rt check off week 5
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
hypoxemic hypoxia
most treatable by bronchial hygeine, removes airway obstruction
indications of bronchial hygiene therapy
difficulty with secretion clearance, >30mL a day, atelectasis caused by mucus plugging, cystic fibrosis, presence of foreign body in airway
hazards of bronchial therapy
increased intracranial pressure, hypoxemia, acute hypotension, vomit and aspiration, bronchospasm
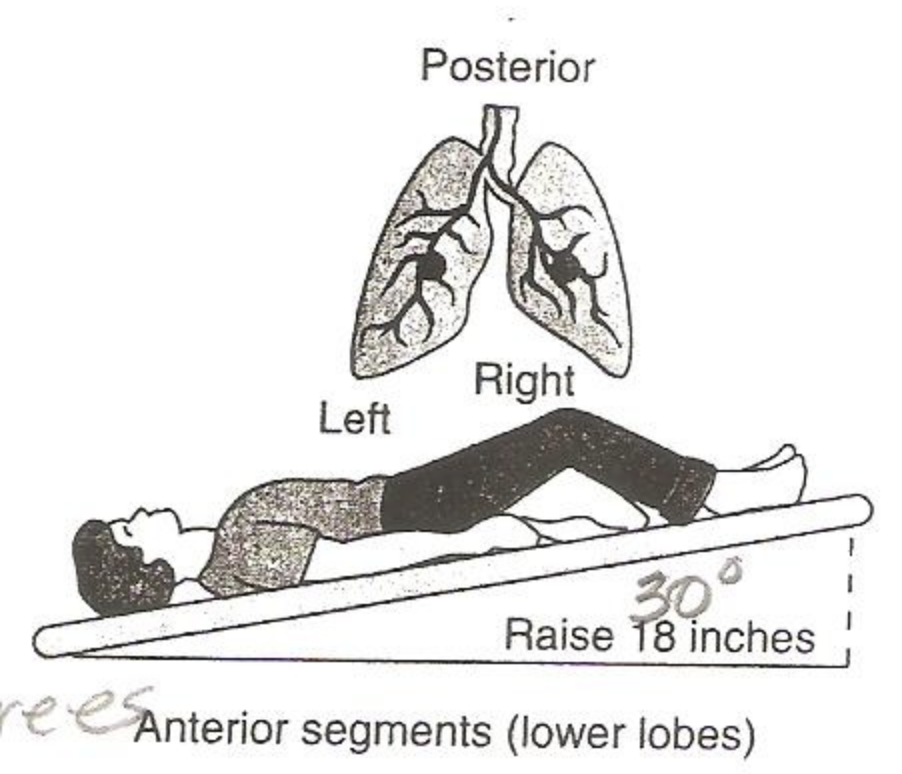
supine feet elevated 30 degrees
anterior lower lobes
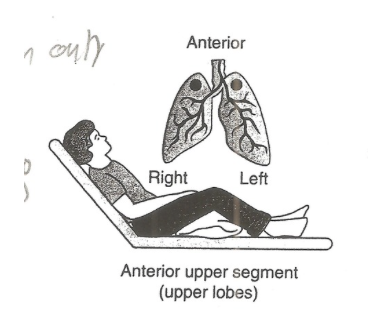
supine head elevated
anterior upper regions
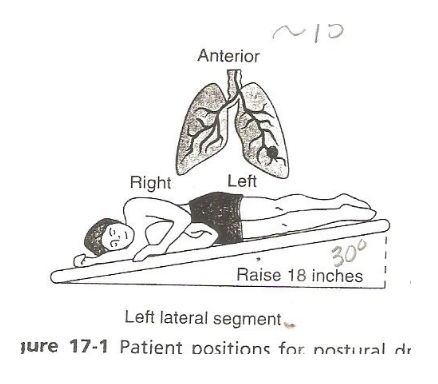
sidelaying, feet elevated 30 degrees
left lateral segment anterior sidelayinbg
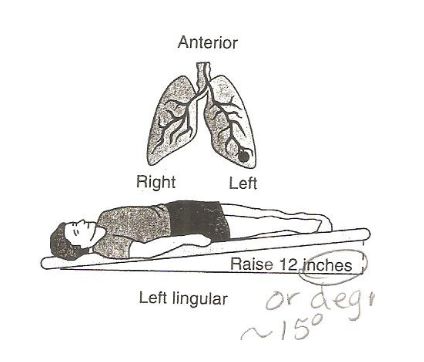
side laying feet elevated 15 degrees
left lingular anterior
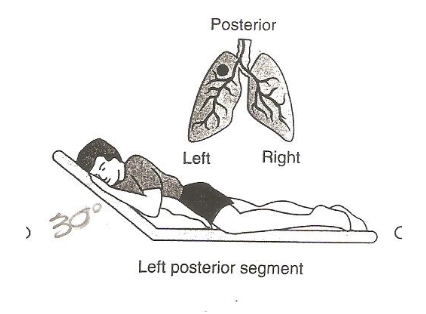
sidelaying head elevated
left posterior segment
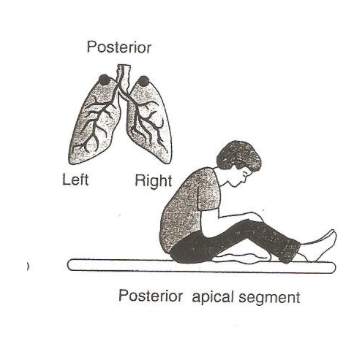
chair position learned forward
posterior apical segment
perform percussion
for 2-3 minutes
exhalations
apply vibration for 3 exhalations towards center
forced expiration technique
forced expirations from low to mid volume with glottis open, huff cough, breathe in and out slowly through pursed lips then huff
autogenic drainage
breathing through low to high lung volumes to move mucus, start with small breaths then breathe out, then medium breaths, then full breaths, followed by huff coughing
PAP therapy duration
10-20 breaths
PEP devices
use 10-20cmH2O expiratory pressure
percussive devices
use 30 cmH2O and start at max frequency then work down, institute periodic 5-10 sec breath hold
incentive spirometry
provides visual cues to patient when desired inspiratory volume of flow is reached, proved to be effective in high risk patients, you inhale into it, mimics a sigh

intermittent positive airway pressure breathing
noninvasive ventilation, goal is to achieve a deep sigh through a positive pressure assisted breath, increases Palv > Ppl
PEP indications
patients with expiratory airflow limitation will best respond, mimics pursed lip breathing by giving expiratory resistance, patient takes larger than tidal breath then exhales through device
oscillating PEP
expiratory pressure of 1-20cmH2O created by patient actively exhaling against a fixed orifice flow resistor or variable orifice thershold