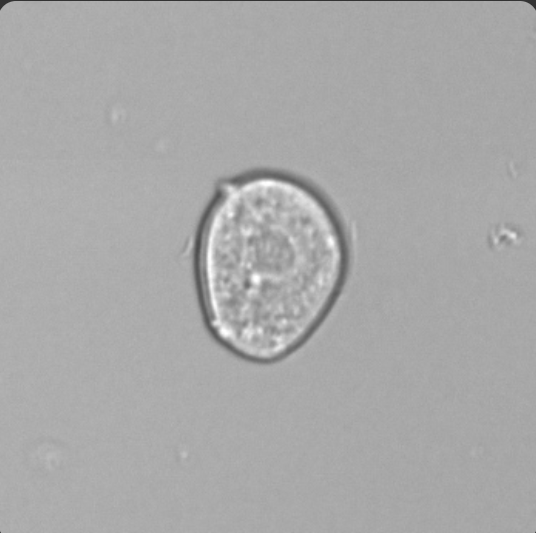
Trichomonas
Looks similar to WBC, must be moving to call

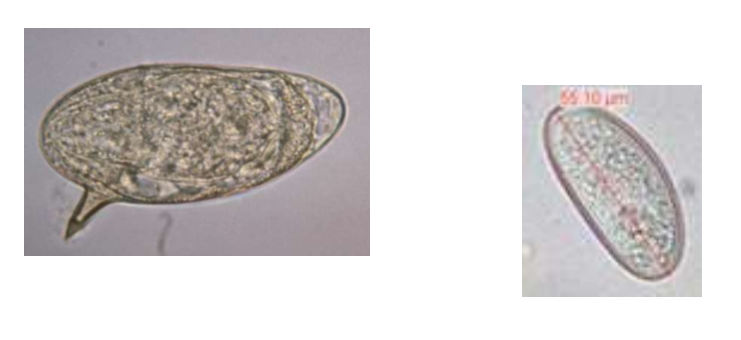
Parasitic eggs/worms
can be schistoma or enterobius
Spermatozoa
Must see heads and tails to call

Starch Crystals
Pseudo maltese cross
From gloves
