Upper & Lower Extremity Physiologic Exams
1/50
Earn XP
Description and Tags
CVT Vascular 1
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
What is an ABI comprised of?
CW waveforms
pressure analysis
What should be the results of an ABI on a healthy patient?
pressure consistent in arms & legs
triphasic CW waveforms
What do the different types of physiologic exams provide?
ABI : initial assessment to establish arterial flow
segmental : determine level/segment of disease
PVR : same as seg but only will waveforms (NO pressures)
What are some capabilities of physiologic testing?
determines % of blood flow perfusing an extremity
determines presence & severity of occlusions
often 1st line of defense in establishing arterial disease
able to account for amount of perfusion by collateral flow (US CANT DO THIS)
What are some limitations of physiologic testing?
unable to distinguish between stenosis vs occlusion
multi-level disease makes it difficult to categorize & decipher specific segments
shows calcified vessels as falsely elevated
artificially elevated thigh pressures due to girth
dialysis patients with fistulas in UE
What should the CW probe be positioned in?
45 - 60 degree angle
What is the PPG sensor?
evaluates the blood flow in the the digits utilizing an infrared sensor that traces the RBCs & produces a distinct tracing
Where should you use a 10cm cuff?
ankles
calves
upper arm
forearm
When should you use a 12cm cuff?
high & low thigh
larger patients
If the cuff is too large how will the BP present?
artificially lower
If the cuff is too small how will the BP present?
artificially higher
What are some contraindications for an ABI or WBI?
patients with…
arterial bypasses
stent placement
deep venous thrombosis
recent groin access
open ulcerations
recent radial or brachial artery access
history of lymph node removal
mastectomy
How do you calculate an ABI?
higher RT/LT ankle pressure / higher arm pressure
How do you calculate an WBI?
higher RT/LT wrist pressure / higher arm pressure
What would indicate aorta-iliac segmental disease?
bilateral thigh pressures less than brachial pressures OR
bilateral high thigh indices of less than 1.25 (difference)
What would indicate ilio-femoral segmental disease?
unilateral thigh pressures less than brachial pressures OR
unilateral high thigh indices of less than 1.25 (difference)
What would indicate femoral-popliteal segmental disease?
pressure drop of 20 - 30 mmHg + from the high thigh OR
pressure drop of 20 - 30 mmHg + from the low thigh to the calf
What would indicate tibial peroneal segmental disease?
pressure drop of 20 - 30 mmHg + from the calf to any of the ankle pressures
A patient experiencing no symptoms may present with an ABI/WBI of..?
> or = 1.0
A patient experiencing claudication may present with an ABI/WBI of..?
< 0.80
A patient experiencing resting pain may present with an ABI/WBI of..?
< 0.40
A patient experiencing impending gangrene may present with an ABI/WBI of..?
< 0.20
A patient experiencing no symptoms may present with a TBI of..?
> 0.70
How would we categorize a mild disease with an ABI? What about TBI?
ABI : 0.90 - < 1.0
TBI : 0.60 - 0.69
How would we categorize a moderate disease with an ABI? What about TBI?
ABI : 0.50 - 0.90
TBI : 0.59 - 0.40
How would we categorize a severe disease with an ABI? What about TBI?
ABI : 0.30 - 0.50
TBI : < 0.39
How would we categorize a critical disease with an ABI?
ABI : < 0.30
What would be considered a brachial pressure gradient?
brachial pressure from one arm to the other has a > or = 15 - 20 mmHg difference
A significant change in a patient’s ankle/wrist brachial index form one visit to another is defined as?
> or = 0.15
What is reactive hyperemia?
a method to stress the flow in the arteries of the lower extremity when a patient is unable to ambulate however it is considered out-dated
What do you need to get a positive result for a physiologic stress test?
post pressure drop of 15-20% + at the 3-minute mark
How do you calculate a physiologic stress test?
take the pressure at the 3 minute mark & divide it by the resting pressure then take that number subtracting it by 1, then multiplying it by 100
ex:
resting pressure is 128 mmHg
3 minute post exercise pressure is 63 mmHg
63 / 128 = 0.49
1 - 0.49 = 0.51
0.51 × 100 = 51% drop
What is an indication for a physiologic stress test?
claudication
What is a contraindication for a physiologic stress test?
cardiac problems
recent stroke
impaired ambulation
severe hypertension
SOB
What should the post-treadmill recovery time be for a patient with no disease?
< 3 minutes
What should the post-treadmill recovery time be for a patient with single-level disease?
2 - 6 minutes
What should the post-treadmill recovery time be for a patient with multi-level disease?
6 - 12 minutes
What should the post-treadmill recovery time be for a patient with severe occlusive disease?
> 15 minutes
How do you examine for popliteal entrapment?
perform ABI first
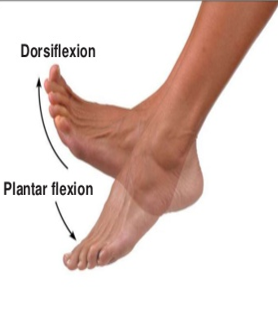
examine flexion maneuvers plantar & dorsi flexion by either :
interrogating with a PPG sensor on pad of great digit or
obtaining CW doppler waveform at both the PTA & DPA
What is plantar flexion?
the pointing of your toe to extend your entire foot
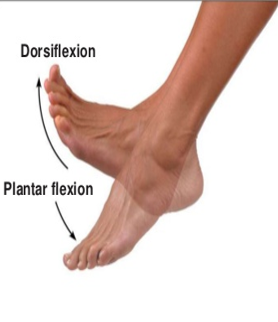
What is dorsi flexion?
the backwards being of your foot
What does laser doppler do?
assesses the characteristics of the microvascular blood volume in the capillary beds of the skin
What are some capabilities of laser doppler?
can determine the healing potential of a wound / ulcer & at which level to amputate
What are some limitations of laser doppler?
ulcerations (skin must be intact)
if patient is unable of remaining still
What are the prominent branches off the subclavian artery?
vertebral
thyrocervical
internal thoracic
costocervical
What is allen’s test?
determines dependency of the radial / ulnar arteries by evaluating waveforms whilst giving manual pressure to each artery individually
What is thoracic outlet syndrome?
compression of subclavian vein/artery by 1st rib resulting in either stenosis, occlusion, embolization, or swelling
What are the 3 types of thoracic outlet syndrome? Which is most common?
neurogenic : caused by compression of brachial plexus by rib (most common)
venous : arm abduction causes subclavian vein to be compressed
arterial : arm abduction & rotated causes subclavian vein to be compressed
How do you examine for thoracic outlet syndrome?
perform WBI 1st
PPG sensors are placed on digits to evaluate waveforms during different maneuvers such as :
sitting still & turning head
moving hands slightly backwards on lap (costoclavicular)
abducting arm 90 & 180 degrees
& whatever position the patient feels symptomatic in

What is the differences between primary & secondary raynaud’s?
primary : idiopathic, symptomatic for years, color changing of digits, bilateral, no ulcerations
secondary : caused by underlying condition, rapid onset, unilateral, occlusion, ulceration present
How do you examine for raynaud’s?
perform WBI 1st
use PPG tracings & evaluate perfusion at rest, in cold water, & in warm water for approximately 1 - 3 minutes each