Hemodialysis access graft
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
AV fistula
A direct connection between an artery and vein that is created to allow access point for dialysis port
AV graft
Uses a synthetic tube to connect an artery and vein to allow an access point for diapysis port
Hemodialysis
Removes creatinine, urea and water from the blood of pts in end-stage renal failure
The closer the fistula to the heart, the greater the risk for…
Developing heart failure
Pre-op assessment for AV fistula
Eval native vessels for selecting appropriate type of graft
Obtain bilateral brachial pressures (should be <20mmHg between both)
Native vein should be >2.5mm for AVF
Native vein >4mm for synthetic graft
Native artery >2mm
Veins should be evaluated for a straight course and within 1cm of skin surface
Requires Palmar arch test
Reactive hyperemia can be performed to assess the feeding artery for appropriate increase in arterial diameter and vessel compliance for fistula placement and maturation
Reactive hyperemia
Clenching the ipsilateral fist during an upper extremity Doppler evaluation should increase distal resistance and pulsatility in the proximal arteries
The clenching should be held for 2mins
Upon release of the clenched fist, the distal resistance drops significantly and flow increases to the head
The RI is measured an a value over 0.7 indicates the feeding artery will not work for successful AVF creation
Indications for post-op AVF/AVG evaluation:
Dialysis equipment provides information regarding then functionality of the graft (dynamic venous pressure (>200mmHg), access recirculation (>12% ABNL), urea reduction ratio (<60% ABNL))
Palpable mass, significant hand pain, venous HTN, water hammer pulse (thumping pulse palpated with acute occlusion of graft)
Decreased of absent thrill = abnormal
Brescia-Cimino
Most common AVF
Radial artery to the cephalic vein at wrist
Snuff box fistula
Anatomical suffbox is also called the radial fossa
Triangular depression on the lateral aspect of the dorsum of the hand
The radial artery, a branch of the radial nerve, and the cephalic vein are found in the snuffbox
Radial artery is connected to the cephalic vein at distal wrist
Because the artery courses directly over the vein in this location, little vessel movement is required during surgery
Brachiocephalic AVF
Brachial artery and antecubital vein at elbow
Brachiobasilic AVF
Brachial artery and basilic vein at elbow
Radiobasilic AVF
Radial artery and basilic vein in the forearm
Synthetic graft
Used when native veins are inadequate or an AVF has failed
PTFE Gore-Tex graft - made of polytetrafluoroethylene, also known as Teflon
Dacron graft - made of synthetic polyester
SHORTER DURATION THAN AVF and LOWER PATENCY RATES
Straight synthetic graft - MOST COMMON; brachial artery to basilic vein in upper arm
Looped synthetic graft - MOST COMMON; brachial artery to antecubital or cephalic vein at elbow; loop extends distally to wrist
Arm position for Fistula evaluation
45 degree angle and externally rotated
AV fistula has a ______ anastomosis site
Single
An AV graft has ________ anastomosis sites
Two
Venous flow proximal to an AV fistula
Becomes pulsatile and turbulent due to high inflow of arterial flow distally
Arterial flow proximal to AV fistula should be…
Low resistance with increased diastolic flow
Pressure will decrease in the artery distal to fistula
Normal flow PSV in AV graft
100-400cm/s
Normal EDV in AF graft
60-200cm/s
Abnormal findings in graft
Graft stenosis suspected with velocities greater than 400cm/s
Velocity ratio = PSV at stenosis/PSV artery prox to stenosis
Ratio at stenosis >2.0 is abnormal
If the flow velocity doubles (or more) between two points in the graft, significant stenosis is suspected
Increase in flow velocity between two segments of 100% or more is considered abnormal
The inflow artery demonstrates a triphasic waveform, graft occlusion is suspected
If the venous outflow vein demonstrates loss of spontaneous flow and respiratory phasicity, stenosis or obstruction of the vein is suspected
Volume flow
Obtained in a straight vein segment, midgraft/fistula is preferred
Measure the diameter of the vein in the area of flow sampling
Doppler measurement obtained by opening sample volume size to include all flow from anterior wall to posterior wall
Abnormal flow volume <500ml/min indicates stenosis
>1200ml/min indicates CHF
Most common sites of dialysis graft stenosis
Venous anastomosis
Outflow vein
Due to arterial flow hitting venous wall, causes damage to lining resulting in hyperplasia Complications:
#1 cause of hemodialysis graft failure is THROMBOSIS of the graft
Stenosis/occlusion
Aneurysm of the graft
Pseudo caused by needle puncture for dialysis
Can cause CHF due to increased flow in venous return to heart
Portion of extremity distal to graft may suffer from ischemic symptoms due to steal syndrome
Infection
Dialysis access steal syndrome most commonly occurs in a
Radiocephalic fistula
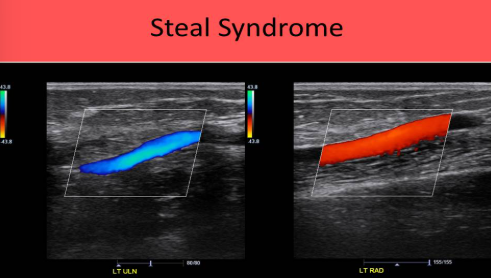
Dialysis access steal syndrome
Distal to the fistula graft, the ulnar artery will be antegrade and the radial artery will be retrograde
Blood travels from the ulnar artery into the hand and moves through the palmar arch to exit the hand in the radial artery
Caused by high volume flow in most cases, but can also occur with inflow stenosis
Both cause flow to be “sucked up” the radial artery and into the outflow vein from the ulnar/palmar arch
PVR or PPG assessment of the affected digits should be compared to the unaffected digits of the opposite hand
Symptoms of Dialysis access steal syndrome
Include increasing pain, polar sensation, paresthesia, Finger/Brachial Index <0.7, cyanotic fingertips
Symptoms increase with use of the arm
Diminished radial pulse on palpation
Duplex eval of Dialysis access steal syndrome
Inflow artery within the 2cm proximal to the fistula anastomosis site
Inflow artery within the first 2cm distal to the fistula anastomosis site
This waveform is used to diagnose steal syndrome, if flow is retrograde in the distal radial (inflow) artery, when flow is moving from the ulnar artery through the palmar arch and cephalad toward the radial artery/fistula
Blood is bein STOLEN from the hand before it is perfused properly
Fistula at the confluence of the artery and vein
Outflow vein at multiple locations along the arm, above and below the fistula
Segmental pressure evaluation
Can only be performed when the wrist cuff can be placed distal to the fistula
In the average sized pt:
12cm cuff placed on the unaffected upper arm
10cm cuff placed at the wrists
2.5cm cuffs placed on the fingers
PPG sensors placed bilaterally on digits
Unaffected arm: Brachial, radial, ulnar and digital waveforms and pressures obtained
Unaffected arm: Radial, ulnar and digital waveforms and pressures obtained
Outflow vein is compressed
Outflow vein compression normal findings:
Causes multiphasic flow patterns in the brachial, radial and ulnar arteries
Digital waveforms should demonstrate consistent amplitude and vary by less than 15mmHg between digits
Digital/Brachial index >0.7
Positive for Dialysis access steal syndrome:
Digital pressures <80mmHg and DBI <0.7
Compression of outflow vein causes increased amplitude of the digital waveforms of the affected arm and an increase in the digital pressures
The increase in pressure and amplitude is caused by the compression of the outflow vein because normal flow is returned to the hand as outflow is obstructed
What is the difference between a hemodialysis fistula and a hemodialysis graft?
A fistula connects a native artery and vein, a graft is a synthetic vessel connecting an artery and vein
The minimum diameter of a native vein that can be used for a hemodialysis fistula is ______, while the minimum diameter of the native vein that will connect to the synthetic vein that will connect to the synthetic graft is __________
2.5mm; 4mm
What is the minimum arterial diameter that can be used for connection to a hemodialysis graft?
2mm
What pre-procedure test is required before creation of a dialysis fistula
Allen test
A patient presents for evaluation of their AVG and the script states “water hammer pulse present” What do you expect to find on the exam?
Occluded graft
What is found in the anatomical snuff box
Distal cephalic vein, distal radial artery, radial nerve
What determines if a fistula is created, or a graft is inserted for dialysis?
If the native vessels are too small for a fistula, a graft is used instead
What is the most common site for stenosis in pts with AVG
Venous anastomosis
What changes occur in the native artery proximal to an AVF?
Flow changes from triphasic to monophasic
What changes occur in the native vein proximal to an AVF?
Increased pulsatility
What is the most common cause of AVG failure?
Thrombosis
How is the volume flow measured in an AVF?
Open the sample volume from wall to wall within a normal segment of the graft and trace the waveform
If the radial and ulnar artery demonstrate flow moving in opposite directions in a pt with an AVG, it is highly suggestive of:
Steal syndrome