PHRM3550 Respiratory
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
Name the obstructive pulmonary diseases.
- asthma
- COPD
- CF
- TB
Name the restrictive pulmonary diseases.
- Pulmonary Fibrosis
- Pulmonary Hypertension
- Lung emergencies
Describe obstructive pulmonary disease.
- characterized by airway obstruction that is worse with expiration
- either more force is required to expire, emptying is slowed, or both
Asthma Attack Signs and Symptoms
- Signs: dyspnea (SOB)
- Symptoms: wheezing and cough
Characterizations of an Asthma Attack
- chest tightness
- bronchial hyper-responsiveness
- thick mucus deposition
Risk factors for asthma
- atopy (sensitive to IgE allergens)
- family history
- allergen exposure
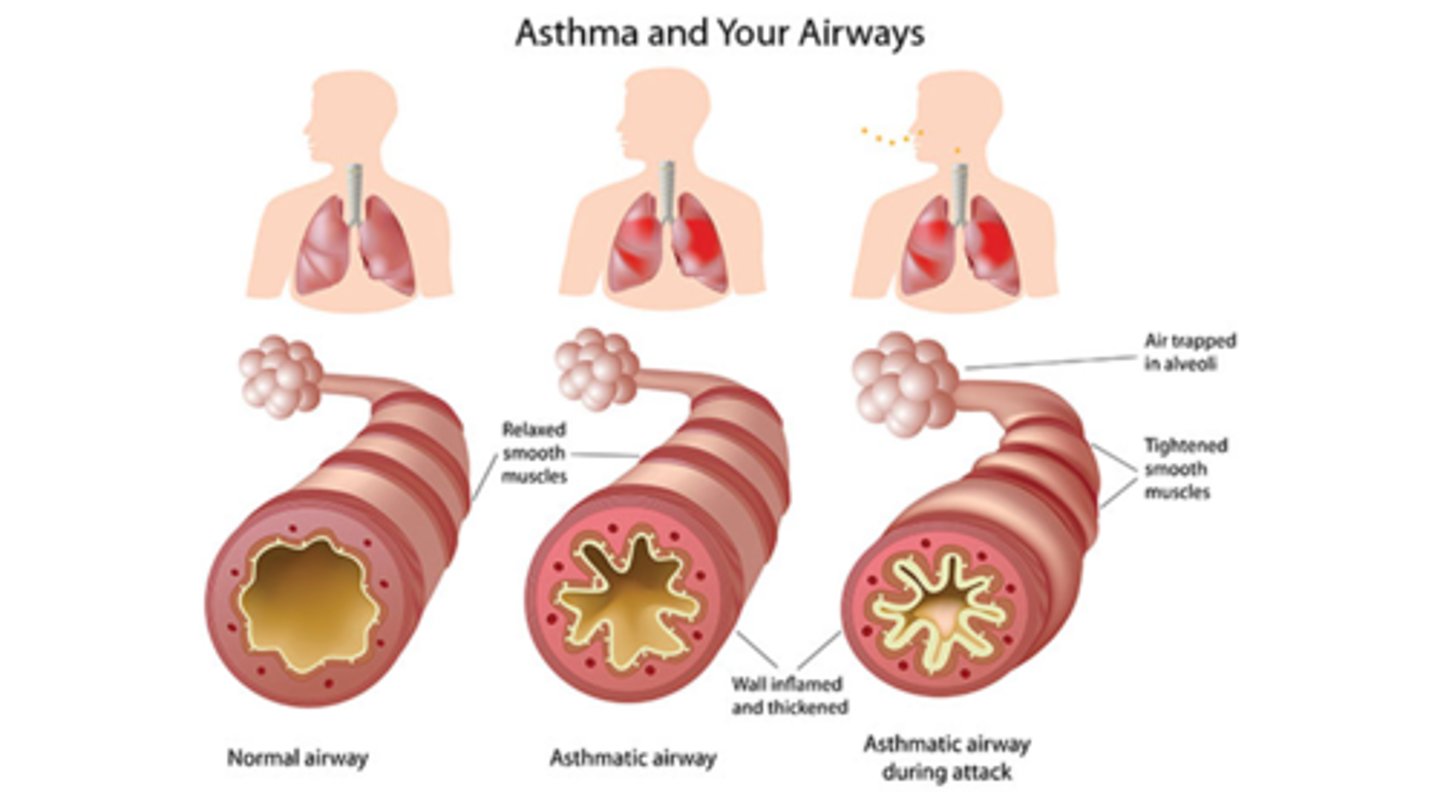
Mechanism of asthma attack
airways react strongly to a certain substance, the muscles around them tighten causing airways to narrow and less air flow to lungs
What is the pathology of asthma?
- airway mucosa is thickened, swollen with fluid, and filled with inflammatory cells
- smooth muscle hypertrophied & contracted airway
- bronchial cells damaged
- stripped airway lumen --> airway hyperactive to triggers
What is the pathology in severe asthma?
1. secretory gland hyperplasia (grows larger & more active)
2. mucus hypersecretion (too much thick mucus)
3. mucus plugging of airways (blocks airways)
What happens when subepithelial myofibroblasts proliferate?
They produce increased interstitial collagen (scar tissue) leading to fixed airway obstruction (permanent blockage)
What is the fundamental problem in asthma?
increased reactivity of airways to stimuli (the airways are extra sensitive to everything)
Describe provocative factors.
things that can trigger or worsen asthma symptoms by making the airways tighten or overreact
What are some physiologic/pharmacologic provocative factors of asthma?
- histamine
- methacholine
- ATP
How is methacholine measured?
spirometer
What are some physiochemical agents (real-life triggers) that are provocative factors for asthma?
- exercise
- air pollutants like SO2 and NO2
- viral respiratory infections
- ingestants like propanolol and aspirin/NSAIDS
What are some allergens that are provocative factors for asthma?
- low MW chemicals (penicillins, isocyanates, anhydrides, chromate)
- complex organic molecules (animal danders, dust mites, enzymes, wood dusts)
Acute treatment of asthma
- elimination of causative agents
- drugs that reverse bronchospasms and airway inflammation
- immediate management: oxygen and inhaled bronchodilators
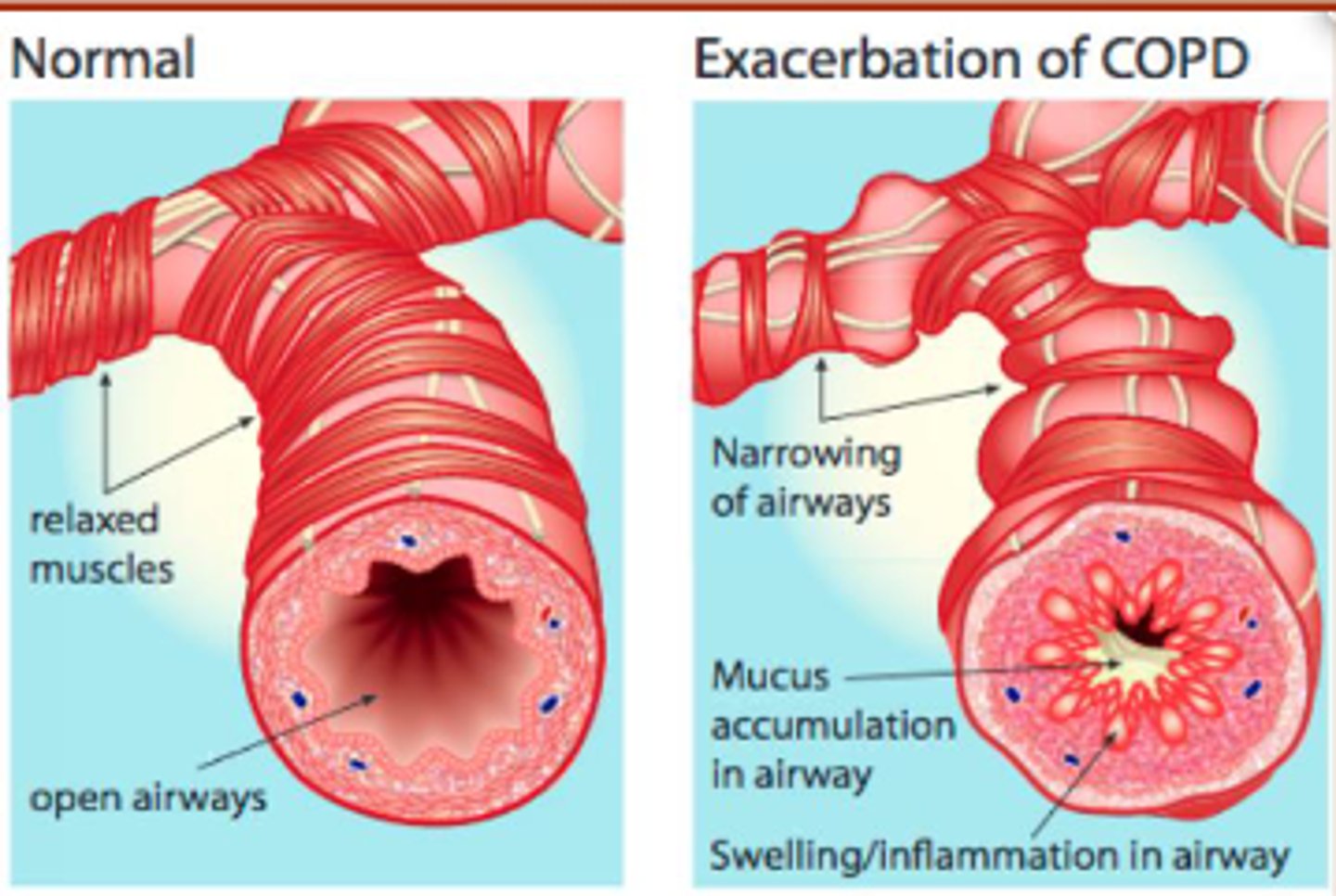
Describe COPD.
- progressive lung disease characterized by airflow limitation that is not reversible
- abnormal inflammatory response to harmful particles or gases
What is COPD primarily caused by (over 90%)?
cigarette smoke (active and second-hand)
Why does less air flow through airways in COPD?
- airways/air sacs lose elastic quality
- walls between air sacs are destroyed, become thick and inflamed
- airways make more mucus, clogging airways
Describe emphysema.
walls between many of the air sacs are damaged, causing them to lose their shape and become floppy
How does emphysema affect gas exchange?
- walls become destroyed --> fewer and larger air sacs
- less surface area, less gas exchange
Clinical signs of COPD Emphysema
- dyspnea on exertion (SOB)
- little coughing and very little sputum (mucus) produced
General Treatments for COPD Emphysema
- supplemental oxygen
- inhaled steroids
- inhaled bronchodilators
- antibiotics if infectious
- smoking cessation drugs
What is chronic bronchitis?
- hypersecretion of yellow-grey mucus
- defined by a history of chronic productive cough that continues for at least 3 months of the year for 2 consecutive years
What can chronic bronchitis develop from?
- a cold, sore throat or flu
- most common among smokers and workers exposed to air pollution
How does chronic obstructive bronchitis affect the airways?
- constantly irritates and inflames the lining
- leads to permanent narrowing of airways
What do asthma and COPD bronchitis have in common?
both cause swelling in airways that makes it difficult to breathe
How is asthma different from COPD bronchitis?
- asthma usually triggered by allergens or activity, bronchitis is usually result of smoking
- asthma can be acute and usually gets better, bronchitis is usually chronic and gets worse
Clinical signs of chronic bronchitis
- decreased tolerance and ability to exercise
- hypoxemia
- wheezing, SOB, cough
- cyanosis
What is Dyspnea?
- difficult or labored respiration (SOB)
- 5 grades/degrees of dyspnea
What is orthopnea?
type of dyspnea that occurs when lying down and is relieved by sitting upright
PND (paroxysmal nocturnal dyspnea)
respiratory distress that awakens the patient from sleep
What is the most common lethal genetic disease among Caucasians?
CF
What is CF characterized by?
- pancreatic insufficiency (mucus blocks digestive enzymes)
- chronic airway infections
- repeated pulmonary exacerbations (flare-ups)
Symptoms of CF
- thick mucus build-up
- bacterial infections that are unresponsive to standard antibiotics
- infections block airways and cause bloody cough
- frequent sinusitis, bronchitis, and pneumonia
What happens in a mutant CFTR channel?
does not move Cl ions causing sticky mucus to build up on the outside of the cell
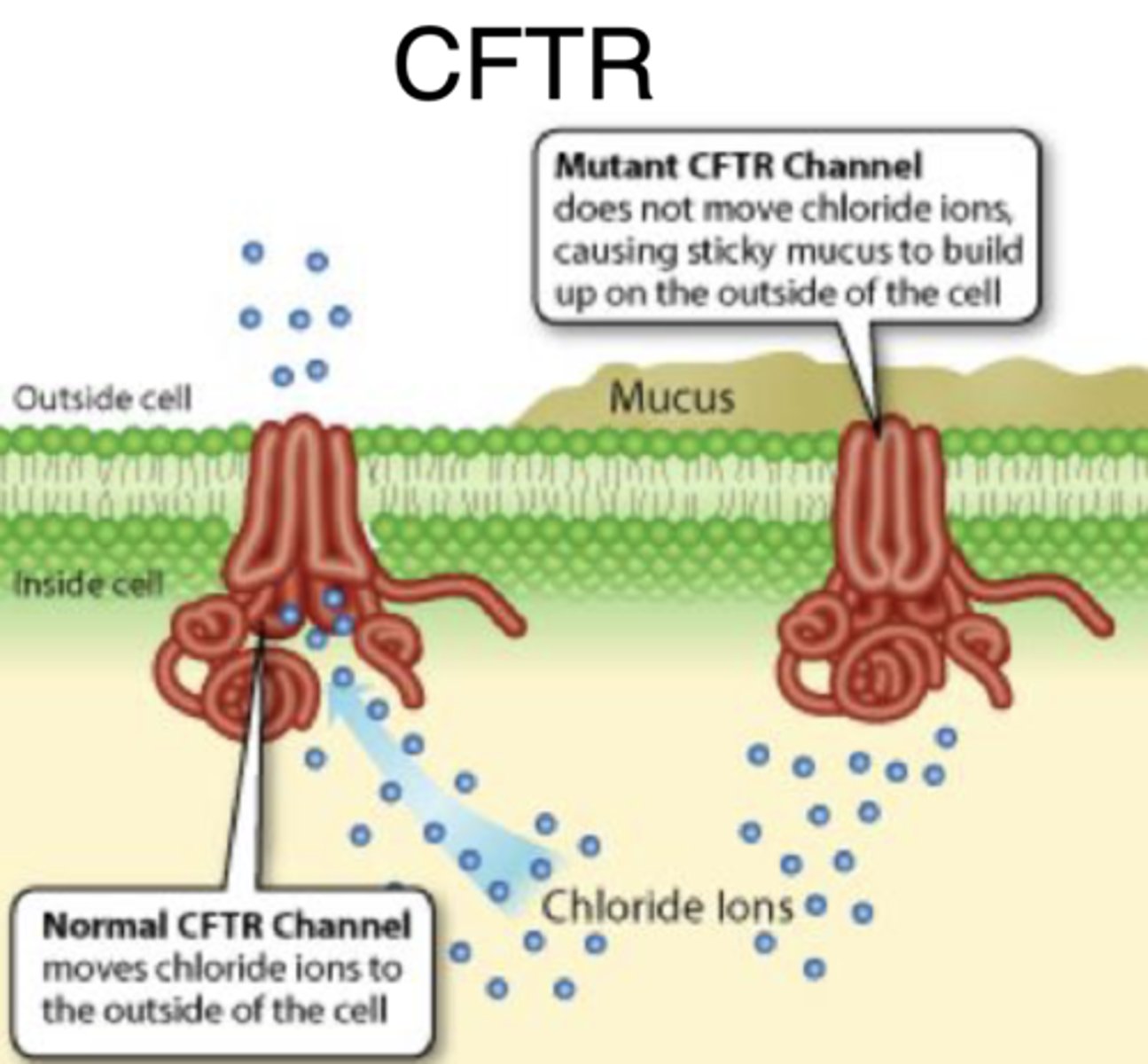
What causes infections in CF?
failure of mucus to detach from ducts that slows mucociliary transport
What defenses does CFTR loss reduce the effectiveness of?
mucociliary transport and antimicrobial activity
What is bronchiectasis?
- localized irreversible dilation of part of a bronchial tree
- usually result of infection or other condition that prevents the airways from clearing mucus
Clinical signs of bronchiectasis
- cupful amounts of pus which are foul in odor
- recurrent lower respiratory tract infections
Signs and symptoms of TB
- cough lasting > 3 weeks
- chest pain, dyspnea
- coughing up blood
- lethargy
- weight loss/anorexia
- chills, fever, night sweats
- pus in sputum
How is TB spread through air?
- acquired from breathing in droplets generated during coughing, sneezing and talking by someone with active TB
What is the bacteria that causes TB?
mycobacterium tuberculosis
Latent TB
- bacteria lives in body without causing illness
- asymptomatic, cannot spread bacteria
- positive skin test
- may develop TB if no treatment for latent infection
Active TB
- active bacteria multiply in body
- individuals feel sick and have symptoms
- can spread bacteria
- positive skin and blood tests
- abnormal chest x-ray
- need treatment
What are the 5 lung emergencies?
- pneumonia
- acute respiratory failure
- aspiration
- acute respiratory distress syndrome
- COVID-19
What does IPF stand for and what is it?
- idiopathic pulmonary fibrosis
- fatal, incurable, chronic, and progressive lung disease
- end stage of interstitial lung diseases
What does pulmonary fibrosis (PF) look like in the imaging?
- distinct chronic, fibrosing (scarring), interstitial pneumonia
- thick, stiff scarring in the interstitial space
What is shown in PF histology (microscope view)?
- fibroblastic foci formation (clusters of scar-making cells)
- excessive deposition of ECM (build-up of extracellular matrix)
Signs and Symptoms of IPF
- SOB
- dry hacking cough
- rapid shallow breathing
- fatigue or malaise
- aching muscles and joints
- chest pain
- cyanosis
- gradual, unintended weight loss
- digital clubbing
What is an exclusion diagnosis?
there's not a single test to prove someone has the disease, so they diagnose by ruling out other possible options
What are used for exclusion diagnosis of IPF?
- Patient history
- chest x-ray (may look normal)
- high resolution computed tomography
- pulmonary function test
- arterial blood gas test
- TB skin test
- Lung biopsy (best way to diagnose)
What does High-Res Computed Tomography show?
shows scar tissue and degree of lung damage
What does arterial blood gas test do?
- measure oxygen and CO2 levels
- rules out infections
Tests/clinical factors for predicting disease progression in IPF.
- DLco
- 6MWT
- FVC
What is DLco ?
diffusing capacity of the lung for CO
6MWT (6-minute walk test) purpose relating to IPF
walk distance correlates with mortality
FVC (forced vital capacity) purpose relating to IPF
initial value correlates with mortality
change over time correlates with progression
What is pulmonary arterial hypertension?
- enlarged right ventricle & constricted pulmonary arteries
- rapidly progressive, fatal, and incurable condition
- characterized by hypertension in the lungs
What does pulmonary arterial hypertension lead to?
right-sided heart failure and premature death
Signs and symptoms of pulmonary arterial hypertension?
- dyspnea
- angina pectoris (chest pain)
- dizziness
- syncope (fainting)
- fatigue
- edema
- dry cough
- Raynaud's (chalky white or dusty blue fingers)
Methods of diagnosis for Pulmonary Arterial Hypertension?
- blood test
- chest x-ray
- doppler EKG
- 6MWT
- right heart catheterization (most reliable)
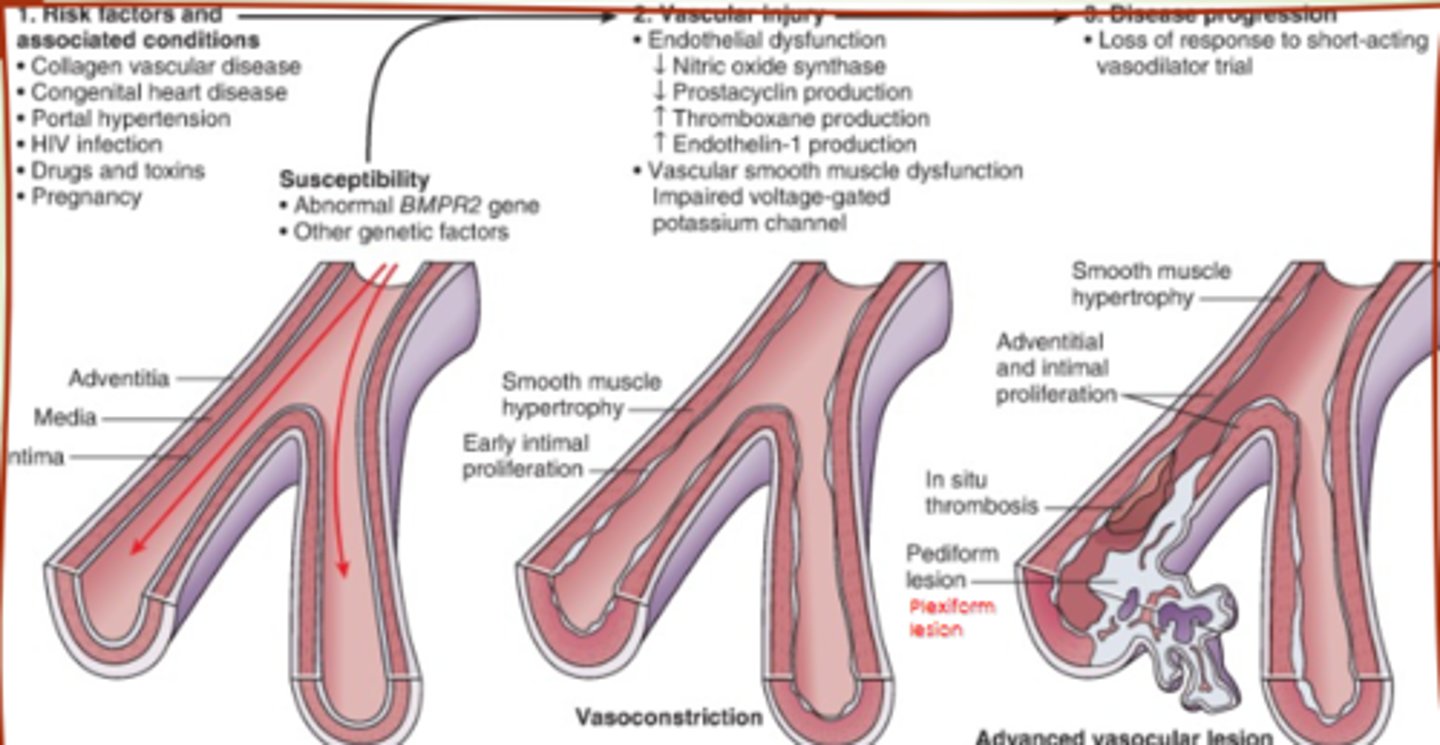
Pathophysiology of pulmonary arterial hypertension
- hypertrophy of smooth muscle (grow too much)
- endothelial dysfunction (lining can't relax)
- adventitial proliferation (outer layers grow too much)
- thrombosis and lesions (clots and scars)
What is Acute Respiratory Failure?
- life-threatening respiratory failure resulting from direct injury to the lungs, airways, or chest wall
- respiratory failure = inadequate gas exchange
Hypoxia vs Hypoxemia vs Hypercapmia
- hypoxia: reduced oxygen of cells in any tissues
- hypoxemia: reduced oxygen in arterial blood
- hypercapmia: too much CO2 in arterial blood
Treatment for hypercapnia
ventilator support/mechanical ventilation
Treatment for hypoxemia
- supplemental oxygen
- treat underlying cause
- respiratory stimulants
What is pulmonary edema?
- excess water in lungs
- emergency situation
Symptoms of pulmonary edema
dyspnea, increased work of breathing, excessive sweating, anxiety, hypoxemia, pale skin
Classic sign of pulmonary edema
pink frothy sputum
Most common cause of pulmonary edema
congestive heart failure
What is Aspiration?
- passage of solid particles into the lung
- can lead to bacterial pneumonia
Predisposing factors of aspiration
altered level of consciousness, seizure disorders, cerebrovascular accident and myasthenia gravis
When is aspiration severe?
large food particles
gastric fluid with pH <2.5
Clinical signs of aspiration
onset of choking, intractable cough
What causes initial development of ARDS (acute respiratory distress syndrome)?
- massive lung inflammatory response
- neutrophils overreact and release a lot of stuff that shouldn't be
Timeline of ARDS
- lungs fill with fluid and collapse
- then forms a thick sticky coating inside air sacs (hyaline membranes)
- finally leads to scarring that makes long-term damage
What is a hyaline membrane?
composed of proteins and dead cells that line the alveoli making gas exchange difficult or impossible
ARDS/ALI treatment
- mechanical ventilation
- prone positioning
- sedation to decrease O2 consumption
- neuromuscular blockers
- drugs to increase cardiac output and manage fluids
SARS CoV2
- enveloped, ssRNA virus
- possesses club-like spikes and an unusually large RNA genome
- genome encodes 4 essential structural proteins
SARS CoV 2 genome encodes for
- Spike protein (S)
- Nucleocapsid protein (N)
- Membrane protein (M)
- Envelope protein (E)
What are the primary reasons for death in COVID19 patients?
- respiratory distress
- infection
- pneumonia
What are the two FDA approved treatments for Covid-19?
- Remdesivir (hospital/IV use)
- Paxlovid (outpatient/oral use)
Remdesivir
- developed and tested to treat ebola
- in vitro antiviral activity against SARS CoV2
- outcompetes proofreading ability of exonuclease
Paxlovid (Nirmatrelvir and Ritonavir)
- Nirmatrelvir: main protease inhibitor
- Ritonavir: anti-HIV-1 protease and strong CYP3A inhibitor